
Current Trends in Stroke Biomarkers: The Prognostic Role of S100B and GFAP

 , , ,
, , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Biomarkers
3. Methods
3.1. Search Strategy
3.2. Study Selection—Eligibility Criteria
4. The Contribution of S100B (Table 1) and GFAP (Table 2)
4.1. S100B Contribution

| No. | Author/Ref. Number | Title | Year | N | Study Design | Stroke Subtypes | Results |
|---|---|---|---|---|---|---|---|
| 1 | Foerch et al. [24] | Elevated serum S100B levels indicate a higher risk of hemorrhagic transformation after thrombolytic therapy in acute stroke | 2007 | 275 | Retrospective study | IS | -Serum S100B values were significantly higher in patients with hemorrhagic transformation compared to patients without |
| 2 | J. Montaner et al. [25] | A panel of biomarkers including caspase-3 and D-dimer may differentiate acute stroke from stroke-mimicking conditions in the emergency department | 2010 | 915 strokes and 90 mimics | Single-center, prospective observational study | IS and ICH | -S100B play a role for distinguishing ischaemic from haemorrhagic stroke |
| 3 | Knauer et al. [26] | A biochemical marker panel in MRI-proven hyperacute ischemic stroke-a prospective study | 2012 | 174 | Prospective cohort study | IS | -Approximately 98% of the patients did not reach the lower limit of the testing range for S100B |
| 4 | Selçuk et al. [27] | The Relationship of Serum S100B Levels with Infarction Size and Clinical Outcome in Acute Ischemic Stroke Patients | 2014 | 50 patients, 26 controls | Prospective, case-control study | IS | -S100B levels showed significantly higher values than the control group -Alteration of S100B levels did not show any significant differences between the 1st to 3rd days and the 1st to 5th days, but were significantly higher on the 3rd day compared to the 5th day -S100B levels were correlated with infarct volume, especially on the 3rd day -Weak correlation between the first month mRS score and S100B levels of the 3rd day -no significant relationship between the concurrent NIHS scores and S100B levels |
| 5 | Deboevere et al. [28] | Value of copeptin and the S-100b protein assay in ruling out the diagnosis of stroke-induced dizziness pattern in emergency departments | 2019 | 135 | Single-center, prospective, observational study | N/A | -S100 levels above normal values were more frequent in patients with stroke than in those without. -Absence of S100 elevation seems to rule out the diagnosis of stroke |
| 6 | Garzelli et al. [29] | Secondary S100B Protein Increase Following Brain Arteriovenous Malformation Rupture is Associated with Cerebral Infarction | 2020 | 216 patients | Single-center, retrospective study | IS | -Secondary S100B protein serum elevation was found in 17.1% of ruptures and was associated with secondary infarction, vasospasm-related infarction, intensive care, and hospital length of stay, but not with early re-bleeding or in-hospital mortality |
| 7 | Iwamoto et al. [30] | Predicting hemorrhagic transformation after large vessel occlusion stroke in the era of mechanical thrombectomy | 2021 | 91 | Single-center, prospective, observational study | IS | -S100B levels were not associated with the development of relevant hemorrhagic transformation, with neurological deterioration/functional outcomes, or with parenchymal hematoma |
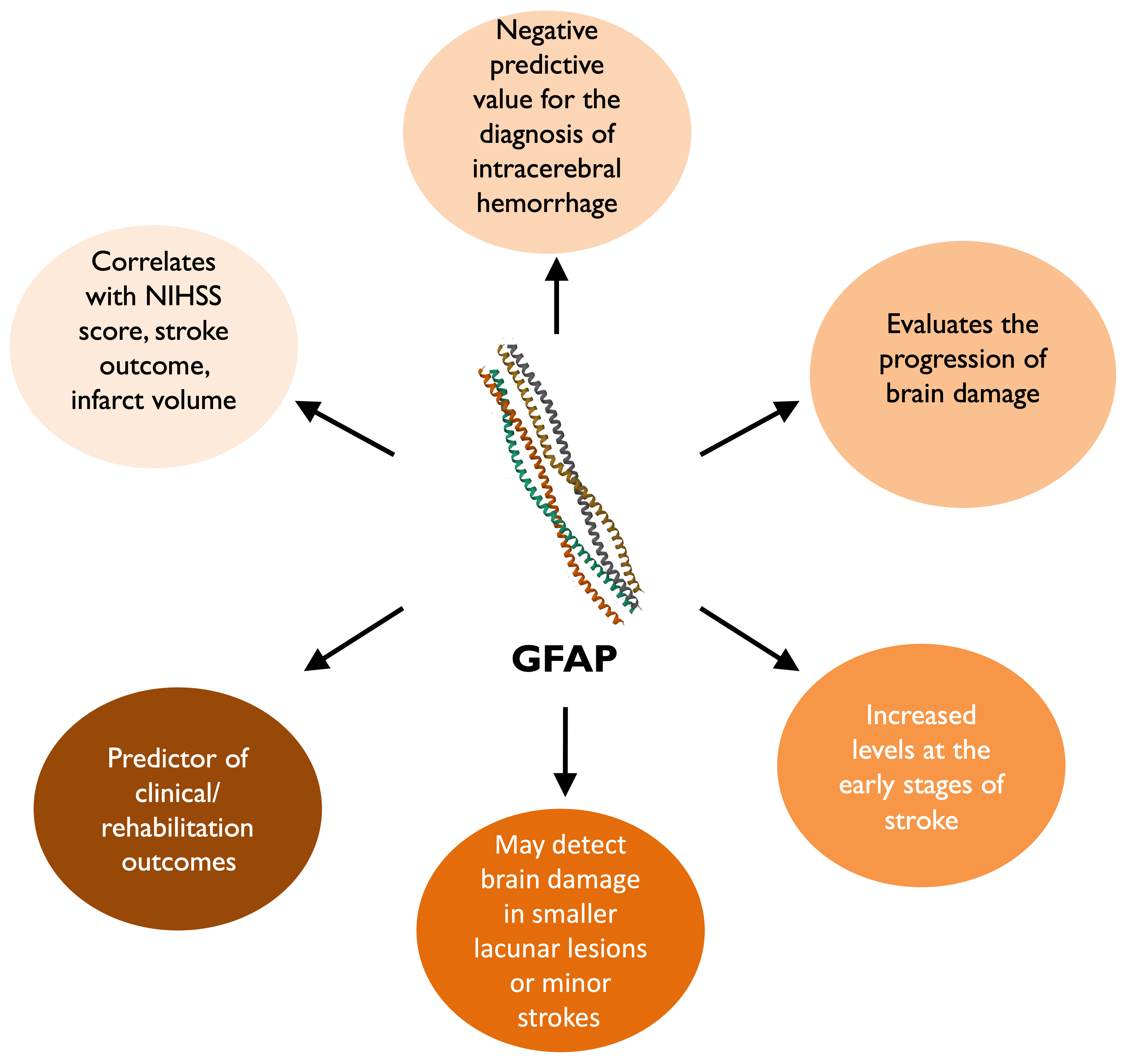
4.2. GFAP Contribution
| No. | Author/Ref. Number | Title (GFAP) | Year | N | Study Design | Stroke Subtypes | Results |
|---|---|---|---|---|---|---|---|
| 1 | Herrmann et al. [41] | Release of glial tissue-specific proteins after acute stroke: A comparative analysis of serum concentrations of protein S-100B and glial fibrillary acidic protein | 2000 | 32 | Cross-sectional study | IS | -GFAP was associated with the volume of brain lesions and the neurological status at discharge from the hospital -GFAP was found to be a more sensitive marker of brain damage in patients with smaller lacunar lesions or minor strokes |
| 2 | Ehrenreich et al. [46] | Circulating damage marker profiles support a neuroprotective effect of erythropoietin in ischemic stroke patients | 2011 | 163 | Randomized Controlled Trial | IS | -EPO-treated patients had significantly lower concentrations over 7 days of observation, as reflected by the composite score of all three markers and by UCH-L1. S100B and GFAP showed a similar tendency. |
| 3 | Bhatia et al. [37] | Role of Blood Biomarkers in Differentiating Ischemic Stroke and Intracerebral Hemorrhage | 2020 | 250 | Cross-sectional | 187 IS, 63 ICH | -GFAP showed low overall discriminatory ability with an AUC of 56% |
| 4 | Misra et al. [48] | Blood biomarkers for the diagnosis and differentiation of stroke: A systematic review and meta-analysis | 2020 | 8085 | Meta-analysis | 5001 IS, 756 ICH | -GFAP successfully differentiated ischemic stroke from intracerebral hemorrhage within 6 h. |
| 5 | O’Connell et al. [36] | Newly identified blood biomarkers of neurological damage are correlated with infarct volume in patients with acute ischemic stroke | 2021 | 43 | Cross-sectional | IS | -Correlation of GFAP with infarct volume |
| 6 | Correia et al. [49] | Early plasma biomarker dynamic profiles are associated with acute ischemic stroke outcomes | 2022 | 54 | Cross-sectional | IS | -GFAP levels exhibited an early and prominent increase between admission and just after treatment. -GFAP rate-of-change between admission and immediately after recanalization had a good discriminative capacity between clinical outcomes. -In patients with admission CT-ASPECTS <9, GFAP rate-of-change was good outcome predictor |
| 7 | Sayad et al. [21] | A magnetoimpedance biosensor microfluidic platform for detection of glial fibrillary acidic protein in blood for acute stroke classification | 2022 | 52 | Technical paper (method for GFAP detection in biofluids) | - | -Detection of recombinant GFAP protein in phosphate-buffered saline and in mouse blood samples (detection limit 0.01 ng/mL) and of physiological GFAP in blood and plasma samples (detection limit 1.0 ng/mL) obtained from acute stroke patients |
| 8 | Pujol-Calderón et al. [43] | Prediction of Outcome After Endovascular Embolectomy in Anterior Circulation Stroke Using Biomarkers | 2022 | 90 | Longitudinal observational study | IS | -At 3 months, GFAP levels were back to normal. -GFAP correlated well to outcome, as well as to infarct volume and NIHSS at 24 h. -The combination of NIHSS at 24 h with either tau, NFL or GFAP at 48 h gave the best poor outcome prediction. |
| 9 | Ferrari et al. [47] | Quantification and prospective evaluation of serum NfL and GFAP as blood-derived biomarkers of outcome in acute ischemic stroke patients | 2023 | 36 | Longitudinal observational study | IS | -GFAP showed an earlier peak on first day after stroke -GFAP correlated with clinical/rehabilitation outcomes both longitudinally and prospectively. -Multivariate analysis revealed that GFAP on the first day was an independent predictor of 3-month NIHSS, TCT, FAC and FIM scores |
| 10 | Florijn et al. [50] | Non-coding RNAs versus protein biomarkers to diagnose and differentiate acute stroke: Systematic review and meta-analysis | 2023 | 20,678 | Meta-analysis | 11,627 IS, 2110 ICH | -Circulating microRNAs and proteins perform equally well in the diagnosis of ischemic stroke -GFAP differentiated subtypes of stroke -A biomarker panel of GFAP and UCH-L1 improved the sensitivity and specificity of UCH-L1 alone to differentiate stroke. |
5. Discussion
5.1. Single Biomarkers and Criteria of Patient Progression
5.2. The Role of S100B
5.2.1. S100B Role in Inflammation and IS/ICH Differentiation
5.2.2. The Prognostic Role of S100B
5.3. GFAP Role in Differentiation between Stroke Subtypes and Differentiation
The Prognostic Role of GFAP and Neurological Status
5.4. Limitations
5.5. Biomarker Panels and Future Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| IS | Ischemic Stroke |
| SNV | selective neuronal vulnerability |
| MBP | Myelin basic protein |
| MT-3 | Metallothionein isoform 3 |
| CSF | Cerebrospinal Fluid |
| EPO | Erythropoietin |
| MMP-9 | Matrix Metalloproteinase-9 |
| AIS | Acute Ischemic Stroke |
| ICH | Intracranial Hemorrhage |
| S100B | S100 calcium-binding protein b |
| GFAP | Glial Fibrillary Acidic Protein |
| DAMP | Damage-Associated Molecular Pattern |
References
- Feigin, V.L.; A Stark, B.; Johnson, C.O.; A Roth, G.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Hreha, K.; Wong, J.; Molton, I.; Nelson, I.K.; Lee, D. The impact of stroke on psychological and physical function outcomes in people with long-term physical disability. Disabil. Health J. 2020, 13, 100919. [Google Scholar] [CrossRef]
- Kabat, H.; Anderson, J.P. Acute arrest of cerebral circulation in man. Arch. Neurol. Psychiatry 1943, 50, 510–528. [Google Scholar] [CrossRef]
- Hara, H.; Sukamoto, T.; Kogure, K. Mechanism and pathogenesis of ischemia-induced neuronal damage. Prog. Neurobiol. 1993, 40, 645–670. [Google Scholar] [CrossRef] [PubMed]
- Lipton, P. Ischemic cell death in brain neurons. Physiol. Rev. 1999, 79, 1431–1568. [Google Scholar] [CrossRef]
- Kandel, E.R.; Schwartz, J.H. Principles of Neural Science, 2nd ed.; Elsevier: New York, NY, USA, 1985. [Google Scholar]
- Barrett, L.F. Seven and a Half Lessons about the Brain; Houghton Mifflin Harcourt: Boston, MA, USA, 2020. [Google Scholar]
- Schmidt-Kastner, R.; Freund, T. Selective vulnerability of the hippocampus in brain ischemia. Neuroscience 1991, 40, 599–636. [Google Scholar] [CrossRef] [PubMed]
- Olsson, T.; Wieloch, T.; Smith, M.-L. Brain damage in a mouse model of global cerebral ischemia. Effect of NMDA receptor blockade. Brain Res. 2003, 982, 260–269. [Google Scholar]
- Mathern, G.W.; Kuhlman, P.A.; Mendoza, D.; Pretorius, J.K. Human fascia dentata anatomy and hippocampal neuron densities differ depending on the epileptic syndrome and age at first seizure. J. Neuropathol. Exp. Neurol. 1997, 56, 199–212. [Google Scholar] [CrossRef]
- Wilde, G.J.C.; Pringle, A.K.; Wright, P.; Iannotti, F. Differential vulnerability of the CA1 and CA3 subfields of the hippocampus to superoxide and hydroxyl radicals in vitro. J. Neurochem. 1997, 69, 883–886. [Google Scholar] [CrossRef]
- Terraneo, L.; Paroni, R.; Bianciardi, P.; Giallongo, T.; Carelli, S.; Gorio, A.; Samaja, M. Brain adaptation to hypoxia and hyperoxia in mice. Redox Biol. 2017, 11, 12–20. [Google Scholar] [CrossRef]
- Gibson, G.E.; Toral-Barza, L.; Manger, T.; Freeman, G. Neurotransmitters and Calcium during Hypoxia. In Cerebral Ischemia and Calcium; Hartmann, A., Kuschinsky, W., Eds.; Springer: Berlin/Heidelberg, Germany, 1989. [Google Scholar] [CrossRef]
- Görlach, A. Control of adenosine transport by hypoxia. Circ. Res. 2005, 97, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Poyton, R.O.; Ball, K.A.; Castello, P.R. Mitochondrial generation of free radicals and hypoxic signaling. Trends Endocrinol. Metab. 2009, 20, 332–340. [Google Scholar] [CrossRef]
- Whiteley, W.; Tian, Y.; Jickling, G.C. Blood biomarkers in stroke: Research and clinical practice. Int. J. Stroke 2012, 7, 435–439. [Google Scholar] [CrossRef]
- Geiger, S.; Holdenrieder, S.; Stieber, P.; Hamann, G.F.; Bruening, R.; Ma, J.; Nagel, D.; Seidel, D. Nucleosomes as a new prognostic marker in early cerebral stroke. J. Neurol. 2007, 254, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Zhang, X.; Peng, S.; Sun, J.; Chen, X.; Deng, Y.; Yi, L. Identification of novel biomarkers in ischemic stroke: A genome-wide integrated analysis. BMC Med Genet. 2020, 21, 66. [Google Scholar] [CrossRef] [PubMed]
- Gayger-Dias, V.; Vizuete, A.F.; Rodrigues, L.; Wartchow, K.M.; Bobermin, L.; Leite, M.C.; Quincozes-Santos, A.; Kleindienst, A.; Gonçalves, C.-A. How S100B crosses brain barriers and why it is considered a peripheral marker of brain injury. Exp. Biol. Med. 2023, 248, 2109–2119. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, H.; Wang, Y.; Zhang, D.; Li, P. Circulating nucleosomes as potential biomarkers for cancer diagnosis and treatment monitoring. Int. J. Biol. Macromol. 2024, 262 Pt 1, 130005. [Google Scholar] [CrossRef] [PubMed]
- Sayad, A.; Uddin, S.M.; Yao, S.; Wilson, H.; Chan, J.; Zhao, H.; Donnan, G.; Davis, S.; Skafidas, E.; Yan, B.; et al. A magnetoimpedance biosensor microfluidic platform for detection of glial fibrillary acidic protein in blood for acute stroke classification. Biosens. Bioelectron. 2022, 211, 114410. [Google Scholar] [CrossRef]
- Hill, M.D.; Jackowski, G.; Bayer, N.; Lawrence, M.; Jaeschke, R. Biochemical markers in acute ischemic stroke. CMAJ 2000, 162, 1139–1140. [Google Scholar] [PubMed]
- Ostendorp, T.; Diez, J.; Heizmann, C.W.; Fritz, G. The crystal structures of human S100B in the zinc- and calcium-loaded state at three pH values reveal zinc ligand swapping. Biochim. Biophys. Acta 2011, 1813, 1083–1091. [Google Scholar] [CrossRef]
- Foerch, C.; Wunderlich, M.T.; Dvorak, F.; Humpich, M.; Kahles, T.; Goertler, M.; Alvarez-Sabín, J.; Wallesch, C.W.; Molina, C.A.; Steinmetz, H.; et al. Elevated serum S100B levels indicate a higher risk of hemorrhagic transformation after thrombolytic therapy in acute stroke. Stroke 2007, 38, 2491–2495. [Google Scholar] [CrossRef] [PubMed]
- Montaner, J.; Mendioroz, M.; Ribó, M.; Delgado, P.; Quintana, M.; Penalba, A.; Chacón, P.; Molina, C.; Fernández-Cadenas, I.; Rosell, A.; et al. A panel of biomarkers including caspase-3 and D-dimer may differentiate acute stroke from stroke-mimicking conditions in the emergency department. J. Intern. Med. 2011, 270, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Knauer, C.; Knauer, K.; Müller, S.; Ludolph, A.C.; Bengel, D.; Müller, H.P.; Huber, R. A biochemical marker panel in MRI-proven hyperacute ischemic stroke-a prospective study. BMC Neurol. 2012, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Selcuk, O.; Yayla, V.; Cabalar, M.; Guzel, V.; Uysal, S.; Gedikbasi, A. The Relationship of Serum S100B Levels with Infarction Size and Clinical Outcome in Acute Ischemic Stroke Patients. Noro Psikiyatr. Arsivi 2014, 51, 395–400. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Deboevere, N.; Marjanovic, N.; Sierecki, M.; Marchetti, M.; Dubocage, M.; Magimel, E.; Mimoz, O.; Guenezan, J. Value of copeptin and the S-100b protein assay in ruling out the diagnosis of stroke-induced dizziness pattern in emergency departments. Scand. J. Trauma, Resusc. Emerg. Med. 2019, 27, 72. [Google Scholar] [CrossRef]
- Garzelli, L.; Jacquens, A.; Amouyal, C.; Premat, K.; Sourour, N.; Cortese, J.; Haffaf, I.; Mathon, B.; Lenck, S.; Clarençon, F.; et al. Secondary S100B Protein Increase Following Brain Arteriovenous Malformation Rupture is Associated with Cerebral Infarction. Molecules 2020, 25, 5177. [Google Scholar] [CrossRef]
- Iwamoto, T.; Kitano, T.; Oyama, N.; Yagita, Y. Predicting hemorrhagic transformation after large vessel occlusion stroke in the era of mechanical thrombectomy. PLoS ONE 2021, 16, e0256170. [Google Scholar] [CrossRef]
- Foerch, C.; Otto, B.; Singer, O.C.; Neumann-Haefelin, T.; Yan, B.; Berkefeld, J.; Steinmetz, H.; Sitzer, M. Serum S100B predicts a malignant course of infarction in patients with acute middle cerebral artery occlusion. Stroke 2004, 35, 2160–2164. [Google Scholar] [CrossRef]
- Wunderlich, M.T.; Ebert, A.D.; Kratz, T.; Goertler, M.; Jost, S.; Herrmann, M. Early neurobehavioral outcome after stroke is related to release of neurobiochemical markers of brain damage. Stroke 1999, 30, 1190–1195. [Google Scholar] [CrossRef]
- Michetti, F.; D’Ambrosi, N.; Toesca, A.; Puglisi, M.A.; Serrano, A.; Marchese, E.; Corvino, V.; Geloso, M.C. The S100B story: From biomarker to active factor in neural injury. J. Neurochem. 2018, 148, 168–187. [Google Scholar] [CrossRef]
- Michetti, F.; Clementi, M.E.; Di Liddo, R.; Valeriani, F.; Ria, F.; Rende, M.; Di Sante, G.; Spica, V.R. The S100B Protein: A Multifaceted Pathogenic Factor More Than a Biomarker. Int. J. Mol. Sci. 2023, 24, 9605. [Google Scholar] [CrossRef] [PubMed]
- Honegger, T.; Schweizer, J.; Bicvic, A.; Westphal, L.P.; Schütz, V.; Inauen, C.; Pokorny, T.; Bracher, K.; Arnold, M.; Fischer, U.; et al. Serum S-100B adds incremental value for the prediction of symptomatic intracranial hemorrhage and brain edema after acute ischemic stroke. Eur. Stroke J. 2022, 8, 309–319. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- O’Connell, G.C.; Smothers, C.G.; Gandhi, S.A. Newly-identified blood biomarkers of neurological damage are correlated with infarct volume in patients with acute ischemic stroke. J. Clin. Neurosci. 2021, 94, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, R.; Warrier, A.R.; Sreenivas, V.; Bali, P.; Sisodia, P.; Gupta, A.; Singh, N.; Srivastava, M.P.; Prasad, K. Role of Blood Biomarkers in Differentiating Ischemic Stroke and Intracerebral Hemorrhage. Neurol. India 2020, 68, 824–829. [Google Scholar] [CrossRef] [PubMed]
- Purroy, F.; Farré-Rodriguez, J.; Mauri-Capdevila, G.; Vicente-Pascual, M.; Farré, J. Basal IL-6 and S100B levels are associated with infarct volume. Acta Neurol. Scand. 2021, 144, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Luger, S.; Koerbel, K.; Oeckel, A.M.; Schneider, H.; Maurer, C.J.; Hintereder, G.; Wagner, M.; Hattingen, E.; Foerch, C. Role of S100B serum concentration as a surrogate outcome parameter after mechanical thrombectomy. Neurology 2021, 97, e2185–e2194. [Google Scholar] [CrossRef]
- Amalia, L. Glial Fibrillary Acidic Protein (GFAP): Neuroinflammation Biomarker in Acute Ischemic Stroke. J. Inflamm. Res. 2021, 14, 7501–7506. [Google Scholar] [CrossRef]
- Herrmann, M.; Vos, P.; Wunderlich, M.T.; de Bruijn, C.H.M.M.; Lamers, K.J.B. Release of glial tissue-specific proteins after acute stroke: A comparative analysis of serum concentrations of protein S-100B and glial fibrillary acidic protein. Stroke 2000, 31, 2670–2677. [Google Scholar] [CrossRef]
- Kim, B.; Kim, S.; Jin, M.S. Crystal structure of the human glial fibrillary acidic protein 1B domain. Biochem Biophys Res Commun. 2018, 503, 2899–2905. [Google Scholar] [CrossRef] [PubMed]
- Pujol-Calderón, F.; Zetterberg, H.; Portelius, E.; Hendén, P.L.; Rentzos, A.; Karlsson, J.-E.; Höglund, K.; Blennow, K.; Rosengren, L.E. Prediction of Outcome After Endovascular Embolectomy in Anterior Circulation Stroke Using Biomarkers. Transl. Stroke Res. 2022, 13, 65–76. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hu, C.; Yang, X.; Mao, D.; Lou, S.; Dai, Q.; Chen, J.; Cheng, X.; Wang, S. Expression levels of ubiquitin C-terminal hydrolase-L1 and serum glial fibrillary acidic protein and its clinical significance in patients with acute cerebral infarction. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2017, 42, 284–290. [Google Scholar] [PubMed]
- Surjawan, Y.; As’Ad, S.; Ranakusuma, T.A.S.; Wijaya, A. GFAP and S100B Protein are Associated with Discharged NIHSS of Anterior Circulation Ischemic Stroke. Indones. Biomed. J. 2012, 4, 112. [Google Scholar] [CrossRef]
- Ehrenreich, H.; Kästner, A.; Weissenborn, K.; Streeter, J.; Sperling, S.; Wang, K.K.; Worthmann, H.; Hayes, R.L.; von Ahsen, N.; Kastrup, A.; et al. Circulating damage marker profiles support a neuroprotective effect of erythropoietin in ischemic stroke patients. Mol. Med. 2011, 17, 1306–1310. [Google Scholar] [CrossRef]
- Ferrari, F.; Rossi, D.; Ricciardi, A.; Morasso, C.; Brambilla, L.; Albasini, S.; Vanna, R.; Fassio, C.; Begenisic, T.; Loi, M.; et al. Quantification and prospective evaluation of serum NfL and GFAP as blood-derived biomarkers of outcome in acute ischemic stroke patients. J. Cereb. Blood Flow Metab. 2023, 43, 1601–1611. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Montaner, J.; Ramiro, L.; Arora, R.; Talwar, P.; Nath, M.; Kumar, A.; Kumar, P.; Pandit, A.K.; Mohania, D.; et al. Blood biomarkers for the diagnosis and differentiation of stroke: A systematic review and meta-analysis. Int. J. Stroke 2020, 15, 704–721. [Google Scholar] [CrossRef]
- Correia, M.; Silva, I.; Gabriel, D.; Simrén, J.; Carneiro, A.; Ribeiro, S.; Dória, H.M.; Varela, R.; Aires, A.; Minta, K.; et al. Early plasma biomarker dynamic profiles are associated with acute ischemic stroke outcomes. Eur. J. Neurol. 2022, 29, 1630–1642. [Google Scholar] [CrossRef]
- Florijn, B.W.; van der Bent, M.L.; Nguyen, T.M.T.; Quax, P.H.; Wermer, M.J.; Nossent, A.Y.; Kruyt, N.D. Non-coding RNAs versus protein biomarkers to diagnose and differentiate acute stroke: Systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 2023, 32, 107388. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Misra, S.; Yadav, A.K.; Sagar, R.; Verma, B.; Grover, A.; Prasad, K. Role of glial fibrillary acidic protein as a biomarker in differentiating intracerebral haemorrhage from ischaemic stroke and stroke mimics: A meta-analysis. Biomarkers 2020, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Aurell, A.; E Rosengren, L.; Karlsson, B.; E Olsson, J.; Zbornikova, V.; Haglid, K.G. Determination of S-100 and glial fibrillary acidic protein concentrations in cerebrospinal fluid after brain infarction. Stroke 1991, 22, 1254–1258. [Google Scholar] [CrossRef]
- Pop, N.O.; Tit, D.M.; Diaconu, C.C.; Munteanu, M.A.; Babes, E.E.; Stoicescu, M.; Popescu, M.I.; Bungau, S. The Alberta Stroke Program Early CT score (ASPECTS): A predictor of mortality in acute ischemic stroke. Exp. Ther. Med. 2021, 22, 1371. [Google Scholar] [CrossRef]
- Quinn, T.J.; Dawson, J.; Walters, M.R.; Lees, K.R. Functional outcome measures in contemporary stroke trials. Int. J. Stroke 2009, 4, 200–205. [Google Scholar] [CrossRef] [PubMed]
- De Marchis, G.M.; Dankowski, T.; König, I.R.; Fladt, J.; Fluri, F.; Gensicke, H.; Foerch, C.; Findling, O.; Kurmann, R.; Fischer, U.; et al. A novel biomarker-based prognostic score in acute ischemic stroke: The CoRisk score. Neurology 2019, 92, e1517–e1525. [Google Scholar] [CrossRef] [PubMed]
- Kattah, J.C.; Talkad, A.V.; Wang, D.Z.; Hsieh, Y.-H. HINTS to diagnose stroke in the acute vestibular syndrome: Three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke 2009, 40, 3504–3510. [Google Scholar] [CrossRef] [PubMed]
- Broderick, J.P.; Adeoye, O.; Elm, J. Evolution of the Modified Rankin Scale and Its Use in Future Stroke Trials. Stroke 2017, 48, 2007–2012. [Google Scholar] [CrossRef]
- Lyden, P.; Raman, R.; Liu, L.; Emr, M.; Warren, M.; Marler, J. National Institutes of Health Stroke Scale certification is reliable across multiple venues. Stroke 2009, 40, 2507–2511. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, A.; Zhao, X.; Wang, C.; Liu, L.; Zheng, H.; Wang, Y.; Cao, Y.; Wang, Y. The Oxfordshire Community Stroke Project classification system predicts clinical outcomes following intravenous thrombolysis: A prospective cohort study. Ther. Clin. Risk Manag. 2016, 12, 1049–1056. [Google Scholar] [CrossRef]
- Gude, M.F.; Blauenfeldt, R.A.; Behrndtz, A.B.; Nielsen, C.N.; Speiser, L.; Simonsen, C.Z.; Johnsen, S.P.; Kirkegaard, H.; Andersen, G. The Prehospital Stroke Score and telephone conference: A prospective validation. Acta Neurol. Scand. 2022, 145, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar]
- Jadav, R.K.; Mortazavi, R.; Yee, K.C. Blood Biomarkers for Triaging Patients for Suspected Stroke: Every Minute Counts. J. Clin. Med. 2022, 11, 4243. [Google Scholar] [CrossRef]
- Montellano, F.A.; Ungethüm, K.; Ramiro, L.; Nacu, A.; Hellwig, S.; Fluri, F.; Whiteley, W.N.; Bustamante, A.; Montaner, J.; Heuschmann, P.U. Role of Blood-Based Biomarkers in Ischemic Stroke Prognosis: A Systematic Review. Stroke 2021, 52, 543–551, Erratum in: Stroke 2021, 52, e106. [Google Scholar] [CrossRef] [PubMed]
- di Biase, L.; Bonura, A.; Pecoraro, P.M.; Carbone, S.P.; Di Lazzaro, V. Unlocking the Potential of Stroke Blood Biomarkers: Early Diagnosis, Ischemic vs. Haemorrhagic Differentiation and Haemorrhagic Transformation Risk: A Comprehensive Review. Int. J. Mol. Sci. 2023, 24, 11545. [Google Scholar] [CrossRef] [PubMed]
- Serena, J.; Blanco, M.; Castellanos, M.; Silva, Y.; Vivancos, J.; Moro, M.A.; Leira, R.; Lizasoain, I.; Castillo, J.; Dávalos, A. The prediction of malignant cerebral infarction by molecular brain barrier disruption markers. Stroke 2005, 36, 1921–1926. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wang, Z.; Huang, Z.-X.; Liu, Z. Biomarkers and the outcomes of ischemic stroke. Front. Mol. Neurosci. 2023, 16, 1171101. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ASPECTS *, [53] |
| Barthel Index score **, [54] |
| CoRisk score ***, [55] |
| HINTS tests #, [56] |
| modified Rankin score (mRS) ##, [57] |
| NIHSS ###, [58] |
| OSCP $, [59] |
| Prehospital Stroke Score (PreSS), [60] |
| TOAST $$$, [61] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anogianakis, G.; Daios, S.; Topouzis, N.; Barmpagiannos, K.; Kaiafa, G.; Myrou, A.; Ztriva, E.; Tsankof, A.; Karlafti, E.; Anogeianaki, A.; et al. Current Trends in Stroke Biomarkers: The Prognostic Role of S100B and GFAP. Life 2024, 14, 1247. https://doi.org/10.3390/life14101247
Anogianakis G, Daios S, Topouzis N, Barmpagiannos K, Kaiafa G, Myrou A, Ztriva E, Tsankof A, Karlafti E, Anogeianaki A, et al. Current Trends in Stroke Biomarkers: The Prognostic Role of S100B and GFAP. Life. 2024; 14(10):1247. https://doi.org/10.3390/life14101247
Chicago/Turabian StyleAnogianakis, Georgios, Stylianos Daios, Nikolaos Topouzis, Konstantinos Barmpagiannos, Georgia Kaiafa, Athena Myrou, Eleftheria Ztriva, Alexandra Tsankof, Eleni Karlafti, Antonia Anogeianaki, and et al. 2024. "Current Trends in Stroke Biomarkers: The Prognostic Role of S100B and GFAP" Life 14, no. 10: 1247. https://doi.org/10.3390/life14101247