Correlation between F18-FDG PET/CT Imaging and BRAF V600E Genetic Mutation for the Early Assessment of Treatment Response in Papillary Thyroid Cancers


Abstract
1. Introduction
2. Patients and Method
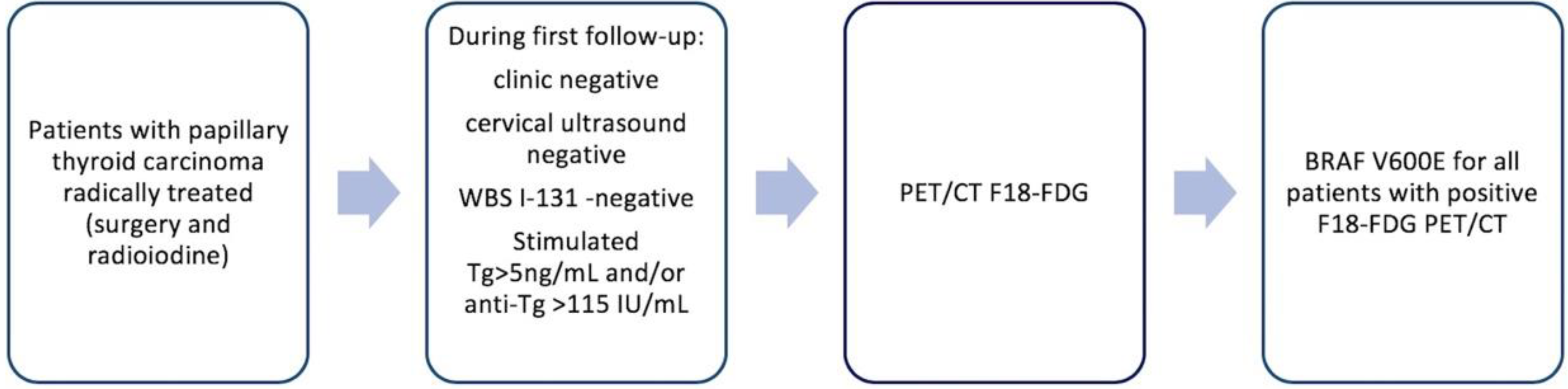
2.1. Patients
2.2. Genetic Analysis
2.3. Positron Emission Tomography/Computed Tomography (PET/CT) Imaging
2.4. Serologic Analysis
2.5. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Garnett, M.J.; Marais, R. Guilty as charged: B-RAF is a human oncogene. Cancer Cell 2004, 6, 313–319. [Google Scholar] [CrossRef] [PubMed]
- de la Fouchardiere, C.; Oussaid, N.; Derbel, O.; Decaussin-Petrucci, M.; Fondrevelle, M.-E.; Wang, Q.; Bringuier, P.-P.; Bournaud-Salinas, C.; Peix, J.-L.; Lifante, J.-C.; et al. Does Molecular Genotype Provide Useful Information in the Management of Radioiodine Refractory Thyroid Cancers? Results of a Retrospective Study. Target. Oncol. 2016, 11, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Sobrinho-Simões, M.; Eloy, C.; Vinagre, J.; Soares, P. Molecular pathology of thyroid tumors: Diagnostic and prognostic relevance. Int. J. Surg. Pathol. 2010, 18, 209S–212S. [Google Scholar] [CrossRef]
- Soares, P.; Celestino, R.; Melo, M.; Fonseca, E.; Sobrinho-Simões, M. Prognostic biomarkers in thyroid cancer. Virchows Arch. 2014, 464, 333–346. [Google Scholar] [CrossRef]
- Chang, J.W.; Park, K.W.; Heo, J.H.; Jung, S.-N.; Liu, L.; Kim, S.M.; Kwon, I.S.; Koo, B.S. Relationship Between (18)F-fluorodeoxyglucose Accumulation and the BRAF (V600E) Mutation in Papillary Thyroid Cancer. World J. Surg. 2018, 42, 114–122. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid Am. Thyroid Assoc. 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Fugazzola, L.; Elisei, R.; Fuhrer, D.; Jarzab, B.; Leboulleux, S.; Newbold, K.; Smit, J. 2019 European Thyroid Association Guidelines for the Treatment and Follow-Up of Advanced Radioiodine-Refractory Thyroid Cancer. Eur. Thyroid J. 2019, 8, 227–245. [Google Scholar] [CrossRef]
- Araque, K.A.; Gubbi, S.; Klubo-Gwiezdzinska, J. Updates on the Management of Thyroid Cancer. Horm. Metab. Res. 2020. [Google Scholar] [CrossRef]
- Fugazzola, L.; Puxeddu, E.; Avenia, N.; Romei, C.; Cirello, V.; Cavaliere, A.; Faviana, P.; Mannavola, D.; Moretti, S.; Rossi, S.; et al. Correlation between B-RAFV600E mutation and clinico-pathologic parameters in papillary thyroid carcinoma: Data from a multicentric Italian study and review of the literature. Endocr. Relat. Cancer 2006, 13, 455–464. [Google Scholar] [CrossRef]
- Larg, M.I.; Barbus, E.; Gabora, K.; Pestean, C.; Cheptea, M.; Piciu, D. 18F-FDG PET/CT in Differentiated Thyroid Carcinoma. Acta Endocrinol. (Buchar. Rom. 2005) 2019, 15, 203–208. [Google Scholar] [CrossRef]
- Smallridge, R.C.; Diehl, N.; Bernet, V. Practice trends in patients with persistent detectable thyroglobulin and negative diagnostic radioiodine whole body scans: A survey of American Thyroid Association members. Thyroid 2014, 24, 1501–1507. [Google Scholar] [CrossRef] [PubMed]
- Soares, P.; Sobrinho-Simões, M. Is BRAF mutation screening useful for preoperative risk stratification in papillary thyroid cancer? Future Oncol. 2009, 5, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-J.; Lee, S.-W.; Pak, K.; Shim, S.-R. Diagnostic performance of PET in thyroid cancer with elevated anti-Tg Ab. Endocr. Relat. Cancer 2018, 25, 643–652. [Google Scholar] [CrossRef]
- Kim, T.Y.; Kim, W.B.; Song, J.Y.; Rhee, Y.S.; Gong, G.; Cho, Y.M.; Kim, S.Y.; Kim, S.C.; Hong, S.J.; Shong, Y.K. The BRAF mutation is not associated with poor prognostic factors in Korean patients with conventional papillary thyroid microcarcinoma. Clin. Endocrinol. (Oxf.) 2005, 63, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Santhanam, P.; Khthir, R.; Solnes, L.B.; Ladenson, P.W. The Relationship Of BRAF(V600E) Mutation Status to FDG PET/CT Avidity in Thyroid Cancer: A Review And Meta-Analysis. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2018, 24, 21–26. [Google Scholar]
- Robbins, R.J.; Wan, Q.; Grewal, R.K.; Reibke, R.; Gonen, M.; Strauss, H.W.; Tuttle, R.M.; Drucker, W.; Larson, S.M. Real-time prognosis for metastatic thyroid carcinoma based on 2-[18F]fluoro-2-deoxy-D-glucose-positron emission tomography scanning. J. Clin. Endocrinol. Metab. 2006, 91, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Brose, M.S.; Nutting, C.M.; Jarzab, B.; Elisei, R.; Siena, S.; Bastholt, L.; de la Fouchardiere, C.; Pacini, F.; Paschke, R.; Shong, Y.K.; et al. Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: A randomised, double-blind, phase 3 trial. Lancet (Lond. Engl.) 2014, 384, 319–328. [Google Scholar] [CrossRef]
- Kish, J.K.; Chatterjee, D.; Wan, Y.; Yu, H.-T.; Liassou, D.; Feinberg, B.A. Lenvatinib and Subsequent Therapy for Radioactive Iodine-Refractory Differentiated Thyroid Cancer: A Real-World Study of Clinical Effectiveness in the United States. Adv. Ther. 2020, 37, 2841–2852. [Google Scholar] [CrossRef]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef]
- Tumino, D.; Frasca, F.; Newbold, K. Updates on the Management of Advanced, Metastatic, and Radioiodine Refractory Differentiated Thyroid Cancer. Front. Endocrinol. (Lausanne) 2017, 8, 312. [Google Scholar] [CrossRef]
- Basu, S.; Parghane, R.V. Grouping of Metastatic Thyroid Carcinoma by Molecular Imaging Features to Allow for Individualized Treatment, with Emphasis on the TENIS Syndrome. J. Nucl. Med. Technol. 2016, 44, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Cooray, S.D.; Topliss, D.J. The management of metastatic radioiodine-refractory differentiated thyroid cancer requires an integrated approach including both directed and systemic therapies. Endocrinol. Diabetes Metab. Case Rep. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-Y.; Chang, J.S.; Huang, S.-M.; Hung, C.-J.; Hung, C.-L.; Chang, C.-T.; Yang, H.-R.; Hsieh, T.-C.; Huang, Y.-H.; Tsai, H.-J. Experience of sorafenib treatment in differentiated thyroid cancer from Taiwan. J. Formos. Med. Assoc. 2020. [Google Scholar] [CrossRef]
- Berdelou, A.; Lamartina, L.; Klain, M.; Leboulleux, S.; Schlumberger, M. Treatment of refractory thyroid cancer. Endocr. Relat. Cancer 2018, 25, R209–R223. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No | Sex | BRAF status | SUV | Age yo | T | N | M | L | V | R | EET | Stage |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | + | 21.57 | 69 | T4a | N1b | 0 | 1 | 1 | 1 | Yes | III |
| 2 | M | + | 16.57 | 72 | T3b | N1b | 0 | 1 | 0 | 1 | Yes | II |
| 3 | M | - | 4.8 | 53 | T3b | N1b | 0 | 0 | 1 | 1 | Yes | II |
| 4 | F | - | 17.09 | 62 | T2 | N1b | 0 | 1 | 0 | 0 | Yes | II |
| 5 | F | + | 2.86 | 58 | T3b | N1b | 0 | 0 | 0 | 0 | Yes | II |
| 6 | F | + | 15 | 60 | T4a | N1b | 0 | 1 | 1 | 1 | Yes | III |
| 7 | F | - | 3.76 | 39 | T3a | N1b | 0 | 0 | 0 | 0 | Yes | I |
| 8 | M | + | 5.7 | 41 | T3b | N1b | 0 | 1 | 0 | 1 | Yes | I |
| 9 | M | + | 2.6 | 63 | T1a | N0 | 0 | 0 | 0 | 0 | Yes | I |
| 10. | F | - | 3.94 | 61 | T2 | N1b | 0 | 1 | 0 | 1 | Yes | II |
| 11. | F | N/a | 3.11 | 62 | T2 | N1b | 0 | 0 | 0 | 0 | No | I |
| 12. | F | + | 2.56 | 66 | T4a | N1b | 0 | 0 | 0 | 1 | Yes | III |
| 13. | M | - | 4.68 | 22 | T3a | N1b | 0 | 1 | 1 | 1 | Yes | I |
| 14. | F | - | 4.82 | 71 | T3b | N0 | 0 | 0 | 1 | 0 | Yes | II |
| 15. | F | - | 17.78 | 72 | T3b | N1b | 1 | 1 | 1 | 1 | Yes | IVB |
| 16. | M | + | 5.61 | 41 | T2 | N1a | 0 | 1 | 1 | 0 | No | I |
| 17. | F | - | 9.86 | 62 | T3a | N1b | 0 | 0 | 0 | 0 | No | II |
| 18. | F | + | 15 | 59 | T2 | N0 | 1 | 0 | 0 | 1 | No | IVB |
| 19. | M | - | 5.25 | 65 | T3a | N0 | 1 | 1 | 1 | 0 | Yes | IVB |
| 20. | F | + | 2.5 | 74 | T1b | N0 | 1 | 0 | 0 | 0 | Yes | IVB |
| Parameter | SUV | Age | T | N | M | L | V | R | Stage | Tg | Anti-Tg | EET |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Student t-test (P) | 0.74 | 0.55 | 0.25 | 0.55 | 0.91 | 0.82 | 0.28 | 0.52 | 0.73 | 0.93 | 0.84 | 0.61 |
| Variable | Correlation Coefficient | P | Interpretation |
|---|---|---|---|
| SUV | 0.080 | 0.743 | Low-intensity positive correlation, statistically insignificant |
| Age | 0.148 | 0.543 | Low-intensity positive correlation, statistically insignificant |
| T | 0.270 | 0.262 | Low-intensity positive correlation, statistically insignificant |
| N | –0.145 | 0.552 | Low-intensity negative correlation, statistically insignificant |
| M | –0.027 | 0.911 | Low-intensity negative correlation, statistically insignificant |
| L | –0.055 | 0.821 | Low-intensity negative correlation, statistically insignificant |
| V | –0.258 | 0.285 | Low-intensity negative correlation, statistically insignificant |
| R | 0.155 | 0524 | Low-intensity positive correlation, statistically insignificant |
| EET | –0.121 | 0.619 | Low-intensity negative correlation, statistically insignificant |
| Stage | 0.082 | 0.737 | Low-intensity positive correlation, statistically insignificant |
| Tg | 0.020 | 0.933 | Low-intensity positive correlation, statistically insignificant |
| Anti-Tg | –0.049 | 0.839 | Low-intensity negative correlation, statistically insignificant |
| Variable | Correlation Coefficient | p Value | Interpretation |
|---|---|---|---|
| SUV | 0.367 | 0.122 | Low-intensity positive correlation, statistically insignificant |
| BRAF V600E | 0.082 | 0.737 | Low-intensity positive correlation, statistically insignificant |
| Age | 0.653 | 0.002 | Positive medium-intensity, statistically significant correlation |
| T | −0.147 | 0.547 | Low-intensity negative correlation, statistically insignificant |
| N | −0.307 | 0.200 | Low-intensity negative correlation, statistically insignificant |
| M | 0.806 | 0.001 | Positive correlation of strong intensity, statistically significant |
| L | −0.015 | 0.95 | Low-intensity negative correlation, statistically insignificant |
| V | 0.145 | 0.551 | Low-intensity positive correlation, statistically insignificant |
| A | 0.180 | 0.460 | Low-intensity positive correlation, statistically insignificant |
| EET | −0.007 | 0.977 | Low-intensity negative correlation, statistically insignificant |
| Tg | 0.131 | 0.592 | Low-intensity positive correlation, statistically insignificant |
| Anti-Tg | 0.115 | 0.639 | Low-intensity positive correlation, statistically insignificant |
| Variable | Correlation Coefficient | p | Interpretation |
|---|---|---|---|
| Age | 0.251 | 0.483 | Low-intensity positive correlation, statistically insignificant |
| T | 0.128 | 0.722 | Low-intensity positive correlation, statistically insignificant |
| N | 0.277 | 0.437 | Low-intensity positive correlation, statistically insignificant |
| M | −0.017 | 0.96 | Low-intensity negative correlation, statistically insignificant |
| L | 0.566 | 0.087 | Positive medium-intensity, statistically insignificant correlation |
| V | 0.482 | 0.157 | Low-intensity positive correlation, statistically insignificant |
| R | 0.666 | 0.035 | Positive medium-intensity, statistically significant correlation |
| EET | −0.095 | 0.793 | Low-intensity negative correlation, statistically insignificant |
| Stage | 0.316 | 0.372 | Low-intensity positive correlation, statistically insignificant |
| Tg | 0.025 | 0.943 | Low-intensity positive correlation, statistically insignificant |
| Anti-Tg | −0.300 | 0.399 | Low-intensity negative correlation, statistically insignificant |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piciu, A.; Larg, M.-I.; Piciu, D. Correlation between F18-FDG PET/CT Imaging and BRAF V600E Genetic Mutation for the Early Assessment of Treatment Response in Papillary Thyroid Cancers. J. Pers. Med. 2020, 10, 52. https://doi.org/10.3390/jpm10020052
Piciu A, Larg M-I, Piciu D. Correlation between F18-FDG PET/CT Imaging and BRAF V600E Genetic Mutation for the Early Assessment of Treatment Response in Papillary Thyroid Cancers. Journal of Personalized Medicine. 2020; 10(2):52. https://doi.org/10.3390/jpm10020052
Chicago/Turabian StylePiciu, Andra, Maria-Iulia Larg, and Doina Piciu. 2020. "Correlation between F18-FDG PET/CT Imaging and BRAF V600E Genetic Mutation for the Early Assessment of Treatment Response in Papillary Thyroid Cancers" Journal of Personalized Medicine 10, no. 2: 52. https://doi.org/10.3390/jpm10020052
APA StylePiciu, A., Larg, M.-I., & Piciu, D. (2020). Correlation between F18-FDG PET/CT Imaging and BRAF V600E Genetic Mutation for the Early Assessment of Treatment Response in Papillary Thyroid Cancers. Journal of Personalized Medicine, 10(2), 52. https://doi.org/10.3390/jpm10020052