
Determinants of Human Asymmetry: Does Asymmetrical Retinal Vasculature Predict Asymmetry Elsewhere in the Body?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Data
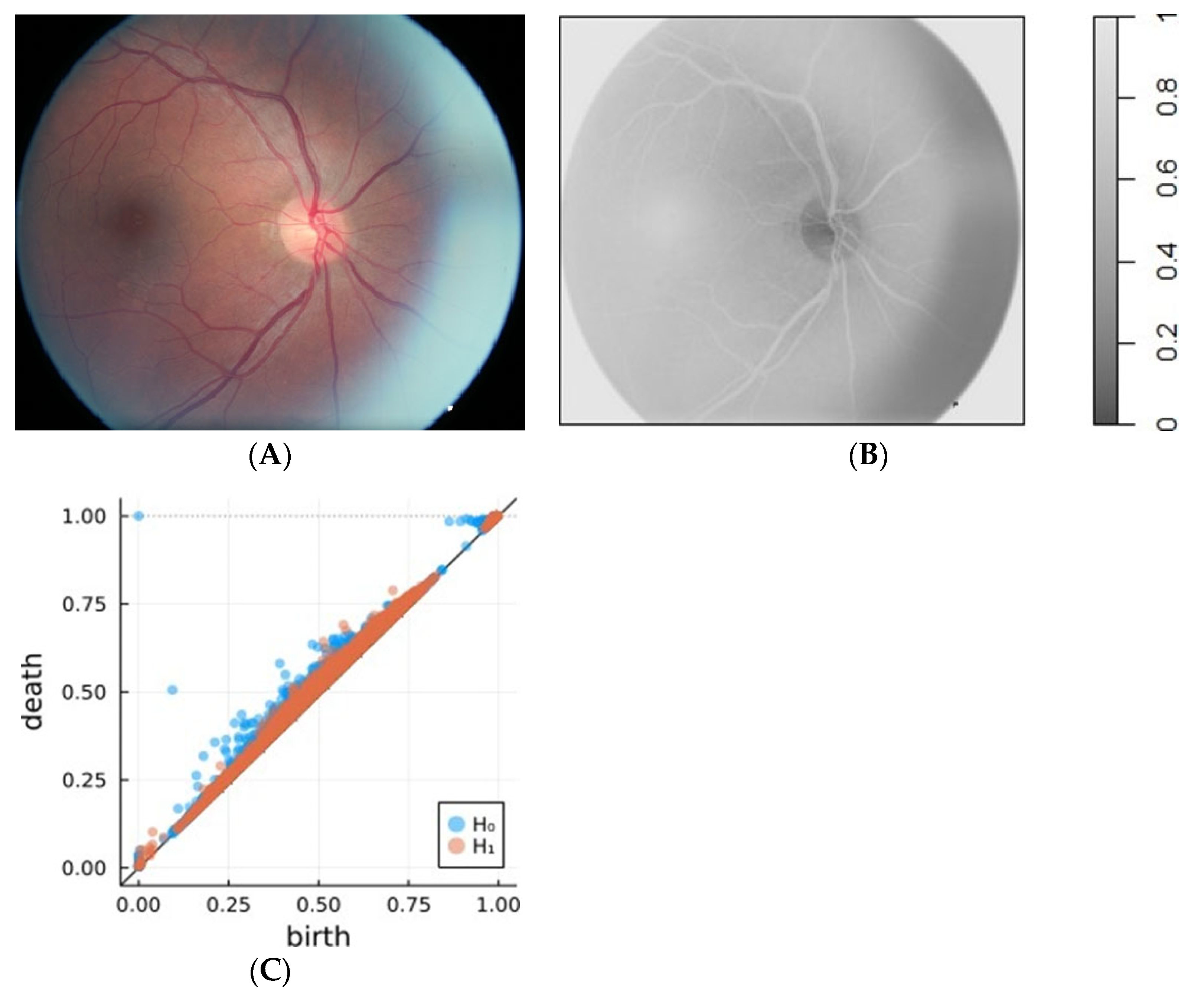
2.2. Retinal Fundus Photographs
2.3. Retinal Vasculature Asymmetry Estimates
2.4. Genotyping and Runs of Homozygosity
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levin, M.; Klar, A.J.S.; Ramsdell, A.F. Introduction: Introduction to provocative questions in left–right asymmetry. Philos. Trans. Biol. Sci. 2016, 371, 20150399. [Google Scholar] [CrossRef] [PubMed]
- Valen, L.V. A study of fluctuating asymmetry. Evol. Int. J. Org. Evol. 1962, 16, 125–142. [Google Scholar] [CrossRef]
- Berretz, G.; Arning, L.; Gerding, W.M.; Friedrich, P.; Fraenz, C.; Schlüter, C.; Epplen, J.T.; Güntürkün, O.; Beste, C.; Genç, E.; et al. Structural asymmetry in the frontal and temporal lobes is associated with PCSK6 VNTR polymorphism. Mol. Neurobiol. 2019, 56, 7765–7773. [Google Scholar] [CrossRef] [PubMed]
- Holló, G. Demystification of animal symmetry: Symmetry is a response to mechanical forces. Biol. Direct 2017, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- Beasley, D.A.E.; Bonisoli-Alquati, A.; Mousseau, T.A. The use of fluctuating asymmetry as a measure of environmentally induced developmental instability: A meta-analysis. Ecol. Indic. 2013, 30, 218–226. [Google Scholar] [CrossRef]
- Palmer, A.R. What determines direction of asymmetry: Genes, environment or chance? Philos. Trans. Biol. Sci. 2016, 371, 20150417. [Google Scholar] [CrossRef] [PubMed]
- Hope, D.; Bates, T.C.; Dykiert, D.; Der, G.; Deary, I.J. Bodily symmetry increases across human childhood. Early Hum. Dev. 2013, 89, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Jandová, M.; Urbanová, P. Studying factors influencing facial developmental instability. Ann. Hum. Biol. 2021, 48, 280–293. [Google Scholar] [CrossRef] [PubMed]
- Palestis, B.G.; Trivers, R. A longitudinal study of changes in fluctuating asymmetry with age in Jamaican youth. Symmetry 2016, 8, 123. [Google Scholar] [CrossRef]
- Graham, J.H.; Özener, B. Fluctuating asymmetry of human populations: A review. Symmetry 2016, 8, 154. [Google Scholar] [CrossRef]
- Klingenberg, C.P. Analyzing Fluctuating asymmetry with geometric morphometrics: Concepts, methods, and applications. Symmetry 2015, 7, 843–934. [Google Scholar] [CrossRef]
- Van Dongen, S.; Wijnaendts, L.C.; Ten Broek, C.M.; Galis, F. Fluctuating asymmetry does not consistently reflect severe developmental disorders in human fetuses. Evol. Int. J. Org. Evol. 2009, 63, 1832–1844. [Google Scholar] [CrossRef] [PubMed]
- Banks, G.C.; Batchelor, J.H.; McDaniel, M.A. Smarter people are (a bit) more symmetrical: A meta-analysis of the relationship between intelligence and fluctuating asymmetry. Intelligence 2010, 38, 393–401. [Google Scholar] [CrossRef]
- Gangestad, S.W. Developmental instability, fluctuating asymmetry, and human psychological science. Emerg. Top. Life Sci. 2022, 6, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Clarke, G.M. Developmental stability and fitness: The evidence is not quite so clear. Am. Nat. 1998, 152, 762–766. [Google Scholar] [CrossRef] [PubMed]
- Carothers, A.D.; Rudan, I.; Kolcic, I.; Polasek, O.; Hayward, C.; Wright, A.F.; Campbell, H.; Teague, P.; Hastie, N.D.; Weber, J.L. Estimating human inbreeding coefficients: Comparison of genealogical and marker heterozygosity approaches. Ann. Hum. Genet. 2006, 70, 666–676. [Google Scholar] [CrossRef]
- Polašek, O.; Hayward, C.; Bellenguez, C.; Vitart, V.; Kolčić, I.; McQuillan, R.; Saftić, V.; Gyllensten, U.; Wilson, J.F.; Rudan, I.; et al. Comparative assessment of methods for estimating individual genome-wide homozygosity-by-descent from human genomic data. BMC Genom. 2010, 11, 139. [Google Scholar] [CrossRef]
- McQuillan, R.; Leutenegger, A.L.; Abdel-Rahman, R.; Franklin, C.S.; Pericic, M.; Barac-Lauc, L.; Smolej-Narancic, N.; Janicijevic, B.; Polasek, O.; Tenesa, A.; et al. Runs of homozygosity in European populations. Am. J. Hum. Genet. 2008, 83, 359–372. [Google Scholar] [CrossRef]
- Clark, D.W.; Okada, Y.; Moore, K.H.S.; Mason, D.; Pirastu, N.; Gandin, I.; Mattsson, H.; Barnes, C.L.K.; Lin, K.; Zhao, J.H.; et al. Associations of autozygosity with a broad range of human phenotypes. Nat. Commun. 2019, 10, 4957. [Google Scholar] [CrossRef]
- Vitart, V.; Biloglav, Z.; Hayward, C.; Janicijevic, B.; Smolej-Narancic, N.; Barac, L.; Pericic, M.; Klaric, I.M.; Skaric-Juric, T.; Barbalic, M.; et al. 3000 years of solitude: Extreme differentiation in the island isolates of Dalmatia, Croatia. Eur. J. Hum. Genet. 2006, 14, 478–487. [Google Scholar] [CrossRef]
- Polašek, O. Global mobility and the break-up of human population isolates—Neglected mechanisms in health, demographics, and anthropology. Croat. Med. J. 2015, 56, 324–325. [Google Scholar] [CrossRef] [PubMed]
- Kirin, M.; McQuillan, R.; Franklin, C.S.; Campbell, H.; McKeigue, P.M.; Wilson, J.F. Genomic runs of homozygosity record population history and consanguinity. PLoS ONE 2010, 5, e13996. [Google Scholar] [CrossRef] [PubMed]
- Ceballos, F.C.; Joshi, P.K.; Clark, D.W.; Ramsay, M.; Wilson, J.F. Runs of homozygosity: Windows into population history and trait architecture. Nat. Rev. Genet. 2018, 19, 220–234. [Google Scholar] [CrossRef] [PubMed]
- Joshi, P.K.; Esko, T.; Mattsson, H.; Eklund, N.; Gandin, I.; Nutile, T.; Jackson, A.U.; Schurmann, C.; Smith, A.V.; Zhang, W.; et al. Directional dominance on stature and cognition in diverse human populations. Nature 2015, 523, 459–462. [Google Scholar] [CrossRef]
- Kirin, M.; Nagy, R.; MacGillivray, T.J.; Polašek, O.; Hayward, C.; Rudan, I.; Campbell, H.; Wild, S.; Wright, A.F.; Wilson, J.F.; et al. Determinants of retinal microvascular features and their relationships in two European populations. J. Hypertens. 2017, 35, 1646–1659. [Google Scholar] [CrossRef] [PubMed]
- Abràmoff, M.D.; Garvin, M.K.; Sonka, M. Retinal imaging and image analysis. IEEE Rev. Biomed. Eng. 2010, 3, 169–208. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.; Khan, T.M.; Naveed, K.; Naqvi, S.S.; Nawaz, S.J. Recent trends and advances in fundus image analysis: A review. Comput. Biol. Med. 2022, 151, 106277. [Google Scholar] [CrossRef]
- Noh, K.J.; Park, S.J.; Lee, S. Scale-space approximated convolutional neural networks for retinal vessel segmentation. Comput. Methods Programs Biomed. 2019, 178, 237–246. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, X.; Ren, J. Blood vessel segmentation from fundus image by a cascade classification framework. Pattern Recognit. 2019, 88, 331–341. [Google Scholar] [CrossRef]
- Rodríguez-Robles, F.; Verdú-Monedero, R.; Berenguer-Vidal, R.; Morales-Sánchez, J.; Sellés-Navarro, I. Analysis of the Asymmetry between Both Eyes in Early Diagnosis of Glaucoma Combining Features Extracted from Retinal Images and OCTs into Classification Models. Sensors 2023, 23, 4737. [Google Scholar] [CrossRef]
- Kang, T.S.; Kim, B.J.; Nam, K.Y.; Lee, S.; Kim, K.; Lee, W.-S.; Kim, J.; Han, Y.S. Asymmetry between right and left fundus images identified using convolutional neural networks. Sci. Rep. 2022, 12, 1444. [Google Scholar] [CrossRef]
- Kaczynski, T.; Mischaikow, K.; Mrozek, M. Computational Homology; Springer: Berlin/Heidelberg, Germany, 2004. [Google Scholar]
- Edelsbrunner, H.; Harer, J. Computational Topology; American Mathematical Society: Providence, RI, USA, 2010. [Google Scholar]
- Biscio, C.A.N.; Møller, J. The Accumulated persistence function, a new useful functional summary statistic for topological data analysis, with a view to brain artery trees and spatial point process applications. J. Comput. Graph. Stat. 2019, 28, 671–681. [Google Scholar] [CrossRef]
- Garside, K.; Henderson, R.; Makarenko, I.; Masoller, C. Topological data analysis of high resolution diabetic retinopathy images. PLoS ONE 2019, 14, e0217413. [Google Scholar] [CrossRef] [PubMed]
- Čufar, M. Ripserer.jl: Flexible and efficient persistent homology computation in Julia. J. Open Source Softw. 2020, 5, 2614. [Google Scholar] [CrossRef]
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.A.; Bender, D.; Maller, J.; Sklar, P.; de Bakker, P.I.; Daly, M.J.; et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 2007, 81, 559–575. [Google Scholar] [CrossRef] [PubMed]
- Bellenguez, C.; Ober, C.; Bourgain, C. Linkage analysis with dense SNP maps in isolated populations. Hum. Hered. 2009, 68, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Harshman, L.G.; Müller, H.G.; Liu, X.; Wang, Y.; Carey, J.R. The symmetry of longevity. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2005, 60, 1233–1237. [Google Scholar] [CrossRef] [PubMed]
- Kuningas, M.; McQuillan, R.; Wilson, J.F.; Hofman, A.; van Duijn, C.M.; Uitterlinden, A.G.; Tiemeier, H. Runs of homozygosity do not influence survival to old age. PLoS ONE 2011, 6, e22580. [Google Scholar] [CrossRef] [PubMed]
- Rudan, I.; Carothers, A.D.; Polasek, O.; Hayward, C.; Vitart, V.; Biloglav, Z.; Kolcic, I.; Zgaga, L.; Ivankovic, D.; Vorko-Jovic, A.; et al. Quantifying the increase in average human heterozygosity due to urbanisation. Eur. J. Hum. Genet. EJHG 2008, 16, 1097–1102. [Google Scholar] [CrossRef]
- Rehberg, J.; Stipčić, A.; Ćorić, T.; Kolčić, I.; Polašek, O. Mortality patterns in Southern Adriatic islands of Croatia: A registry-based study. Croat. Med. J. 2018, 59, 118–123. [Google Scholar] [CrossRef]
- Kolčić, I.; Relja, A.; Gelemanović, A.; Miljković, A.; Boban, K.; Hayward, C.; Rudan, I.; Polašek, O. Mediterranean diet in the southern Croatia—Does it still exist? Croat. Med. J. 2016, 57, 415–424. [Google Scholar] [CrossRef]
- McGrath, J.; Somlo, S.; Makova, S.; Tian, X.; Brueckner, M. Two populations of node monocilia initiate left-right asymmetry in the mouse. Cell 2003, 114, 61–73. [Google Scholar] [CrossRef]
- Vandenberg, L.N.; Levin, M. A unified model for left-right asymmetry? Comparison and synthesis of molecular models of embryonic laterality. Dev. Biol. 2013, 379, 1–15. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Parameter | Island of Vis | Island of Korcula | City of Split | Total | p |
|---|---|---|---|---|---|
| Sex; n (%) Men Women | 0.564 | ||||
| 237 (38.4) | 195 (41.5) | 307 (39.1) | 739 (39.5) | ||
| 380 (61.6) | 275 (58.5) | 479 (60.9) | 1134 (60.5) | ||
| Comorbidity One Multiple None | <0.001 | ||||
| 185 (30.0) | 121 (25.7) | 209 (26.6) | 515 (27.5) | ||
| 171 (27.7) | 123 (26.2) | 92 (11.7) | 386 (20.6) | ||
| 261 (42.3) | 226 (48.1) | 485 (61.7) | 972 (51.9) | ||
| Age | 55.63 ± 14.22 | 54.47 ± 15.62 | 51.04 ± 14.07 | 53.41 ± 14.66 | <0.001 |
| Years of schooling | 10.04 ± 3.42 | 10.53 ± 3.32 | 13.09 ± 2.89 | 11.40 ± 3.48 | <0.001 |
| Subjective material status | 2.98 ± 0.76 | 3.12 ± 0.71 | 3.32 ± 0.69 | 3.16 ± 0.74 | <0.001 |
| Objective material status | * | 3.24 ± 1.43 | 4.16 ± 1.4 | 3.82 ± 1.48 | <0.001 |
| Household material status | 9.53 ± 2.65 | 10.22 ± 2.44 | 11.3 ± 2.34 | 10.45 ± 2.59 | <0.001 |
| ReVA.0; r (p) | ReVA.1; r (p) | |
|---|---|---|
| ReVA.0 | - | 0.994 (<0.001) |
| ReVA.1 | 0.994 (<0.001) | - |
| Spheric power | 0.133 (<0.001) | 0.135 (<0.001) |
| Cylinder power | 0.163 (<0.001) | 0.164 (<0.001) |
| Angle | 0.042 (0.135) | 0.045 (0.117) |
| Corneal radius | 0.124 (<0.001) | 0.123 (<0.001) |
| Corneal thickness | 0.082 (<0.001) | 0.085 (<0.001) |
| Anterior chamber length | 0.189 (<0.001) | 0.193 (<0.001) |
| Lens thickness | 0.084 (<0.001) | 0.087 (<0.001) |
| Posterior chamber length | 0.165 (<0.001) | 0.169 (<0.001) |
| Axial length | 0.191 (<0.001) | 0.197 (<0.001) |
| Audiometry, 0.25 Hz | 0.011 (0.641) | 0.007 (0.757) |
| Audiometry, 0.5 Hz | 0.030 (0.199) | 0.031 (0.192) |
| Audiometry, 1 Hz | 0.033 (0.165) | 0.031 (0.184) |
| Audiometry, 2 Hz | −0.009 (0.701) | −0.006 (0.788) |
| Audiometry, 3 Hz | 0.035 (0.131) | 0.037 (0.110) |
| Audiometry, 4 Hz | 0.054 (0.020) | 0.050 (0.032) |
| Audiometry, 6 Hz | −0.004 (0.856) | −0.005 (0.822) |
| Audiometry, 8 Hz | 0.052 (0.028) | 0.052 (0.025) |
| ABPI, radial artery | 0.034 (0.175) | 0.032 (0.200) |
| ABPI posterior tibial artery | 0.101 (<0.001) | 0.097 (<0.001) |
| ABPI dorsal foot artery | 0.034 (0.176) | 0.033 (0.181) |
| ROH, number of segments | 0.229 (<0.001) | 0.229 (<0.001) |
| ROH, kb | 0.101 (<0.001) | 0.099 (<0.001) |
| ROH, average kb | 0.098 (<0.001) | 0.100 (<0.001) |
| ROH, number of segments, rLD | 0.213 (<0.001) | 0.213 (<0.001) |
| ROH, kb, rLD | 0.089 (<0.001) | 0.088 (<0.001) |
| ROH, average kb, rLD | 0.108 (<0.001) | 0.111 (<0.001) |
| Variable | Unadjusted Model, HR [95% CI]; p | Adjusted Model, HR [95% CI]; p |
|---|---|---|
| Age | 1.10 [1.09–1.12]; <0.001 | 1.09 [1.08–1.11]; <0.001 |
| Sex | ||
| Men (Ref) | 1.00 | 1.00 |
| Women | 0.53 [0.41–0.69]; <0.001 | 0.49 [0.37–0.64]; <0.001 |
| Cohort | ||
| Vis (Ref) | 1.00 | 1.00 |
| Korcula | 0.87 [0.56–1.36]; 0.533 | 0.62 [0.36–1.04]; 0.069 |
| Split | 0.58 [0.41–0.82]; 0.002 | 0.88 [0.59–1.29]; 0.500 |
| Multiple asymmetries | ||
| No (Ref) | 1.00 | 1.00 |
| Yes | 0.97 [0.59–1.59]; 0.899 | 0.74 [0.45–1.22]; 0.237 |
| Comorbidity load | 1.64 [1.49–1.80]; <0.001 | 1.20 [1.08–1.35]; 0.002 |
| ROH, number of segments | 1.02 [1.00–1.05]; 0.031 | 0.99 [0.97–1.02]; 0.789 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plećaš, D.; Gotovac Đogaš, V.; Polašek, O.; Škunca Herman, J. Determinants of Human Asymmetry: Does Asymmetrical Retinal Vasculature Predict Asymmetry Elsewhere in the Body? Life 2024, 14, 929. https://doi.org/10.3390/life14080929
Plećaš D, Gotovac Đogaš V, Polašek O, Škunca Herman J. Determinants of Human Asymmetry: Does Asymmetrical Retinal Vasculature Predict Asymmetry Elsewhere in the Body? Life. 2024; 14(8):929. https://doi.org/10.3390/life14080929
Chicago/Turabian StylePlećaš, Doris, Vesna Gotovac Đogaš, Ozren Polašek, and Jelena Škunca Herman. 2024. "Determinants of Human Asymmetry: Does Asymmetrical Retinal Vasculature Predict Asymmetry Elsewhere in the Body?" Life 14, no. 8: 929. https://doi.org/10.3390/life14080929