
Evaluating the Efficacy of Resect-and-Discard and Resect-and-Retrieve Strategies for Diminutive Colonic Polyps

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Selection Criteria
2.2. Endoscopic Equipment and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Background Characteristics
3.2. Lesion Characteristics
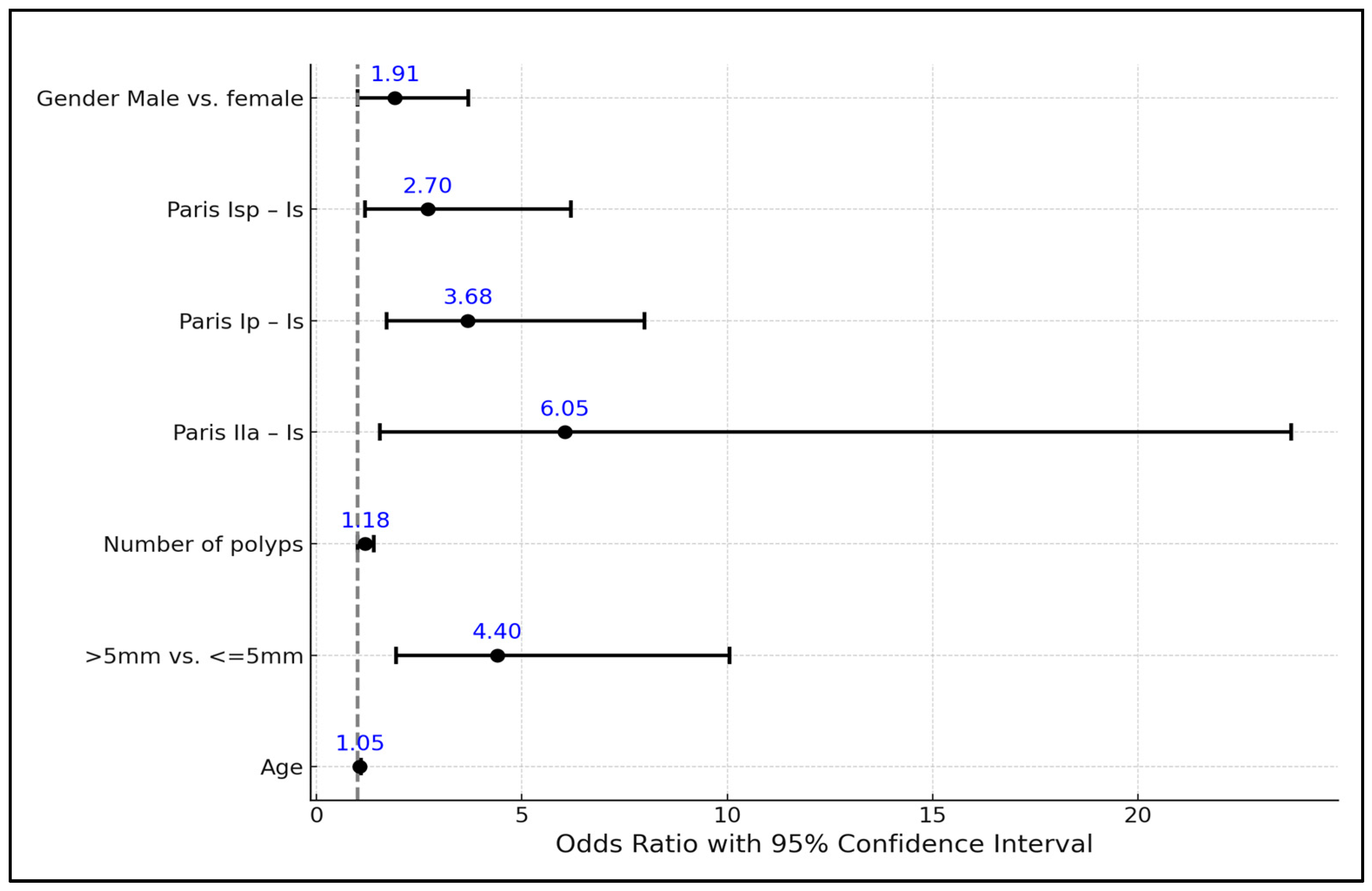
3.3. Risk Factor Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Fearon, E.R.; Vogelstein, B. A genetic model for colorectal tumorigenesis. Cell 1990, 61, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Bretthauer, M.; Løberg, M.; Wieszczy, P.; Kalager, M.; Emilsson, L.; Garborg, K.; Rupinski, M.; Dekker, E.; Spaander, M.; Bugajski, M.; et al. Effect of Colonoscopy Screening on Risks of Colorectal Cancer and Related Death. N. Engl. J. Med. 2022, 387, 1547–1556. [Google Scholar] [CrossRef] [PubMed]
- Ignjatovic, A.; East, J.E.; Suzuki, N.; Vance, M.; Guenther, T.; Saunders, B.P. Optical diagnosis of small colorectal polyps at routine colonoscopy (Detect InSpect ChAracterise Resect and Discard; DISCARD trial): A prospective cohort study. Lancet Oncol. 2009, 10, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Willems, P.; Djinbachian, R.; Ditisheim, S.; Orkut, S.; Pohl, H.; Barkun, A.; Bouin, M.; Faulques, B.; von Renteln, D. Uptake and barriers for implementation of the resect and discard strategy: An international survey. Endosc. Int. Open 2020, 08, E684–E692. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, S.J.; Hyun, J.H.; Han, K.S.; Kim, B.C.; Hong, C.W.; Lee, S.-J.; Sohn, D.K. Correlation between bowel preparation and the adenoma detection rate in screening colonoscopy. Ann. Coloproctol. 2017, 33, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.T.; Rustagi, T.; Laine, L. What level of bowel prep quality requires early repeat colonoscopy: Systematic review and meta-analysis of the impact of preparation quality on adenoma detection rate. Am. J. Gastroenterol. 2014, 109, 1714–1723. [Google Scholar] [CrossRef]
- Kim, J.S.; Kang, S.H.; Moon, H.S.; Lee, E.S.; Kim, S.H.; Sung, J.K.; Lee, B.S.; Jeong, H.Y.; Chung, W.S. Impact of Bowel Preparation Quality on Adenoma Identification During Colonoscopy and Optimal Timing of Surveillance. Dig. Dis. Sci. 2015, 60, 3092–3099. [Google Scholar] [CrossRef]
- Sherer, E.A.; Imler, T.D.; Imperiale, T.F. The effect of colonoscopy preparation quality on adenoma detection rates. Gastrointest. Endosc. 2012, 75, 545–553. [Google Scholar] [CrossRef]
- Rees, C.J.; Rajasekhar, P.T.; Wilson, A.; Close, H.; Rutter, M.D.; Saunders, B.P.; East, J.E.; Maier, R.; Moorghen, M.; Muhammad, U.; et al. Narrow band imaging optical diagnosis of small colorectal polyps in routine clinical practice: The Detect Inspect Characterise Resect and Discard 2 (DISCARD 2) study. Gut 2016, 66, 887–895. [Google Scholar] [CrossRef]
- Patrun, J.; Okreša, L.; Iveković, H.; Rustemovi, N. Diagnostic accuracy of NICE classification system for optical recognition of predictive morphology of colorectal polyps. Gastroenterol. Res. Pract. 2018, 2018, 7531368. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.C.L.; Siau, K.; Cannatelli, R.; Antonelli, G.; Shivaji, U.N.; Ghosh, S.; Saltzman, J.R.; Hassan, C.; Iacucci, M. Training methods in optical diagnosis and characterization of colorectal polyps: A systematic review and meta-analysis. Endosc. Int. Open 2021, 09, E716–E726. [Google Scholar] [CrossRef]
- Rondonotti, E.; Hassan, C.; Tamanini, G.; Antonelli, G.; Andrisani, G.; Leonetti, G.; Paggi, S.; Amato, A.; Scardino, G.; Di Paolo, D.; et al. Artificial intelligence-assisted optical diagnosis for the resect-and-discard strategy in clinical practice: The Artificial intelligence BLI Characterization (ABC) study. Endoscopy 2023, 55, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Soltani, I.; von Renteln, D. Diagnosis and Treatment of Diminutive Polyps in the Colon. Curr. Treat. Options Gastroenterol. 2020, 18, 175–187. [Google Scholar] [CrossRef]
- Taghiakbari, M.; Pohl, H.; Djinbachian, R.; Barkun, A.; Marques, P.; Bouin, M.; Deslandres, E.; Panzini, B.; Bouchard, S.; Weber, A.; et al. The location-based resect and discard strategy for diminutive colorectal polyps: A prospective clinical study. Endoscopy 2022, 54, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Kessler, W.R.; Imperiale, T.F.; Klein, R.W.; Wielage, R.C.; Rex, D.K. A quantitative assessment of the risks and cost savings of forgoing histologic examination of diminutive polyps. Endoscopy 2011, 43, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Ferlitsch, M.; Moss, A.; Hassan, C.; Bhandari, P.; Dumonceau, J.M.; Paspatis, G.; Jover, R.; Langner, C.; Bronzwaer, M.; Nalankilli, K.; et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2017, 49, 270–297. [Google Scholar] [CrossRef] [PubMed]
- Odom, S.R.; Duffy, S.D.; Barone, J.E.; Ghevariya, V.; McClane, S.J. The rate of adenocarcinoma in endoscopically removed colorectal polyps. Am. Surg. 2005, 71, 1024–1026. [Google Scholar] [CrossRef]
- Ponugoti, P.L.; Cummings, O.W.; Rex, D.K. Risk of cancer in small and diminutive colorectal polyps. Dig. Liver Dis. 2017, 49, 34–37. [Google Scholar] [CrossRef]
- Butterly, L.F.; Chase, M.P.; Pohl, H.; Fiarman, G.S. Prevalence of clinically important histology in small adenomas. Clin. Gastroenterol. Hepatol. 2006, 4, 343–348. [Google Scholar] [CrossRef]
- Gschwantler, M.; Kriwanek, S.; Langner, E.; Göritzer, B.; Schrutka-Kölbl, C.; Brownstone, E.; Feichtinger, H.; Weiss, W. High-grade dysplasia and invasive carcinoma in colorectal adenomas: A multivariate analysis of the impact of adenoma and patient characteristics. Eur. J. Gastroenterol. Hepatol. 2002, 14, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Hassan, C.; Antonelli, G.; Dumonceau, J.M.; Regula, J.; Bretthauer, M.; Chaussade, S.; Dekker, E.; Ferlitsch, M.; Gimeno-Garcia, A.; Jover, R.; et al. Post-polypectomy colonoscopy surveillance: European Society of Gastrointestinal Endoscopy (ESGE) Guideline-Update 2020. Endoscopy 2020, 52, 687–700. [Google Scholar] [CrossRef] [PubMed]
- Jin, E.H.; Lee, D.; Bae, J.H.; Kang, H.Y.; Kwak, M.S.; Seo, J.Y.; Yang, J.I.; Yang, S.Y.; Lim, S.H.; Yim, J.Y.; et al. Improved Accuracy in Optical Diagnosis of Colorectal Polyps Using Convolutional Neural Networks with Visual Explanations. Gastroenterology 2020, 158, 2169–2179.e8. [Google Scholar] [CrossRef] [PubMed]
- Duong, A.; Pohl, H.; Djinbachian, R.; Deshêtres, A.; Barkun, A.N.; Marques, P.N.; Bouin, M.; Deslandres, E.; Aguilera-Fish, A.; Leduc, R.; et al. Evaluation of the polyp-based resect and discard strategy: A retrospective study. Endoscopy 2022, 54, 128–135. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Number of Patients (n = 427) |
|---|---|
| Age (years) | 59.42 (±11.19) |
| Gender | |
| Male | 257 (60.2%) |
| Female | 170 (39.8%) |
| Indication for colonoscopy | |
| Lower gastrointestinal tract symptoms | 182 (42.6%) |
| Screening | 123 (28.8%) |
| FIT-positive screening | 10 (2.3%) |
| Post CRC surveillance | 31 (7.3%) |
| Post polypectomy surveillance | 78 (18.3%) |
| IBD surveillance | 3 (0.7%) |
| Adequate bowel preparation (%) | 375 (87.8%) |
| Variables | 0–3 mm (n = 256) | 4–5 mm (n = 216) | 6–9 mm (n = 153) | >10 mm (n = 165) | Total (n = 790) | p Value |
|---|---|---|---|---|---|---|
| Age | <0.001 1 | |||||
| Mean (SD) | 58.6 (10.9) | 58.7 (10.6) | 61.0 (10.5) | 62.4 (9.6) | 59.9 (10.6) | |
| Range | 31.0–79.0 | 31.0–82.0 | 31.0–82.0 | 27.0–89.0 | 27.0–89.0 | |
| Gender | 0.701 2 | |||||
| Female | 100.0 (39.1%) | 89.0 (41.2%) | 54.0 (35.3%) | 62.0 (37.6%) | 305.0 (38.6%) | |
| Male | 156.0 (60.9%) | 127.0 (58.8%) | 99.0 (64.7%) | 103.0 (62.4%) | 485.0 (61.4%) | |
| Histology | <0.001 2 | |||||
| Hyperplastic | 69.0 (27.0%) | 20.0 (9.3%) | 9.0 (5.9%) | 4.0 (2.4%) | 102.0 (12.9%) | |
| Other | 1.0 (0.4%) | 0.0 (0.0%) | 0.0 (0.0%) | 3.0 (1.8%) | 4.0 (0.5%) | |
| SSA | 14.0 (5.5%) | 25.0 (11.6%) | 17.0 (11.1%) | 9.0 (5.5%) | 65.0 (8.2%) | |
| TA with HGD | 0.0 (0.0%) | 6.0 (2.8%) | 9.0 (5.9%) | 16.0 (9.7%) | 31.0 (3.9%) | |
| TA with LGD | 169.0 (66.0%) | 159.0 (73.6%) | 106.0 (69.3%) | 99.0 (60.0%) | 533.0 (67.5%) | |
| TVA with HGD | 0.0 (0.0%) | 2.0 (0.9%) | 3.0 (1.1%) | 18.0 (10.9%) | 23.0 (2.9%) | |
| TVA with LGD | 2.0 (0.8%) | 3.0 (1.4%) | 8.0 (5.2%) | 16.0 (9.7%) | 29.0 (3.7%) | |
| Inflammatory | 1.0 (0.4%) | 1.0 (0.5%) | 1.0 (0.7%) | 0.0 (0.0%) | 3.0 (0.4%) | |
| Location | 0.115 2 | |||||
| Right | 85.0 (33.2%) | 57.0 (26.4%) | 48.0 (31.4%) | 54.0 (32.7%) | 244.0 (30.9%) | |
| Left | 106.0 (41.4%) | 102.0 (47.2%) | 63.0 (41.2%) | 84.0 (50.9%) | 355.0 (44.9%) | |
| Transverse | 65.0 (25.4%) | 57.0 (26.4%) | 42.0 (27.5%) | 27.0 (16.4%) | 191.0 (24.2%) | |
| Paris | <0.001 2 | |||||
| IIa | 0.0 (0.0%) | 0.0 (0.0%) | 1.0 (0.7%) | 11.0 (6.7%) | 12.0 (1.5%) | |
| Ip | 0.0 (0.0%) | 2.0 (0.9%) | 14.0 (9.2%) | 66.0 (40.0%) | 82.0 (10.4%) | |
| Isp | 0.0 (0.0%) | 18.0 (8.3%) | 38.0 (24.8%) | 21.0 (12.7%) | 77.0 (9.7%) | |
| Is | 256.0 (100%) | 196.0 (90.7%) | 100.0 (65.3%) | 67.0 (40.6%) | 619.0 (78.4%) | |
| HGD present | <0.001 2 | |||||
| No | 256.0 (100%) | 208.0 (96.3%) | 141.0 (92.2%) | 131.0 (79.4%) | 736.0 (93.2%) | |
| Yes | 0.0 (0.0%) | 8.0 (3.7%) | 12.0 (7.8%) | 34.0 (20.6%) | 54.0 (6.8%) |
| Predictor | Estimate | SE | Z | p-Value | Odds Ratio | 95% CI—Lower | 95% CI—Upper |
|---|---|---|---|---|---|---|---|
| Intercept | −7.86 | 1.26 | −6.25 | <0.001 | 0.001 | 0.001 | 0.004 |
| Age | 0.05 | 0.02 | 2.71 | 0.01 | 1.05 | 1.01 | 1.08 |
| Size | |||||||
| >5 mm vs. ≤5 mm | 1.49 | 0.42 | 3.54 | <0.001 | 4.4 | 1.94 | 10.06 |
| Number of polyps | 0.16 | 0.08 | 2.04 | 0.04 | 1.18 | 1.00 | 1.39 |
| Paris: | |||||||
| IIa–Is | 1.8 | 0.7 | 2.58 | 0.01 | 6.05 | 1.54 | 23.73 |
| Ip–Is | 1.3 | 0.39 | 3.3 | <0.001 | 3.68 | 1.7 | 7.98 |
| Isp–Is | 0.99 | 0.42 | 2.36 | 0.02 | 2.7 | 1.18 | 6.19 |
| Gender | |||||||
| Male vs. female | 0.65 | 0.34 | 1.93 | 0.05 | 1.91 | 0.99 | 3.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Groza, A.L.; Miutescu, B.; Tefas, C.; Popa, A.; Ratiu, I.; Sirli, R.; Popescu, A.; Motofelea, A.C.; Tantau, M. Evaluating the Efficacy of Resect-and-Discard and Resect-and-Retrieve Strategies for Diminutive Colonic Polyps. Life 2024, 14, 532. https://doi.org/10.3390/life14040532
Groza AL, Miutescu B, Tefas C, Popa A, Ratiu I, Sirli R, Popescu A, Motofelea AC, Tantau M. Evaluating the Efficacy of Resect-and-Discard and Resect-and-Retrieve Strategies for Diminutive Colonic Polyps. Life. 2024; 14(4):532. https://doi.org/10.3390/life14040532
Chicago/Turabian StyleGroza, Andrei Lucian, Bogdan Miutescu, Cristian Tefas, Alexandru Popa, Iulia Ratiu, Roxana Sirli, Alina Popescu, Alexandru Catalin Motofelea, and Marcel Tantau. 2024. "Evaluating the Efficacy of Resect-and-Discard and Resect-and-Retrieve Strategies for Diminutive Colonic Polyps" Life 14, no. 4: 532. https://doi.org/10.3390/life14040532
APA StyleGroza, A. L., Miutescu, B., Tefas, C., Popa, A., Ratiu, I., Sirli, R., Popescu, A., Motofelea, A. C., & Tantau, M. (2024). Evaluating the Efficacy of Resect-and-Discard and Resect-and-Retrieve Strategies for Diminutive Colonic Polyps. Life, 14(4), 532. https://doi.org/10.3390/life14040532