Abstract
Background and objective: Sarcopenia with muscle wasting and weakness is a common occurrence among patients with chronic obstructive pulmonary disease (COPD). We aimed to evaluate the clinical outcomes of sarcopenia in patients with COPD. Methods: We reviewed the electronic medical records of 71 patients with COPD between 1 January 2012, and 31 December 2018. We longitudinally analyzed clinical outcomes in patients with COPD with and without sarcopenia. Results: Compared to the non-sarcopenia group COPD, the sarcopenia group showed a higher rate of acute exacerbation events of COPD (AE COPD, 84.6% vs. 31.0%, p = 0.001), all-cause mortality (30.8% vs. 5.2%, p = 0.022), and pneumonia occurrence per year (median [first quartile–third quartile]; 0.2 [0.0–1.6] vs. 0.0 [0.0–0.2], p = 0.025). Sarcopenia was an independent risk factor for AE COPD in Cox regression analysis (hazard ratio, 5.982; 95% confidence interval, 1.576–22.704). Hand grip strength was associated with the COPD Assessment Test (CAT) score and annual Charlson’s comorbidity index score change. Total skeletal muscle mass index (SMMI) was associated with the modified medical research council dyspnea scale score, CAT score, body mass index, airflow obstruction, dyspnea, and exercise (BODE) index, and alanine transaminase. Trunk SMMI was significantly associated with AE COPD, while appendicular SMMI was associated with BODE index and annual intensive care unit admissions for AE COPD. Conclusions: Sarcopenia is associated with clinical prognosis, pneumonia occurrence, and the acute exacerbation of COPD requiring intensive care in patients with COPD. Therefore, it is important to carefully monitor sarcopenia development as well as recommend appropriate exercise and nutritional supplementation in patients with COPD.
1. Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive and persistent airway disease with an enormous socioeconomic burden worldwide. COPD is associated with multi-morbid conditions, including cardiovascular disease, osteoporosis, muscle weakness, depression, and lung cancer [1]. Further, COPD is associated with loss of muscle mass, especially in patients with moderate-to-severe COPD and acute COPD exacerbations [2,3,4,5].
Sarcopenia, a progressive and systemic skeletal muscle disorder, is closely associated with an elevated risk of detrimental outcomes, including falls, fractures, physical disability, and mortality [6,7]. According to the European Working Group on Sarcopenia in Older People (EWGSOP2) guidelines, sarcopenia is diagnosed based on two main criteria: low muscle strength and low muscle quantity or quality. Additionally, when low physical performance is present in conjunction with these criteria, it is defined as severe sarcopenia [7]. The reported prevalence of sarcopenia is 10–27% in the general population [8]. Similarly, the prevalence of sarcopenia among patients with COPD ranges from 8% in population-based studies to 21% in clinic-based studies [9].
Sarcopenia has been reported to result in worsening clinical outcomes, forced expiratory volume in the first second (FEV1), and reduced exercise capacity and quality of life [10]. In particular, the acute exacerbation of COPD (AE COPD) and sarcopenia interact and adversely affect the prognosis of COPD [11]. However, data on the long-term clinical outcomes of patients with COPD who also have sarcopenia are still insufficient.
Based on the European Working Group on Sarcopenia in Older People (EWGSOP) criteria, we previously reported that the prevalence of sarcopenia among patients with COPD was 25% [12]. Moreover, sarcopenia was associated with respiratory symptoms and exercise tolerance in stable patients with COPD. However, this was a cross-sectional analysis, which limits the clinical interpretation of the findings. In addition, the Asian Working Group for Sarcopenia (AWGS) was updated in 2019 and can be applied to Asians [13].
We hypothesize that sarcopenia not only increases the risk of AE COPD but also correlates with worsening symptoms and an overall poor prognosis. Therefore, our objective was to assess the extended clinical outcomes of COPD patients with sarcopenia, as defined by the AWGS 2019 criteria, utilizing the cohort derived from the preceding cross-sectional study [12].
2. Materials and Methods
2.1. Study Design and Patients
In our previous cross-sectional study, we enrolled eligible patients who provided written informed consent (Figure 1) [12]. The inclusion criteria were age >40 years, COPD diagnosis according to the Global Initiative for Chronic Obstructive Lung Disease, and outpatient visits between June 2012 and June 2014 to Gangnam Severance Hospital. We excluded patients with active lung disease, bronchial asthma, lung resection or transplantation, severe cardiovascular disease, COPD exacerbation within the last month, severe dyspnea impeding the six-minute walk distance test, lower-leg trauma, severe muscle weakness, and an inability to comprehend the informed consent documents. Patients were followed up at the outpatient clinic. We retrospectively reviewed their electronic medical records until 31 December 2018. Further, consenting patients were included in a secondary cross-sectional analysis of muscle mass measurements.
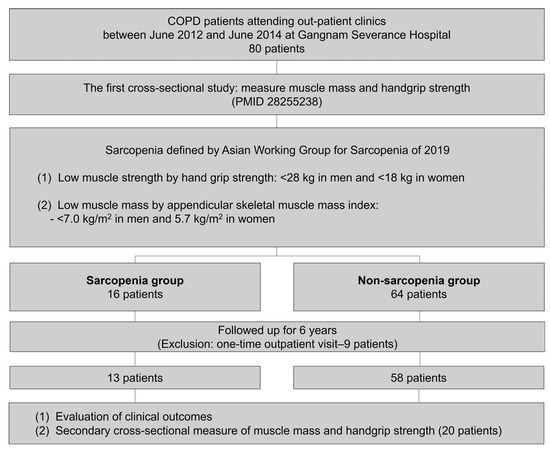
Figure 1.
Study flow.
2.2. Measurement of Muscle Mass and Strength
Muscle mass was quantified using bioelectrical impedance analysis (BIA; Body Composition Analysis 1000; MediGate, Seoul, South Korea) in the first cross-sectional analysis and dual-energy X-ray absorptiometry (DEXA; Horizon W, Hologic Inc., Bedford, MA, USA), which is the gold-standard technique for molecular-level analysis of body composition [14], in the second cross-sectional analysis. The fat mass index (FMI) and fat-free mass index (FFMI) were calculated as the fat mass and fat-free mass (FFM), respectively, divided by the square of the patient’s height (kg/height2). The skeletal muscle mass index (SMMI) was calculated as skeletal muscle mass (SMM) divided by the square of the patient’s height (kg/height2). The appendicular and truncal SMMI (ASMI and TSMI, respectively) reflected the muscle mass of the limbs and trunk, respectively.
Handgrip strength (HGS) was measured using a Jamar handheld dynamometer (Patterson Medical, Warrenville, IL, USA), which has validated reliability in community-dwelling older adults. Participants were seated with the shoulders at 0° adduction and neutral rotation, elbows at 90° flexion, and forearms in a neutral position. The participants performed three trials with 1 min rest intervals, and the average values were recorded.
2.3. Definition of Sarcopenia
Sarcopenia was confirmed by the presence of both low muscle strength and low muscle mass based on the AWGS 2019 guidelines. Low muscle mass was defined as an appendicular skeletal muscle mass index (ASMI) by BIA of <7.0 kg/m2 in men and 5.7 kg/m2 in women. Low muscle strength was defined by HGS values of <28 kg in men and <18 kg in women.
2.4. Data Collection
Demographic characteristics included age, sex, height (cm), weight (kg), and body mass index (BMI; kg/m2). Comorbidities were analyzed using Charlson’s comorbidity index (CCI). FEV1, forced vital capacity (FVC), and forced mid-expiratory flow (FEF25–75%) were measured using spirometry (Vmax 229; SensorMedics, Yorba Linda, CA, USA), and converted to z-scores of the Global Lung Function Initiative 2012 (GLI 2012). Hemoglobin, aspartate aminotransferase (AST), alanine transaminase (ALT), blood urea nitrogen, creatinine, and C-reactive protein were measured at baseline and during follow-up visits. Interleukin-6 and high-sensitivity tumor necrosis factor-alpha (hsTNF-α) were measured in the second cross-sectional analysis.
2.5. Clinical Outcomes and Symptoms
The primary endpoint was the occurrence of AE COPD, while secondary endpoints included all-cause mortality, pneumonia development, outpatient/emergency room visits, and admissions to the general ward or intensive care unit (ICU). COPD symptoms were evaluated using the Korean version of the COPD Assessment Test (CAT) questionnaire (GlaxoSmithKline, London, UK) and the modified Medical Research Council (mMRC) dyspnea scale. We evaluated the BMI, degree of airflow obstruction, dyspnea, and exercise capacity using the BMI, airflow obstruction, dyspnea, and exercise (BODE) index [15].
3. Ethics
This study was approved by the Institutional Review Board (IRB) of Gangnam Severance Hospital (number: 3-2018-0109). Participants provided written informed consent to participate in the second cross-sectional study. Data were collected in accordance with the amended Declaration of Helsinki. All data for the retrospective analysis of clinical outcomes were fully anonymized before being accessed, and the ethics committee waived the requirement for written informed consent because of the retrospective nature of this study.
4. Statistical Analysis
Between-group comparisons of categorical variables were performed using the chi-square test or Fisher’s exact test. Based on the Shapiro–Wilk test, parametric and non-parametric continuous variables were compared using an independent two-sample t-test and Kruskal–Wallis rank sum test, respectively. Between-group comparisons of temporal changes in spirometry findings were performed using two-way repeated measures analysis of variance (RM-ANOVA). Correlations between variables were analyzed using Pearson’s correlation analysis. Statistical significance was set at p < 0.05.
Statistical analyses were conducted using R (version 4.0.2; R Foundation for Statistical Computing, Vienna, Austria) software. Cox regression analysis was performed using “survival” R package. In the multivariate model, age, sex, CCI, and variables with p < 0.100 in the univariate Cox regression analysis were included. Multicollinearity was assessed using the variance inflation factor (VIF), and a VIF of 5 or greater was considered to indicate the presence of multicollinearity. Pearson’s correlation analysis and RM-ANOVA were performed using the “stats” and “rstatix” R packages, respectively. Spirometry values were converted to z-score by reference values of GLI 2012 using the “rspiro” R package. Kaplan–Meier analysis was performed using the “survminer” R package.
5. Results
Baseline characteristics
Among 71 patients with COPD, there were 13 and 58 patients with and without sarcopenia, respectively (Table 1). There were no significant between-group differences in age, sex, height, CCI score, waist–hip ratio, smoking history, and treatment of COPD. Body weight and BMI were lower in the sarcopenia group than in the non-sarcopenia group (median [first quartile; third quartile]; 56.0 [50.0; 61.7] vs. 63.9 [59.0; 70.0], p = 0.005; and 21.5 [20.1;22.5] vs. 23.2 [21.5; 25.7], p = 0.003; respectively). SMMI, FFM, and FMMI were lower in the sarcopenia group than in the non-sarcopenia group (mean ± standard deviation; 8.6 ± 0.7 vs. 9.7 ± 0.9, p < 0.001; 43.7 ± 4.6 vs. 48.9 ± 6.8, p = 0.011; and 16.1 ± 1.0 vs. 17.6 ± 1.2, p < 0.001; respectively). There were no significant between-group differences in fat mass and FMI (13.0 ± 3.7 vs. 16.2 ± 5.6, p = 0.054 and 4.8 ± 1.5 vs. 5.9 ± 2.0, p = 0.086; respectively). HGS was lower in the sarcopenia group than in the non-sarcopenia group (26.3 [24.7; 26.3] vs. 33.7 [29.0; 39.3], p < 0.001). There were no significant between-group differences in baseline spirometry findings. Regarding baseline laboratory data, only ALT (IU/L) levels were higher in the sarcopenia group than in the non-sarcopenia group (14.0 [11.0; 18.0] vs. 19.0 [14.0; 23.0], p = 0.030).

Table 1.
Baseline characteristics.
6. Clinical Outcomes and Prognosis of Patients with COPD with Sarcopenia
Throughout the observation period, the sarcopenia group experienced a higher incidence (advent of events) and frequency (events per year) of AE COPD than non-sarcopenia group (84.6% vs. 31.0%, p = 0.001 and 0.6 [0.3; 1.1] vs. 0.0 [0.0; 0.2], p = 0.001, respectively; Table 2). Furthermore, the experience and frequency of admissions for COPD (84.6% vs. 27.6%, p < 0.001 and 0.6 [0.3; 1.1] vs. 0.0 [0.0; 0.2], p < 0.001; respectively), and experience and frequency of ICU admissions for AE COPD (30.8 vs. 3.4%, p = 0.008 and 0.0 [0.0; 0.2] vs. 0.0 [0.0; 0.0], p = 0.001; respectively), all-cause admissions (92.3% vs. 55.2%, p = 0.029), ICU admissions (38.5% vs. 5.2%, p = 0.003), frequency of all-cause admission (0.5 [0.2; 2.2] vs. 0.2 [0.0; 0.5], p = 0.025), and frequency of ICU admission (0.0 [0.0; 0.2] vs. 0.0 [0.0; 0.0], p = 0.001) were all higher in the sarcopenia group. The sarcopenia group had a higher all-cause mortality rate (30.8% vs. 5.2%, p = 0.022).
Table 2.
Comparison of clinical outcomes between groups during the observational period.
The sarcopenia group had a significantly higher frequency of annual pneumonia (0.2 [0.0; 1.6] vs. 0.0 [0.0; 0.2], p = 0.025), but their experience of pneumonia was not higher than the non-sarcopenia group (53.8% vs. 31.0%, p = 0.217). There were no between-group differences in annual changes in the z-score of FEV1, FVC, FEV1/FVC, and FEF25–75% (p = 0.960, p = 1.000, p = 0.990, and p = 0.980, respectively; Figure S1).
In the Kaplan–Meier analysis, cumulative AE COPD and all-cause mortality were significantly higher in COPD with sarcopenia than COPD without sarcopenia (median follow-up 1305 and 2075 days, Figure 2A and Figure 2B, respectively).
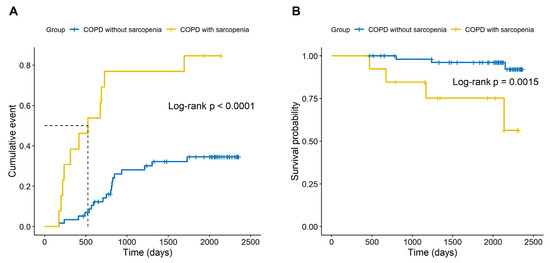
Figure 2.
Cumulative acute exacerbation events and all-cause mortality of chronic obstructive pulmonary disease. (A) Acute exacerbation of chronic obstructive pulmonary disease. (B) All-cause mortality in patients with chronic obstructive pulmonary disease.
In the Cox regression analysis for hazard ratios of AE COPD, statistically significant variables in the univariate analysis were pneumonia development per year (hazard ratio (HR) 2.430; 95% confidence interval [CI], 1.607–3.676, Table 3), fat-free mass index (HR 0.728; 95% CI, 0.541–0.979), ASMI (HR, 0.533; 95% CI, 0.298–0.952), hand grip strength (HR, 0.951; 95% CI, 0.917–0.988), and sarcopenia (HR, 5.311; 95% CI, 2.479–11.379). In the multivariate analysis, pneumonia development per year (HR, 2.094; 95% CI, 1.271–3.449), FEV1/FVC z-score (HR, 0.607; 95% CI, 0.427–0.864), and sarcopenia (HR, 5.982; 95% CI, 1.576–22.704) were identified as significant factors for AE COPD.
Table 3.
Cox regression analysis for hazard ratio of COPD acute exacerbations.
7. Correlations of HGS, SMMI, TSMI, and ASMI with Clinical Parameters in the Secondary Cross-Sectional Analysis
A total of 20 patients participated in secondary cross-sectional analysis (Supplementary Table S1). HGS was negatively correlated with age, CAT score change, and annual CCI score change (correlation coefficient [r] = −0.490, p = 0.028; r = −0.468, p = 0.038; and r = −0.473, p = 0.035; respectively; Table 4); moreover, it was positively correlated with BMI, total SMMI, and ASMI (r = 0.515, p = 0.020; r = 0.641, p = 0.003; and r = 0.645, p = 0.004, respectively).
Table 4.
Correlations of HGS, SMMI, TSMI, and ASMI with clinical parameters in the secondary cross-sectional analysis.
SMMI was negatively correlated with mMRC, CAT score, and BODE index (r = −0.515, p = 0.024; r = −0.482, p = 0.050; and r = −0.638, p = 0.003, respectively); further, it was positively correlated with BMI, FFMI, TSMI, ASMI, HGS, AST, and ALT (r = 0.852, p < 0.001; r = 0.992, p < 0.001; r = 0.763, p < 0.001; r = 0.895, p < 0.001; r = 0.641, p = 0.003; r = 0.543, p = 0.016; and r = 0.466, p = 0.044, respectively).
TSMI was negatively correlated with experience of AE COPD (r = −0.562, p = 0.019) and positively correlated with BMI, FFMI, SMMI, and AST (r = 0.483, p = 0.050; r = 0.715, p = 0.001; r = 0.763, p < 0.001; and r = 0.563, p = 0.019, respectively).
ASMI was negatively correlated with BODE index and ICU admissions per year (r = −0.648, p = 0.004 and r = −0.479, p = 0.044, respectively); furthermore, it was positively correlated with BMI, FFMI, FMI, SMMI, and HGS (r = 0.890, p < 0.001; r = 0.716, p = 0.001; r = 0.611, p = 0.009; r = 0.895, p < 0.001; and r = 0.645, p = 0.004, respectively).
8. Discussion
Sarcopenia was associated with all-cause mortality, COPD exacerbation, and pneumonia development in patients with COPD. These findings suggest the need for early sarcopenia identification; in addition, nutritional supplementation and exercise are recommended for patients with COPD.
According to the EWGSOP2 and AWGS 2019 guidelines, low muscle strength is a characteristic feature of sarcopenia. Muscle strength is measured using the HGS and chair stand tests, while muscle quantity/quality can be measured using DEXA or BIA. However, there is no specific screening protocol for sarcopenia in patients with COPD, especially Asian patients. Accordingly, there is a need to establish a specified cutoff value for Asian patients and determine the optimal period of sarcopenia screening in patients with COPD.
We designed the current study as a follow-up of our prior study [12]. For the definition of sarcopenia in the previous study, low muscle mass was defined as a skeletal muscle mass index (SMMI) at least two standard deviations below normal sex-specific means in young persons, and low muscle strength was defined as hand grip strength (HGS) values of ≤30 kg in men and ≤20 kg in women, according to the recommendation of the European Working Group on Sarcopenia in Older People (EWGSOP). However, in early 2018, the Working Group updated the original definition of sarcopenia with the EWGSOP2 definition, with a focus on low muscle strength as a key characteristic of sarcopenia. We assessed the clinical significance of HGS in patients with COPD. We observed a negative correlation between CAT score, annual CCI score changes and HGS. Similarly, Martinez et al. reported that a higher handgrip strength (HGS) is associated with a lower frequency of exacerbations in patients with COPD [16]. The identification of handgrip weakness is a straightforward measure that not only provides prognostic information but also complements known predictors such as the BODE index and BMI in assessments of patients with COPD [17]. Therefore, periodic HGS evaluation can be useful for the evaluation of sarcopenia and sarcopenia-related outcomes in COPD patients; however, further research is required.
The main parameter for muscle mass measurements in previous studies is ASMI [7,9,18,19]. We analyzed the association between muscle mass in each body part (total SMMI, TSMI, and ASMI) and clinical outcomes. There were strong correlations among the muscle mass parameters; however, they showed different associations with clinical outcomes. Specifically, TSMI showed a stronger association with COPD symptoms than ASMI, while ASMI showed a stronger association with BODE index and ICU admissions for AE COPD than TSMI. Additionally, total SMMI tended to better reflect various clinical outcomes than TSMI or ASMI. Therefore, total SMMI may be a better evaluation index for muscle mass in patients with COPD than ASMI; however, we conducted the study with a small sample size and, as this was a secondary study utilizing participants from the previous research, we did not perform a proper sample size evaluation. Therefore, further research with an appropriate sample size assessment is warranted.
Sarcopenia is correlated with mortality in the general population. Bachettini et al. reported that severe sarcopenia according to EWGSOP2 increased mortality in older people (hazard ratio 4.11, 95% confidence interval 1.88–9.00) [20]. Similarly, Miguel et al. showed a synergistic effect of sarcopenia and COPD on mortality in older patients with COPD [21]. Although we included a small sample size, the sarcopenia group showed a higher all-cause mortality rate than the non-sarcopenia group. Sarcopenia and HGS are associated with the frequency of AE COPD [2,22,23]. Perrot et al. reported that sarcopenia was highly prevalent among patients with COPD during an acute exacerbation (48%) and after recovery (30%) [2]. Lee et al. reported that HGS at admission for AE COPD was negatively associated with risk of exacerbation in the following year [23]. In our analysis, muscle mass and HGS were significant risk factors for AE COPD in the univariate analysis; however, their statistical significance diminished in the multivariate analysis. Interestingly, sarcopenia, a variable that considers both muscle mass and HGS, showed statistically significant results. This suggests the importance of evaluating sarcopenia in COPD patients by considering both muscle mass and hand grip strength, rather than considering each separately.
Sarcopenia is a risk factor for pneumonia in older people, and there is a relationship between respiratory muscle strength and pneumonia [24]. We observed no significant relationship between sarcopenia and experience of pneumonia; however, annual pneumonia development was higher in the sarcopenia group than in the non-sarcopenia group. Muscle strength and muscle mass were not significantly associated with annual pneumonia development, which could be attributed to our small sample size; further large-scale studies are warranted.
We found that ALT was significantly associated with sarcopenia and positively correlated with muscle mass. Several studies have reported a relationship between ALT and sarcopenia [25,26,27]. ALT levels are commonly used to evaluate liver disease; however, they can reflect skeletal muscle volume as ALT is also distributed in the heart, muscles, and kidney [28]. Accordingly, low ALT levels are associated with COPD development, acute exacerbations, and mortality [28,29]. Lasman et al. reported that low ALT levels are associated with mortality in patients with COPD with a history of exacerbation [29]. Taken together, these findings demonstrate the clinical utility of measuring ALT levels in patients with COPD.
In contrast to the results of previous studies [30,31], there were no significant between-group differences in baseline and annual changes in spirometry findings in the current study. Nathalie et al. described that FEV1 decreased more in patients with COPD who also had sarcopenia than in those without sarcopenia [30]. Park et al. reported that a decrease in MMI was significantly associated with accelerated FEV1 decline in men [31]. In the current study, we included only 71 patients with COPD and a follow-up period of less than 5 years, retrospectively. The small number of patients and short follow-up duration may have affected the result.
Recent studies also describe that chronic low-grade inflammation may play an important role in the development of sarcopenia. Byun et al. [12] and Gao et al. [32] reported that inflammatory markers, such as IL-6, hs-TNFα, and resistin, are associated with sarcopenia. These associations have been debated in several studies. Tang et al. did not support the utility of the inflammatory indexes, such as neutrophil, lymphocyte, monocyte, and platelet counts, and C-reactive protein (CRP) as biomarkers of sarcopenia [33]. Kamper et al. also reported that only high levels of hsCRP, but not TNF-α, IL-4, and IFN-γ, were weakly associated with low muscle mass [34]. The current study also did not show a significant association between the inflammatory markers CRP, IL-6, and hsTNF-α. Because inflammatory markers are affected by various factors, such as infections, diseases, and sarcopenia, different results can be reported depending on the patient’s accompanying conditions. Furthermore, this also suggests that chronic low-grade inflammation is not the main cause of sarcopenia.
A strength of our study is its long-term follow-up period (6 years) of patients with COPD and sarcopenia, which revealed a correlation between sarcopenia and all-cause mortality, COPD exacerbation, and pneumonia development. However, this study has several limitations. First, the sample size was small, which might have contributed to the lack of statistical significance for some findings. In addition, we did not conduct sample size calculations for the comparison of each variable. Consequently, this may have resulted in inadequate sample sizes for certain variables, potentially leading to an inability to achieve statistical significance. Second, clinical outcomes were evaluated through a retrospective review of electronic medical records, which could have resulted in biases. Third, the use of BIA measurements in the first cross-sectional study and DEXA measurements in the second cross-sectional study presents a limitation to the accurate evaluation of changes that occurred over the observation period.
In conclusion, sarcopenia is a common comorbidity that negatively affects clinical outcomes in patients with COPD. Specifically, sarcopenia is positively associated with all-cause mortality, acute exacerbations, and pneumonia occurrence in patients with COPD. These findings suggest the need for early sarcopenia identification, as well as recommending nutritional supplementation and exercise for patients with COPD. Moreover, protocols and guidelines for screening sarcopenia in patients with COPD may be required.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/life13081628/s1, Table S1: Baseline characteristics of participants in secondary cross-sectional analysis; Figure S1: Annual changes in spirometry findings
Author Contributions
Y.J.C. contributed to the conception and design of this study, analysed and interpreted the data, drafted and revised the article, and approved the final version of the article for publication. T.K., H.J.P. and J.H.C. collected, generated, and analysed the data, contributed to the draft, revised the article, and approved the final version of the article for publication. M.K.B., as the corresponding author, provided constructive criticism on the concept and design of this study, interpreted the data, drafted and revised the article, and approved the final version of the article for publication. All authors have read and agreed to the published version of the manuscript.
Funding
Sponsorship for this study was funded by the Handok Inc. Seoul, Korea (grant number: 3-2018-0109). The funders had no role in study design, data collection, analysis, decision to publish, and preparation of the manuscript.
Institutional Review Board Statement
This study was approved by the Institutional Review Board (IRB) of Gangnam Severance Hospital (number: 3-2018-0109).
Informed Consent Statement
Participants provided written informed consent to participate in the second cross-sectional study. And All data for the retrospective analysis of clinical outcomes were fully anonymized before being accessed, and the ethics committee waived the requirement for written informed consent because of the retrospective nature of this study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to no permission for data provision when IRB approval was obtained. Data can be made available from the first or corresponding author (contact: Yong Jun Choi or Min Kwang Byun, cyj0717@yuhs.ac or littmann@yuhs.ac, respectively) and IRB (gnocr@yuhs.ac) for re-searchers who meet the criteria for access to confidential data.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AE COPD | acute exacerbation of chronic obstructive pulmonary disease |
| ALT | alanine transaminase |
| ASMI | appendicular skeletal muscle mass index |
| AST | aspartate aminotransferase |
| AWGS | Asian Working Group for Sarcopenia |
| BIA | bioelectrical impedance analysis |
| BMI | body mass index |
| BODE | body mass index, airflow obstruction, dyspnea, and exercise |
| CAT | Chronic Obstructive Pulmonary Disease Assessment Test |
| CCI | Charlson’s comorbidity index |
| COPD | chronic obstructive pulmonary disease |
| DEXA | dual-energy X-ray absorptiometry |
| EWGSOP | European Working Group on Sarcopenia in Older People |
| EWGSOP2 | European Working Group on Sarcopenia in Older People of 2018 |
| FEF25–75% | forced mid-expiratory flow |
| FEV1 | Forced expiratory volume in the first second |
| FFM | fat-free mass |
| FFMI | fat-free mass index |
| FMI | fat mass index |
| FVC | forced vital capacity |
| GLI 2012 | Global Lung Function Initiative 2012 (GLI 2012) |
| HGS | handgrip strength |
| ICU | intensive care unit |
| mMRC | modified Medical Research Council |
| SMM | skeletal muscle mass |
| SMMI | skeletal muscle mass index |
| RM-ANOVA | repeated measures analysis of variance |
| TSMI | truncal skeletal muscle mass index |
References
- Rabe, K.F.; Watz, H. Chronic obstructive pulmonary disease. Lancet 2017, 389, 1931–1940. [Google Scholar] [CrossRef]
- Perrot, L.; Greil, A.; Boirie, Y.; Farigon, N.; Mulliez, A.; Costes, F.; Caillaud, D. Prevalence of sarcopenia and malnutrition during acute exacerbation of copd and after 6 months recovery. Eur. J. Clin. Nutr. 2020, 74, 1556–1564. [Google Scholar] [CrossRef]
- Costa, T.M.D.R.L.; Costa, F.M.; Moreira, C.A.; Rabelo, L.M.; Boguszewski, C.L.; Borba, V.Z.C. Sarcopenia in copd: Relationship with copd severity and prognosis. J. Bras. Pneumol. 2015, 41, 415–421. [Google Scholar] [CrossRef]
- Maltais, F.; Decramer, M.; Casaburi, R.; Barreiro, E.; Burelle, Y.; Debigaré, R.; Dekhuijzen, P.N.; Franssen, F.; Gayan-Ramirez, G.; Gea, J.; et al. An official american thoracic society/european respiratory society statement: Update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2014, 189, e15–e62. [Google Scholar] [CrossRef]
- Spruit, M.A.; Gosselink, R.; Troosters, T.; Kasran, A.; Gayan-Ramirez, G.; Bogaerts, P.; Bouillon, R.; Decramer, M. Muscle force during an acute exacerbation in hospitalised patients with copd and its relationship with cxcl8 and igf-i. Thorax 2003, 58, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised european consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global prevalence of sarcopenia and severe sarcopenia: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Benz, E.; Trajanoska, K.; Lahousse, L.; Schoufour, J.D.; Terzikhan, N.; De Roos, E.; de Jonge, G.B.; Williams, R.; Franco, O.H.; Brusselle, G.; et al. Sarcopenia in copd: A systematic review and meta-analysis. Eur. Respir. Rev. 2019, 28, 190049. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Osadnik, C.; Phu, S.; Morita, A.A.; Duque, G.; Probst, V.S. Diagnosis, prevalence, and clinical impact of sarcopenia in copd: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 1164–1176. [Google Scholar] [CrossRef]
- Gosker, H.R.; Langen, R.C.; Simons, S.O. Role of acute exacerbations in skeletal muscle impairment in copd. Expert Rev. Respir. Med. 2021, 15, 103–115. [Google Scholar] [CrossRef]
- Byun, M.K.; Cho, E.N.; Chang, J.; Ahn, C.M.; Kim, H.J. Sarcopenia correlates with systemic inflammation in copd. Int. J. Chron. Obs. Pulmon. Dis. 2017, 12, 669–675. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, G.; Ponti, F.; Agostini, M.; Amadori, M.; Battista, G.; Bazzocchi, A. The role of dxa in sarcopenia. Aging Clin. Exp. Res. 2016, 28, 1047–1060. [Google Scholar] [CrossRef]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef]
- Martinez, C.H.; Diaz, A.A.; Meldrum, C.A.; McDonald, M.N.; Murray, S.; Kinney, G.L.; Hokanson, J.E.; Curtis, J.L.; Bowler, R.P.; Han, M.K.; et al. Handgrip strength in chronic obstructive pulmonary disease. Associations with acute exacerbations and body composition. Ann. Am. Thorac. Soc. 2017, 14, 1638–1645. [Google Scholar] [CrossRef]
- Burtin, C.; Ter Riet, G.; Puhan, M.A.; Waschki, B.; Garcia-Aymerich, J.; Pinto-Plata, V.; Celli, B.; Watz, H.; Spruit, M.A. Handgrip weakness and mortality risk in copd: A multicentre analysis. Thorax 2016, 71, 86–87. [Google Scholar] [CrossRef]
- Wallengren, O.; Bosaeus, I.; Frändin, K.; Lissner, L.; Falk Erhag, H.; Wetterberg, H.; Rydberg Sterner, T.; Rydén, L.; Rothenberg, E.; Skoog, I. Comparison of the 2010 and 2019 diagnostic criteria for sarcopenia by the european working group on sarcopenia in older people (ewgsop) in two cohorts of swedish older adults. BMC Geriatr. 2021, 21, 600. [Google Scholar] [CrossRef] [PubMed]
- Limpawattana, P.; Inthasuwan, P.; Putraveephong, S.; Boonsawat, W.; Theerakulpisut, D.; Sawanyawisuth, K. Sarcopenia in chronic obstructive pulmonary disease: A study of prevalence and associated factors in the southeast asian population. Chron. Respir. Dis. 2018, 15, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Bachettini, N.P.; Bielemann, R.M.; Barbosa-Silva, T.G.; Menezes, A.M.B.; Tomasi, E.; Gonzalez, M.C. Sarcopenia as a mortality predictor in community-dwelling older adults: A comparison of the diagnostic criteria of the european working group on sarcopenia in older people. Eur. J. Clin. Nutr. 2020, 74, 573–580. [Google Scholar] [CrossRef]
- Borda, M.; Patino-Hernandez, D.; Celis, C.; Cano, C.; Perez-Zepeda, M. Sarcopenia, lung disease and mortality: A secondary analysis of the creles study. Geriatr. Gerontol. Aging 2019, 13, 36–38. [Google Scholar] [CrossRef]
- Abdulai, R.M.; Jensen, T.J.; Patel, N.R.; Polkey, M.I.; Jansson, P.; Celli, B.R.; Rennard, S.I. Deterioration of limb muscle function during acute exacerbation of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2017, 197, 433–449. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.T.; Wang, P.H. Handgrip strength during admission for copd exacerbation: Impact on further exacerbation risk. BMC Pulm. Med. 2021, 21, 245. [Google Scholar] [CrossRef]
- Okazaki, T.; Ebihara, S.; Mori, T.; Izumi, S.; Ebihara, T. Association between sarcopenia and pneumonia in older people. Geriatr. Gerontol. Int. 2020, 20, 7–13. [Google Scholar] [CrossRef]
- Vespasiani-Gentilucci, U.; De Vincentis, A.; Ferrucci, L.; Bandinelli, S.; Antonelli Incalzi, R.; Picardi, A. Low alanine aminotransferase levels in the elderly population: Frailty, disability, sarcopenia, and reduced survival. J. Gerontol. A Biol. Sci. Med Sci. 2018, 73, 925–930. [Google Scholar] [CrossRef]
- Gallo, P.; De Vincentis, A.; Bandinelli, S.; Ferrucci, L.; Picardi, A.; Antonelli Incalzi, R.; Vespasiani-Gentilucci, U. Combined evaluation of aminotransferases improves risk stratification for overall and cause-specific mortality in older patients. Aging Clin. Exp. Res. 2021, 33, 3321–3331. [Google Scholar] [CrossRef]
- He, Y.; Ding, F.; Yin, M.; Zhang, H.; Hou, L.; Cui, T.; Xu, J.; Yue, J.; Zheng, Q. High serum ast/alt ratio and low serum ins*pa product are risk factors and can diagnose sarcopenia in middle-aged and older adults. Front. Endocrinol. 2022, 13, 843610. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Kwon, D.S.; Kim, T.; Cho, J.H.; Kim, H.J.; Byun, M.K.; Park, H.J. Low alanine aminotransferase as a risk factor for chronic obstructive pulmonary disease in males. Sci. Rep. 2021, 11, 14829. [Google Scholar] [CrossRef]
- Lasman, N.; Shalom, M.; Turpashvili, N.; Goldhaber, G.; Lifshitz, Y.; Leibowitz, E.; Berger, G.; Saltzman-Shenhav, G.; Brom, A.; Cohen, D.; et al. Baseline low alt activity is associated with increased long-term mortality after copd exacerbations. BMC Pulm. Med. 2020, 20, 133. [Google Scholar] [CrossRef]
- Martínez-Luna, N.; Orea-Tejeda, A.; González-Islas, D.; Flores-Cisneros, L.; Keirns-Davis, C.; Sánchez-Santillán, R.; Pérez-García, I.; Gastelum-Ayala, Y.; Martínez-Vázquez, V.; Martínez-Reyna, Ó. Association between body composition, sarcopenia and pulmonary function in chronic obstructive pulmonary disease. BMC Pulm. Med. 2022, 22, 106. [Google Scholar] [CrossRef]
- Park, H.K.; Lee, S.H.; Lee, S.Y.; Kim, S.S.; Park, H.W. Relationships between lung function decline and skeletal muscle and fat mass changes: A longitudinal study in healthy individuals. J. Cachexia Sarcopenia Muscle 2021, 12, 2145–2153. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Deng, M.; Li, Y.; Yin, Y.; Zhou, X.; Zhang, Q.; Hou, G. Resistin as a systemic inflammation-related biomarker for sarcopenia in patients with chronic obstructive pulmonary disease. Front. Nutr. 2022, 9, 921399. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.; Xie, L.; Tan, L.; Hu, X.; Yang, M. Inflammatory indexes are not associated with sarcopenia in chinese community-dwelling older people: A cross-sectional study. BMC Geriatr. 2020, 20, 457. [Google Scholar] [CrossRef]
- Kamper, R.S.; Alcazar, J.; Andersen, L.L.; Haddock, B.; Jørgensen, N.R.; Hovind, P.; Suetta, C. Associations between inflammatory markers, body composition, and physical function: The copenhagen sarcopenia study. J. Cachexia Sarcopenia Muscle 2021, 12, 1641–1652. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).