

Predictors of Outcomes and a Weighted Mortality Score for Moderate to Severe Subdural Hematoma

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Patient Selection
2.2. Data Items
2.3. Statistical Analysis
2.4. Data Availability
3. Results
3.1. Cohort Characteristics
3.2. Predictors of Mortality in Patients with Subdural Hematoma
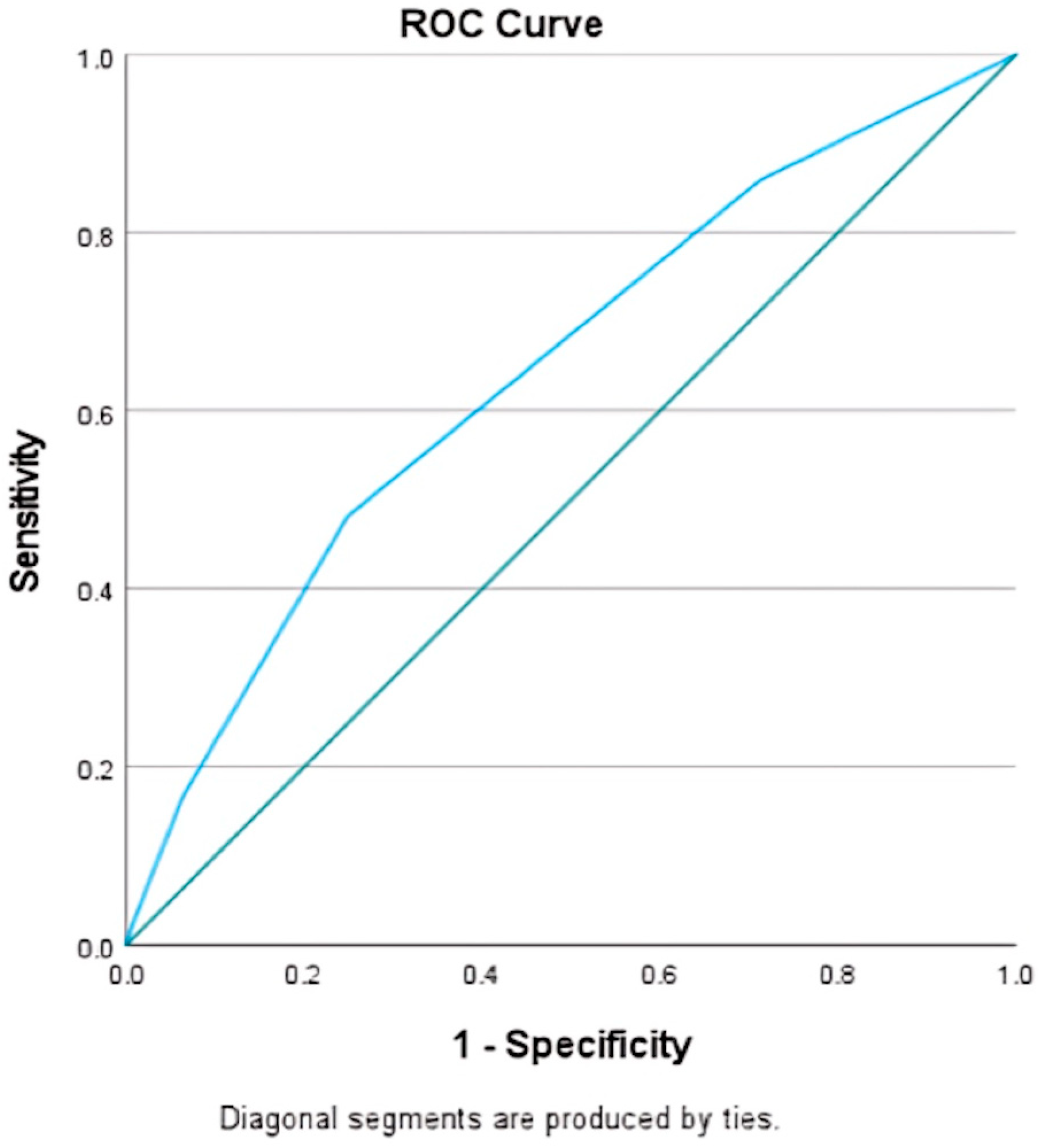
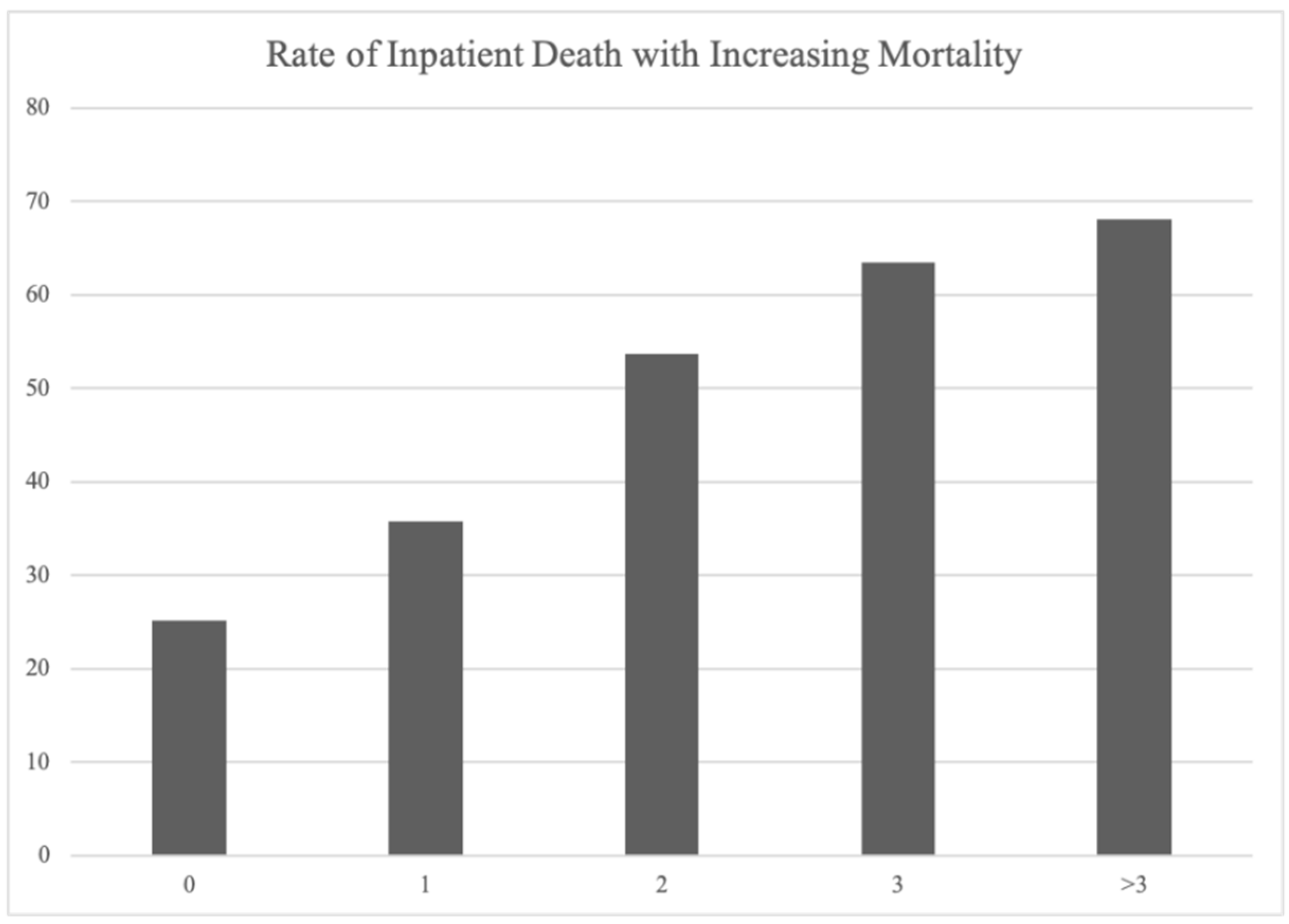
3.3. Moderate-to-Severe Subdural Hematoma Mortality Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ducruet, A.F.; Grobelny, B.T.; Zacharia, B.E.; Hickman, Z.L.; DeRosa, P.L.; Anderson, K.; Sussman, E.; Carpenter, A.; Connolly, E.S. The surgical management of chronic subdural hematoma. Neurosurg. Rev. 2012, 35, 155–169. [Google Scholar] [CrossRef]
- Feghali, J.; Yang, W.; Huang, J. Updates in Chronic Subdural Hematoma: Epidemiology, Etiology, Pathogenesis, Treatment, and Outcome. World Neurosurg. 2020, 141, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Rauhala, M.; Helén, P.; Huhtala, H.; Heikkilä, P.; Iverson, G.L.; Niskakangas, T.; Öhman, J.; Luoto, T.M. Chronic subdural hematoma—Incidence, complications, and financial impact. Acta Neurochir. 2020, 162, 2033–2043. [Google Scholar] [CrossRef] [PubMed]
- Cenic, A.; Bhandari, M.; Reddy, K. Management of chronic subdural hematoma: A national survey and literature review. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2005, 32, 501–506. [Google Scholar] [CrossRef]
- Sastry, R.A.; Pertsch, N.; Tang, O.; Shao, B.; Toms, S.A.; Weil, R.J. Frailty and Outcomes after Craniotomy or Craniectomy for Atraumatic Chronic Subdural Hematoma. World Neurosurg. 2020, 145, e242–e251. [Google Scholar] [CrossRef]
- Weigel, R.; Schilling, L.; Krauss, J.K. The pathophysiology of chronic subdural hematoma revisited: Emphasis on aging processes as key factor. GeroScience 2022, 44, 1353–1371. [Google Scholar] [CrossRef] [PubMed]
- Sahyouni, R.; Goshtasbi, K.; Mahmoodi, A.; Tran, D.K.; Chen, J.W. Chronic Subdural Hematoma: A Historical and Clinical Perspective. World Neurosurg. 2017, 108, 948–953. [Google Scholar] [CrossRef]
- Markwalder, T.-M. The course of chronic subdural hematomas after burr-hole craniostomy with and without closed-system drainage. Neurosurg. Clin. N. Am. 2000, 11, 541–546. [Google Scholar] [CrossRef]
- Nouri, A.; Gondar, R.; Schaller, K.; Meling, T. Chronic Subdural Hematoma (cSDH): A review of the current state of the art. Brain Spine 2021, 1, 100300. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-I.; Lee, J.-H.; Park, S.-W.; Nam, T.-K.; Min, B.-K.; Hwang, S.-N. Analysis of Prognostic Factors for Chronic Subdural Hematoma. J. Korean Neurotraumatol. Soc. 2008, 4, 14–18. [Google Scholar] [CrossRef]
- Kwon, C.-S.; Al-Awar, O.; Richards, O.; Izu, A.; Lengvenis, G. Predicting Prognosis of Patients with Chronic Subdural Hematoma: A New Scoring System. World Neurosurg. 2018, 109, e707–e714. [Google Scholar] [CrossRef]
- Rozzelle, C.J.; Wofford, J.L.; Branch, C.L. Predictors of hospital mortality in older patients with subdural hematoma. J. Am. Geriatr. Soc. 1995, 43, 240–244. [Google Scholar] [CrossRef]
- Alford, E.N.; Rotman, L.E.; Erwood, M.S.; Oster, R.A.; Davis, M.C.; Pittman, H.B.C.; Zeiger, H.E.; Fisher, W.S. Development of the Subdural Hematoma in the Elderly (SHE) score to predict mortality. J. Neurosurg. 2019, 132, 1616–1622. [Google Scholar] [CrossRef] [PubMed]
- Stanišić, M.; Pripp, A.H. A Reliable Grading System for Prediction of Chronic Subdural Hematoma Recurrence Requiring Reoperation After Initial Burr-Hole Surgery. Neurosurgery 2017, 81, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Weimer, J.M.; Gordon, E.; Frontera, J.A. Predictors of Functional Outcome After Subdural Hematoma: A Prospective Study. Neurocrit. Care 2017, 26, 70–79. [Google Scholar] [CrossRef]
- Schneck, M.J.; Maheswaran, M.; Leurgans, S. Predictors of outcomes after nontraumatic subdural hematoma. J. Stroke Cerebrovasc. Dis. 2004, 13, 192–195. [Google Scholar] [CrossRef]
- Wang, S.; Ma, Y.; Zhao, X.; Yang, C.; Gu, J.; Weng, W.; Hui, J.; Mao, Q.; Gao, G.; Feng, J. Risk factors of hospital mortality in chronic subdural hematoma: A retrospective analysis of 1117 patients, a single institute experience. J. Clin. Neurosci. 2019, 67, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Bartek, J.; Sjåvik, K.; Dhawan, S.; Sagberg, L.M.; Kristiansson, H.; Ståhl, F.; Förander, P.; Chen, C.C.; Jakola, A.S. Clinical Course in Chronic Subdural Hematoma Patients Aged 18–49 Compared to Patients 50 Years and Above: A Multicenter Study and Meta-Analysis. Front. Neurol. 2019, 10, 311. [Google Scholar] [CrossRef]
- Abe, Y.; Maruyama, K.; Yokoya, S.; Noguchi, A.; Sato, E.; Nagane, M.; Shiokawa, Y. Outcomes of chronic subdural hematoma with preexisting comorbidities causing disturbed consciousness. J. Neurosurg. 2017, 126, 1042–1046. [Google Scholar] [CrossRef]
- Link, T.W.; Schwarz, J.T.; Paine, S.M.; Kamel, H.; Knopman, J. Middle Meningeal Artery Embolization for Recurrent Chronic Subdural Hematoma: A Case Series. World Neurosurg. 2018, 118, e570–e574. [Google Scholar] [CrossRef]
- Hanif, H.; Farook, S.; Suriya, S.S.; Gondal, M.U.R.; Bilal, M.I.; Sheikh, A.B. Middle Meningeal Artery Embolization: A Paradigm Shift in Approach of Chronic Subdural Hematoma. J. Community Hosp. Intern. Med. Perspect. 2022, 12, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Oishi, M.; Toyama, M.; Tamatani, S.; Kitazawa, T.; Saito, M. Clinical Factors of Recurrent Chronic Subdural Hematoma. Neurol. Med. Chir. 2001, 41, 382–386. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Total (29,915) | Discharged (17,780, 59.4%) | Inpatient Death (12,135, 40.6%) | OR (95% CI) | p Value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age > 70 | 10,860 (36.3%) | 5165 (29%) | 5695 (46.9%) | 2.16 (2.06–2.27) | <0.001 |
| Female | 10,550 (35.3%) | 6085 (34.2%) | 4465 (36.8%) | 1.12 (1.07–1.17) | <0.001 |
| Caucasian | 17,735 (59.3%) | 10,260 (57.7%) | 7475 (61.6%) | 1.18 (1.12–1.23) | <0.001 |
| Public Insurance | 19,125 (63.9%) | 10,970 (61.7%) | 8155 (67.2%) | 1.27 (1.21–1.34) | <0.001 |
| Clinical Comorbidities | |||||
| Long-term Anticoagulation | 3630 (12.1%) | 1505 (8.5%) | 2125 (17.5%) | 2.30 (2.14–2.46) | <0.001 |
| Diabetes mellitus | 4475 (15%) | 2270 (12.8%) | 2205 (18.2%) | 1.52 (1.42–1.62) | <0.001 |
| Hyperlipidemia | 4655 (15.6%) | 2640 (14.8%) | 2015 (16.6%) | 1.14 (1.07–1.22) | <0.001 |
| Hypertension | 10,630 (35.5%) | 6220 (35%) | 4410 (36.3%) | 1.06 (1.01–1.11) | <0.001 |
| Obesity | 825 (2.8%) | 455 (2.6%) | 370 (3%) | 1.20 (1.04–1.38) | <0.001 |
| Clinical Characteristics | |||||
| Hyponatremia | 3255 (10.9%) | 2460 (13.8%) | 795 (6.6%) | 0.44 (0.40–0.48) | <0.001 |
| Cardiac Arrest | 1230 (4.1%) | 135 (0.8%) | 1095 (9%) | 12.96 (10.82–15.57) | <0.001 |
| Seizures | 2295 (7.7%) | 1705 (9.6%) | 590 (4.9%) | 0.48 (0.44–0.53) | <0.001 |
| Clinical Severity Variables | |||||
| Mechanical Ventilation | 13,935 (46.6%) | 7785 (43.8%) | 6150 (50.7%) | 1.32 (1.26–1.38) | <0.001 |
| Hydrocephalus | 740 (2.5%) | 370 (2.1%) | 370 (3%) | 1.48 (1.28–1.71) | <0.001 |
| Herniation | 6955 (23.2%) | 2780 (15.6%) | 4175 (34.4%) | 2.83 (2.68–2.99) | <0.001 |
| Hemiplegia | 2700 (9%) | 2040 (11.5%) | 660 (5.4%) | 0.44 (0.41–0.49) | <0.001 |
| Aphasia | 1670 (5.6%) | 1425 (8%) | 245 (2%) | 0.24 (0.21–0.27) | <0.001 |
| Variable | OR (95% CI) | p Value |
|---|---|---|
| Female | 0.95 (0.90–0.99) | 0.032 |
| Age > 70 | 2.24 (2.12–2.36) | <0.001 |
| Caucasian | 1.02 (0.97–1.07) | 0.387 |
| Public Insurance | 0.92 (0.88–0.98) | <0.001 |
| Q1 Median Income | 0.96 (0.91–1.01) | 0.114 |
| Variable | OR (95% CI) | p Value |
|---|---|---|
| Long-term anticoagulation | 2.08 (1.97–2.20) | <0.001 |
| Diabetes Mellitus | 1.66 (1.54–1.79) | <0.001 |
| Hyperlipidemia | 0.81 (0.75–0.87) | <0.001 |
| Hypertension | 0.84 (0.80–0.89) | <0.001 |
| Obesity | 1.12 (0.97–1.30) | 0.137 |
| Mechanical Ventilation | 1.44 (1.37–1.52) | <0.001 |
| Hydrocephalus | 1.28 (1.09–1.49) | <0.001 |
| External ventricular drain | 0.93 (0.85–1.02) | 0.111 |
| Hyponatremia | 0.45 (0.41–0.49) | <0.001 |
| Herniation | 2.64 (2.50–2.80) | <0.001 |
| Non-epileptic Seizure | 0.51 (0.46–0.56) | <0.001 |
| Status Epilepticus | 0.78 (0.61–0.99) | 0.043 |
| B Coefficient | OR (95% CI) | p Value | Weighted Coefficient | |
|---|---|---|---|---|
| Female | −0.05 | 0.90 (0.90–1.00) | 0.061 | |
| Age > 70 | 0.84 | 2.32 (2.19–2.47) | <0.001 | 1 |
| Public Insurance | −0.09 | 0.91 (0.86–0.96) | <0.001 | |
| Long Term Steroids | −0.34 | 0.71 (0.53–0.95) | 0.022 | |
| Diabetes mellitus | 0.23 | 1.26 (1.17–1.35) | <0.001 | 1 |
| Hyperlipidemia | −0.19 | 0.82 (0.77–0.89) | <0.001 | |
| Hypertension | −0.18 | 0.84 (0.80–0.89) | <0.001 | |
| Mechanical Ventilation | 0.36 | 1.44 (1.37–1.51) | <0.001 | 1 |
| Hydrocephalus | 0.24 | 1.27 (1.09–1.49) | <0.001 | 1 |
| Hyponatremia | −0.80 | 0.45 (0.41–0.49) | <0.001 | |
| Herniation | 0.99 | 2.69 (2.54–2.85) | <0.001 | 1 |
| Seizures | −0.68 | 0.51 (0.46–0.56) | <0.001 | |
| Status Epilepticus | −0.23 | 0.79 (0.62–1.01) | 0.064 |
| Variable | Coefficient |
|---|---|
| Age > 70 | 1 |
| Diabetes mellitus | 1 |
| Mechanical Ventilation | 1 |
| Hydrocephalus | 1 |
| Herniation | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vazquez, S.; Jain, A.K.; Nolan, B.; Spirollari, E.; Clare, K.; Thomas, A.; Soldozy, S.; Ali, S.; Sukul, V.; Rosenberg, J.; et al. Predictors of Outcomes and a Weighted Mortality Score for Moderate to Severe Subdural Hematoma. Life 2024, 14, 1049. https://doi.org/10.3390/life14081049
Vazquez S, Jain AK, Nolan B, Spirollari E, Clare K, Thomas A, Soldozy S, Ali S, Sukul V, Rosenberg J, et al. Predictors of Outcomes and a Weighted Mortality Score for Moderate to Severe Subdural Hematoma. Life. 2024; 14(8):1049. https://doi.org/10.3390/life14081049
Chicago/Turabian StyleVazquez, Sima, Aarti K. Jain, Bridget Nolan, Eris Spirollari, Kevin Clare, Anish Thomas, Sauson Soldozy, Syed Ali, Vishad Sukul, Jon Rosenberg, and et al. 2024. "Predictors of Outcomes and a Weighted Mortality Score for Moderate to Severe Subdural Hematoma" Life 14, no. 8: 1049. https://doi.org/10.3390/life14081049
APA StyleVazquez, S., Jain, A. K., Nolan, B., Spirollari, E., Clare, K., Thomas, A., Soldozy, S., Ali, S., Sukul, V., Rosenberg, J., Mayer, S., Khatri, R., Jankowitz, B. T., Singer, J., Gandhi, C., & Al-Mufti, F. (2024). Predictors of Outcomes and a Weighted Mortality Score for Moderate to Severe Subdural Hematoma. Life, 14(8), 1049. https://doi.org/10.3390/life14081049