
Effectiveness of Cognitive Rehabilitation in Parkinson’s Disease: A Systematic Review and Meta-Analysis

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Quality Assessment and Risk of Bias in the Included Studies
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
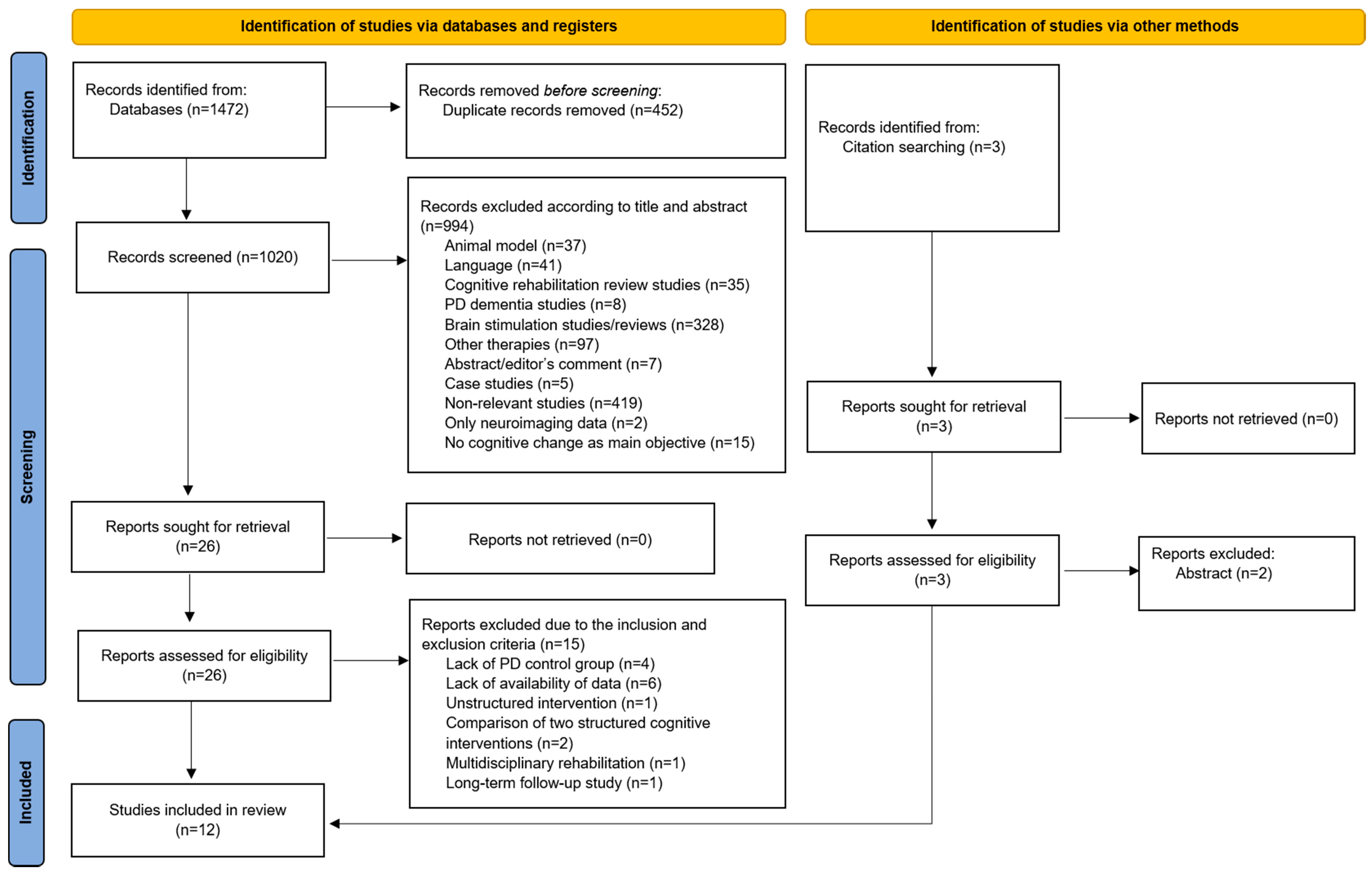
3.1. Study Selection
3.2. Study Characteristics
3.3. Effectiveness of Cognitive Rehabilitation
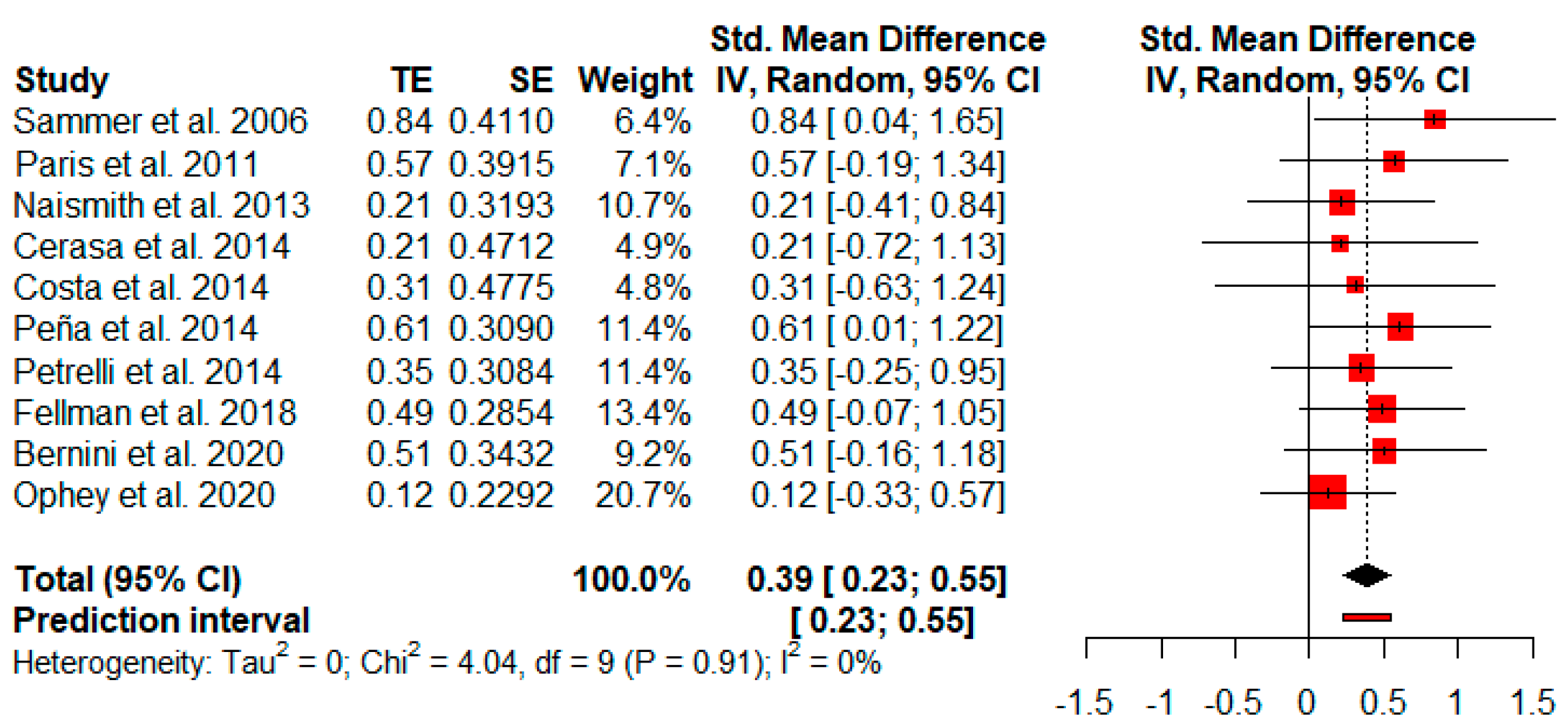
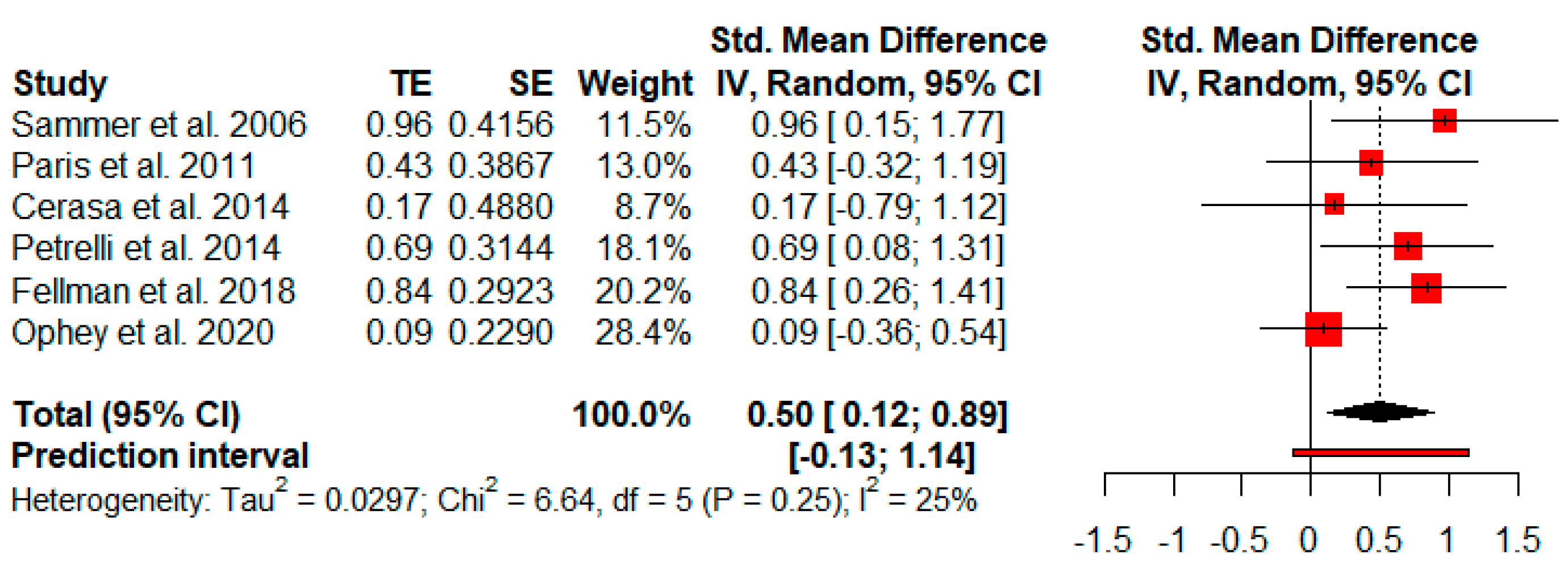
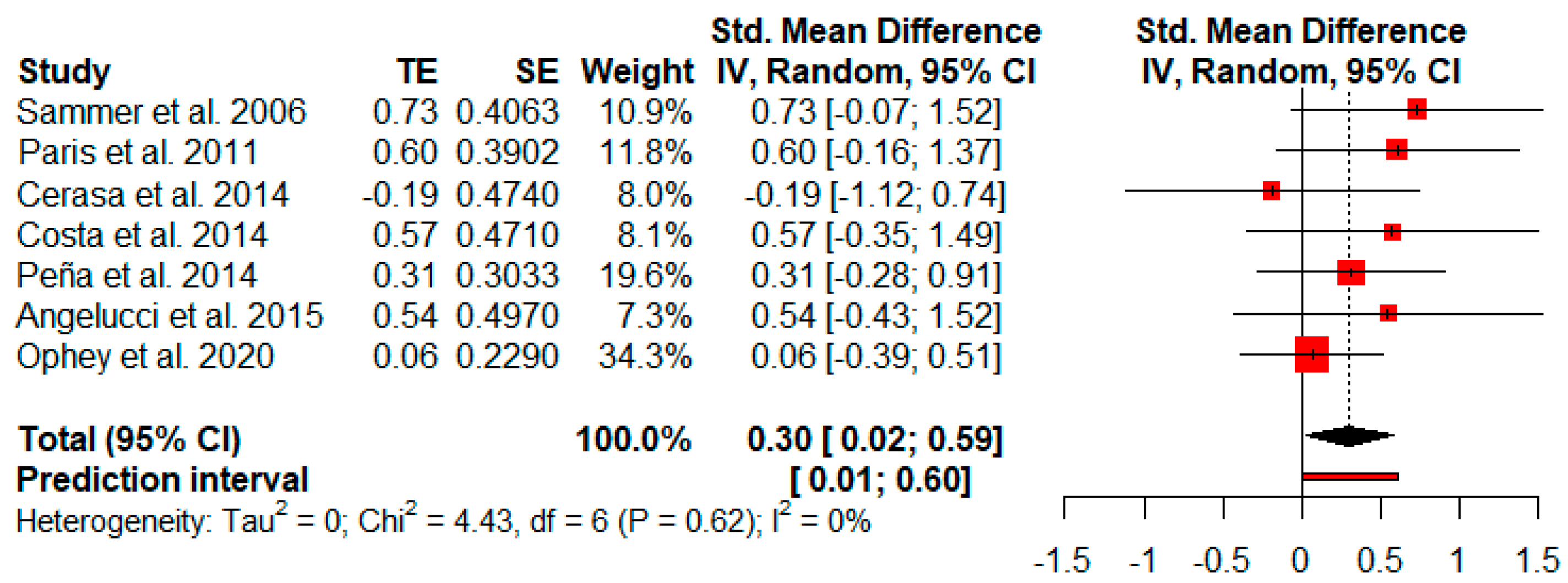
3.3.1. Overall Cognitive Functions
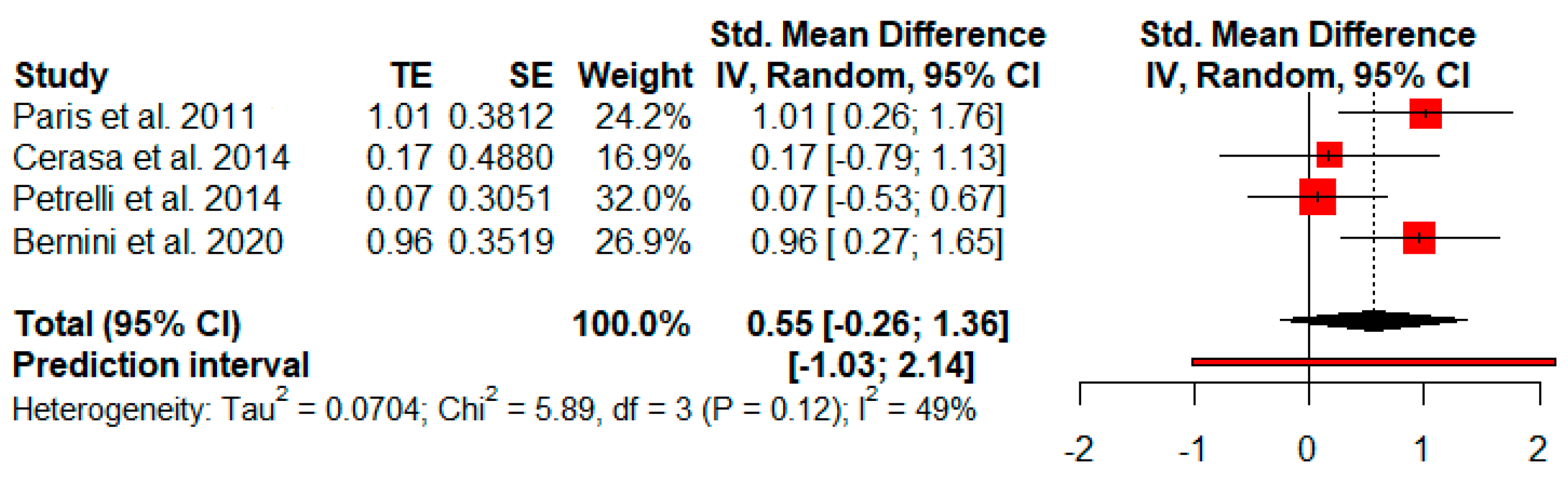
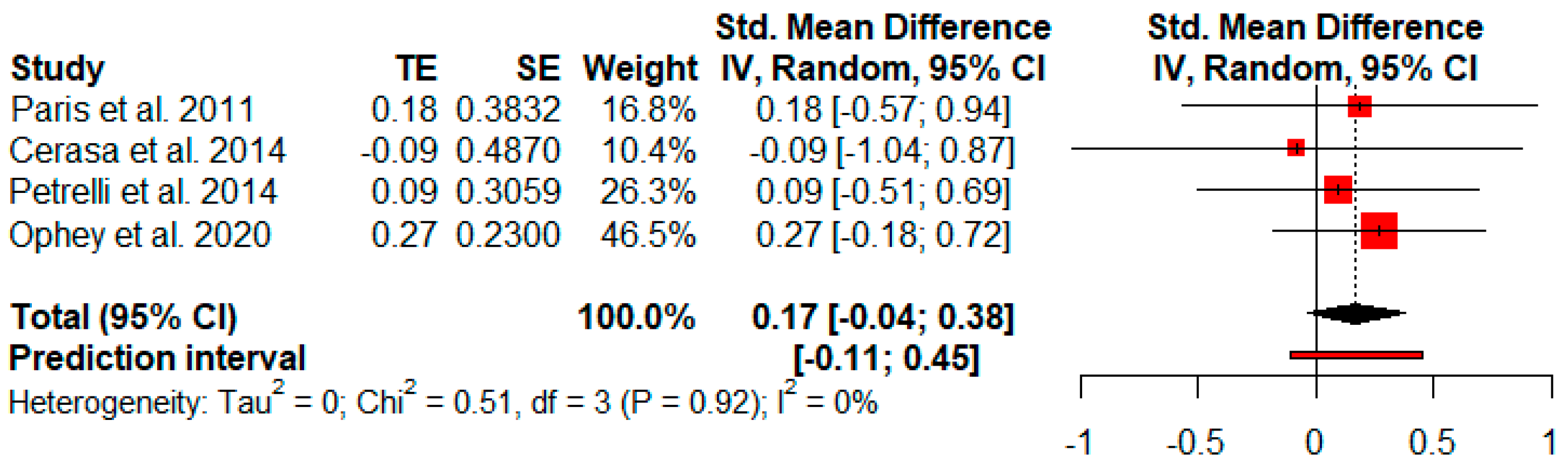
3.3.2. Global Cognitive Status
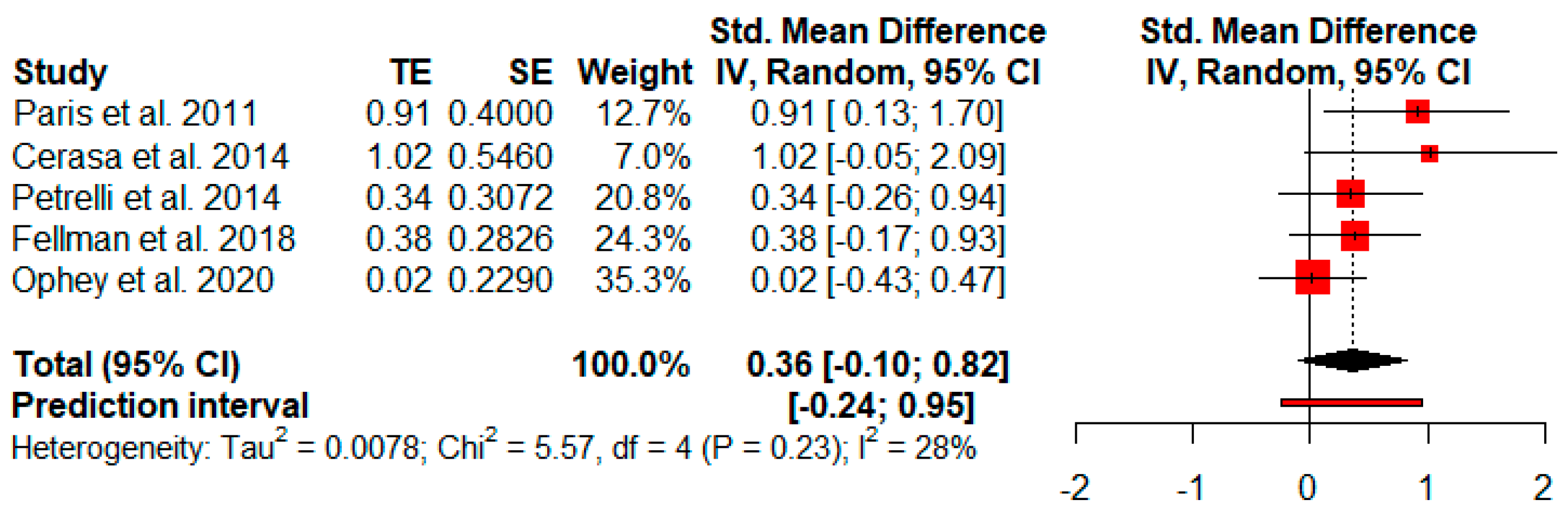
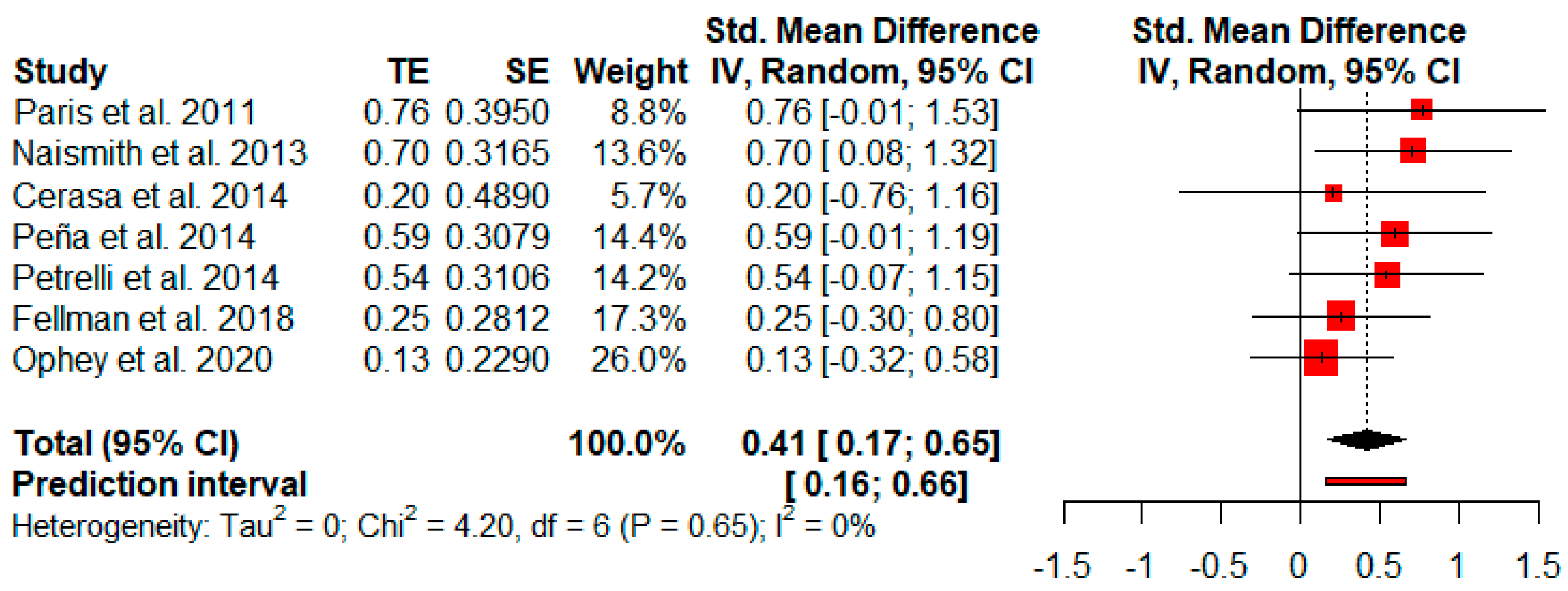
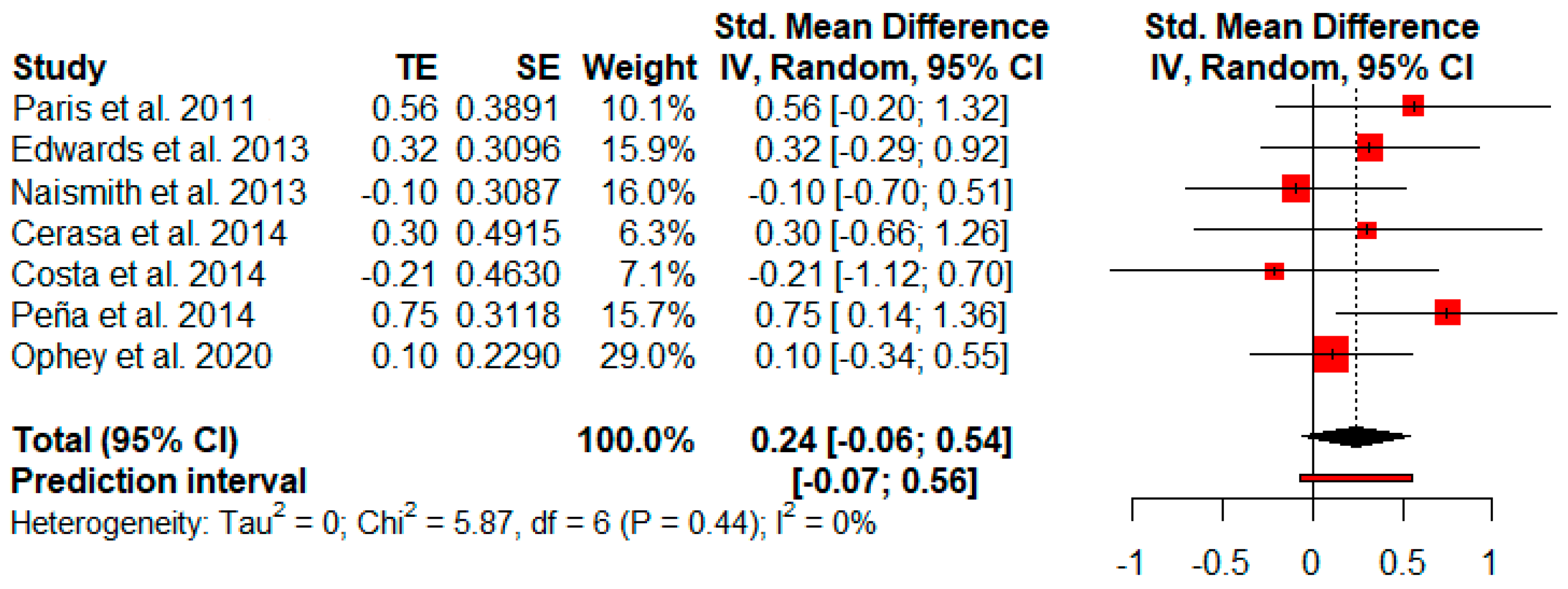
3.3.3. Attention
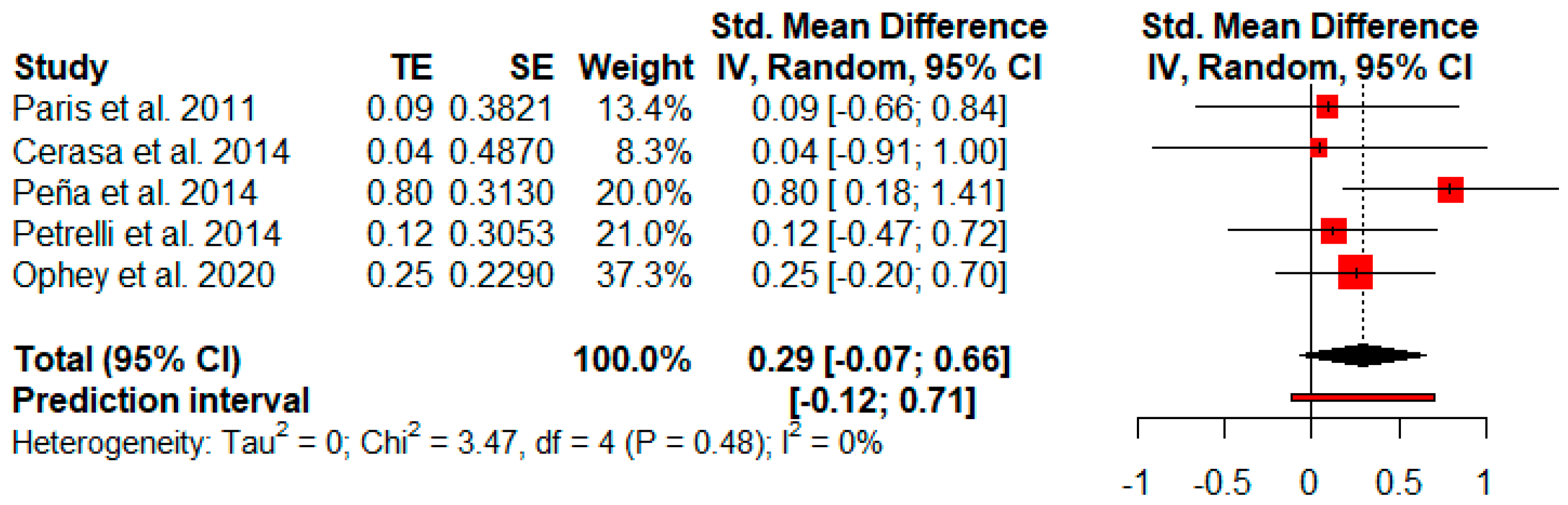
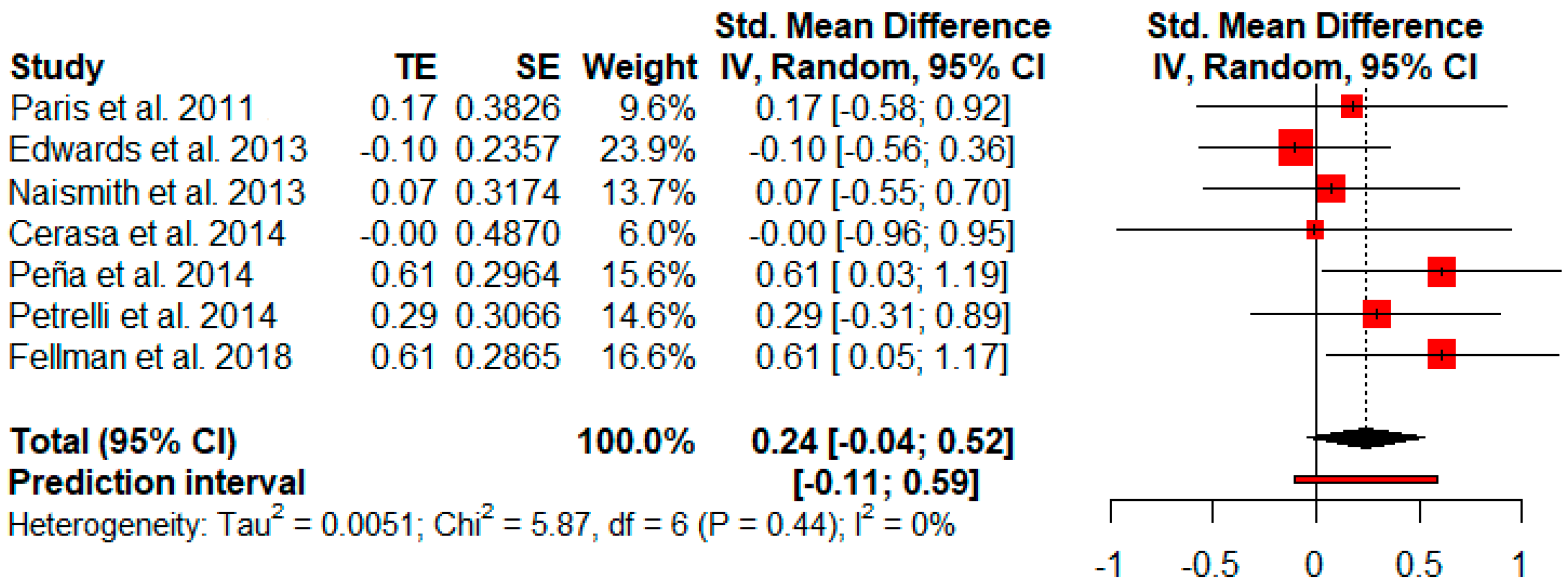
3.3.4. Working Memory
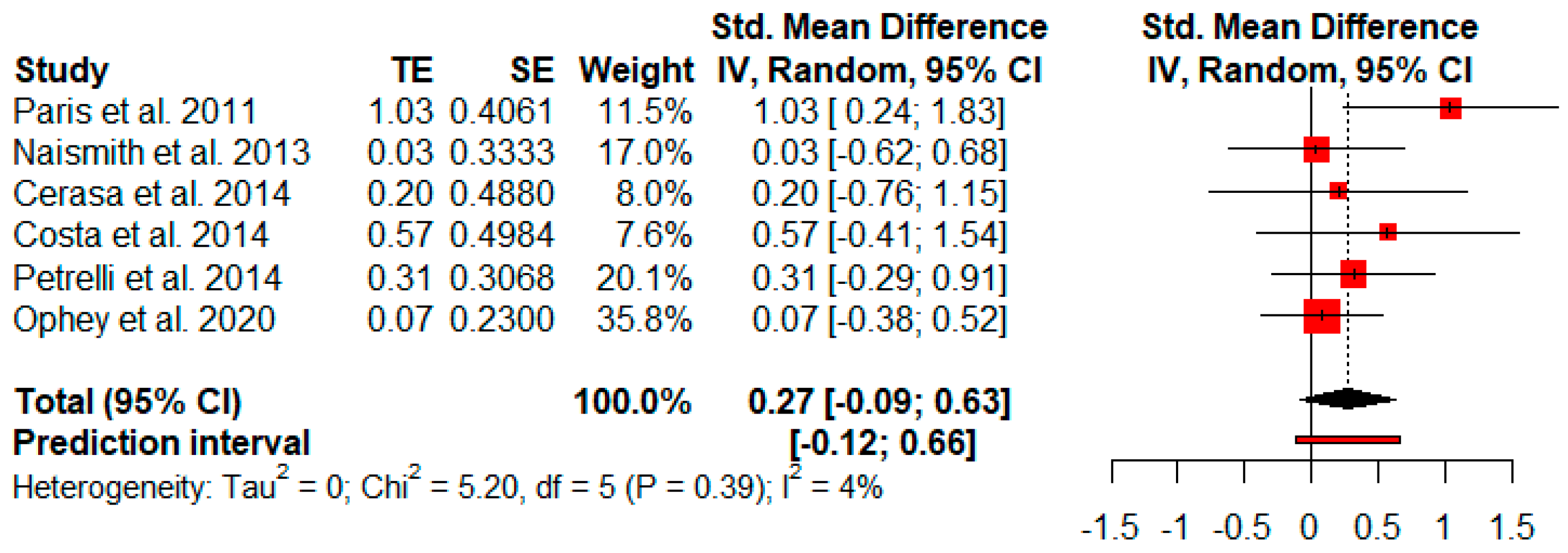
3.3.5. Verbal Memory
3.3.6. Visual Memory
3.3.7. Verbal Fluency
3.3.8. Executive Functions
3.3.9. Visuospatial and Visuoconstructive Abilities
3.3.10. Processing Speed
3.3.11. Others: Functionality, Depressive Symptoms and Quality of Life
3.4. Moderator Analyses
3.5. Publication Bias
3.6. Sensitivity Analyses
4. Discussion
5. Importance of Cognitive Rehabilitation in Personalized Medicine
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.-E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Prim. 2017, 3, 17013. [Google Scholar] [CrossRef] [PubMed]
- Schapira, A.H.; Chaudhuri, K.R.; Jenner, P. Non-motor features of Parkinson disease. Nat. Rev. Neurosci. 2017, 18, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Emre, M.; Aarsland, D.; Brown, R.; Burn, D.J.; Duyckaerts, C.; Mizuno, Y.; Broe, G.A.; Cummings, J.; Dickson, D.W.; Gauthier, S.; et al. Clinical diagnostic criteria for dementia associated with Parkinson’s disease. Mov. Disord. 2007, 22, 1689–1707. [Google Scholar] [CrossRef] [PubMed]
- Baiano, C.; Barone, P.; Trojano, L.; Santangelo, G. Prevalence and clinical aspects of mild cognitive impairment in Parkinson’s disease: A meta-analysis. Mov. Disord. 2020, 35, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Svenningsson, P.; Westman, E.; Ballard, C.; Aarsland, D. Cognitive impairment in patients with Parkinson’s disease: Diagnosis, biomarkers, and treatment. Lancet Neurol. 2012, 11, 697–707. [Google Scholar] [CrossRef]
- Aarsland, D.; Creese, B.; Politis, M.; Chaudhuri, K.R.; Ffytche, D.H.; Weintraub, D.; Ballard, C. Cognitive decline in Parkinson disease. Nat. Rev. Neurol. 2017, 13, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Sasikumar, S.; Strafella, A.P. Imaging mild cognitive impairment and dementia in Parkinson’s disease. Front. Neurol. 2020, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hely, M.A.; Reid, W.G.; Adena, M.A.; Halliday, G.M.; Morris, J.G. The Sydney multicenter study of Parkinson’s disease: The inevitability of dementia at 20 years. Mov. Disord. 2008, 23, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Van de Weijer, S.; Hommel, A.; Bloem, B.; Nonnekes, J.; De Vries, N. Promising non-pharmacological therapies in PD: Targeting late stage disease and the role of computer based cognitive training. Park. Relat. Disord. 2018, 46, S42–S46. [Google Scholar] [CrossRef] [PubMed]
- Titova, N.; Chaudhuri, K.R. Personalized medicine in Parkinson’s disease: Time to be precise. Mov. Disord. 2017, 32, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, H.; Venneri, A. Cognitive rehabilitation in Parkinson’s disease: A systematic review. J. Park. Dis. 2018, 8, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Biundo, R.; Weis, L.; Fiorenzato, E.; Antonini, A. Cognitive rehabilitation in Parkinson’s disease: Is it feasible? Arch. Clin. Neuropsychol. 2017, 32, 840–860. [Google Scholar] [CrossRef] [PubMed]
- Couture, M.; Giguère-Rancourt, A.; Simard, M. The impact of cognitive interventions on cognitive symptoms in idiopathic Parkinson’s disease: A systematic review. Aging Neuropsychol. Cogn. 2018, 26, 637–659. [Google Scholar] [CrossRef] [PubMed]
- Díez-Cirarda, M.; Ibarretxe-Bilbao, N.; Peña, J.; Ojeda, N. Neurorehabilitation in Parkinson’s disease: A critical review of cognitive rehabilitation effects on cognition and brain. Neural Plast. 2018, 2018, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hindle, J.V.; Petrelli, A.; Clare, L.; Kalbe, E. Nonpharmacological enhancement of cognitive function in Parkinson’s disease: A systematic review. Mov. Disord. 2013, 28, 1034–1049. [Google Scholar] [CrossRef] [PubMed]
- Glizer, D.; MacDonald, P.A. Cognitive training in Parkinson’s disease: A review of studies from 2000 to 2014. Park. Dis. 2016, 2016, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, B.J.; Gasson, N.; Bucks, R.S.; Troeung, L.; Loftus, A.M. Cognitive training and noninvasive brain stimulation for cognition in Parkinson’s disease: A meta-analysis. Neurorehabilit. Neural Repair 2017, 31, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Leung, I.H.; Walton, C.C.; Hallock, H.; Lewis, S.J.; Valenzuela, M.; Lampit, A. Cognitive training in Parkinson disease. Neurology 2015, 85, 1843–1851. [Google Scholar] [CrossRef] [PubMed]
- Orgeta, V.; McDonald, K.R.; Poliakoff, E.; Hindle, J.V.; Clare, L.; Leroi, I. Cognitive training interventions for dementia and mild cognitive impairment in Parkinson’s disease. Cochrane Database Syst. Rev. 2020, 2, CD011961. [Google Scholar] [CrossRef] [PubMed]
- Vlagsma, T.T.; Koerts, J.; Fasotti, L.; Tucha, O.; Van Laar, T.; Dijkstra, H.; Spikman, J.M. Parkinson’s patients’ executive profile and goals they set for improvement: Why is cognitive rehabilitation not common practice? Neuropsychol. Rehabil. 2015, 26, 216–235. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.; Brennan, S.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Version 6.2 (Updated February 2021); 2021; Available online: www.training.cochrane.org/handbook (accessed on 30 April 2021).
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martín, P.; Gil-Nagel, A.; Gracia, L.M.; Gómez, J.B.; Martínez-Sarriés, J.; Bermejo, F. The Cooperative Multicentric Group Unified Parkinson’s disease rating scale characteristics and structure. Mov. Disord. 1994, 9, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Cumming, G. Understanding the New Statistics: Effect Sizes, Confidence Intervals, and Meta-Analysis; Routledge: New York, NY, USA, 2012. [Google Scholar]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I² index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D.D. Doing Meta-Analysis in R: A Hands-on Guide; Chapman and Hall/CRC: Boca Raton, FL, USA, 2019. [Google Scholar] [CrossRef]
- Cheung, M.W.-L.; Vijayakumar, R. A Guide to Conducting a Meta-Analysis. Neuropsychol. Rev. 2016, 26, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Dickersin, K. The existence of publication bias and risk factors for its occurrence. JAMA 1990, 263, 1385–1389. [Google Scholar] [CrossRef] [PubMed]
- Rothstein, H.R.; Sutton, A.J.; Borenstein, M. Publication Bias in Meta-Analysis; John Wiley and Sons: Hoboken, NJ, USA, 2006; pp. 1–7. [Google Scholar]
- Egger, M.C.M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Sammer, G.; Reuter, I.; Hullmann, K.; Kaps, M.; Vaitl, D. Training of executive functions in Parkinson’s disease. J. Neurol. Sci. 2006, 248, 115–119. [Google Scholar] [CrossRef] [PubMed]
- París, A.P.; Saleta, H.G.; Maraver, M.D.L.C.C.; Silvestre, E.; Freixa, M.G.; Torrellas, C.P.; Pont, S.A.; Nadal, M.F.; Garcia, S.A.; Bartolomé, M.V.P.; et al. Blind randomized controlled study of the efficacy of cognitive training in Parkinson’s disease. Mov. Disord. 2011, 26, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.D.; Hauser, R.A.; O’Connor, M.L.; Valdés, E.G.; Zesiewicz, T.A.; Uc, E.Y. Randomized trial of cognitive speed of processing training in Parkinson disease. Neurology 2013, 81, 1284–1290. [Google Scholar] [CrossRef]
- Naismith, S.L.; Mowszowski, L.; Diamond, K.; Lewis, S.J. Improving memory in Parkinson’s disease: A healthy brain ageing cognitive training program. Mov. Disord. 2013, 28, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Cerasa, A.; Gioia, M.C.; Salsone, M.; Donzuso, G.; Chiriaco, C.; Realmuto, S.; Nicoletti, A.; Bellavia, G.; Banco, A.; D’Amelio, M.; et al. Neurofunctional correlates of attention rehabilitation in Parkinson’s disease: An explorative study. Neurol. Sci. 2014, 35, 1173–1180. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.; Peppe, A.; Serafini, F.; Zabberoni, S.; Barban, F.; Caltagirone, C.; Carlesimo, G.A. Prospective memory performance of patients with Parkinson’s disease depends on shifting aptitude: Evidence from cognitive rehabilitation. J. Int. Neuropsychol. Soc. 2014, 20, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Peña, J.; Ibarretxe-Bilbao, N.; García-Gorostiaga, I.; Gomez-Beldarrain, M.A.; Díez-Cirarda, M.; Ojeda, N. Improving functional disability and cognition in Parkinson disease: Randomized controlled trial. Neurology 2014, 83, 2167–2174. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, A.; Kaesberg, S.; Barbe, M.T.; Timmermann, L.; Fink, G.R.; Kessler, J.; Kalbe, E. Effects of cognitive training in Parkinson’s disease: A randomized controlled trial. Park. Relat. Disord. 2014, 20, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Eangelucci, F.; Epeppe, A.; Carlesimo, G.A.; Eserafini, F.; Ezabberoni, S.; Ebarban, F.; Eshofany, J.; Ecaltagirone, C.; Ecosta, A. A pilot study on the effect of cognitive training on BDNF serum levels in individuals with Parkinson’s disease. Front. Hum. Neurosci. 2015, 9, 130. [Google Scholar] [CrossRef] [PubMed]
- Fellman, D.; Salmi, J.; Ritakallio, L.; Ellfolk, U.; Rinne, J.O.; Laine, M. Training working memory updating in Parkinson’s disease: A randomised controlled trial. Neuropsychol. Rehabil. 2018, 30, 673–708. [Google Scholar] [CrossRef] [PubMed]
- Bernini, S.; Panzarasa, S.; Barbieri, M.; Sinforiani, E.; Quaglini, S.; Tassorelli, C.; Bottiroli, S. A double-blind randomized controlled trial of the efficacy of cognitive training delivered using two different methods in mild cognitive impairment in Parkinson’s disease: Preliminary report of benefits associated with the use of a computerized tool. Aging Clin. Exp. Res. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ophey, A.; Giehl, K.; Rehberg, S.; Eggers, C.; Reker, P.; van Eimeren, T.; Kalbe, E. Effects of working memory training in patients with Parkinson’s disease without cognitive impairment: A randomized controlled trial. Park. Relat. Disord. 2020, 72, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed]
- Titova, N.; Chaudhuri, K.R. Personalized medicine and nonmotor symptoms in Parkinson’s diseas. Int. Rev. Neurobiol. 2017, 134, 1257–1281. [Google Scholar] [PubMed]
- Calleo, J.; Burrows, C.; Levin, H.; Marsh, L.; Lai, E.; York, M.K. Cognitive rehabilitation for executive dysfunction in Parkinson’s disease: Application and current directions. Park. Dis. 2011, 2012, 1–6. [Google Scholar] [CrossRef]
- Wykes, T.; Reeder, C.; Landau, S.; Matthiasson, P.; Haworth, E.; Hutchinson, C. Does age matter? Effects of cognitive rehabilitation across the age span. Schizophr. Res. 2009, 113, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Kontis, D.; Huddy, V.; Reeder, C.; Landau, S.; Wykes, T. Effects of age and cognitive reserve on cognitive remediation therapy outcome in patients with schizophrenia. Am. J. Geriatr. Psychiatry 2013, 21, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Küster, O.C.; Fissler, P.; Laptinskaya, D.; Thurm, F.; Scharpf, A.; Woll, A.; Kolassa, S.; Kramer, A.F.; Elbert, T.; Von Arnim, C.A.F.; et al. Cognitive change is more positively associated with an active lifestyle than with training interventions in older adults at risk of dementia: A controlled interventional clinical trial. BMC Psychiatry 2016, 16, 315. [Google Scholar] [CrossRef]
- Klein, C.; Westenberger, A. Genetics of Parkinson’s disease. Cold Spring Harb. Perspect. Med. 2012, 2, a008888. [Google Scholar] [CrossRef] [PubMed]
- Fagan, E.S.; Pihlstrøm, L. Genetic risk factors for cognitive decline in Parkinson’s disease: A review of the literature. Eur. J. Neurol. 2017, 24, 561-e20. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.; Fitzpatrick, R.; Doll, H.; Playford, D.; Jenkinson, C. Does self-reported well-being of patients with Parkinson’s disease influence caregiver strain and quality of life? Park. Relat. Disord. 2011, 17, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martín, P.; Rodríguez-Blázquez, C.; Forjaz, M.J. Quality of life and burden in caregivers for patients with Parkinson’s disease: Concepts, assessment and related factors. Expert Rev. Pharm. Outcomes Res. 2012, 12, 221–230. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Sample | Characteristics of the Sample | H&Y Stages | Intervention | Format | Duration | Domains Trained | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Sammer et al., 2006 [36] | 26 PD 12 PD-CR 14 PD-ACG | Age: 70.8 PD-CR 68.5 PD-ACG Years of education: - | 2–3 | CR: Executive Function Training (Paper) ACG: Standard Treatment (Occupational Therapy, Physical Therapy and Treatment) (Paper) | Group | 10 sessions 30 min/session | -Working memory -Executive functions | Improvements in PD-CR: -Executive functions |
| París et al., 2011 [37] | 28 PD 12 PD-CR 16 PD-CG | Age: 64.7 PD-CR 65.4 PD-CG Years of education: 9.8 PD-CR 9.5 PD-CG | 1–3 | “SmartBrain Tool” (Paper + Computer) | Group + home | 12 sessions 3 times/week 4 weeks 45 min/session | -Attention -Memory -Psychomotor speed -Executive functions -Visuospatial abilities -Language -Calculation abilities | Improvements in PD-CR: -Attention -Processing speed -Visual memory -Visuospatial and visuoconstructive abilities -Semantic fluency -Executive functions |
| Edwards et al., 2013 [38] | 74 PD 32 PD-CR 42 PD-CG | Age: 69.4 PD-CR 68.2 PD-CG Years of education: 14.8 PD-CR 15.4 PD-CG | 1–3 | “Insight Software” (Computer) | Home | 36 sessions 3 times/week 3 months 60 min/session | -Processing speed | Improvements in PD-CR: -Processing speed |
| Naismith et al., 2013 [39] | 50 PD 35 PD-CR 15 PD-CG | Age: 68.5 PD-CR 64.9 PD-CG Years of education: 14.9 PD-CR 14.0 PD-CG | 1–3 | Cognitive training (Neuropsychological Educational Approach to Remediation (NEAR)) + Psychoeducation (Computer) | Group | 14 sessions 7 weeks 2 times/week 60 min of CR 60 min psycho-education | -Memory -Psychomotor speed -Mental flexibility -Verbal fluency | Improvements in PD-CR: -Verbal memory |
| Cerasa et al., 2014 [40] | 15 PD 8 PD-CR 7 PD-CG | Age: 61.1 PD-CR 58.3 PD-CG Years of education: 8 PD-CR 8 PD-CG | 1–3 | CR: “Rehacom” CG: Simple visuomotor coordination tapping task (Computer) | Group (CR) + Individual (CG) | 6 weeks 2 times/week 60 min/session | -Attention -Information processing task | Improvements in PD-CR: -Attention/ Processing speed -Working memory Increased functional brain activity: -Left dorsolateral prefrontal cortex -Superior left parietal cortex |
| Costa et al., 2014 [41] | 17 PD-MCI 9 PD-CR 8 PD-CG | Age: 66.1 PD-CR 70.9 PD-CG Years of education: 11.2 PD-CR 10.6 PD-CG | 1–3 | CR: Cognitive change training CG: Breathing training (Paper) | - | 4 weeks 3 times/week 45 min/session | -Shifting abilities (Verbal fluency and Trail Making Test) | Improvements in PD-CR: -Verbal fluency -Trail Making Test -Prospective memory procedures |
| Peña et al., 2014 [42] | 42 PD 20 PD-CR 22 PD-ACG | Age: 67.7 PD-CR 68.1 PD-ACG Years of education: 10.5 PD-CR 10.2 PD-ACG | 1–3 | CR: “REHACOP” ACG: Occupational activities (Paper) | Group | 39 sessions 13 weeks 2 times/week 60 min/session | -Attention -Memory -Language -Executive functions -Social cognition -Processing speed | Improvements in PD-CR: -Processing speed -Visual memory -Social cognition -Functional disability |
| Petrelli et al., 2014 [43] | 65 PD 22 PD-NV 22 PD-MF 21 PD-CG | Age: 69.2 PD-NV 68.8 PD-MF 69.1 PD-CG Years of education: 13.1 PD-NV 13.6 PD-MF 12.8 PD-CG | 1–3 | NV: “NEUROvitalis” (Computer) MF: “Mentally fit” (Paper) | Group + Individual | 12 sessions 6 weeks 2 times/week 90 min/session | NV -Attention -Verbal memory -Visual memory -Executive functions MF -Attention -Memory -Creativity | Improvements in PD-NV versus PD-CG: -Working memory -Verbal memory Improvements in PD-MF versus PD-CG: -Depressive symptoms Improvements in PD-NV versus PD-MF: -Working memory |
| Angelucci et al., 2015 [44] | 15 PD-MCI 7 PD-CR 8 PD-CG | Age: 67.6 PD-CR 71.9 PD-CG Years of education: 11.7 PD-CR 10.6 PD-CG | - | CR: Cognitive change training CG: Simple cognitive tests (Paper) | - | 12 sessions 4 weeks 3 times/week 45 min/session | -Executive functions | Improvements in PD-CR: -Executive functions |
| Fellman et al., 2018 [45] | 52 PD 26 PD-CR 26 PD-ACG | Age: 64.8 PD-CR 65.5 PD-ACG Years of education: 5.3 PD-CR 5.5 PD-ACG | - | CR: Working memory ACG: Online quiz task “Älypää” (Computer) | Home | 3 weeks 3 times/week 30 min/session | -Working memory | Improvements in PD-CR: -Working memory -Depressive symptoms |
| Bernini et al., 2020 [46] | 53 PD 18 PD-CCT 12 PD-PCT 18 PD-CG | Age: 74.6 PD-CCT 69.8 PD-PCT 69.3 PD-CG Years of education: 9.5 PD-CCT 8.0 PD-PCT 7.6 PD-CG | ≤3 | CCT: “CoRe” (Computer) PCT: “CoRe” (Paper) CG: Unstructured activities | Group | 3 weeks 4 times/week 45 min/session | -Logical executive functions -Attention/processing speed -Working memory -Episodic long-term memory | Improvements in PD-CCT versus PD-PCT: -Global cognition Improvements in PD-CCT versus CG: -Global cognition -Attention/processing speed |
| Ophey et al., 2020 [47] | 75 PD 37 PD-CR 38 PD-CG | Age: 64.0 PD-CR 63.8 PD-CG Years of education: 15.0 PD-CR 15.5 PD-CG | 2–3 | CR: “NeuroNation” (Computer) | Individual + home | 5 weeks 5 times/week 30 min/session | -Working memory | Improvements in PD-CR: -No improvements Assesment after 3 months: -Verbal working memory -Visuoconstructive abilities |
| Model Number | Predictor Variables | k | df | Fmoderator | Qresidual | R2 | β | p |
|---|---|---|---|---|---|---|---|---|
| 1 | Age of participants | 10 | 8 | 3.96 | 2.70 | 0% | 0.04 | 0.08 |
| 2 | Years of education | 9 | 7 | 4.45 | 4.45 | 0% | −0.03 | 0.07 |
| 3 | H&Y | 8 | 6 | 2.03 | 2.79 | 0% | 0.66 | 0.20 |
| 4 | Duration of PD (years) | 9 | 7 | 1.10 | 2.36 | 0% | 0.01 | 0.32 |
| 5 | Baseline global cognitive scores | 10 | 8 | 0.30 | 3.90 | 0% | 0.00 | 0.60 |
| 6 | Total number of conducted sessions | 10 | 8 | 0.02 | 4.03 | 0% | −0.00 | 0.89 |
| 7 | Training session duration (min) | 10 | 8 | 0.02 | 4.03 | 0% | 0.01 | 0.87 |
| 8 | Frequency of weekly sessions | 9 | 7 | 1.72 | 2.19 | 0% | −0.08 | 0.23 |
| 9 | UPDRS-III | 8 | 6 | 0.03 | 2.4 | 0% | 0.01 | 0.87 |
| 10 | Tools for cognitive training (pencil & paper or computer) | 10 | 7 | 1.71 | 2.71 | 0% | −0.12 | 0.24 |
| 11 | Age × Years of education | 9 | 5 | 2.71 | 1.04 | 0% | 0.01 | 0.15 |
| 12 | Duration of PD × H&Y | 8 | 4 | 1.70 | 1.64 | 0% | −0.06 | 0.30 |
| 13 | H&Y × UPDRS-III | 6 | 2 | 0.43 | 1.05 | 0% | −1.54 | 0.75 |
| 14 | Total number of sessions conducted × Training session duration (min) | 10 | 6 | 4.04 | 1.33 | 0% | 0.00 | 0.07 |
| 15 | Total number of sessions conducted × Frequency of weekly sessions | 9 | 5 | 4.41 | 0.75 | 0% | −0.02 | 0.04 * |
| 16 | Training session duration (min) × Frequency of weekly sessions | 9 | 5 | 2.21 | 1.17 | 0% | 0.01 | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanchez-Luengos, I.; Balboa-Bandeira, Y.; Lucas-Jiménez, O.; Ojeda, N.; Peña, J.; Ibarretxe-Bilbao, N. Effectiveness of Cognitive Rehabilitation in Parkinson’s Disease: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 429. https://doi.org/10.3390/jpm11050429
Sanchez-Luengos I, Balboa-Bandeira Y, Lucas-Jiménez O, Ojeda N, Peña J, Ibarretxe-Bilbao N. Effectiveness of Cognitive Rehabilitation in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(5):429. https://doi.org/10.3390/jpm11050429
Chicago/Turabian StyleSanchez-Luengos, Itsasne, Yolanda Balboa-Bandeira, Olaia Lucas-Jiménez, Natalia Ojeda, Javier Peña, and Naroa Ibarretxe-Bilbao. 2021. "Effectiveness of Cognitive Rehabilitation in Parkinson’s Disease: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 5: 429. https://doi.org/10.3390/jpm11050429
APA StyleSanchez-Luengos, I., Balboa-Bandeira, Y., Lucas-Jiménez, O., Ojeda, N., Peña, J., & Ibarretxe-Bilbao, N. (2021). Effectiveness of Cognitive Rehabilitation in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 11(5), 429. https://doi.org/10.3390/jpm11050429