
Geranylgeraniol Application in Human Osteoblasts and Osteoclasts for Reversal of the Effect of Bisphosphonates
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culture
2.2. Bisphosphonates and Geranylgeraniol
2.3. Cell Viability
2.4. Vitronectin Receptor Staining and Cell Count
2.5. Bone Resorption Pit Assay
2.6. Messenger RNA Extraction and Quantitative Real-Time Polymerase Chain Reaction
2.7. Western Blot Analysis
2.8. Statistical Analysis
3. Results
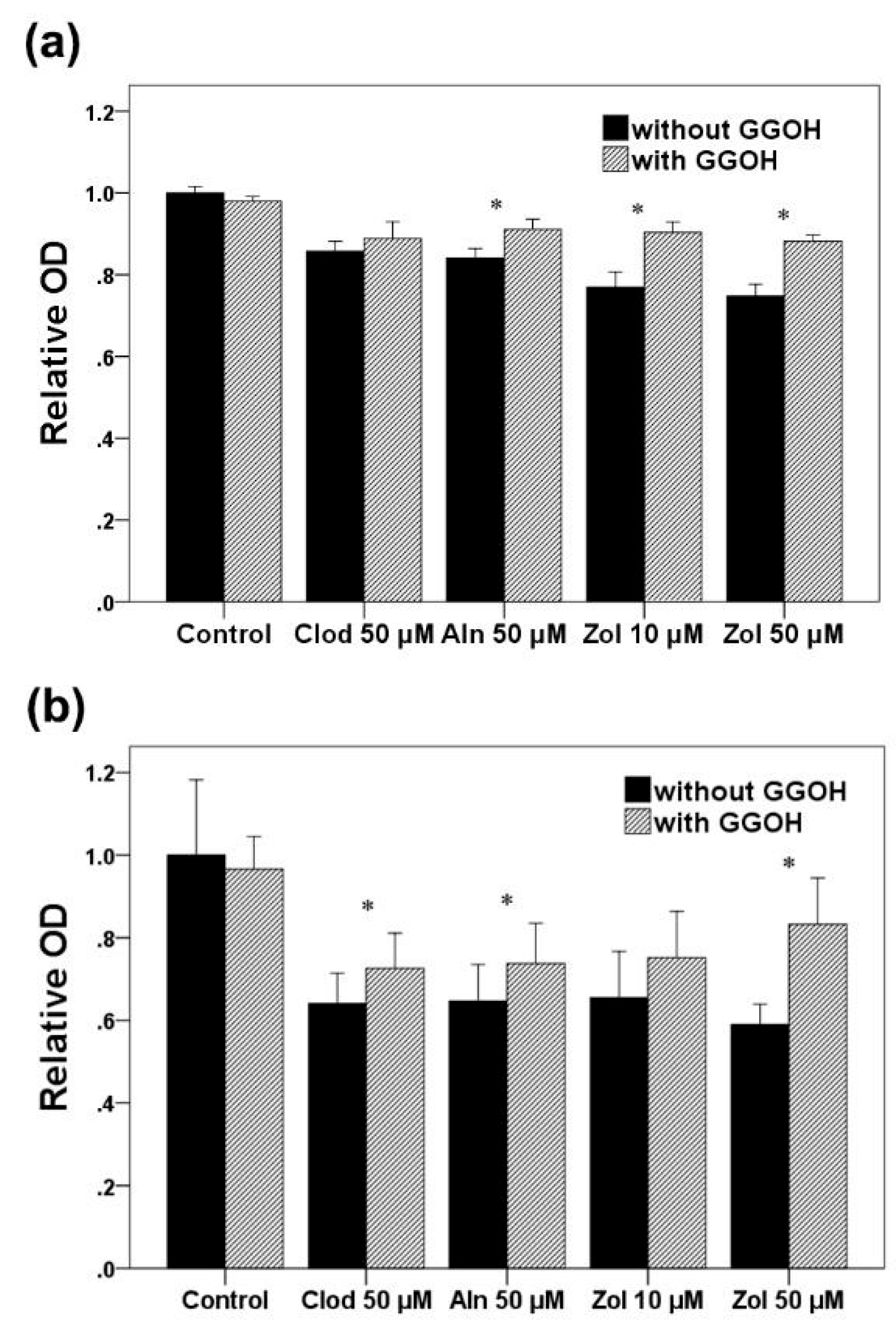
3.1. Cell Viability
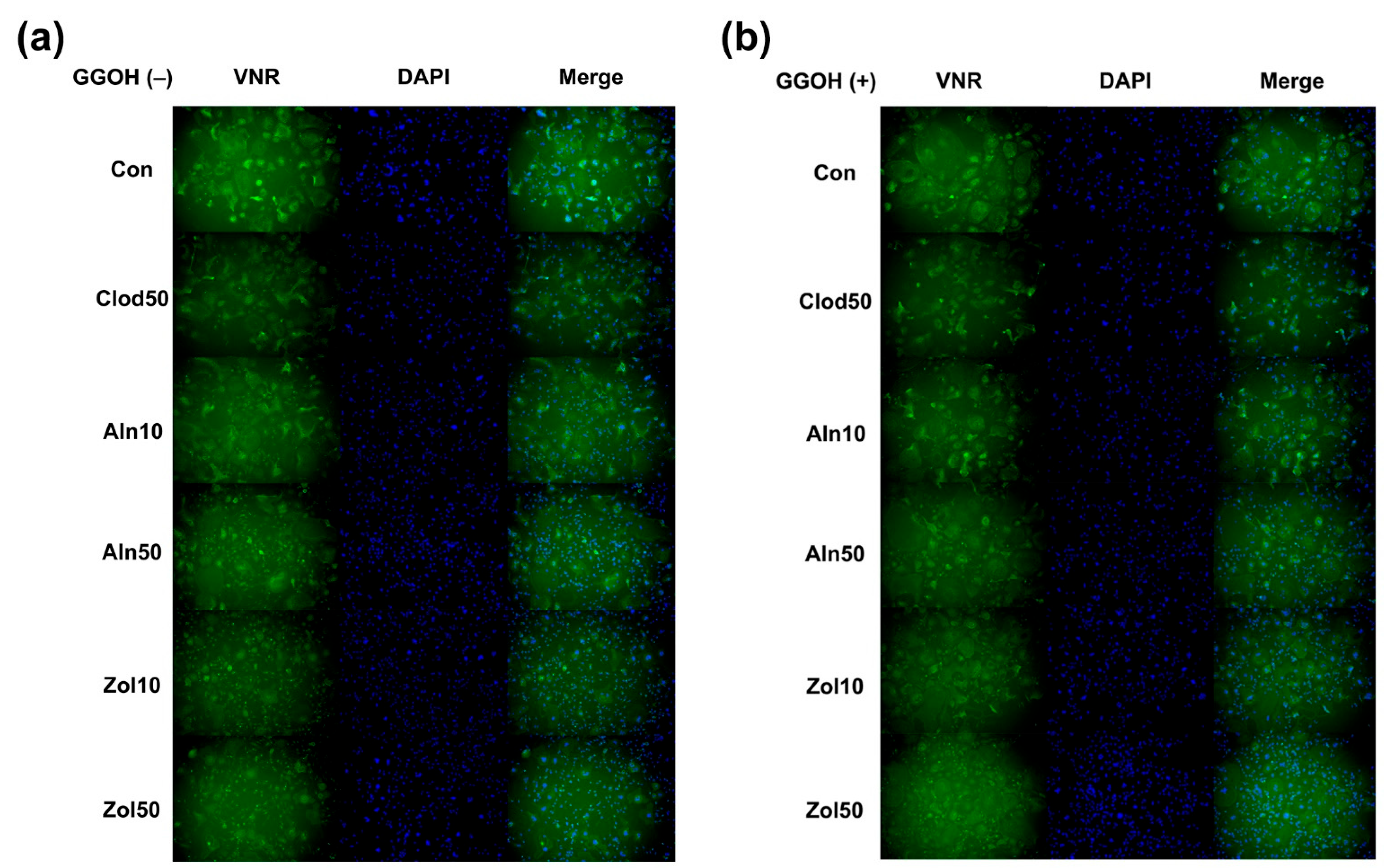
3.2. Osteoclast Differentiation
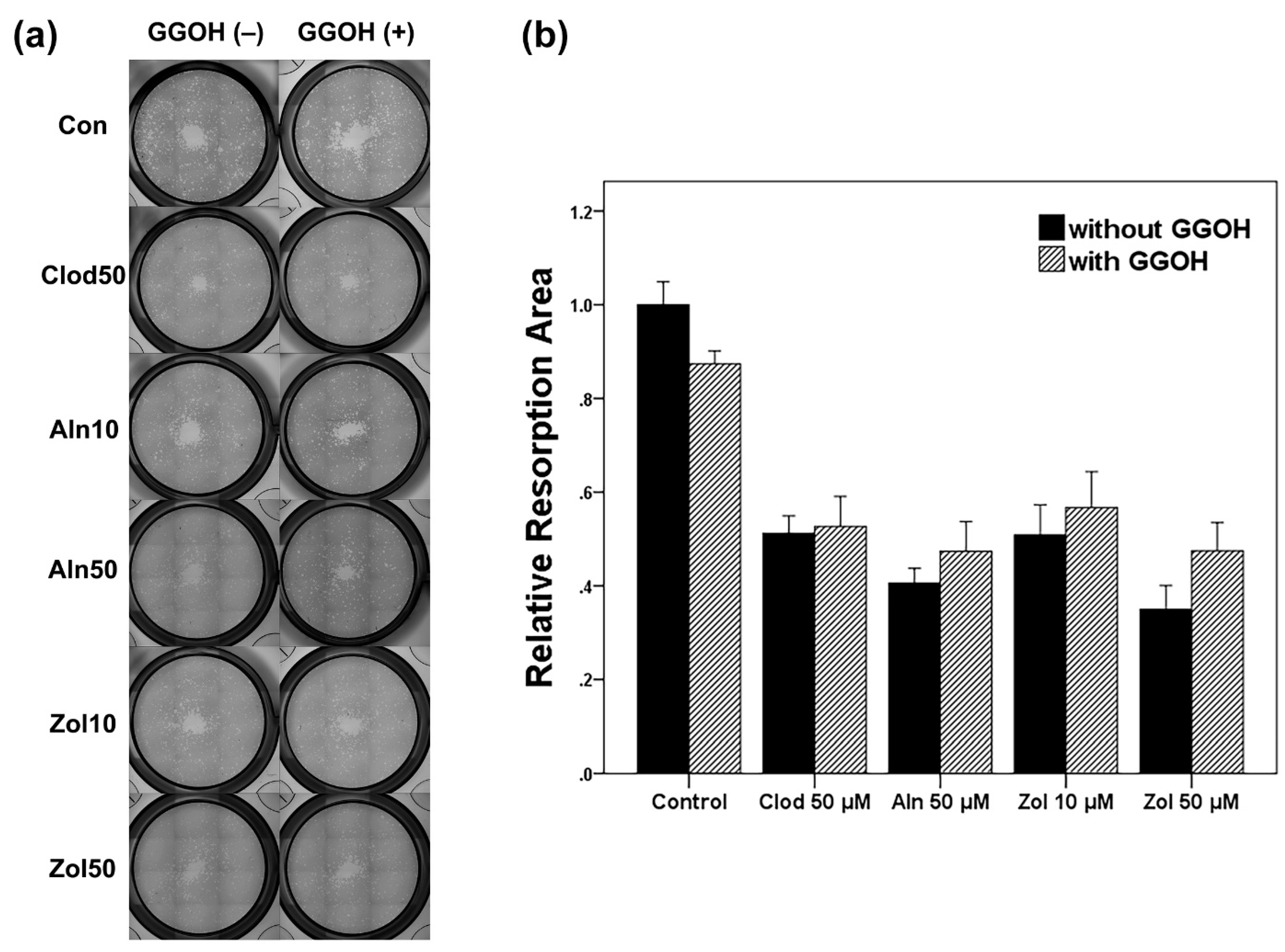
3.3. Resorption Area Analysis
3.4. Gene Expression and Protein Synthesis
3.4.1. Osteoblasts
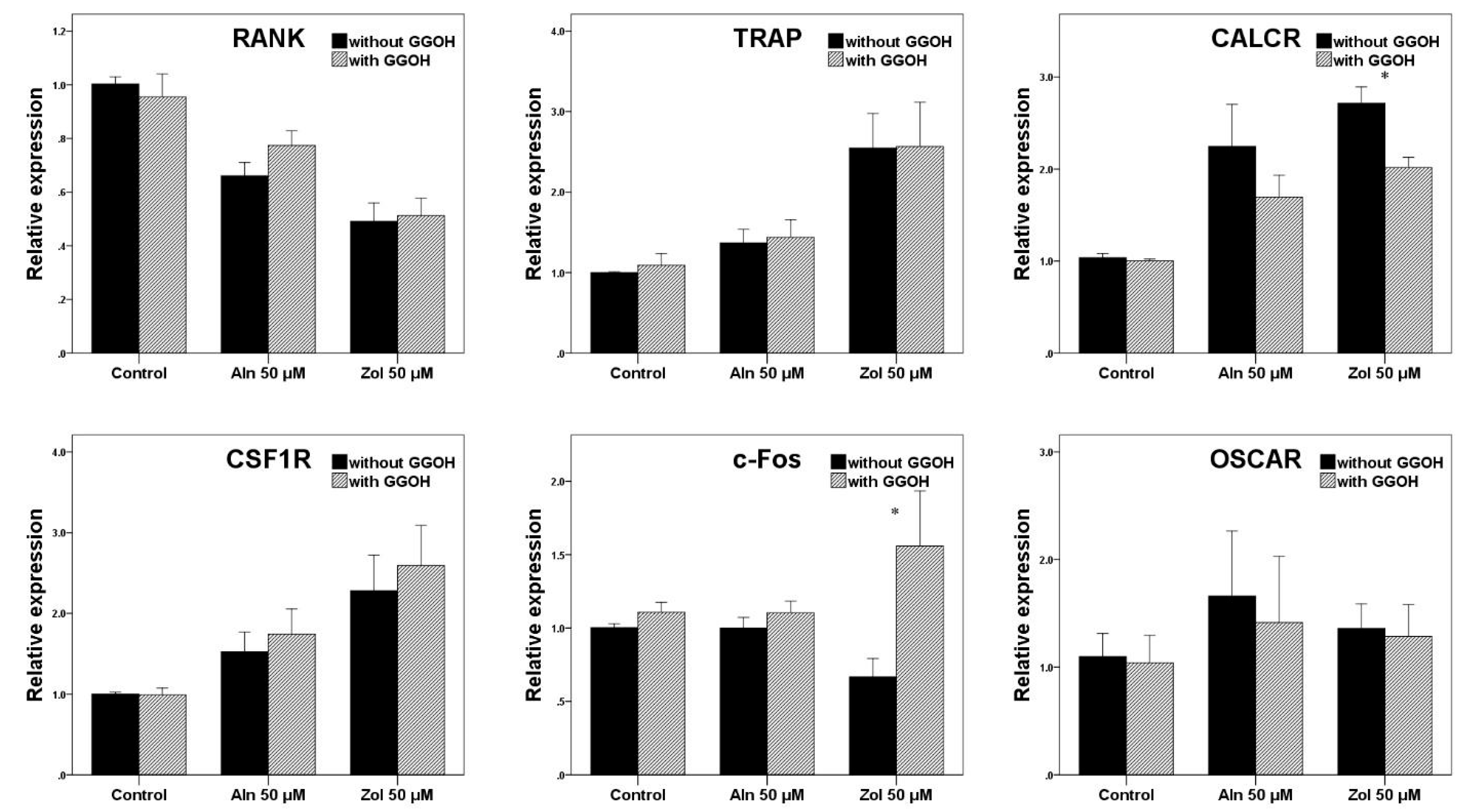
3.4.2. Osteoclasts
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walsh, J.P.; Ward, L.C.; Stewart, G.O.; Will, R.K.; Criddle, R.A.; Prince, R.L.; Stuckey, B.G.; Dhaliwal, S.S.; Bhagat, C.I.; Retallack, R.W.; et al. A randomized clinical trial comparing oral alendronate and intravenous pamidronate for the treatment of Paget’s disease of bone. Bone 2004, 34, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Majoor, B.C.; Appelman-Dijkstra, N.M.; Fiocco, M.; van de Sande, M.A.; Dijkstra, P.S.; Hamdy, N.A. Outcome of Long-Term Bisphosphonate Therapy in McCune-Albright Syndrome and Polyostotic Fibrous Dysplasia. J. Bone Miner. Res. 2017, 32, 264–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parisi, M.S.; Oliveri, M.B.; Mautalen, C.A. Bone mineral density response to long-term bisphosphonate therapy in fibrous dysplasia. J. Clin. Densitom. 2001, 4, 167–172. [Google Scholar] [CrossRef] [PubMed]
- McKeage, K.; Plosker, G.L. Zoledronic acid: A pharmacoeconomic review of its use in the management of bone metastases. Pharmacoeconomics 2008, 26, 251–268. [Google Scholar] [CrossRef]
- Smith, M.R. Zoledronic acid to prevent skeletal complications in cancer: Corroborating the evidence. Cancer Treat. Rev. 2005, 31 (Suppl. 3), 19–25. [Google Scholar] [CrossRef]
- Hosaka, S.; Katagiri, H.; Niwakawa, M.; Harada, H.; Wasa, J.; Murata, H.; Takahashi, M. Radiotherapy combined with zoledronate can reduce skeletal-related events in renal cell carcinoma patients with bone metastasis. Int. J. Clin. Oncol. 2018, 23, 1127–1133. [Google Scholar] [CrossRef]
- Russell, R.G. Bisphosphonates: The first 40 years. Bone 2011, 49, 2–19. [Google Scholar] [CrossRef]
- McGowan, K.; McGowan, T.; Ivanovski, S. Risk factors for medication-related osteonecrosis of the jaws: A systematic review. Oral Dis. 2018, 24, 527–536. [Google Scholar] [CrossRef]
- Yamada, S.I.; Kurita, H.; Kondo, E.; Suzuki, S.; Nishimaki, F.; Yoshimura, N.; Morioka, M.; Ishii, S.; Kamata, T. Treatment outcomes and prognostic factors of medication-related osteonecrosis of the jaw: A case- and literature-based review. Clin. Oral Investig. 2019, 23, 3203–3211. [Google Scholar] [CrossRef]
- Hernlund, E.; Svedbom, A.; Ivergard, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jonsson, B.; Kanis, J.A. Osteoporosis in the European Union: Medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch. Osteoporos. 2013, 8, 136. [Google Scholar] [CrossRef] [Green Version]
- Saad, F. Clinical benefit of zoledronic acid for the prevention of skeletal complications in advanced prostate cancer. Clin. Prostate Cancer 2005, 4, 31–37. [Google Scholar] [CrossRef]
- Abrahamsen, B. Adverse effects of bisphosphonates. Calcif. Tissue Int. 2010, 86, 421–435. [Google Scholar] [CrossRef]
- Reid, I.R. Osteonecrosis of the jaw: Who gets it, and why? Bone 2009, 44, 4–10. [Google Scholar] [CrossRef]
- Luckman, S.P.; Hughes, D.E.; Coxon, F.P.; Graham, R.; Russell, G.; Rogers, M.J. Nitrogen-containing bisphosphonates inhibit the mevalonate pathway and prevent post-translational prenylation of GTP-binding proteins, including Ras. J. Bone Miner. Res. 1998, 13, 581–589. [Google Scholar] [CrossRef]
- Rogers, M.J.; Crockett, J.C.; Coxon, F.P.; Monkkonen, J. Biochemical and molecular mechanisms of action of bisphosphonates. Bone 2011, 49, 34–41. [Google Scholar] [CrossRef]
- Sinensky, M.; Lutz, R.J. The prenylation of proteins. Bioessays 1992, 14, 25–31. [Google Scholar] [CrossRef]
- Palsuledesai, C.C.; Distefano, M.D. Protein prenylation: Enzymes, therapeutics, and biotechnology applications. ACS Chem. Biol. 2015, 10, 51–62. [Google Scholar] [CrossRef] [Green Version]
- Ziebart, T.; Koch, F.; Klein, M.O.; Guth, J.; Adler, J.; Pabst, A.; Al-Nawas, B.; Walter, C. Geranylgeraniol—A new potential therapeutic approach to bisphosphonate associated osteonecrosis of the jaw. Oral Oncol. 2011, 47, 195–201. [Google Scholar] [CrossRef]
- Zafar, S.; Coates, D.E.; Cullinan, M.P.; Drummond, B.K.; Milne, T.; Seymour, G.J. Zoledronic acid and geranylgeraniol regulate cellular behaviour and angiogenic gene expression in human gingival fibroblasts. J. Oral Pathol. Med. 2014, 43, 711–721. [Google Scholar] [CrossRef]
- Koneski, F.; Popovic-Monevska, D.; Gjorgoski, I.; Krajoska, J.; Popovska, M.; Muratovska, I.; Velickovski, B.; Petrushevska, G.; Popovski, V. In vivo effects of geranylgeraniol on the development of bisphosphonate-related osteonecrosis of the jaws. J. Craniomaxillofac. Surg. 2018, 46, 230–236. [Google Scholar] [CrossRef]
- Pabst, A.M.; Kruger, M.; Ziebart, T.; Jacobs, C.; Sagheb, K.; Walter, C. The influence of geranylgeraniol on human oral keratinocytes after bisphosphonate treatment: An in vitro study. J. Craniomaxillofac. Surg. 2015, 43, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Pabst, A.M.; Kruger, M.; Sagheb, K.; Ziebart, T.; Jacobs, C.; Blatt, S.; Goetze, E.; Walter, C. The influence of geranylgeraniol on microvessel sprouting after bisphosphonate substitution in an in vitro 3D-angiogenesis assay. Clin. Oral Investig. 2017, 21, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Favia, G.; Tempesta, A.; Limongelli, L.; Crincoli, V.; Maiorano, E. Medication-related osteonecrosis of the jaw: Surgical or non-surgical treatment? Oral Dis. 2018, 24, 238–242. [Google Scholar] [CrossRef]
- Jung, J.; Yoo, H.Y.; Kim, G.T.; Lee, J.W.; Lee, Y.A.; Kim, D.Y.; Kwon, Y.D. Short-Term Teriparatide and Recombinant Human Bone Morphogenetic Protein-2 for Regenerative Approach to Medication-Related Osteonecrosis of the Jaw: A Preliminary Study. J. Bone Miner. Res. 2017, 32, 2445–2452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owosho, A.A.; Estilo, C.L.; Huryn, J.M.; Yom, S.K. Pentoxifylline and tocopherol in the management of cancer patients with medication-related osteonecrosis of the jaw: An observational retrospective study of initial case series. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 455–459. [Google Scholar] [CrossRef] [Green Version]
- Zafar, S.; Cullinan, M.P.; Drummond, B.K.; Seymour, G.J.; Coates, D.E. Effects of zoledronic acid and geranylgeraniol on angiogenic gene expression in primary human osteoclasts. J. Oral Sci. 2020, 62, 79–83. [Google Scholar] [CrossRef] [Green Version]
- Fliefel, R.M.; Entekhabi, S.A.; Ehrenfeld, M.; Otto, S. Geranylgeraniol (GGOH) as a Mevalonate Pathway Activator in the Rescue of Bone Cells Treated with Zoledronic Acid: An In Vitro Study. Stem Cells Int. 2019, 2019, 4351327. [Google Scholar] [CrossRef] [Green Version]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Marx, R.E. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef]
- Wennerberg, K.; Rossman, K.L.; Der, C.J. The Ras superfamily at a glance. J. Cell Sci. 2005, 118, 843–846. [Google Scholar] [CrossRef] [Green Version]
- Jeong, A.; Suazo, K.F.; Wood, W.G.; Distefano, M.D.; Li, L. Isoprenoids and protein prenylation: Implications in the pathogenesis and therapeutic intervention of Alzheimer’s disease. Crit. Rev. Biochem. Mol. Biol. 2018, 53, 279–310. [Google Scholar] [CrossRef]
- Zafar, S.; Coates, D.E.; Cullinan, M.P.; Drummond, B.K.; Milne, T.; Seymour, G.J. Effects of zoledronic acid and geranylgeraniol on the cellular behaviour and gene expression of primary human alveolar osteoblasts. Clin. Oral Investig. 2016, 20, 2023–2035. [Google Scholar] [CrossRef]
- Casey, P.J.; Solski, P.A.; Der, C.J.; Buss, J.E. p21ras is modified by a farnesyl isoprenoid. Proc. Natl. Acad. Sci. USA 1989, 86, 8323–8327. [Google Scholar] [CrossRef] [Green Version]
- Colicelli, J. Human RAS superfamily proteins and related GTPases. Sci. STKE 2004, 2004, RE13. [Google Scholar] [CrossRef] [Green Version]
- Ho, H.J.; Shirakawa, H.; Giriwono, P.E.; Ito, A.; Komai, M. A novel function of geranylgeraniol in regulating testosterone production. Biosci. Biotechnol. Biochem. 2018, 82, 956–962. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Forward (5′-3′) | Reverse (5′-3′) |
|---|---|---|
| ALP | CCGTGGCAACTCT ATCTTTGG | GCCATACAGGAT GGCAGTGA |
| OC | AAGAGACCCAGG CGCTACCT | AACTCGTCACAG TCCGGATTG |
| M-CSF | CTCCAGAGAGAG GAGCCTGA | AGTATAGACACT CGTCACTGGTG |
| RANKL | ATACCCTGATGAAAGGAGGA | GGGGCTCAATCTATATCTCG |
| COL1 | CCCTGGAAAGAATGGAGATGAT | ACTGAAACCTCTGTGTCCCTTCA |
| RUNX2 | AGCAAGGTTCAACGATCTGAGAT | TTTGTGAAGACGGTTATGGTCAA |
| RANK | TGTGGCACTGGATCAATGAG | GTCTTGCTGACCAATGAGAG |
| TRAP | GATCCTGGGTGCAGACTTCA | GCGCTTGGAGATCTTAGAGT |
| CALCR | GACAACTGCTGGCTGAGTG | GAAGCAGTAGATGGTCGCAA |
| CSF1R | GGCTCCTGGGCCTTCATACC | CAAAGGCTCCAGCTCCGAGG |
| c-Fos | TGTCTGTGGCTTCCCTTGAT | ATCAAAGGGCTCGGTCTTCA |
| OSCAR | GAGTAGCTGAAAGGAAGACGCGAT | CAGAGCGCTGATTGGTCCATCTTA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.; Park, J.S.; Chun, J.; Al-Nawas, B.; Ziebart, T.; Kwon, Y.-D. Geranylgeraniol Application in Human Osteoblasts and Osteoclasts for Reversal of the Effect of Bisphosphonates. Life 2023, 13, 1353. https://doi.org/10.3390/life13061353
Jung J, Park JS, Chun J, Al-Nawas B, Ziebart T, Kwon Y-D. Geranylgeraniol Application in Human Osteoblasts and Osteoclasts for Reversal of the Effect of Bisphosphonates. Life. 2023; 13(6):1353. https://doi.org/10.3390/life13061353
Chicago/Turabian StyleJung, Junho, Jung Soo Park, Jeewan Chun, Bilal Al-Nawas, Thomas Ziebart, and Yong-Dae Kwon. 2023. "Geranylgeraniol Application in Human Osteoblasts and Osteoclasts for Reversal of the Effect of Bisphosphonates" Life 13, no. 6: 1353. https://doi.org/10.3390/life13061353