
Evaluating the Role of Susceptibility Inducing Cofactors and of Acetaminophen in the Etiology of Autism Spectrum Disorder


Abstract
:1. Introduction
1.1. An Actual Rise in the Prevalence of ASD
“What is the reason for the high (1 in 645) prevalence rates? We doubt that differences in diagnostic criteria and survey methods account for these high rates, although such factors may explain the large differences between the studies done between 1966 and 1980 and the studies done since 1983. In fact, the earlier studies were carefully performed using good survey methods. Although in some studies the diagnostic criteria may have been different, the diagnostic criteria were similar in the study by Hoshino et al. (Fukushima J Med Sci 1979;26:31-42.) and in our study, and both studies were done in Japan in similar cultural, ethnic, and socioeconomic regions. However, our prevalence is three times that of Hoshino et al. Could the real prevalence of autism be increasing in the world?”
“…it was not possible to account entirely for the effect of the diagnostic criteria on the prevalence estimates as the ICD-10 and DSM-IV diagnostic schema leave some scope for variation in their interpretation and application.”
“If MMR and thimerosal [factors related to vaccination] aren’t responsible, what’s the causative factor for autism? The simple answer is that it is not known.”
1.2. Fetal Alcohol Spectrum Disorder as Another Example of an Analgesic-Mediated Spectrum of Developmental Injury
1.3. The Metabolism of Acetaminophen and the Etiology of ASD
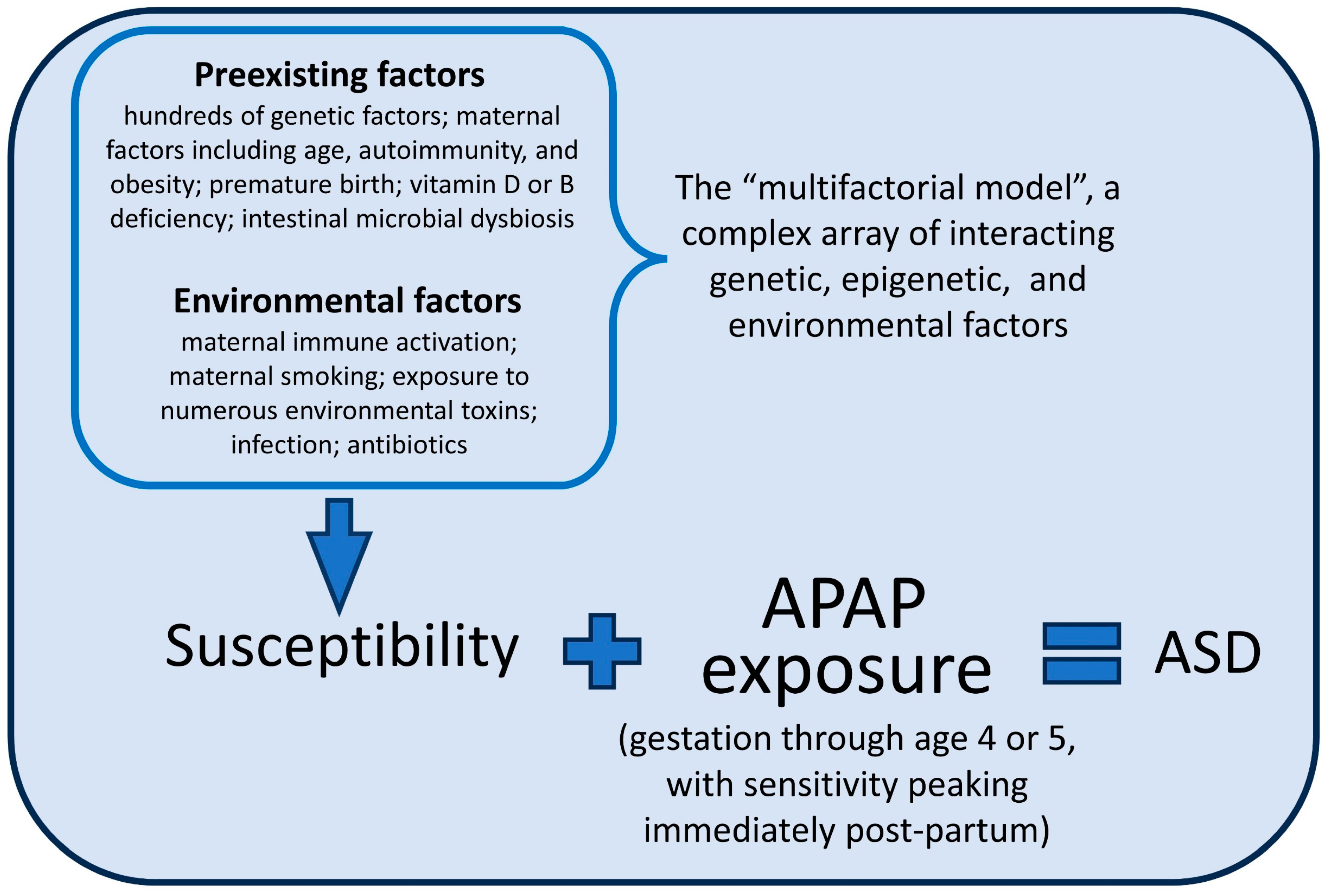
1.4. The Weight of Evidence and the Role of Acetaminophen in the Etiology of ASD
1.5. Multivariate Analysis of Cohort Data: Assessment of Methods by an In Silico Study
2. Materials and Methods
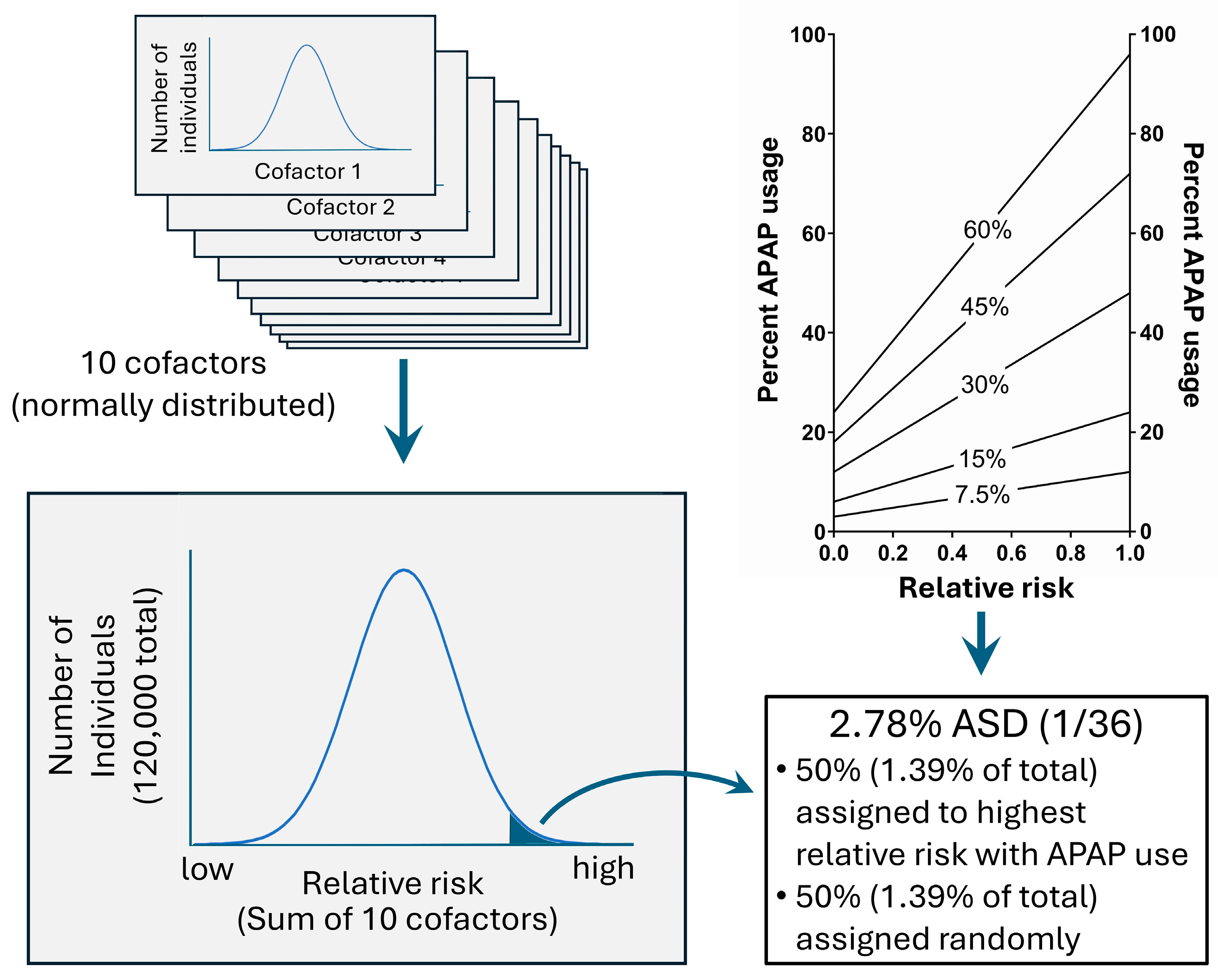
In Silico Evaluation of the Cox Regression Model
3. Results
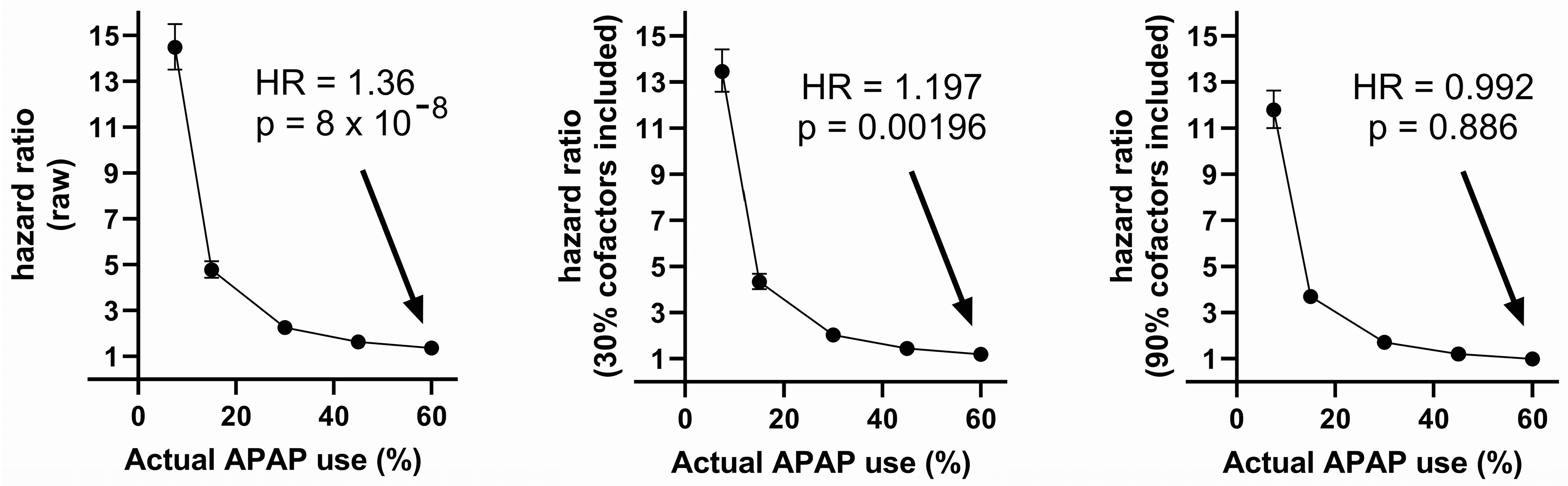
3.1. The Effect of Treating Cofactors (Predisposing Factors) as Confounding Factors in a Cox Regression Analysis
3.2. The Effects of Under-Reported Acetaminophen Use during Pregnancy in a Cox Regression Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, E.; Jones, J.P., 3rd; Bono-Lunn, D.; Kuchibhatla, M.; Palkar, A.; Cendejas Hernandez, J.; Sarafian, J.T.; Lawton, V.G.; Anderson, L.G.; Konsoula, Z.; et al. The safety of pediatric use of paracetamol (acetaminophen): A narrative review of direct and indirect evidence. Minerva Pediatr. 2022, 74, 774–788. [Google Scholar] [CrossRef]
- Zhao, L.; Jones, J.; Anderson, L.; Konsoula, Z.; Nevison, C.; Reissner, K.; Parker, W. Acetaminophen causes neurodevelopmental injury in susceptible babies and children: No valid rationale for controversy. Clin. Exp. Pediatr. 2023, 67, 126. [Google Scholar] [CrossRef]
- Parker, W.; Anderson, L.G.; Jones, J.P.; Anderson, R.; Williamson, L.; Bono-Lunn, D.; Konsoula, Z. The Dangers of Acetaminophen for Neurodevelopment Outweigh Scant Evidence for Long-Term Benefits. Children 2024, 11, 44. [Google Scholar] [CrossRef]
- Schultz, S.T.; Klonoff-Cohen, H.S.; Wingard, D.L.; Akshoomoff, N.A.; Macera, C.A.; Ji, M. Acetaminophen (paracetamol) use, measles-mumps-rubella vaccination, and autistic disorder. The results of a parent survey. Autism 2008, 12, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Freed, G.L.; Clark, S.J.; Butchart, A.T.; Singer, D.C.; Davis, M.M. Parental vaccine safety concerns in 2009. Pediatrics 2010, 125, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, A.; Zeldin, A.; Schuster, E.; Barrett, C.; Lehrer, D. Vaccine-related beliefs and practices of parents of children with autism spectrum disorders. Am. J. Intellect. Dev. Disabil. 2012, 117, 233–242. [Google Scholar] [CrossRef]
- Ji, Y.; Azuine, R.E.; Zhang, Y.; Hou, W.; Hong, X.; Wang, G.; Riley, A.; Pearson, C.; Zuckerman, B.; Wang, X. Association of Cord Plasma Biomarkers of In Utero Acetaminophen Exposure with Risk of Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in Childhood. JAMA Psychiatry 2020, 77, 180–189. [Google Scholar] [CrossRef]
- Frisch, M.; Simonsen, J. Ritual circumcision and risk of autism spectrum disorder in 0- to 9-year-old boys: National cohort study in Denmark. J. R. Soc. Med. 2015, 108, 266–279. [Google Scholar] [CrossRef] [PubMed]
- Durso, G.R.O.; Luttrell, A.; Way, B.M. Over-the-Counter Relief from Pains and Pleasures Alike: Acetaminophen Blunts Evaluation Sensitivity to Both Negative and Positive Stimuli. Psychol. Sci. 2015, 26, 750–758. [Google Scholar] [CrossRef]
- Dewall, C.N.; Macdonald, G.; Webster, G.D.; Masten, C.L.; Baumeister, R.F.; Powell, C.; Combs, D.; Schurtz, D.R.; Stillman, T.F.; Tice, D.M.; et al. Acetaminophen reduces social pain: Behavioral and neural evidence. Psychol. Sci. 2010, 21, 931–937. [Google Scholar] [CrossRef]
- Roberts, I.D.; Krajbich, I.; Way, B.M. Acetaminophen influences social and economic trust. Sci. Rep. 2019, 9, 4060. [Google Scholar] [CrossRef] [PubMed]
- Cendejas-Hernandez, J.; Sarafian, J.; Lawton, V.; Palkar, A.; Anderson, L.; Lariviere, V.; Parker, W. Paracetamol (Acetaminophen) Use in Infants and Children was Never Shown to be Safe for Neurodevelopment: A Systematic Review with Citation Tracking. Eur. J. Pediatr. 2022, 181, 1835–1857. [Google Scholar] [CrossRef]
- Hinz, B.; Cheremina, O.; Brune, K. Acetaminophen (paracetamol) is a selective cyclooxygenase-2 inhibitor in man. FASEB J. 2008, 22, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Hogestatt, E.D.; Jonsson, B.A.; Ermund, A.; Andersson, D.A.; Bjork, H.; Alexander, J.P.; Cravatt, B.F.; Basbaum, A.I.; Zygmunt, P.M. Conversion of acetaminophen to the bioactive N-acylphenolamine AM404 via fatty acid amide hydrolase-dependent arachidonic acid conjugation in the nervous system. J. Biol. Chem. 2005, 280, 31405–31412. [Google Scholar] [CrossRef] [PubMed]
- Ottani, A.; Leone, S.; Sandrini, M.; Ferrari, A.; Bertolini, A. The analgesic activity of paracetamol is prevented by the blockade of cannabinoid CB1 receptors. Eur. J. Pharmacol. 2006, 531, 280–281. [Google Scholar] [CrossRef] [PubMed]
- Viberg, H.; Eriksson, P.; Gordh, T.; Fredriksson, A. Paracetamol (Acetaminophen) Administration During Neonatal Brain Development Affects Cognitive Function and Alters Its Analgesic and Anxiolytic Response in Adult Male Mice. Toxicol. Sci. 2013, 138, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Herrington, J.A.; Guss Darwich, J.; Harshaw, C.; Brigande, A.M.; Leif, E.B.; Currie, P.J. Elevated ghrelin alters the behavioral effects of perinatal acetaminophen exposure in rats. Dev. Psychobiol. 2022, 64, e22252. [Google Scholar] [CrossRef] [PubMed]
- Harshaw, C.; Warner, A.G. Interleukin-1β-induced inflammation and acetaminophen during infancy: Distinct and interactive effects on social-emotional and repetitive behavior in C57BL/6J mice. Pharmacol. Biochem. Behav. 2022, 220, 173463. [Google Scholar] [CrossRef]
- Philippot, G.; Gordh, T.; Fredriksson, A.; Viberg, H. Adult neurobehavioral alterations in male and female mice following developmental exposure to paracetamol (acetaminophen): Characterization of a critical period. J. Appl. Toxicol. 2017, 37, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Suda, N.; Hernandez, J.C.; Poulton, J.; Jones, J.P.; Konsoula, Z.; Smith, C.; Parker, W. Therapeutic doses of paracetamol with co-administration of cysteine and mannitol during early development result in long term behavioral changes in laboratory rats. PLoS ONE 2020, 16, e0253543. [Google Scholar] [CrossRef]
- Blecharz-Klin, K.; Wawer, A.; Jawna-Zboińska, K.; Pyrzanowska, J.; Piechal, A.; Mirowska-Guzel, D.; Widy-Tyszkiewicz, E. Early paracetamol exposure decreases brain-derived neurotrophic factor (BDNF) in striatum and affects social behaviour and exploration in rats. Pharmacol. Biochem. Behav. 2018, 168, 25–32. [Google Scholar] [CrossRef]
- Baker, B.H.; Rafikian, E.E.; Hamblin, P.B.; Strait, M.D.; Yang, M.; Pearson, B.L. Sex-specific neurobehavioral and prefrontal cortex gene expression alterations following developmental acetaminophen exposure in mice. Neurobiol. Dis. 2023, 177, 105970. [Google Scholar] [CrossRef]
- Dean, S.L.; Knutson, J.F.; Krebs-Kraft, D.L.; McCarthy, M.M. Prostaglandin E2 is an endogenous modulator of cerebellar development and complex behavior during a sensitive postnatal period. Eur. J. Neurosci. 2012, 35, 1218–1229. [Google Scholar] [CrossRef]
- Posadas, I.; Santos, P.; Blanco, A.; Muñoz-Fernández, M.; Ceña, V. Acetaminophen induces apoptosis in rat cortical neurons. PLoS ONE 2010, 5, e15360. [Google Scholar] [CrossRef] [PubMed]
- Sher, D.A.; Gibson, J.L. Pioneering, prodigious and perspicacious: Grunya Efimovna Sukhareva’s life and contribution to conceptualising autism and schizophrenia. Eur. Child Adolesc. Psychiatry 2023, 32, 475–490. [Google Scholar] [CrossRef]
- Kanner, L. Autistic disturbances of affective contact. Nerv. Child 1943, 2, 217–250. [Google Scholar]
- Asperger, H. Die “Autistischen Psychopathen” im Kindesalter. Arch. Für Psychiatr. Und Nervenkrankh. 1944, 117, 76–136. [Google Scholar] [CrossRef]
- Baron-Cohen, S. Leo Kanner, Hans Asperger, and the discovery of autism. Lancet 2015, 386, 1329–1330. [Google Scholar] [CrossRef]
- Easton, T.; Herrera, S. J&J’s Dirty Little Secret; Forbes: New York, NY, USA, 1998; pp. 42–44. [Google Scholar]
- ProPublica. Use Only as Directed. 2013. Available online: https://www.propublica.org/article/tylenol-mcneil-fda-use-only-as-directed (accessed on 15 April 2024).
- Matsuishi, T.; Shiotsuki, Y.; Yoshimura, K.; Shoji, H.; Imuta, F.; Yamashita, F. High prevalence of infantile autism in Kurume City, Japan. J. Child Neurol. 1987, 2, 268–271. [Google Scholar] [CrossRef]
- Coury, D.L.; Nash, P.L. Epidemiology and etiology of autistic spectrum disorders difficult to determine. Pediatr. Ann. 2003, 32, 696–700. [Google Scholar] [CrossRef]
- Nyhan, W.L. Toxicity of drugs in the neonatal period. J. Pediatr. 1961, 59, 1–20. [Google Scholar] [CrossRef]
- Lotter, V. Childhood autism in Africa. J. Child Psychol. Psychiatry Allied Discip. 1978, 19, 231–244. [Google Scholar] [CrossRef]
- Neph, A. A Comparison of Healthcare between Nicaragua and the United States and the Feasibility of Naturopathic Medicine. Honor. Proj. 2011, 73. [Google Scholar]
- Vargas-Palacios, E.; Pineda, R.; Galán-Rodas, E. The politicised and crumbling Nicaraguan health system. Lancet 2018, 392, 2694–2695. [Google Scholar] [CrossRef] [PubMed]
- Spinazzi, N.A.; Santoro, J.D.; Pawlowski, K.; Anzueto, G.; Howe, Y.J.; Patel, L.R.; Baumer, N.T. Co-occurring conditions in children with Down syndrome and autism: A retrospective study. J. Neurodev. Disord. 2023, 15, 9. [Google Scholar] [CrossRef]
- Maenner, M.J.; Warren, Z.; Williams, A.R.; Amoakohene, E.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Fitzgerald, R.T.; Furnier, S.M.; Hughes, M.M.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2023, 72, 1–14. [Google Scholar] [CrossRef]
- Decoteau, C.L. The “Western disease”: Autism and Somali parents’ embodied health movements. Soc. Sci. Med. 2017, 177, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Sterwald, C.; Baker, J. Frosted Intellectuals: How Dr. Leo Kanner Constructed the Autistic Family. Perspect. Biol. Med. 2019, 62, 690–709. [Google Scholar] [CrossRef]
- Reid, N.; Shanley, D.C.; Logan, J.; White, C.; Liu, W.; Hawkins, E. International Survey of Specialist Fetal Alcohol Spectrum Disorder Diagnostic Clinics: Comparison of Diagnostic Approach and Considerations Regarding the Potential for Unification. Int. J. Environ. Res. Public Health 2022, 19, 15663. [Google Scholar] [CrossRef]
- Hus, Y.; Segal, O. Challenges Surrounding the Diagnosis of Autism in Children. Neuropsychiatr. Dis. Treat. 2021, 17, 3509–3529. [Google Scholar] [CrossRef]
- Hen-Herbst, L.; Jirikowic, T.; Hsu, L.Y.; McCoy, S.W. Motor performance and sensory processing behaviors among children with fetal alcohol spectrum disorders compared to children with developmental coordination disorders. Res. Dev. Disabil. 2020, 103, 103680. [Google Scholar] [CrossRef] [PubMed]
- Coll, S.-M.; Foster, N.E.V.; Meilleur, A.; Brambati, S.M.; Hyde, K.L. Sensorimotor skills in autism spectrum disorder: A meta-analysis. Res. Autism Spectr. Disord. 2020, 76, 101570. [Google Scholar] [CrossRef]
- Antshel, K.M.; Russo, N. Autism Spectrum Disorders and ADHD: Overlapping Phenomenology, Diagnostic Issues, and Treatment Considerations. Curr. Psychiatry Rep. 2019, 21, 34. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, C.; Benz, J.; Pei, J.; Andrew, G.; Schuller, G.; Abele-Webster, L.; Alton, C.; Lord, L. The impact of an ADHD co-morbidity on the diagnosis of FASD. Can. J. Clin. Pharmacol. 2010, 17, e165–e176. [Google Scholar] [PubMed]
- Lai, M.C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Weyrauch, D.; Schwartz, M.; Hart, B.; Klug, M.G.; Burd, L. Comorbid Mental Disorders in Fetal Alcohol Spectrum Disorders: A Systematic Review. J. Dev. Behav. Pediatr. 2017, 38, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Matson, J.L.; Shoemaker, M. Intellectual disability and its relationship to autism spectrum disorders. Res. Dev. Disabil. 2009, 30, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Chokroborty-Hoque, A.; Alberry, B.; Singh, S.M. Exploring the complexity of intellectual disability in fetal alcohol spectrum disorders. Front. Pediatr. 2014, 2, 90. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.H.; Stade, B.; Reynolds, J.N.; Rasmussen, C.; Andrew, G.; Hwang, P.A.; Carlen, P.L. The remarkably high prevalence of epilepsy and seizure history in fetal alcohol spectrum disorders. Alcohol. Clin. Exp. Res. 2010, 34, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Hanlon-Dearman, A.; Chen, M.L.; Olson, H.C. Understanding and managing sleep disruption in children with fetal alcohol spectrum disorder. Biochem. Cell Biol. 2018, 96, 267–274. [Google Scholar] [CrossRef]
- Amos-Kroohs, R.M.; Fink, B.A.; Smith, C.J.; Chin, L.; Van Calcar, S.C.; Wozniak, J.R.; Smith, S.M. Abnormal Eating Behaviors Are Common in Children with Fetal Alcohol Spectrum Disorder. J. Pediatr. 2016, 169, 194–200.e1. [Google Scholar] [CrossRef] [PubMed]
- Reid, N.; Moritz, K.M.; Akison, L.K. Adverse health outcomes associated with fetal alcohol exposure: A systematic review focused on immune-related outcomes. Pediatr. Allergy Immunol. 2019, 30, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Al-Beltagi, M. Autism medical comorbidities. World J. Clin. Pediatr. 2021, 10, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Zhu, Y.; Wang, T.; Zhang, X.; Zhang, K.; Zhang, Z. Genetic risk factors for autism-spectrum disorders: A systematic review based on systematic reviews and meta-analysis. J. Neural Transm. 2021, 128, 717–734. [Google Scholar] [CrossRef] [PubMed]
- Sambo, D.; Goldman, D. Genetic Influences on Fetal Alcohol Spectrum Disorder. Genes 2023, 14, 195. [Google Scholar] [CrossRef] [PubMed]
- Modabbernia, A.; Velthorst, E.; Reichenberg, A. Environmental risk factors for autism: An evidence-based review of systematic reviews and meta-analyses. Mol. Autism 2017, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Gossage, J.P. Maternal risk factors for fetal alcohol spectrum disorders: Not as simple as it might seem. Alcohol Res. Health 2011, 34, 15–26. [Google Scholar] [PubMed]
- Daniolou, S.; Pandis, N.; Znoj, H. The Efficacy of Early Interventions for Children with Autism Spectrum Disorders: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 5100. [Google Scholar] [CrossRef]
- Reid, N.; Dawe, S.; Shelton, D.; Harnett, P.; Warner, J.; Armstrong, E.; LeGros, K.; O’Callaghan, F. Systematic Review of Fetal Alcohol Spectrum Disorder Interventions Across the Life Span. Alcohol. Clin. Exp. Res. 2015, 39, 2283–2295. [Google Scholar] [CrossRef]
- Thompson, T.; Oram, C.; Correll, C.U.; Tsermentseli, S.; Stubbs, B. Analgesic Effects of Alcohol: A Systematic Review and Meta-Analysis of Controlled Experimental Studies in Healthy Participants. J. Pain 2017, 18, 499–510. [Google Scholar] [CrossRef]
- Ohashi, N.; Kohno, T. Analgesic Effect of Acetaminophen: A Review of Known and Novel Mechanisms of Action. Front. Pharmacol. 2020, 11, 580289. [Google Scholar] [CrossRef] [PubMed]
- Luo, G.; Huang, L.; Zhang, Z. The molecular mechanisms of acetaminophen-induced hepatotoxicity and its potential therapeutic targets. Exp. Biol. Med. 2023, 248, 412–424. [Google Scholar] [CrossRef] [PubMed]
- Zakhari, S. Overview: How is alcohol metabolized by the body? Alcohol Res. Health 2006, 29, 245–254. [Google Scholar] [PubMed]
- McGill, M.R.; Jaeschke, H. Metabolism and disposition of acetaminophen: Recent advances in relation to hepatotoxicity and diagnosis. Pharm. Res. 2013, 30, 2174–2187. [Google Scholar] [CrossRef] [PubMed]
- Alberti, A.; Pirrone, P.; Elia, M.; Waring, R.H.; Romano, C. Sulphation deficit in “low-functioning” autistic children: A pilot study. Biol. Psychiatry 1999, 46, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Pagan, C.; Benabou, M.; Leblond, C.; Cliquet, F.; Mathieu, A.; Lemière, N.; Goubran-Botros, H.; Delorme, R.; Leboyer, M.; Callebert, J.; et al. Decreased phenol sulfotransferase activities associated with hyperserotonemia in autism spectrum disorders. Transl. Psychiatry 2021, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Geier, D.A.; Kern, J.K.; Garver, C.R.; Adams, J.B.; Audhya, T.; Geier, M.R. A prospective study of transsulfuration biomarkers in autistic disorders. Neurochem. Res. 2009, 34, 386–393. [Google Scholar] [CrossRef] [PubMed]
- James, S.J.; Cutler, P.; Melnyk, S.; Jernigan, S.; Janak, L.; Gaylor, D.W.; Neubrander, J.A. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am. J. Clin. Nutr. 2004, 80, 1611–1617. [Google Scholar] [CrossRef] [PubMed]
- Vargas, D.L.; Nascimbene, C.; Krishnan, C.; Zimmerman, A.W.; Pardo, C.A. Neuroglial activation and neuroinflammation in the brain of patients with autism. Ann. Neurol. 2005, 57, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Meyer, U.; Feldon, J.; Dammann, O. Schizophrenia and autism: Both shared and disorder-specific pathogenesis via perinatal inflammation? Pediatr. Res. 2011, 69, 26R–33R. [Google Scholar] [CrossRef]
- Stancioiu, F.; Bogdan, R.; Dumitrescu, R. Neuron-Specific Enolase (NSE) as a Biomarker for Autistic Spectrum Disease (ASD). Life 2023, 13, 1736. [Google Scholar] [CrossRef]
- Dong, D.; Zielke, H.R.; Yeh, D.; Yang, P. Cellular stress and apoptosis contribute to the pathogenesis of autism spectrum disorder. Autism Res. 2018, 11, 1076–1090. [Google Scholar] [CrossRef] [PubMed]
- Frye, R.E.; Sequeira, J.M.; Quadros, E.V.; James, S.J.; Rossignol, D.A. Cerebral folate receptor autoantibodies in autism spectrum disorder. Mol. Psychiatry 2013, 18, 369–381. [Google Scholar] [CrossRef]
- James, S.J. Autism and Folate-dependent One-carbon Metabolism: Serendipity and Critical Branch-point Decisions in Science. Glob. Adv. Health Med. 2013, 2, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Parker, W.; Hornik, C.D.; Bilbo, S.; Holzknecht, Z.E.; Gentry, L.; Rao, R.; Lin, S.S.; Herbert, M.R.; Nevison, C.D. The role of oxidative stress, inflammation and acetaminophen exposure from birth to early childhood in the induction of autism. J. Int. Med. Res. 2017, 45, 407–438. [Google Scholar] [CrossRef]
- McFadden, J. Razor sharp: The role of Occam’s razor in science. Ann. N. Y. Acad. Sci. 2023, 1530, 8–17. [Google Scholar] [CrossRef]
- Ahlqvist, V.H.; Sjöqvist, H.; Dalman, C.; Karlsson, H.; Stephansson, O.; Johansson, S.; Magnusson, C.; Gardner, R.M.; Lee, B.K. Acetaminophen Use During Pregnancy and Children’s Risk of Autism, ADHD, and Intellectual Disability. Jama 2024, 331, 1205–1214. [Google Scholar] [CrossRef]
- Vatcheva, K.P.; Lee, M.; McCormick, J.B.; Rahbar, M.H. The Effect of Ignoring Statistical Interactions in Regression Analyses Conducted in Epidemiologic Studies: An Example with Survival Analysis Using Cox Proportional Hazards Regression Model. Epidemiology 2015, 6, 216. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.; Frewer, V.; Cox, G.; Williams, K.; Ure, A. Prevalence and Age of Onset of Regression in Children with Autism Spectrum Disorder: A Systematic Review and Meta-analytical Update. Autism Res. 2021, 14, 582–598. [Google Scholar] [CrossRef]
- Bandoli, G.; Palmsten, K.; Chambers, C. Acetaminophen use in pregnancy: Examining prevalence, timing, and indication of use in a prospective birth cohort. Paediatr. Perinat. Epidemiol. 2020, 34, 237–246. [Google Scholar] [CrossRef]
- Woodbury, M.L.; Cintora, P.; Ng, S.; Hadley, P.A.; Schantz, S.L. Examining the relationship of acetaminophen use during pregnancy with early language development in children. Pediatr. Res. 2023, 95, 1883–1896. [Google Scholar] [CrossRef] [PubMed]
- Bornehag, C.G.; Reichenberg, A.; Hallerback, M.U.; Wikstrom, S.; Koch, H.M.; Jonsson, B.A.; Swan, S.H. Prenatal exposure to acetaminophen and children’s language development at 30 months. Eur. Psychiatry 2018, 51, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Westerlund, T.; Barzi, S.; Bernsten, C. Consumer views on safety of over-the-counter drugs, preferred retailers and information sources in Sweden: After re-regulation of the pharmacy market. Pharm. Pract. 2017, 15, 894. [Google Scholar] [CrossRef] [PubMed]
- Case 1:22-md-03043-DLC Document 1381, Page 111. Filed 12/18/23. 2024. Available online: https://casetext.com/case/in-re-acetaminophen-asd-adhd-prods-liab-litig-103 (accessed on 26 February 2024).
- Alemany, S.; Avella-García, C.; Liew, Z.; García-Esteban, R.; Inoue, K.; Cadman, T.; López-Vicente, M.; González, L.; Riaño Galán, I.; Andiarena, A.; et al. Prenatal and postnatal exposure to acetaminophen in relation to autism spectrum and attention-deficit and hyperactivity symptoms in childhood: Meta-analysis in six European population-based cohorts. Eur. J. Epidemiol. 2021, 36, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Ertmann, R.K.; Møller, J.J.; Waldorff, F.B.; Siersma, V.; Reventlow, S.; Söderström, M. The majority of sick children receive paracetamol during the winter. Dan. Med. J. 2012, 59, A4555. [Google Scholar] [PubMed]
- Bittker, S.S.; Bell, K.R. Acetaminophen, antibiotics, ear infection, breastfeeding, vitamin D drops, and autism: An epidemiological study. Neuropsychiatr. Dis. Treat. 2018, 14, 1399–1414. [Google Scholar] [CrossRef] [PubMed]
- Bittker, S.S.; Bell, K.R. Postnatal Acetaminophen and Potential Risk of Autism Spectrum Disorder among Males. Behav. Sci. 2020, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Lewerissa, E.I.; Nadif Kasri, N.; Linda, K. Epigenetic regulation of autophagy-related genes: Implications for neurodevelopmental disorders. Autophagy 2024, 20, 15–28. [Google Scholar] [CrossRef]
- Miners, J.O.; Robson, R.A.; Birkett, D.J. Paracetamol metabolism in pregnancy. Br. J. Clin. Pharmacol. 1986, 22, 359–362. [Google Scholar] [CrossRef]
- O’Hara, K.; Wright, I.M.; Schneider, J.J.; Jones, A.L.; Martin, J.H. Pharmacokinetics in neonatal prescribing: Evidence base, paradigms and the future. Br. J. Clin. Pharmacol. 2015, 80, 1281–1288. [Google Scholar] [CrossRef]
- Evans, S.S.; Repasky, E.A.; Fisher, D.T. Fever and the thermal regulation of immunity: The immune system feels the heat. Nat. Rev. Immunol. 2015, 15, 335–349. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.E.; Farrar, H.C. Fever and Antipyretic Use in Children. Pediatrics 2011, 127, 580–587. [Google Scholar] [CrossRef] [PubMed]
- El-Radhi, A.S.M. Fever management: Evidence vs current practice. Clin. Pediatr. 2012, 1, 29–33. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number Cofactors Included | Variable | HR (p-Value) | Lower-Upper 95% CI |
|---|---|---|---|
| 0 | APAP | 2.461 (2 × 10−16) | 2.675–2.265 |
| 3 | Cofactor 1 | 1.219 (2 × 10−16) | 1.241–1.198 |
| 3 | Cofactor 2 | 1.197 (2 × 10−16) | 1.217–1.176 |
| 3 | Cofactor 3 | 1.186 (2 × 10−16) | 1.207–1.166 |
| 3 | APAP | 1.844 (2 × 10−16) | 2.007–1.694 |
| 9 | Cofactor 1 | 1.250 (2 × 10−16) | 1.275–1.231 |
| 9 | Cofactor 2 | 1.210 (2 × 10−16) | 1.233–1.192 |
| 9 | Cofactor 3 | 1.203 (2 × 10−16) | 1.227–1.185 |
| 9 | Cofactor 4 | 1.221 (2 × 10−16) | 1.245–1.203 |
| 9 | Cofactor 5 | 1.215 (2 × 10−16) | 1.238–1.197 |
| 9 | Cofactor 6 | 1.235 (2 × 10−16) | 1.260–1.217 |
| 9 | Cofactor 7 | 1.216 (2 × 10−16) | 1.240–1.199 |
| 9 | Cofactor 8 | 1.227 (2 × 10−16) | 1.251–1.208 |
| 9 | Cofactor 9 | 1.215 (2 × 10−16) | 1.238–1.197 |
| 9 | APAP | 0.905 (0.0264) | 0.828–0.988 |
| Number Cofactors Included | Variable | HR (p-Value) | Lower-Upper 95% CI |
|---|---|---|---|
| 0 | APAP | 1.364 (8.13 × 10−8) | 1.218–1.528 |
| 3 | Cofactor 1 | 1.238 (2 × 10−16) | 1.217–1.260 |
| 3 | Cofactor 2 | 1.216 (2 × 10−16) | 1.196–1.237 |
| 3 | Cofactor 3 | 1.205 (2 × 10−16) | 1.185–1.226 |
| 3 | APAP | 1.197 (0.00196) | 1.068–1.341 |
| 9 | Cofactor 1 | 1.250 (2 × 10−16) | 1.229–1.272 |
| 9 | Cofactor 2 | 1.210 (2 × 10−16) | 1.190–1.230 |
| 9 | Cofactor 3 | 1.203 (2 × 10−16) | 1.183–1.224 |
| 9 | Cofactor 4 | 1.221 (2 × 10−16) | 1.200–1.242 |
| 9 | Cofactor 5 | 1.215 (2 × 10−16) | 1.194–1.236 |
| 9 | Cofactor 6 | 1.235 (2 × 10−16) | 1.214–1.256 |
| 9 | Cofactor 7 | 1.216 (2 × 10−16) | 1.196–1.237 |
| 9 | Cofactor 8 | 1.227 (2 × 10−16) | 1.206–1.248 |
| 9 | Cofactor 9 | 1.215 (2 × 10−16) | 1.194–1.235 |
| 9 | APAP | 0.992 (0.886) | 0.885–1.111 |
| Distinct Problems Identifying the Contribution of Acetaminophen Exposure to the Prevalence of ASD Using a Multivariate Analysis | Result/Solution |
|---|---|
| Evaluation of databases that capture a limited time during neurodevelopment will capture only a fraction of the risk of acetaminophen exposure *. Measures of exposure during all relevant time periods (e.g., during pregnancy, immediately postpartum, between 12 and 18 months of age) are not available for any cohort. | Odds ratios calculated based on one time period underestimate the impact of acetaminophen on neurodevelopment; the effects of acetaminophen within one developmental period should be considered in conjunction with effects during other developmental periods for policy making purposes. |
| Heavy use of acetaminophen among non-sensitive individuals reduces the calculated risk of exposure. | Relatively low odds ratios (e.g., 1.2–2.0) merit policy change if exposure is prevalent. |
| Underreporting of acetaminophen use reduces the calculated risk of exposure. | Exposure determination should be rigorous. |
| Variables associated with sensitivity cannot be treated as confounding factors. | Model assumptions determine outcomes: Calculate risks using interacting variables. |
| Exposure during one time period (e.g., pregnancy) may correlate with exposure during other time periods (e.g., first 18 months of life). | Assessment of risk during one time period correlates to an unknown degree with risk at other time periods; risks during specific time periods cannot be reliably determined. |
| Some variables associated with sensitivity during one time period (e.g., pregnancy) correlate with or may be identical to variables associated with sensitivity during other time periods (e.g., first 18 months of life). | Assessment of exposure during one time period may correlate with exposure at other time periods; risks during specific time periods cannot be reliably determined. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, J.P., III; Williamson, L.; Konsoula, Z.; Anderson, R.; Reissner, K.J.; Parker, W. Evaluating the Role of Susceptibility Inducing Cofactors and of Acetaminophen in the Etiology of Autism Spectrum Disorder. Life 2024, 14, 918. https://doi.org/10.3390/life14080918
Jones JP III, Williamson L, Konsoula Z, Anderson R, Reissner KJ, Parker W. Evaluating the Role of Susceptibility Inducing Cofactors and of Acetaminophen in the Etiology of Autism Spectrum Disorder. Life. 2024; 14(8):918. https://doi.org/10.3390/life14080918
Chicago/Turabian StyleJones, John P., III, Lauren Williamson, Zacharoula Konsoula, Rachel Anderson, Kathryn J. Reissner, and William Parker. 2024. "Evaluating the Role of Susceptibility Inducing Cofactors and of Acetaminophen in the Etiology of Autism Spectrum Disorder" Life 14, no. 8: 918. https://doi.org/10.3390/life14080918