
Hypoglossal Nerve Stimulation Therapy in a Belgian Cohort of Obstructive Sleep Apnea Patients

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
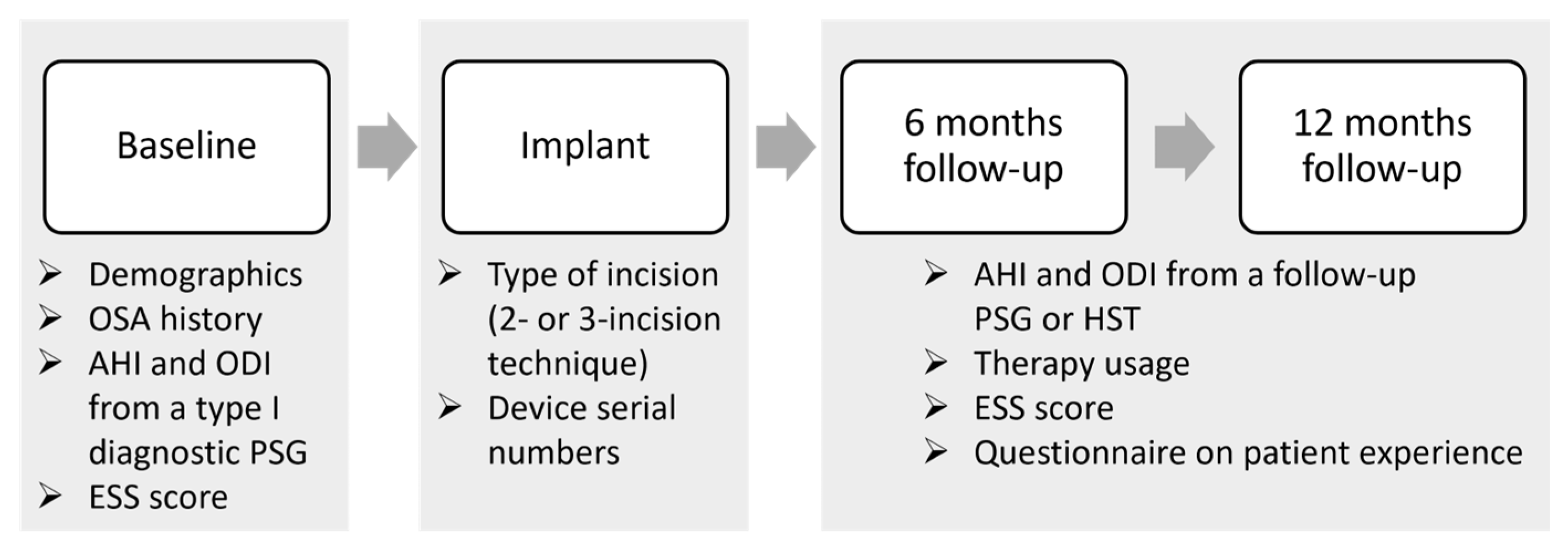
2.1. Study Design and Population
2.2. Hypoglossal Nerve Stimulation Therapy
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Study Population
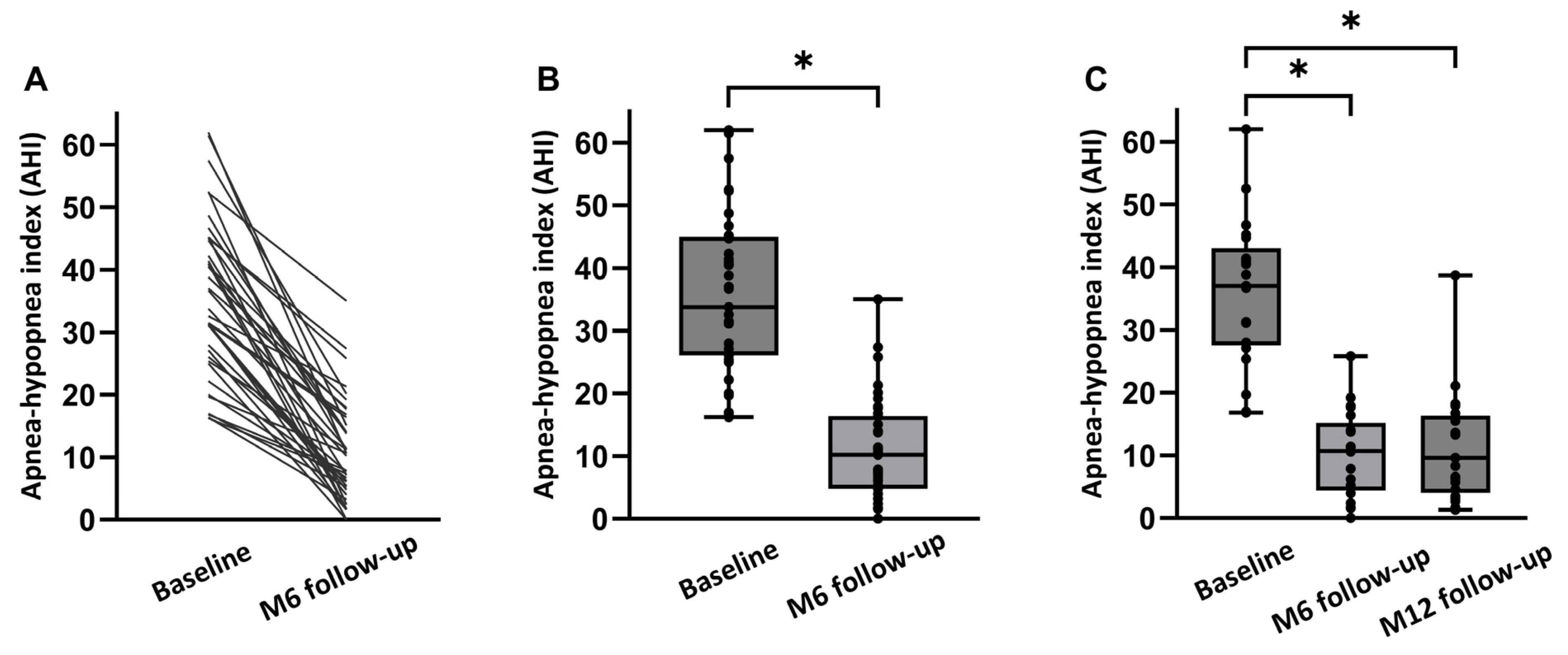
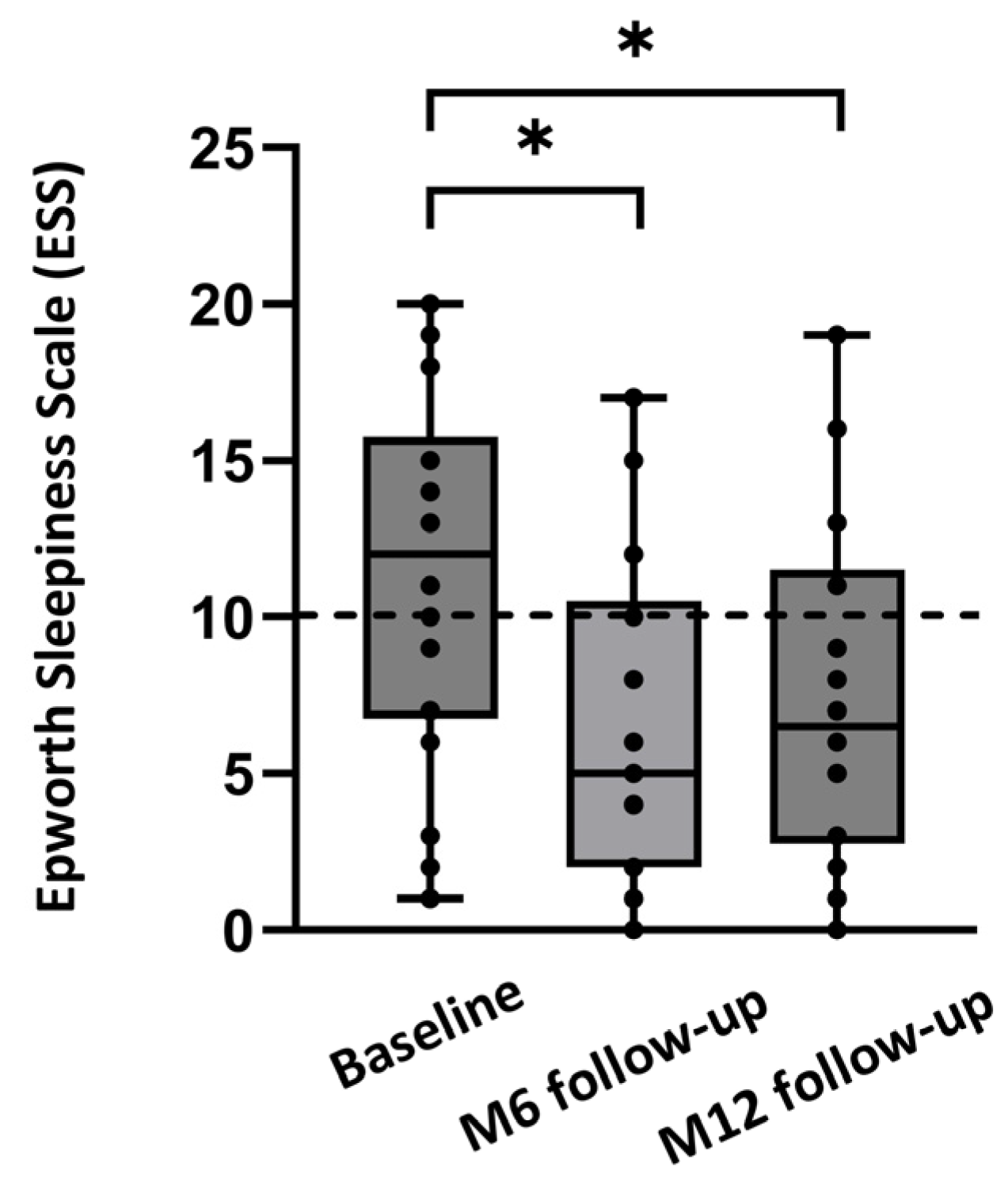
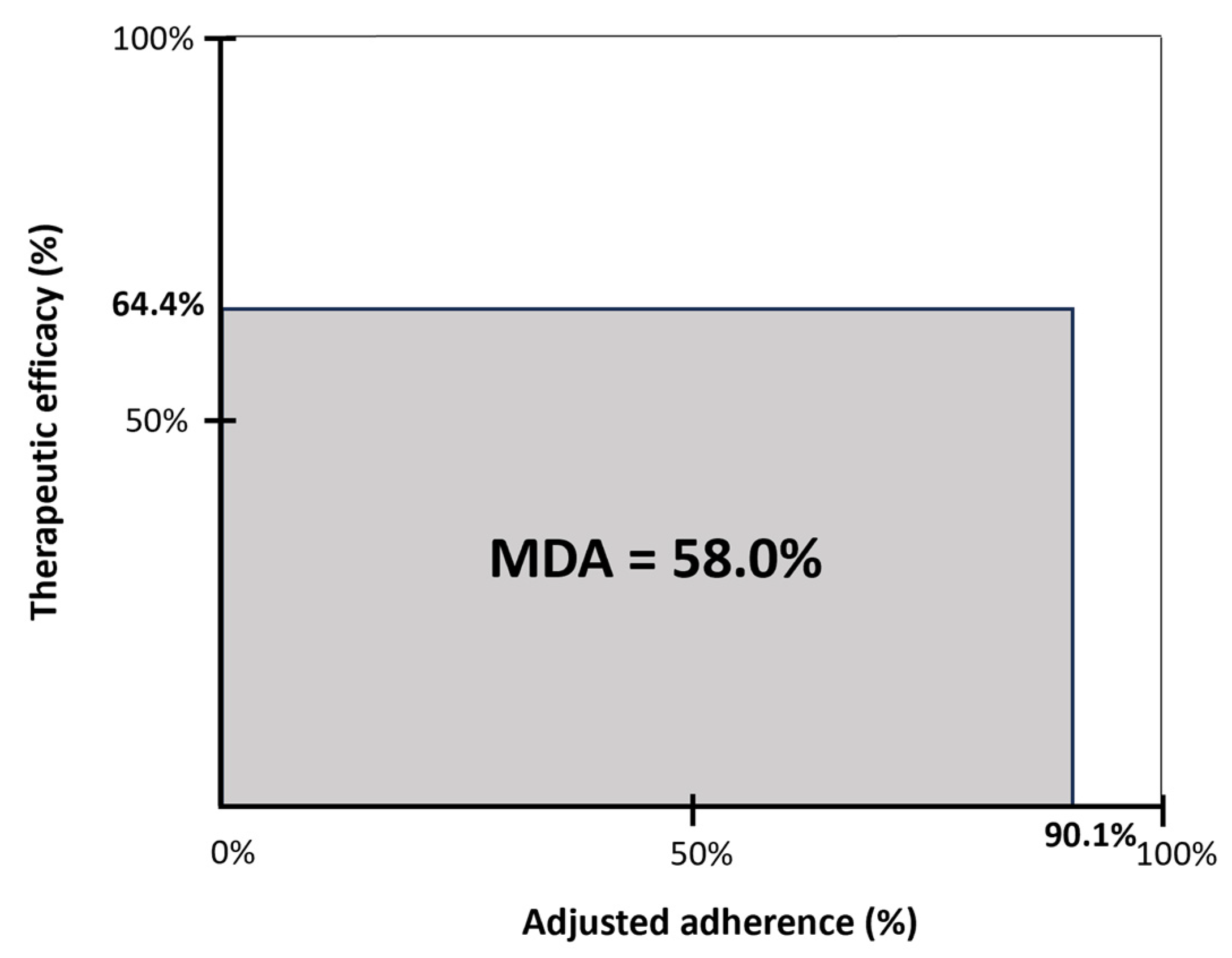
3.2. Outcome Measures at 6 Months Post-Implantation
3.3. Outcome Measures at 12 Months Post-Implantation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Remmers, J.E.; deGroot, W.J.; Sauerland, E.K.; Anch, A.M. Pathogenesis of upper airway occlusion during sleep. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1978, 44, 931–938. [Google Scholar] [CrossRef]
- Cheshire, K.; Engleman, H.; Deary, I.; Shapiro, C.; Douglas, N.J. Factors impairing daytime performance in patients with sleep apnea/hypopnea syndrome. Arch. Intern. Med. 1992, 152, 538–541. [Google Scholar] [CrossRef]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Blustein, J.; Finn, L.; Palta, M. Sleep-disordered breathing and motor vehicle accidents in a population-based sample of employed adults. Sleep 1997, 20, 608–613. [Google Scholar] [CrossRef]
- Peker, Y.; Hedner, J.; Norum, J.; Kraiczi, H.; Carlson, J. Increased incidence of cardiovascular disease in middle-aged men with obstructive sleep apnea: A 7-year follow-up. Am. J. Respir. Crit. Care Med. 2002, 166, 159–165. [Google Scholar] [CrossRef]
- Peker, Y.; Carlson, J.; Hedner, J. Increased incidence of coronary artery disease in sleep apnoea: A long-term follow-up. Eur. Respir. J. 2006, 28, 596–602. [Google Scholar] [CrossRef]
- Peppard, P.E.; Young, T.; Palta, M.; Skatrud, J. Prospective study of the association between sleep-disordered breathing and hypertension. N. Engl. J. Med. 2000, 342, 1378–1384. [Google Scholar] [CrossRef] [PubMed]
- Svedmyr, S.; Hedner, J.; Bailly, S.; Fanfulla, F.; Hein, H.; Lombardi, C.; Ludka, O.; Mihaicuta, S.; Parati, G.; Pataka, A.; et al. Blood pressure control in hypertensive sleep apnoea patients of the European Sleep Apnea Database cohort-effects of positive airway pressure and antihypertensive medication. Eur. Heart J. Open 2023, 3, oead109. [Google Scholar] [CrossRef]
- Tasbakan, M.S.; Grote, L.; Hedner, J.; Kvamme, J.A.; Verbraecken, J.; McNicholas, W.T.; Roisman, G.; Tkacova, R.; Bonsignore, M.R.; Saaresranta, T.; et al. Positive airway pressure (PAP) treatment reduces glycated hemoglobin (HbA1c) levels in obstructive sleep apnea patients with concomitant weight loss: Longitudinal data from the ESADA. J. Sleep Res. 2021, 30, e13331. [Google Scholar] [CrossRef]
- Labarca, G.; Saavedra, D.; Dreyse, J.; Jorquera, J.; Barbe, F. Efficacy of CPAP for Improvements in Sleepiness, Cognition, Mood, and Quality of Life in Elderly Patients With OSA: Systematic Review and Meta-analysis of Randomized Controlled Trials. Chest 2020, 158, 751–764. [Google Scholar] [CrossRef]
- Lin, H.J.; Yeh, J.H.; Hsieh, M.T.; Hsu, C.Y. Continuous positive airway pressure with good adherence can reduce risk of stroke in patients with moderate to severe obstructive sleep apnea: An updated systematic review and meta-analysis. Sleep Med. Rev. 2020, 54, 101354. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, C.E.; Issa, F.G.; Berthon-Jones, M.; Eves, L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet 1981, 1, 862–865. [Google Scholar] [CrossRef] [PubMed]
- Dieltjens, M.; Vanderveken, O. Oral Appliances in Obstructive Sleep Apnea. Healthcare 2019, 7, 141. [Google Scholar] [CrossRef] [PubMed]
- Randerath, W.; de Lange, J.; Hedner, J.; Ho, J.; Marklund, M.; Schiza, S.; Steier, J.; Verbraecken, J. Current and novel treatment options for obstructive sleep apnoea. ERJ Open Res. 2022, 8, 00126–2022. [Google Scholar] [CrossRef] [PubMed]
- Verbraecken, J.; Dieltjens, M.; Op de Beeck, S.; Vroegop, A.; Braem, M.; Vanderveken, O.; Randerath, W. Non-CPAP therapy for obstructive sleep apnoea. Breathe 2022, 18, 220164. [Google Scholar] [CrossRef] [PubMed]
- Randerath, W.J.; Verbraecken, J.; Andreas, S.; Bettega, G.; Boudewyns, A.; Hamans, E.; Jalbert, F.; Paoli, J.R.; Sanner, B.; Smith, I.; et al. Non-CPAP therapies in obstructive sleep apnoea. Eur. Respir. J. 2011, 37, 1000–1028. [Google Scholar] [CrossRef]
- Randerath, W.; Verbraecken, J.; de Raaff, C.A.L.; Hedner, J.; Herkenrath, S.; Hohenhorst, W.; Jakob, T.; Marrone, O.; Marklund, M.; McNicholas, W.T.; et al. European Respiratory Society guideline on non-CPAP therapies for obstructive sleep apnoea. Eur. Respir. Rev. 2021, 30, 210200. [Google Scholar] [CrossRef]
- Plaza, G.; Baptista, P.; O’Connor-Reina, C.; Bosco, G.; Perez-Martin, N.; Pang, K.P. Prospective multi-center study on expansion sphincter pharyngoplasty. Acta Otolaryngol. 2019, 139, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Iannella, G.; Lechien, J.R.; Perrone, T.; Meccariello, G.; Cammaroto, G.; Cannavicci, A.; Burgio, L.; Maniaci, A.; Cocuzza, S.; Di Luca, M.; et al. Barbed reposition pharyngoplasty (BRP) in obstructive sleep apnea treatment: State of the art. Am. J. Otolaryngol. 2022, 43, 103197. [Google Scholar] [CrossRef]
- Lin, H.C.; Friedman, M. Transoral robotic OSA surgery. Auris Nasus Larynx 2021, 48, 339–346. [Google Scholar] [CrossRef]
- Li, K.; Holey, J.E.; Guilleminault, C. Maxillomandibular Advancement for OSA: A 25-year perspective. Orthod. Fr. 2022, 93 (Suppl. S1), 97–108. [Google Scholar] [CrossRef] [PubMed]
- Beyers, J.; Dieltjens, M.; Kastoer, C.; Opdebeeck, L.; Boudewyns, A.N.; De Volder, I.; Van Gastel, A.; Verbraecken, J.A.; De Backer, W.A.; Braem, M.J.; et al. Evaluation of a Trial Period With a Sleep Position Trainer in Patients With Positional Sleep Apnea. J. Clin. Sleep Med. 2018, 14, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Camacho, M.; Certal, V.; Abdullatif, J.; Zaghi, S.; Ruoff, C.M.; Capasso, R.; Kushida, C.A. Myofunctional Therapy to Treat Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. Sleep 2015, 38, 669–675. [Google Scholar] [CrossRef]
- Taranto-Montemurro, L.; Messineo, L.; Sands, S.A.; Azarbarzin, A.; Marques, M.; Edwards, B.A.; Eckert, D.J.; White, D.P.; Wellman, A. The Combination of Atomoxetine and Oxybutynin Greatly Reduces Obstructive Sleep Apnea Severity. A Randomized, Placebo-controlled, Double-Blind Crossover Trial. Am. J. Respir. Crit. Care Med. 2019, 199, 1267–1276. [Google Scholar] [CrossRef]
- Strollo, P.J., Jr.; Soose, R.J.; Maurer, J.T.; de Vries, N.; Cornelius, J.; Froymovich, O.; Hanson, R.D.; Padhya, T.A.; Steward, D.L.; Gillespie, M.B.; et al. Upper-airway stimulation for obstructive sleep apnea. N. Engl. J. Med. 2014, 370, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Suurna, M.V.; Jacobowitz, O.; Chang, J.; Koutsourelakis, I.; Smith, D.; Alkan, U.; D’Agostino, M.; Boon, M.; Heiser, C.; Hoff, P.; et al. Improving outcomes of hypoglossal nerve stimulation therapy: Current practice, future directions, and research gaps. Proceedings of the 2019 International Sleep Surgery Society Research Forum. J. Clin. Sleep Med. 2021, 17, 2477–2487. [Google Scholar] [CrossRef]
- Strollo, P.J., Jr.; Gillespie, M.B.; Soose, R.J.; Maurer, J.T.; de Vries, N.; Cornelius, J.; Hanson, R.D.; Padhya, T.A.; Steward, D.L.; Woodson, B.T.; et al. Upper Airway Stimulation for Obstructive Sleep Apnea: Durability of the Treatment Effect at 18 Months. Sleep 2015, 38, 1593–1598. [Google Scholar] [CrossRef]
- Soose, R.J.; Woodson, B.T.; Gillespie, M.B.; Maurer, J.T.; de Vries, N.; Steward, D.L.; Strohl, K.P.; Baskin, J.Z.; Padhya, T.A.; Badr, M.S.; et al. Upper Airway Stimulation for Obstructive Sleep Apnea: Self-Reported Outcomes at 24 Months. J. Clin. Sleep Med. 2016, 12, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Woodson, B.T.; Soose, R.J.; Gillespie, M.B.; Strohl, K.P.; Maurer, J.T.; de Vries, N.; Steward, D.L.; Baskin, J.Z.; Badr, M.S.; Lin, H.S.; et al. Three-Year Outcomes of Cranial Nerve Stimulation for Obstructive Sleep Apnea: The STAR Trial. Otolaryngol. Head Neck Surg. 2016, 154, 181–188. [Google Scholar] [CrossRef]
- Gillespie, M.B.; Soose, R.J.; Woodson, B.T.; Strohl, K.P.; Maurer, J.T.; de Vries, N.; Steward, D.L.; Baskin, J.Z.; Badr, M.S.; Lin, H.S.; et al. Upper Airway Stimulation for Obstructive Sleep Apnea: Patient-Reported Outcomes after 48 Months of Follow-up. Otolaryngol. Head Neck Surg. 2017, 156, 765–771. [Google Scholar] [CrossRef]
- Woodson, B.T.; Strohl, K.P.; Soose, R.J.; Gillespie, M.B.; Maurer, J.T.; de Vries, N.; Padhya, T.A.; Badr, M.S.; Lin, H.S.; Vanderveken, O.M.; et al. Upper Airway Stimulation for Obstructive Sleep Apnea: 5-Year Outcomes. Otolaryngol. Head Neck Surg. 2018, 159, 194–202. [Google Scholar] [CrossRef]
- Boon, M.; Huntley, C.; Steffen, A.; Maurer, J.T.; Sommer, J.U.; Schwab, R.; Thaler, E.; Soose, R.; Chou, C.; Strollo, P.; et al. Upper Airway Stimulation for Obstructive Sleep Apnea: Results from the ADHERE Registry. Otolaryngol. Head Neck Surg. 2018, 159, 379–385. [Google Scholar] [CrossRef]
- Heiser, C.; Steffen, A.; Boon, M.; Hofauer, B.; Doghramji, K.; Maurer, J.T.; Sommer, J.U.; Soose, R.; Strollo, P.J., Jr.; Schwab, R.; et al. Post-approval upper airway stimulation predictors of treatment effectiveness in the ADHERE registry. Eur. Respir. J. 2019, 53, 1801405. [Google Scholar] [CrossRef]
- Thaler, E.; Schwab, R.; Maurer, J.; Soose, R.; Larsen, C.; Stevens, S.; Stevens, D.; Boon, M.; Huntley, C.; Doghramji, K.; et al. Results of the ADHERE upper airway stimulation registry and predictors of therapy efficacy. Laryngoscope 2020, 130, 1333–1338. [Google Scholar] [CrossRef]
- Suurna, M.V.; Steffen, A.; Boon, M.; Chio, E.; Copper, M.; Patil, R.D.; Green, K.; Hanson, R.; Heiser, C.; Huntley, C.; et al. Impact of Body Mass Index and Discomfort on Upper Airway Stimulation: ADHERE Registry 2020 Update. Laryngoscope 2021, 131, 2616–2624. [Google Scholar] [CrossRef] [PubMed]
- Steffen, A.; Sommer, J.U.; Hofauer, B.; Maurer, J.T.; Hasselbacher, K.; Heiser, C. Outcome after one year of upper airway stimulation for obstructive sleep apnea in a multicenter German post-market study. Laryngoscope 2018, 128, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Steffen, A.; Sommer, U.J.; Maurer, J.T.; Abrams, N.; Hofauer, B.; Heiser, C. Long-term follow-up of the German post-market study for upper airway stimulation for obstructive sleep apnea. Sleep Breath. 2020, 24, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Heiser, C.; Steffen, A.; Hofauer, B.; Mehra, R.; Strollo, P.J., Jr.; Vanderveken, O.M.; Maurer, J.T. Effect of Upper Airway Stimulation in Patients with Obstructive Sleep Apnea (EFFECT): A Randomized Controlled Crossover Trial. J. Clin. Med. 2021, 10, 2880. [Google Scholar] [CrossRef]
- Van de Heyning, P.H.; Badr, M.S.; Baskin, J.Z.; Cramer Bornemann, M.A.; De Backer, W.A.; Dotan, Y.; Hohenhorst, W.; Knaack, L.; Lin, H.S.; Maurer, J.T.; et al. Implanted upper airway stimulation device for obstructive sleep apnea. Laryngoscope 2012, 122, 1626–1633. [Google Scholar] [CrossRef]
- Vanderveken, O.M.; Maurer, J.T.; Hohenhorst, W.; Hamans, E.; Lin, H.S.; Vroegop, A.V.; Anders, C.; de Vries, N.; Van de Heyning, P.H. Evaluation of drug-induced sleep endoscopy as a patient selection tool for implanted upper airway stimulation for obstructive sleep apnea. J. Clin. Sleep Med. 2013, 9, 433–438. [Google Scholar] [CrossRef]
- Kent, D.T.; Chio, E.G.; Weiner, J.S.; Heiser, C.; Suurna, M.V.; Weidenbecher, M. A Noninferiority Analysis of 3- vs 2-Incision Techniques for Hypoglossal Nerve Stimulator Implantation. Otolaryngol. Head Neck Surg. 2022, 167, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Heiser, C.; Hofauer, B.; Lozier, L.; Woodson, B.T.; Stark, T. Nerve monitoring-guided selective hypoglossal nerve stimulation in obstructive sleep apnea patients. Laryngoscope 2016, 126, 2852–2858. [Google Scholar] [CrossRef] [PubMed]
- Heiser, C.; Thaler, E.; Boon, M.; Soose, R.J.; Woodson, B.T. Updates of operative techniques for upper airway stimulation. Laryngoscope 2016, 126 (Suppl. S7), S12–S16. [Google Scholar] [CrossRef] [PubMed]
- Vanderveken, O.M.; Beyers, J.; Op de Beeck, S.; Dieltjens, M.; Willemen, M.; Verbraecken, J.A.; De Backer, W.A.; Van de Heyning, P.H. Development of a Clinical Pathway and Technical Aspects of Upper Airway Stimulation Therapy for Obstructive Sleep Apnea. Front. Neurosci. 2017, 11, 523. [Google Scholar] [CrossRef] [PubMed]
- Soose, R.J.; Faber, K.; Greenberg, H.; Boon, M.; Woodson, T.; Strollo, P. Post-implant care pathway: Lessons learned and recommendations after 5 years of clinical implementation of hypoglossal nerve stimulation therapy. Sleep 2021, 44, S4–S10. [Google Scholar] [CrossRef] [PubMed]
- Sher, A.E.; Schechtman, K.B.; Piccirillo, J.F. The efficacy of surgical modifications of the upper airway in adults with obstructive sleep apnea syndrome. Sleep 1996, 19, 156–177. [Google Scholar] [CrossRef] [PubMed]
- Vanderveken, O.M.; Dieltjens, M.; Wouters, K.; De Backer, W.A.; Van de Heyning, P.H.; Braem, M.J. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax 2013, 68, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Heiser, C.; Steffen, A.; Strollo, P.J., Jr.; Giaie-Miniet, C.; Vanderveken, O.M.; Hofauer, B. Hypoglossal nerve stimulation versus positive airway pressure therapy for obstructive sleep apnea. Sleep Breath. 2023, 27, 693–701. [Google Scholar] [CrossRef]
- Bosschieter, P.F.N.; de Vries, N.; Mehra, R.; Manchanda, S.; Padhya, T.A.; Vanderveken, O.M.; Ravesloot, M.J.L.; Investigators, A.R. Similar effect of hypoglossal nerve stimulation for obstructive sleep apnea in 5 disease severity categories. J. Clin. Sleep Med. 2022, 18, 1657–1665. [Google Scholar] [CrossRef]
- Kent, D.; Huyett, P.; Yu, P.; Roy, A.; Mehra, R.; Rundo, J.V.; Stahl, S.; Manchanda, S. Comparison of clinical pathways for hypoglossal nerve stimulation management: In-laboratory titration polysomnography vs home-based efficacy sleep testing. J. Clin. Sleep Med. 2023, 19, 1905–1912. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Age (years) | 55.0 ± 11.9 |
| Gender (% male) | 79% |
| BMI (kg/m2) | 27.5 ± 2.8 |
| Systolic blood pressure (mmHg) | 131.6 ± 16.3 |
| Diastolic blood pressure (mmHg) | 82.7 ± 11.1 |
| AHI (events/h) | 33.8 [26.1;45.0] |
| ODI ≥ 3% (events/h) | 24.9 [12.9;31.2] |
| ESS score | 11.0 [7.0;18.0] |
| Parameter | Baseline | Month 6 | Change | p-Value |
|---|---|---|---|---|
| BMI (kg/m2) | 27.5 ± 2.8 | 27.3 ± 2.8 | - | >0.05 |
| AHI (events/h) | 33.8 [26.1;45.0] | 10.2 [4.8;16.4] | −23.6 [−32.7;−14.9] | <0.001 |
| ODI ≥ 3% (events/h) | 25.5 [12.2;31.5] | 7.9 [5.2;16.7] | −14.0 [−20.8;−3.9] | <0.001 |
| ESS | 12.0 [7.0;18.0] | 6.0 [2.5;11.0] | −5.0 [−8.5;−1.0] | <0.001 |
| Therapy usage (h/night) | - | 7.4 [6.6;8.0] | - | - |
| Parameter | Baseline | Month 12 | Change | p-Value |
|---|---|---|---|---|
| BMI (kg/m2) | 27.5 ± 2.8 | 27.1 ± 3.5 | - | >0.05 |
| AHI (events/h) | 37.0 [27.6;43.1] | 9.6 [4.1;16.4] | −24.8 [−32.2;−16.5] | <0.001 |
| ODI ≥ 3% (events/h) | 28.1 [19.4;33.8] | 15.9 [3.9;21.7] | −11.7 [−18.6;−3.1] | <0.001 |
| ESS | 12.0 [6.8;15.8] | 6.5 [2.8;11.5] | −3.0 [−9.3;−1.0] | 0.012 |
| Therapy usage (h/night) | - | 7.0 [5.9;8.2] | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Loo, D.; Dieltjens, M.; Engelen, S.; Verbraecken, J.; Vanderveken, O.M. Hypoglossal Nerve Stimulation Therapy in a Belgian Cohort of Obstructive Sleep Apnea Patients. Life 2024, 14, 788. https://doi.org/10.3390/life14070788
Van Loo D, Dieltjens M, Engelen S, Verbraecken J, Vanderveken OM. Hypoglossal Nerve Stimulation Therapy in a Belgian Cohort of Obstructive Sleep Apnea Patients. Life. 2024; 14(7):788. https://doi.org/10.3390/life14070788
Chicago/Turabian StyleVan Loo, Dorine, Marijke Dieltjens, Sanne Engelen, Johan Verbraecken, and Olivier M. Vanderveken. 2024. "Hypoglossal Nerve Stimulation Therapy in a Belgian Cohort of Obstructive Sleep Apnea Patients" Life 14, no. 7: 788. https://doi.org/10.3390/life14070788
APA StyleVan Loo, D., Dieltjens, M., Engelen, S., Verbraecken, J., & Vanderveken, O. M. (2024). Hypoglossal Nerve Stimulation Therapy in a Belgian Cohort of Obstructive Sleep Apnea Patients. Life, 14(7), 788. https://doi.org/10.3390/life14070788