
Curcumin as a Multifunctional Spice Ingredient against Mental Disorders in Humans: Current Clinical Studies and Bioavailability Concerns


 , ,
, , 

Abstract
:1. Introduction
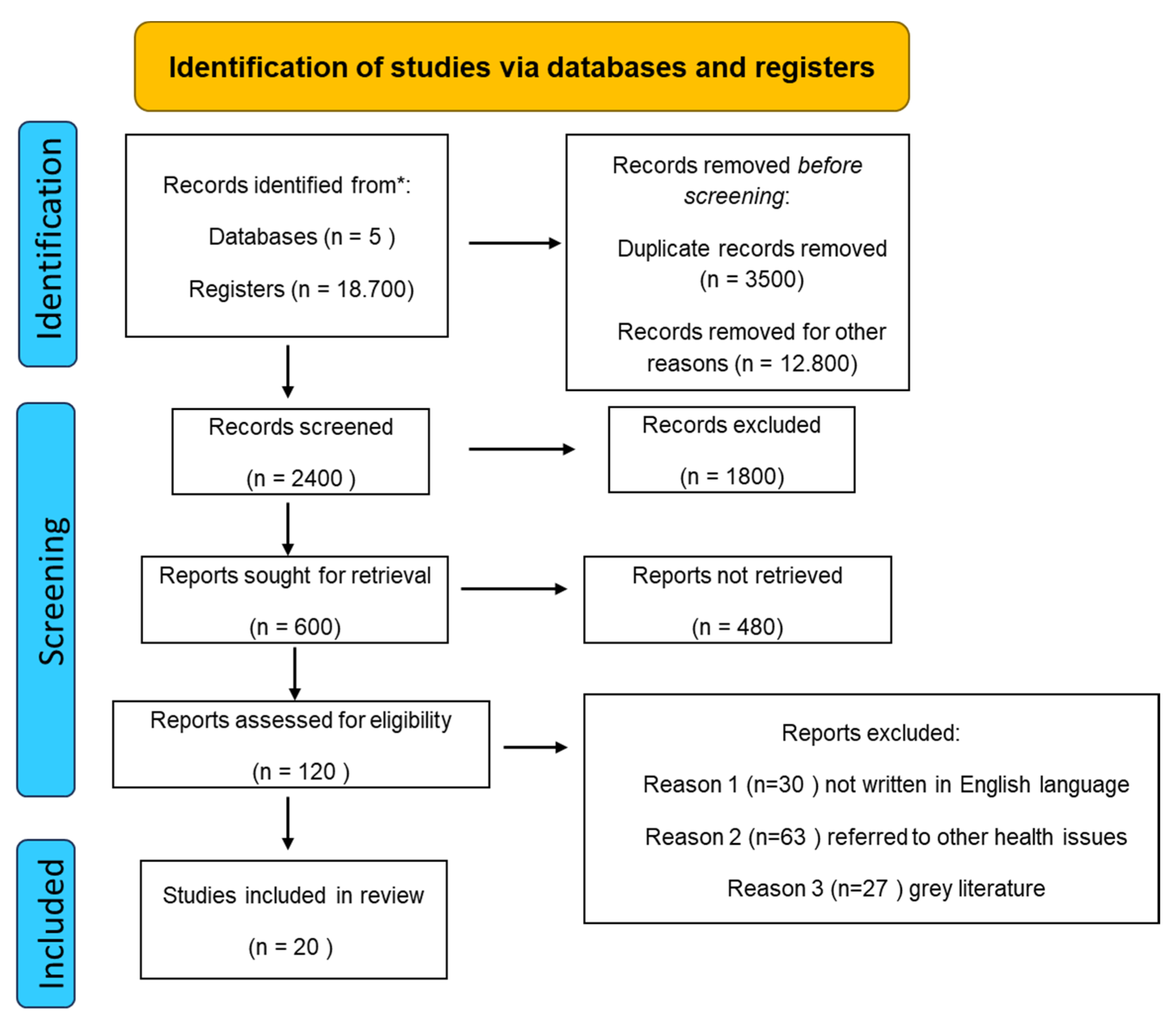
2. Materials and Methods
3. Curcumin’s Chemical Properties
4. Results
4.1. Depression
4.2. Curcumin and Depression
4.3. Bipolar Disorder
4.4. Curcumin in Bipolar Disorder Treatment
4.5. Curcumin and Anxiety and Stress Disorders
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Arias, D.; Saxena, S.; Verguet, S. Quantifying the global burden of mental disorders and their economic value. EClinicalMedicine 2022, 54, 101675. [Google Scholar] [CrossRef] [PubMed]
- Kumari, A.; Raina, N.; Wahi, A.; Goh, K.W.; Sharma, P.; Nagpal, R.; Jain, A.; Ming, L.C.; Gupta, M. Wound-Healing Effects of Curcumin and Its Nanoformulations: A Comprehensive Review. Pharmaceutics 2022, 14, 2288. [Google Scholar] [CrossRef] [PubMed]
- Bássoli, R.M.F.; Audi, D.; Ramalho, B.J.; Audi, M.; Quesada, K.R.; Barbalho, S.M. The Effects of Curcumin on Neurodegenerative Diseases: A Systematic Review. J. Herb. Med. 2023, 42, 100771. [Google Scholar] [CrossRef]
- Awad, A.S.; El-Sharif, A.A. Curcumin immune-mediated and anti-apoptotic mechanisms protect against renal ischemia/reperfusion and distant organ induced injuries. Int. Immunopharmacol. 2011, 11, 992–996. [Google Scholar] [CrossRef] [PubMed]
- Sanmukhani, J.; Satodia, V.; Trivedi, J.; Patel, T.; Tiwari, D.; Panchal, B.; Goel, A.; Tripathi, C.B. Efficacy and safety of curcumin in major depressive disorder: A randomized controlled trial. Phytother. Res. 2014, 28, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Benameur, T.; Giacomucci, G.; Panaro, M.A.; Ruggiero, M.; Trotta, T.; Monda, V.; Pizzolorusso, I.; Lofrumento, D.D.; Porro, C.; Messina, G. New Promising Therapeutic Avenues of Curcumin in Brain Diseases. Molecules 2021, 27, 236. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, S.K.; Dhir, A. An overview of curcumin in neurological disorders. Indian J. Pharm. Sci. 2010, 72, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Hewlings, S.J.; Kalman, D.S. Curcumin: A Review of Its Effects on Human Health. Foods 2017, 6, 92. [Google Scholar] [CrossRef]
- Xu, X.Y.; Meng, X.; Li, S.; Gan, R.Y.; Li, Y.; Li, H.B. Bioactivity, Health Benefits, and Related Molecular Mechanisms of Curcumin: Current Progress, Challenges, and Perspectives. Nutrients 2018, 10, 1553. [Google Scholar] [CrossRef]
- Zheng, Q.T.; Yang, Z.H.; Yu, L.Y.; Ren, Y.Y.; Huang, Q.X.; Liu, Q.; Ma, X.Y.; Chen, Z.K.; Wang, Z.B.; Zheng, X. Synthesis and antioxidant activity of curcumin analogs. J. Asian Nat. Prod. Res. 2017, 19, 489–503. [Google Scholar] [CrossRef]
- Ng, Q.X.; Koh, S.S.H.; Chan, H.W.; Ho, C.Y.X. Clinical Use of Curcumin in Depression: A Meta-Analysis. J. Am. Med. Dir. Assoc. 2017, 18, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Ku, B.; Tie, L.; Yao, H.; Jiang, W.; Ma, X.; Li, X. Curcumin reverses the effects of chronic stress on behavior, the HPA axis, BDNF expression and phosphorylation of CREB. Brain Res. 2006, 1122, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ghosh, S.S.; Ghosh, S. Curcumin improves intestinal barrier function: Modulation of intracellular signaling, and organization of tight junctions. Am. J. Physiol. Cell Physiol. 2017, 312, C438–C445. [Google Scholar] [CrossRef] [PubMed]
- Ammon, H.P.; Wahl, M.A. Pharmacology of Curcuma longa. Planta Med. 1991, 57, 1–7. [Google Scholar] [CrossRef]
- Liu, W.; Zhai, Y.; Heng, X.; Che, F.Y.; Chen, W.; Sun, D.; Zhai, G. Oral bioavailability of curcumin: Problems and advancements. J. Drug Target. 2016, 24, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Tabanelli, R.; Brogi, S.; Calderone, V. Improving Curcumin Bioavailability: Current Strategies and Future Perspectives. Pharmaceutics 2021, 13, 1715. [Google Scholar] [CrossRef] [PubMed]
- Slika, L.; Patra, D. A short review on chemical properties, stability and nano-technological advances for curcumin delivery. Expert Opin. Drug Deliv. 2020, 17, 61–75. [Google Scholar] [CrossRef] [PubMed]
- Roman, B.; Retajczyk, M.; Sałaciński, Ł.; Pełech, R. Curcumin—Properties, Applications and Modification of Structure. Mini-Rev. Org. Chem. 2020, 17, 486–495. [Google Scholar] [CrossRef]
- Priyadarsini, K.I. Chemical and structural features influencing the biological activity of curcumin. Curr. Pharm. Des. 2013, 19, 2093–2100. [Google Scholar] [CrossRef]
- Priyadarsini, K.I. The chemistry of curcumin: From extraction to therapeutic agent. Molecules 2014, 19, 20091–20112. [Google Scholar] [CrossRef]
- Tahay, P.; Parsa, Z.; Zamani, P.; Safari, N. A structural and optical study of curcumin and curcumin analogs. J. Iran. Chem. Soc. 2022, 19, 3177–3188. [Google Scholar] [CrossRef]
- Mary, C.P.V.; Vijayakumar, S.; Shankar, R. Metal chelating ability and antioxidant properties of Curcumin-metal complexes—A DFT approach. J. Mol. Graph. Model. 2018, 79, 1–14. [Google Scholar] [CrossRef]
- Aggarwal, B.B.; Sundaram, C.; Malani, N.; Ichikawa, H. Curcumin: The Indian solid gold. In The Molecular Targets and Therapeutic Uses of Curcumin in Health and Disease; Aggarwal, B.B., Surh, Y.-J., Shishodia, S., Eds.; Advances in Experimental Medicine and Biology; Springer: Boston, MA, USA, 2007; pp. 1–75. [Google Scholar] [CrossRef]
- Metzler, M.; Pfeiffer, E.; Schulz, S.I.; Dempe, J.S. Curcumin uptake and metabolism. Biofactors 2013, 39, 14–20. [Google Scholar] [CrossRef]
- Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B. Bioavailability of curcumin: Problems and promises. Mol. Pharm. 2007, 4, 807–818. [Google Scholar] [CrossRef]
- Pan, M.H.; Huang, T.M.; Lin, J.K. Biotransformation of curcumin through reduction and glucuronidation in mice. Drug Metab. Dispos. 1999, 27, 486–494. [Google Scholar] [PubMed]
- Shoba, G.; Joy, D.; Joseph, T.; Majeed, M.; Rajendran, R.; Srinivas, P.S. Influence of piperine on the pharmacokinetics of curcumin in animals and human volunteers. Planta Med. 1998, 64, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Gota, V.S.; Maru, G.B.; Soni, T.G.; Gandhi, T.R.; Kochar, N.; Agarwal, M.G. Safety and pharmacokinetics of a solid lipid curcumin particle formulation in osteosarcoma patients and healthy volunteers. J. Agric. Food Chem. 2010, 58, 2095–2099. [Google Scholar] [CrossRef]
- Hundshammer, C.; Schön, C.; Kimura, M.; Furune, T.; Terao, K.; Dana Elgeti, D.; Mohr, R. Enhanced metabolic bioavailability of tetrahydrocurcumin after oral supplementation of a γ-cyclodextrin curcumin complex. J. Funct. Food 2021, 79, 104410. [Google Scholar] [CrossRef]
- Yallapu, M.M.; Nagesh, P.K.; Jaggi, M.; Chauhan, S.C. Therapeutic Applications of Curcumin Nanoformulations. AAPS J. 2015, 17, 1341–1356. [Google Scholar] [CrossRef]
- Belmaker, R.H.; Agam, G. Major depressive disorder. N. Engl. J. Med. 2008, 358, 55–68. [Google Scholar] [CrossRef]
- Krishnan, V.; Nestler, E.J. The molecular neurobiology of depression. Nature 2008, 455, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Drevets, W.C. Neuroimaging and neuropathological studies of depression: Implications for the cognitive-emotional features of mood disorders. Curr. Opin. Neurobiol. 2001, 11, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Khandaker, G.M.; Zammit, S.; Burgess, S.; Lewis, G.; Jones, P.B. Association between a functional interleukin 6 receptor genetic variant and risk of depression and psychosis in a population-based birth cohort. Brain Behav. Immun. 2018, 69, 264–272. [Google Scholar] [CrossRef]
- Mihailova, S.; Ivanova-Genova, E.; Lukanov, T.; Stoyanova, V.; Milanova, V.; Naumova, E. A study of TNF-α, TGF-β, IL-10, IL-6, and IFN-γ gene polymorphisms in patients with depression. J. Neuroimmunol. 2016, 293, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Duman, R.; Aghajanian, G.K. Synaptic dysfunction in depression: Potential therapeutic targets. Science 2012, 338, 68–72. [Google Scholar] [CrossRef]
- Duman, R.S.; Monteggia, L.M. A neurotrophic model for stress-related mood disorders. Biol. Psychiatry 2006, 59, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Delva, N.C.; Stanwood, G.D. Dysregulation of brain dopamine systems in major depressive disorder. Exp. Biol. Med. 2021, 246, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
- Belujon, P.; Grace, A.A. Dopamine System Dysregulation in Major Depressive Disorders. Int. J. Neuropsychopharmacol. 2017, 20, 1036–1046. [Google Scholar] [CrossRef]
- Cavaleri, D.; Moretti, F.; Bartoccetti, A.; Mauro, S.; Crocamo, C.; Carrà, G.; Bartoli, F. The role of BDNF in major depressive disorder, related clinical features, and antidepressant treatment: Insight from meta-analyses. Neurosci. Biobehav. Rev. 2023, 149, 105159. [Google Scholar] [CrossRef]
- Kugaya, A.; Sanacora, G. Beyond monoamines: Glutamatergic function in mood disorders. CNS Spectr. 2005, 10, 808–819. [Google Scholar] [CrossRef]
- Khoodoruth, M.A.S.; Estudillo-Guerra, M.A.; Pacheco-Barrios, K.; Nyundo, A.; Chapa-Koloffon, G.; Ouanes, S. Glutamatergic System in Depression and Its Role in Neuromodulatory Techniques Optimization. Front. Psychiatry 2022, 13, 886918. [Google Scholar] [CrossRef] [PubMed]
- Pariante, C.M.; Nemeroff, C.B. Chapter 14—Unipolar depression. In Handbook of Clinical Neurology; Aminoff, M.J., Boller, F., Swaab, D.F., Eds.; Neurobiology of Psychiatric Disorders; Elsevier: Amsterdam, The Netherlands, 2012; Volume 106, pp. 239–249. [Google Scholar] [CrossRef]
- Ramaholimihaso, T.; Bouazzaoui, F.; Kaladjian, A. Curcumin in Depression: Potential Mechanisms of Action and Current Evidence-A Narrative Review. Front. Psychiatry 2020, 11, 572533. [Google Scholar] [CrossRef] [PubMed]
- Taworntawat, C.; Neeser, K.J.; Somrongthong, R.; O’Brien, T.E. Measuring Success of Meditation, Curcumin Supplementation and Sunlight Exposure among Office Workers with Mild Depression. Indian J. Forensic Med. Toxicol. 2022, 16, 112–121. [Google Scholar] [CrossRef]
- Yu, J.J.; Pei, L.B.; Zhang, Y.; Wen, Z.Y.; Yang, J.L. Chronic Supplementation of Curcumin Enhances the Efficacy of Antidepressants in Major Depressive Disorder: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. J. Clin. Psychopharmacol. 2015, 35, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Kuszewski, J.C.; Wong, R.H.X.; Wood, L.G.; Howe, P.R.C. Effects of fish oil and curcumin supplementation on cerebrovascular function in older adults: A randomized controlled trial. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 625–633. [Google Scholar] [CrossRef]
- Cox, K.H.; Pipingas, A.; Scholey, A.B. Investigation of the effects of solid lipid curcumin on cognition and mood in a healthy older population. J. Psychopharmacol. 2015, 29, 642–651. [Google Scholar] [CrossRef]
- Esmaily, H.; Sahebkar, A.; Iranshahi, M.; Ganjali, S.; Mohammadi, A.; Ferns, G.; Ghayour-Mobarhan, M. An investigation of the effects of curcumin on anxiety and depression in obese individuals: A randomized controlled trial. Chin. J. Integr. Med. 2015, 21, 332–338. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Maes, M.; Meddens, M.J.; Maker, G.L.; Arnoldussen, E.; Drummond, P.D. Curcumin and major depression: A randomised, double-blind, placebo-controlled trial investigating the potential of peripheral biomarkers to predict treatment response and antidepressant mechanisms of change. Eur. Neuropsychopharmacol. 2015, 25, 38–50. [Google Scholar] [CrossRef]
- Kanchanatawan, B.; Tangwongchai, S.; Sughondhabhirom, A.; Suppapitiporn, S.; Hemrunrojn, S.; Carvalho, A.F.; Maes, M. Add-on Treatment with Curcumin Has Antidepressive Effects in Thai Patients with Major Depression: Results of a Randomized Double-Blind Placebo-Controlled Study. Neurotox. Res. 2018, 33, 621–633. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Drummond, P.D. Efficacy of curcumin, and a saffron/curcumin combination for the treatment of major depression: A randomised, double-blind, placebo-controlled study. J. Affect. Disord. 2017, 207, 188–196. [Google Scholar] [CrossRef]
- Akbarzadeh, F.; Niksun, N.; Behravan, G.; Behdani, F.; Mohammadpour, A.H.; Jaafari, M.; Hosseini, T.; Rajai, Z.; Ebrahimi, A.; Eslamzadeh, M. The effect of adding curcumin to sodium valproate in treatment of patients with bipolar disorder in the acute phase of mania: A randomized double-blind clinical trial. Front. Psychiatry 2023, 14, 1068277. [Google Scholar] [CrossRef] [PubMed]
- Bergman, J.; Miodownik, C.; Bersudsky, Y.; Sokolik, S.; Lerner, P.P.; Kreinin, A.; Polakiewicz, J.; Lerner, V. Curcumin as an add-on to antidepressive treatment: A randomized, double-blind, placebo-controlled, pilot clinical study. Clin. Neuropharmacol. 2013, 36, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Panahi, Y.; Badeli, R.; Karami, G.R.; Sahebkar, A. Investigation of the efficacy of adjunctive therapy with bioavailability-boosted curcuminoids in major depressive disorder. Phytother. Res. 2015, 29, 17–21. [Google Scholar] [CrossRef]
- Fanaei, H.; Khayat, S.; Kasaeian, A.; Javadimehr, M. Effect of curcumin on serum brain-derived neurotrophic factor levels in women with premenstrual syndrome: A randomized, double-blind, placebo-controlled trial. Neuropeptides 2016, 56, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Asadi, S.; Gholami, M.S.; Siassi, F.; Qorbani, M.; Sotoudeh, G. Beneficial effects of nano-curcumin supplement on depression and anxiety in diabetic patients with peripheral neuropathy: A randomized, double-blind, placebo-controlled clinical trial. Phytother. Res. 2020, 34, 896–903. [Google Scholar] [CrossRef]
- Latif, R.; Mumtaz, S.; Al Sheikh, M.H.; Chathoth, S.; Nasser Al Naimi, S. Effects of Turmeric on Cardiovascular Risk Factors, Mental Health, and Serum Homocysteine in Overweight, Obese Females. Altern. Ther. Health Med. 2021, 27, 114–119. [Google Scholar] [PubMed]
- Lopresti, A.L.; Smith, S.J.; Rea, A.; Michel, S. Efficacy of a curcumin extract (Curcugen™) on gastrointestinal symptoms and intestinal microbiota in adults with self-reported digestive complaints: A randomised, double-blind, placebo-controlled study. BMC Complement. Med. Ther. 2021, 21, 40. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Ma, Z.; Zhang, X.; Zhou, F. Evaluation of Effect of Curcumin on Psychological State of Patients with Pulmonary Hypertension by Magnetic Resonance Image under Deep Learning. Contrast Media Mol. Imaging 2021, 2021, 9935754. [Google Scholar] [CrossRef]
- Donovan, E.K.; Kekes-Szabo, S.; Lin, J.C.; Massey, R.L.; Cobb, J.D.; Hodgin, K.S.; Ness, T.J.; Hangee-Bauer, C.; Younger, J.W. A Placebo-Controlled, Pseudo-Randomized, Crossover Trial of Botanical Agents for Gulf War Illness: Curcumin (Curcuma longa), Boswellia (Boswellia serrata), and French Maritime Pine Bark (Pinus pinaster). Int. J. Environ. Res. Public Health 2021, 18, 2468. [Google Scholar] [CrossRef]
- Pandaran Sudheeran, S.; Jacob, D.; Natinga Mulakal, J.; Gopinathan Nair, G.; Maliakel, A.; Maliakel, B.; Kuttan, R.; Im, K. Safety, Tolerance, and Enhanced Efficacy of a Bioavailable Formulation of Curcumin With Fenugreek Dietary Fiber on Occupational Stress: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. J. Clin. Psychopharmacol. 2016, 36, 236–243. [Google Scholar] [CrossRef]
- Kawasaki, K.; Muroyama, K.; Murosaki, S. Effect of a water extract of Curcuma longa on emotional states in healthy participants. Biosci. Microbiota Food Health 2018, 37, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Khatri, D.K.; Juvekar, A.R. Kinetics of Inhibition of Monoamine Oxidase Using Curcumin and Ellagic Acid. Pharmacogn. Mag. 2016, 12 (Suppl. S2), S116–S120. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Berk, M.; Schulze, T.G.; Carvalho, A.F.; Suppes, T.; Calabrese, J.R.; Gao, K.; Miskowiak, K.W.; Grande, I. Bipolar disorders. Nat. Rev. Dis. Primers 2018, 4, 18008. [Google Scholar] [CrossRef] [PubMed]
- Hamdani, N.; Doukhan, R.; Kurtlucan, O.; Tamouza, R.; Leboyer, M. Immunity, inflammation, and bipolar disorder: Diagnostic and therapeutic implications. Curr. Psychiatry Rep. 2013, 15, 387. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Jung, H.G.; Myint, A.M.; Kim, H.; Park, S.H. Imbalance between pro-inflammatory and anti-inflammatory cytokines in bipolar disorder. J. Affect. Disord. 2007, 104, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Brietzke, E.; Stertz, L.; Fernandes, B.S.; Kauer-Sant’anna, M.; Mascarenhas, M.; Escosteguy Vargas, A.; Chies, J.A.; Kapczinski, F. Comparison of cytokine levels in depressed, manic and euthymic patients with bipolar disorder. J. Affect. Disord. 2009, 116, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Rosenblat, J.D.; McIntyre, R.S. Bipolar Disorder and Immune Dysfunction: Epidemiological Findings, Proposed Pathophysiology and Clinical Implications. Brain Sci. 2017, 7, 144. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Vansteelandt, K.; Correll, C.U.; Mitchell, A.J.; De Herdt, A.; Sienaert, P.; Probst, M.; De Hert, M. Metabolic syndrome and metabolic abnormalities in bipolar disorder: A meta-analysis of prevalence rates and moderators. Am. J. Psychiatry 2013, 170, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Nierenberg, A.A.; Agustini, B.; Köhler-Forsberg, O.; Cusin, C.; Katz, D.; Sylvia, L.G.; Peters, A.; Berk, M. Diagnosis and Treatment of Bipolar Disorder: A Review. JAMA 2023, 330, 1370–1380. [Google Scholar] [CrossRef]
- Sigitova, E.; Fišar, Z.; Hroudová, J.; Cikánková, T.; Raboch, J. Biological hypotheses and biomarkers of bipolar disorder. Psychiatry Clin. Neurosci. 2017, 71, 77–103. [Google Scholar] [CrossRef]
- Scola, G.; Andreazza, A.C. The role of neurotrophins in bipolar disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2015, 56, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Gandal, M.J.; Haney, J.R.; Parikshak, N.N.; Leppa, V.; Ramaswami, G.; Hartl, C.; Schork, A.J.; Appadurai, V.; Buil, A.; Werge, T.M.; et al. Shared molecular neuropathology across major psychiatric disorders parallels polygenic overlap. Science 2018, 359, 693–697. [Google Scholar] [CrossRef]
- Sarris, J.; Lake, J.; Hoenders, R. Bipolar disorder and complementary medicine: Current evidence, safety issues, and clinical considerations. J. Altern. Complement. Med. 2011, 17, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Brietzke, E.; Mansur, R.B.; Zugman, A.; Carvalho, A.F.; Macêdo, D.S.; Cha, D.S.; Abílio, V.C.; McIntyre, R.S. Is there a role for curcumin in the treatment of bipolar disorder? Med. Hypotheses 2013, 80, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.; Mocking, R.J.; Ruhé, H.G.; Visser, I.; Koeter, M.W.; Assies, J.; Bockting, C.L.; Olff, M.; Schene, A.H. Longitudinal hypothalamic-pituitary-adrenal axis trait and state effects in recurrent depression. Psychoneuroendocrinology 2012, 37, 892–902. [Google Scholar] [CrossRef]
- Xu, Y.; Ku, B.; Cui, L.; Li, X.; Barish, P.A.; Foster, T.C.; Ogle, W.O. Curcumin reverses impaired hippocampal neurogenesis and increases serotonin receptor 1A mRNA and brain-derived neurotrophic factor expression in chronically stressed rats. Brain Res. 2007, 1162, 9–18. [Google Scholar] [CrossRef]
- Tan, X.; Poulose, E.M.; Raveendran, V.V.; Zhu, B.T.; Stechschulte, D.J.; Dileepan, K.N. Regulation of the expression of cyclooxygenases and production of prostaglandin I₂ and E₂ in human coronary artery endothelial cells by curcumin. J. Physiol. Pharmacol. 2011, 62, 21–28. [Google Scholar]
- COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- de Kloet, E.R.; Joëls, M.; Holsboer, F. Stress and the brain: From adaptation to disease. Nat. Rev. Neurosci. 2005, 6, 463–475. [Google Scholar] [CrossRef]
- Lopresti, A.L. Potential Role of Curcumin for the Treatment of Major Depressive Disorder. CNS Drugs 2022, 36, 123–141. [Google Scholar] [CrossRef]
- Mawson, A.R.; Croft, A.M. Gulf War Illness: Unifying Hypothesis for a Continuing Health Problem. Int. J. Environ. Res. Public Health 2019, 16, 111. [Google Scholar] [CrossRef] [PubMed]
- Reddy, D.N.K.; Huang, F.Y.; Wang, S.P.; Kumar, R. Synergistic Antioxidant and Antibacterial Activity of Curcumin-C3 Encapsulated Chitosan Nanoparticles. Curr. Pharm. Des. 2020, 26, 5021–5029. [Google Scholar] [CrossRef]
- Kocaadam, B.; Şanlier, N. Curcumin, an active component of turmeric (Curcuma longa), and its effects on health. Crit. Rev. Food Sci. Nutr. 2017, 57, 2889–2895. [Google Scholar] [CrossRef] [PubMed]
- Coppen, A.; Bolander-Gouaille, C. Treatment of depression: Time to consider folic acid and vitamin B12. J. Psychopharmacol. 2005, 19, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Mimica, B.; Bučević Popović, V.; Banjari, I.; Jeličić Kadić, A.; Puljak, L. Methods Used for Enhancing the Bioavailability of Oral Curcumin in Randomized Controlled Trials: A Meta-Research Study. Pharmaceuticals 2022, 15, 939. [Google Scholar] [CrossRef] [PubMed]
- Sunagawa, Y.; Hirano, S.; Katanasaka, Y.; Miyazaki, Y.; Funamoto, M.; Okamura, N.; Hojo, Y.; Suzuki, H.; Doi, O.; Yokoji, T.; et al. Colloidal submicron-particle curcumin exhibits high absorption efficiency-a double-blind, 3-way crossover study. J. Nutr. Sci. Vitaminol. 2015, 61, 37–44. [Google Scholar] [CrossRef]
- Small, G.W.; Siddarth, P.; Li, Z.; Miller, K.J.; Ercoli, L.; Emerson, N.D.; Martinez, J.; Wong, K.P.; Liu, J.; Merrill, D.A.; et al. Memory and Brain Amyloid and Tau Effects of a Bioavailable Form of Curcumin in Non-Demented Adults: A Double-Blind, Placebo-Controlled 18-Month Trial. Am. J. Geriatr. Psychiatry 2018, 26, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Ho, J.N.; Kook, H.R.; Lee, S.; Oh, J.J.; Hong, S.K.; Lee, S.E.; Byun, S.S. Theracurmin® efficiently inhibits the growth of human prostate and bladder cancer cells via induction of apoptotic cell death and cell cycle arrest. Oncol. Rep. 2016, 35, 1463–1472. [Google Scholar] [CrossRef]
- Lee, B.; Lee, H. Systemic Administration of Curcumin Affect Anxiety-Related Behaviors in a Rat Model of Posttraumatic Stress Disorder via Activation of Serotonergic Systems. Evid. Based Complement. Altern. Med. 2018, 2018, 041309. [Google Scholar] [CrossRef]
- Hussain, Y.; Khan, H.; Alam, W.; Ali, Z.; Ibrar, M. Curcumin targeting oxidative mediators for therapeutic effects in diabetes and its related complications. Phytonutrients 2022, 1, 27–30. [Google Scholar] [CrossRef]
- Pratti, V.L.; Thomas, M.; Bhoite, R.; Satyavrat, V. Investigating Bioavailability of Curcumin and Piperine Combination in Comparison to Turmeric Rhizomes: An in vitro Study. J. Exp. Pharmacol. 2024, 16, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.A.; Sun, P.; Duan, C.; Cao, Y.; Kong, B.; Wang, H.; Chen, Q. Improving stability and bioavailability of curcumin by quaternized chitosan coated nanoemulsion. Food Res. Int. 2023, 174 Pt 1, 113634. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhang, H.; Zhao, H.; Fu, S.; Li, R.; Wang, Z.; Wang, Y.; Lu, W.; Yang, X. Nanoparticle encapsulation using self-assembly abietic acid to improve oral bioavailability of curcumin. Food Chem. 2024, 436, 137676. [Google Scholar] [CrossRef] [PubMed]
- Alavi, F.; Ciftci, O.N. Green and single-step simultaneous composite starch aerogel formation-high bioavailability curcumin particle formation. Int. J. Biol. Macromol. 2024, 264, 129945. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Type, Participants (N) | Type of Mental Disorder and Screening Tools | Supplementation | Main Results | Ref. |
|---|---|---|---|---|
| Cross-sectional study, 68 office workers, 2 groups (OG and CG) | Mild depression. At Day 0, Day 30 and Day 60, all subjects were compared in terms of vitamin D, BDNF, IL-6 and PHQ-9. | Curcumin caps: 1000 mg × 2 in the OG. Mindfulness meditation sunlight exposure in both groups, 8 weeks observation. | Vitamin D in Day 0, 30 and Day 30, 60 intervals were significantly higher in OG than in CG. IL-6 serum levels decreased on Day 30 in OG than in CG. Depression scores were lower in OG than in CG at Day 30 and Day 60. | [45] |
| Randomized, double-blind, placebo-controlled study, 108 male adults | Major Depressive Disorder, The Chinese version of 17-item HDRS, MADRS | 1000 mg × 2 curcumin (capsules) or placebo soybean powder daily for 6 weeks on the basis of their current antidepressant medications. | Significant antidepressant behavioral response in depressed patients. ↓ Inflammatory cytokines interleukin 1β and tumor necrosis factor α level and salivary cortisol concentrations. ↑ Plasma BDNF levels. Reports of mild nausea in the curcumin and escitalopram group. | [46] |
| Randomized, double-blind, placebo-controlled, 2 × 2 factorial design, 152 overweight or obese non-depressed adults (50–80 years) trial | Mental health and Well-Being, POMS questionnaire | Curcumin (160 mg/day), fish oil (2000 mg docosahexaenoic acid + 400 mg eicosapentaenoic acid/day), or a combination of both for 16 weeks. | ↓ SMCs (compared to no curcumin treatment). Combining curcumin with fish oil did not result in additive effects. | [47] |
| Randomized, double-blind, placebo-controlled trial, 60 healthy older adults (60–85 years) | Mood disorders: psychological stress, fatigue, Trait scale of the STAI, BDI-II, Depression, Anxiety and Stress Scales. Chalder Fatigue Scale | A solid lipid curcumin formulation (400 mg as Longvida®) was administrated orally (1 h and 3 h after a single dose), chronic (4 weeks) and acute-on-chronic (1 h and 3 h after single dose following chronic treatment. | Significant improvements in fatigue, anxiety and stress compared to control group were observed. No side effects. Hepatocellular safety was retained. LDL levels were reduced. | [48] |
| RCT, double-blind, cross-over trial, 30 obese patients | Anxiety and depression, BDI-II | Curcumin (1 g/day) or placebo for a period of 30 days. Following a wash-out interval of 2 weeks, each subject was crossed over to the alternative regimen for a further 30 days. | ↓ Anxiety symptoms. No significant impact on BDI-II scores. | [49] |
| Randomized, double-blind, placebo-controlled trial, 56 adults (18–65 y) diagnosed with major depressive disorder | Major depression, IDS-SR30, STAI, various urinary and plasma biomarkers. | 2 × 500 mg/day curcumin extract or placebo for 8 weeks. | ↑ Urinary thromboxane B2 and substance P. ↓ IDS-SR30 score. | [50] |
| Randomized double-blind placebo-controlled study, 65 patients (18–63 y) | Major depression, MADRS (1979) and HAM-A | Curcumin (increasing dose from 500 to 1500 mg/day) or placebo for 12 weeks. | Improved MADRS scores. The effects were more pronounced in males compared to females. No statistically significant treatment-emerging adverse effects and no significant effects of curcumin on blood chemistry and ECG measurements. Significant antidepressant effects in participants with MDD. Curcumin administration was safe and well tolerated even when combined with antidepressants. | [51] |
| Randomized, double-blind, placebo-controlled trial, 123 adults with depression, mean age 43 years, 14 males and 109 females | Major depression, IDS-SR30, STAI | 2 × 250 mg/day curcumin extract or 2 × 500 mg/day curcumin extract or 2 × 250 mg/day curcumin extract +15 mg safran extract or placebo for 12 weeks. | Curcumin treatment group associated with significantly greater decrease in IDS-SR30, STAI-state and STAI-trait scores. No differences in efficacy between the active treatment groups. Adverse effects: diarrhea and loose bowels in the high-dose (2 × 500 mg/day) curcumin group. | [52] |
| Randomized double-blind clinical trial, 55 adults with BD | Bipolar disorder in the mania phase, YMRS, MMSE, CGI | 40 mg nano-curcumin (Sinacurcumin) daily, combined with valproic acid medication (600 mg/day + 20 mg/kg) for 4 weeks. | No significant differences between groups. | [53] |
| Randomized, single-blind trial, 60 adults with MDD | Major depressive disorder, HDRS, CGI | Fluoxetine (20 mg) taken in the morning, or 2 × 500 mg/day curcumin extract or fluoxetine (2 × 20 mg/day) taken in the morning + 2 × 500 mg/day curcumin extract for 6 weeks. | No significance in group differences. Increased frequency of gastritis in the fluoxetine and curcumin group was observed. | [5] |
| Randomized double-blind control trial, 40 adults 20–40 years old | Depression, CGI-Severity Scale, HDRS, MADRS | 500 mg curcumin + 120 mg of ellagic acid (70% concentrate) extracted from pomegranate’s peel, and 50 mg of piperine or placebo together with antidepressants (escitalopram or venlafaxine) 5 weeks | No adverse effects. No significant differences between the groups. Patients in the curcumin group tended to have more rapid relief of depressive symptoms when compared to those in the placebo group. | [54] |
| Clinical trial, 111 adults with MDD at the age of 18–65 y | Major depressive disorder, HADS, BDI–II | 1000 mg/day curcumin extract (C3 Complex) + 10 mg piperine or placebo on standard antidepressant treatment for 6 weeks | ↓ HADS anxiety and depression subscale scores and BDI–II affective, somatic and cognitive subscale scores | [55] |
| Randomized, double-blind, placebo-controlled trial, 70 women with premenstrual syndrome | PMS mental symptoms, PMS symptom self-report questionnaire, serum BDNF measurement. | 100 mg × 2 /day curcumin or placebo for 3 consecutive menstrual cycles. Each cycle lasted for 10 days. | Curcumin group showed improvement in mood, physical and behavioral PMS symptoms. ↑ Serum BDNF after 3 months of treatment. No side effects were reported. | [56] |
| Randomized, double-blind, placebo-controlled trial, 80 adults with type 2 diabetes | Depression and anxiety, DASS-21 | 80 mg/day nano-curcumin capsules or placebo for 8 weeks. | ↓ DASS-21 depression and anxiety score. No reduction in the stress score. | [57] |
| Single-arm trial, 36 young female with a body mass index ≥ 23 kg/m2 | Mental health, DASS-21 | 2 g of turmeric in capsules/day for 90 days. | ↓ DASS-21 anxiety score. ↓ Depression or stress scores. No adverse effects were reported. | [58] |
| Randomized, double-blind, placebo-controlled trial, 79 adults with self-reported digestive complaints (18–65 y) | Depression, anxiety and Stress, DASS-21, SF-36 | 2 × 500 mg/day curcumin extract or placebo for 8 weeks. | ↓ DASS-21 anxiety score and GSRS score. No other between-group differences in other DASS-21 or SF-36 subscale scores. No adverse effects were reported. | [59] |
| Placebo-controlled trial (randomization details not included), 30 adults (5 males and 25 females) with pulmonary hypertension (18–78 y) | Anxiety and depression, SAS, SDS | 60 mg/day of curcumin + conventional antidepressant treatment with the curcumin dose, gradually increasing to 120 mg/day or conventional antidepressant treatment for 3 months. | SAS and SDS scores were significantly lower in the curcumin group compared to control one. No adverse effects were reported. | [60] |
| Randomized control cross-over trial, 20 men 37–65 years old without current post-traumatic stress disorder or major depression | Gulf War Illness, HADS for screening depression and anxiety severity, Qualtrics Research Suite Offline Application (Qualtrics, Provo, UT, USA) and a Visual Analog Scale for measuring symptoms (pain, fatigue, gastrointestinal distress, cognitive dysfunction, depressed mood, dermatologic complaints and respiratory problems) | Pure Encapsulation’s Curcuma <<Meriva>> turmeric phytosome 100 mg/day (low dose and 4000 mg/day (high dose). Pure Encapsulation’s Boswellia product: 400 mg/day and 800 mg/day. Pure Encapsulation’s Pycnogenol (pine bark extract): 200 mg/day and 400 mg/day, Duration 1 month (30 ± 3 days) of placebo, 1 month (30 ± 3 days) of lower-dose botanical, and 1 month (30 ± 3 days) of higher-dose of each botanical. | Curcumin reduced GWI symptom severity significantly more than placebo at both the lower and higher dose. Maritime pine was more effective than placebo at the higher dose. | [61] |
| A double-blinded pilot-controlled study, 60 healthy adults working at responsible positions 33 years old 3 groups | Occupational stress, SF-36 Perceived Stress Scale Beck Anxiety Inventory, and SF-36 health survey scales were employed in the study | Curcumin (Curcuma-galactomannoside (500 mg × 2/day, standard B. curcumin (500 mg × 2/day) Placebo. | Curcumagalactomannoside group: Significant improvements in quality-of-life score. Significant reduction in stress score. Reduced anxiety, oxidative markers and perceived stress. | [62] |
| Randomized double-blind placebo-controlled parallel group trial, 48 healthy adults, 20–64 years old 3 groups | Emotional fatigue, anxiety, POMS | Water extract of C. longa (WEC): 150 mg WEC and 0.40 mg bisacurone (Low-WEC group) 900 mg WEC and 2.40 mg bisacurone (High-WEC group), Matching placebo tablets (placebo group) daily 8 weeks | POMS score of Low WEC group was significantly lower than the placebo group. | [63] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spanoudaki, M.; Papadopoulou, S.K.; Antasouras, G.; Papadopoulos, K.A.; Psara, E.; Vorvolakos, T.; Solovos, E.; Chrysafi, M.; Psallas, M.; Mentzelou, M.; et al. Curcumin as a Multifunctional Spice Ingredient against Mental Disorders in Humans: Current Clinical Studies and Bioavailability Concerns. Life 2024, 14, 479. https://doi.org/10.3390/life14040479
Spanoudaki M, Papadopoulou SK, Antasouras G, Papadopoulos KA, Psara E, Vorvolakos T, Solovos E, Chrysafi M, Psallas M, Mentzelou M, et al. Curcumin as a Multifunctional Spice Ingredient against Mental Disorders in Humans: Current Clinical Studies and Bioavailability Concerns. Life. 2024; 14(4):479. https://doi.org/10.3390/life14040479
Chicago/Turabian StyleSpanoudaki, Maria, Sousana K. Papadopoulou, Georgios Antasouras, Konstantinos A. Papadopoulos, Evmorfia Psara, Theofanis Vorvolakos, Evangelos Solovos, Maria Chrysafi, Michalis Psallas, Maria Mentzelou, and et al. 2024. "Curcumin as a Multifunctional Spice Ingredient against Mental Disorders in Humans: Current Clinical Studies and Bioavailability Concerns" Life 14, no. 4: 479. https://doi.org/10.3390/life14040479
APA StyleSpanoudaki, M., Papadopoulou, S. K., Antasouras, G., Papadopoulos, K. A., Psara, E., Vorvolakos, T., Solovos, E., Chrysafi, M., Psallas, M., Mentzelou, M., Ourda, D., & Giaginis, C. (2024). Curcumin as a Multifunctional Spice Ingredient against Mental Disorders in Humans: Current Clinical Studies and Bioavailability Concerns. Life, 14(4), 479. https://doi.org/10.3390/life14040479