
Elevated De Ritis Ratio as a Predictor for Acute Kidney Injury after Radical Retropubic Prostatectomy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
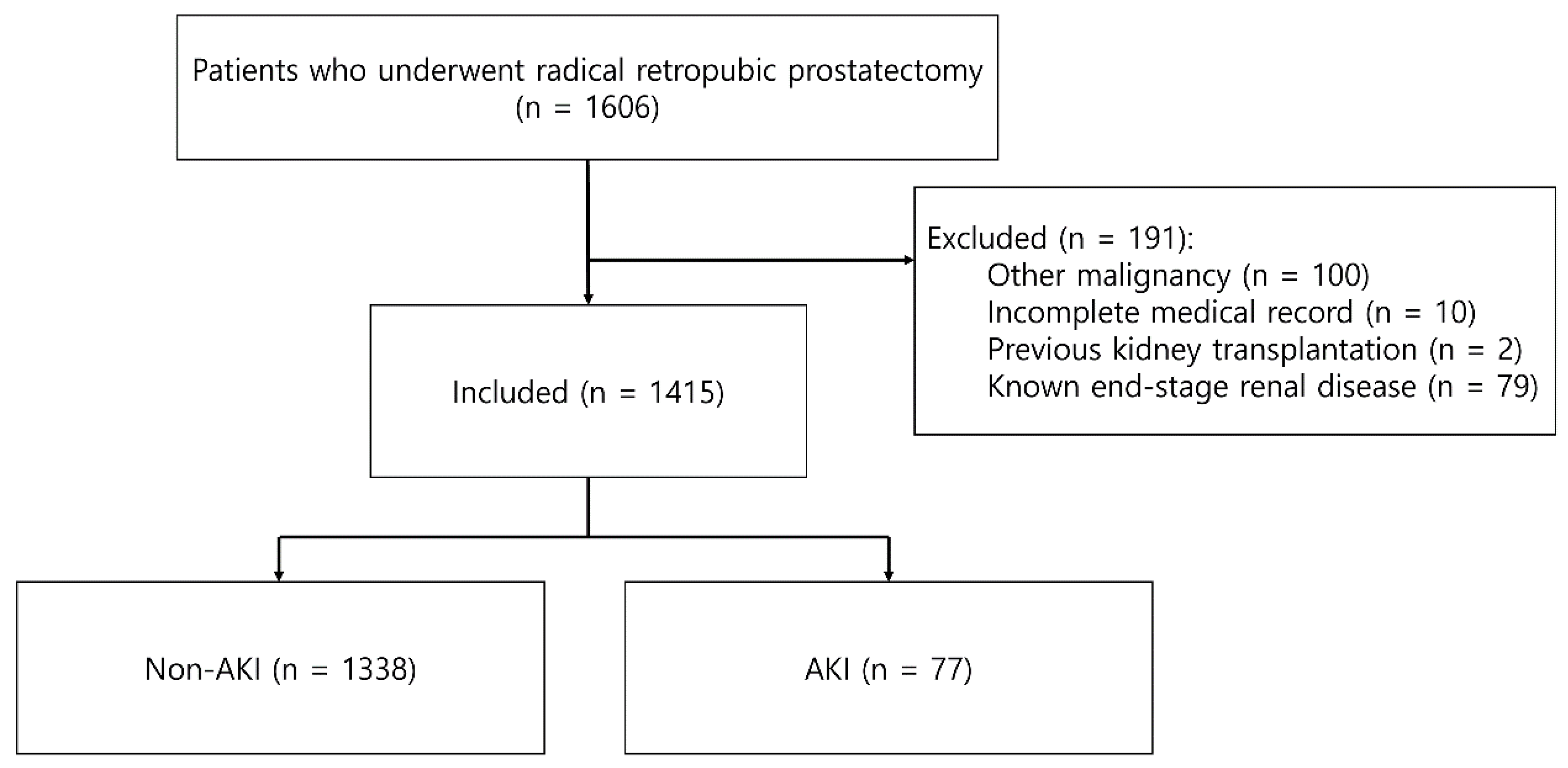
2.1. Patients
2.2. Anesthesia and Monitoring
2.3. Surgical Protocol
2.4. Data Collection
2.5. Definitions of the De Ritis Ratio and AKI
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Gainsburg, D.M. Anesthetic concerns for robotic-assisted laparoscopic radical prostatectomy. Minerva Anestesiol. 2012, 78, 596–604. [Google Scholar] [PubMed]
- Basiri, A.; de la Rosette, J.J.; Tabatabaei, S.; Woo, H.H.; Laguna, M.P.; Shemshaki, H. Comparison of retropubic, laparoscopic and robotic radical prostatectomy: Who is the winner? World J. Urol. 2018, 36, 609–621. [Google Scholar] [CrossRef] [PubMed]
- Joo, E.Y.; Moon, Y.J.; Yoon, S.H.; Chin, J.H.; Hwang, J.H.; Kim, Y.K. Comparison of Acute Kidney Injury After Robot-Assisted Laparoscopic Radical Prostatectomy Versus Retropubic Radical Prostatectomy: A Propensity Score Matching Analysis. Medicine 2016, 95, e2650. [Google Scholar] [CrossRef]
- Gumbert, S.D.; Kork, F.; Jackson, M.L.; Vanga, N.; Ghebremichael, S.J.; Wang, C.Y.; Eltzschig, H.K. Perioperative Acute Kidney Injury. Anesthesiology 2020, 132, 180–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ritis, F.; Coltorti, M.; Giusti, G. An enzymic test for the diagnosis of viral hepatitis; the transaminase serum activities. Clin. Chim. Acta 1957, 2, 70–74. [Google Scholar] [CrossRef]
- Yu, J.; Kim, H.Y.; Kong, Y.G.; Park, J.H.; Seo, Y.J.; Kim, Y.K. De Ritis ratio as a predictor of 1-year mortality after burn surgery. Burns 2021, in press. [Google Scholar] [CrossRef]
- Riedl, J.M.; Posch, F.; Prager, G.; Eisterer, W.; Oehler, L.; Sliwa, T.; Wilthoner, K.; Petzer, A.; Pichler, P.; Hubmann, E.; et al. The AST/ALT (De Ritis) ratio predicts clinical outcome in patients with pancreatic cancer treated with first-line nab-paclitaxel and gemcitabine: Post hoc analysis of an Austrian multicenter, noninterventional study. Ther. Adv. Med. Oncol. 2020, 12, 1758835919900872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knittelfelder, O.; Delago, D.; Jakse, G.; Reinisch, S.; Partl, R.; Stranzl-Lawatsch, H.; Renner, W.; Langsenlehner, T. The AST/ALT (De Ritis) Ratio Predicts Survival in Patients with Oral and Oropharyngeal Cancer. Diagnostics 2020, 10, 973. [Google Scholar] [CrossRef]
- Gorgel, S.N.; Kose, O.; Koc, E.M.; Ates, E.; Akin, Y.; Yilmaz, Y. The prognostic significance of preoperatively assessed AST/ALT (De Ritis) ratio on survival in patients underwent radical cystectomy. Int. Urol. Nephrol. 2017, 49, 1577–1583. [Google Scholar] [CrossRef]
- Ikeda, T.; Ishihara, H.; Takagi, T.; Fukuda, H.; Yoshida, K.; Iizuka, J.; Kobayashi, H.; Okumi, M.; Ishida, H.; Kondo, T.; et al. The De Ritis (Aspartate Transaminase/Alanine Transaminase) Ratio as a Prognosticator in Patients With End-stage Renal Disease-associated Renal Cell Carcinoma. Clin. Genitourin. Cancer 2020, 18, 236–240.e231. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Chen, C.; Lu, J.; Zheng, J.; Ma, X.C.; Yuan, X.Y.; Huo, K.; Han, J.F. De Ritis ratio (AST/ALT) as an independent predictor of poor outcome in patients with acute ischemic stroke. Neuropsychiatr. Dis. Treat. 2017, 13, 1551–1557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinellu, A.; Arru, F.; De Vito, A.; Sassu, A.; Valdes, G.; Scano, V.; Zinellu, E.; Perra, R.; Madeddu, G.; Carru, C.; et al. The De Ritis ratio as prognostic biomarker of in-hospital mortality in COVID-19 patients. Eur. J. Clin. Investig. 2021, 51, e13427. [Google Scholar] [CrossRef]
- Djavan, B.; Kazzazi, A.; Dulabon, L.; Momtahen, S.; Dianat, S.S.; Sand, M.; Cheetham, P.; Janetschek, G.; Lepor, H.; Graefen, M. Indications and trends in pelvic lymph node dissection for prostate cancer. Eur. Urol. Suppl. 2011, 10, e38–e43. [Google Scholar] [CrossRef]
- Tarantino, G.; Crocetto, F.; Vito, C.D.; Martino, R.; Pandolfo, S.D.; Creta, M.; Aveta, A.; Buonerba, C.; Imbimbo, C. Clinical factors affecting prostate-specific antigen levels in prostate cancer patients undergoing radical prostatectomy: A retrospective study. Future Sci. OA 2021, 7, Fso643. [Google Scholar] [CrossRef]
- Yu, J.; Hong, B.; Park, J.Y.; Lee, Y.; Hwang, J.H.; Kong, Y.G.; Kim, Y.K. Comparison of a Significant Decline in the Glomerular Filtration Rate between Ileal Conduit and Ileal Neobladder Urinary Diversions after Radical Cystectomy: A Propensity Score-Matched Analysis. J. Clin. Med. 2020, 9, 2236. [Google Scholar] [CrossRef]
- McNeal, J.E.; Villers, A.A.; Redwine, E.A.; Freiha, F.S.; Stamey, T.A. Capsular penetration in prostate cancer. Significance for natural history and treatment. Am. J. Surg. Pathol. 1990, 14, 240–247. [Google Scholar] [CrossRef]
- Sofer, M.; Savoie, M.; Kim, S.S.; Civantos, F.; Soloway, M.S. Biochemical and pathological predictors of the recurrence of prostatic adenocarcinoma with seminal vesicle invasion. J. Urol. 2003, 169, 153–156. [Google Scholar] [CrossRef]
- Cheng, L.; Slezak, J.; Bergstralh, E.J.; Myers, R.P.; Zincke, H.; Bostwick, D.G. Preoperative prediction of surgical margin status in patients with prostate cancer treated by radical prostatectomy. J. Clin. Oncol. 2000, 18, 2862–2868. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Kong, Y.G.; Park, J.H.; Kim, Y.K. Acute kidney injury after burn surgery: Preoperative neutrophil/lymphocyte ratio as a predictive factor. Acta Anaesthesiol. Scand. 2019, 63, 240–247. [Google Scholar] [CrossRef]
- Joung, K.W.; Choi, S.S.; Kong, Y.G.; Yu, J.; Lim, J.; Hwang, J.H.; Kim, Y.K. Incidence and Risk Factors of Acute Kidney Injury after Radical Cystectomy: Importance of Preoperative Serum Uric Acid Level. Int. J. Med. Sci. 2015, 12, 599–604. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Park, J.Y.; Ha, S.; Hwang, J.H.; Kim, Y.K. C-reactive Protein/Albumin Ratio and Acute Kidney Injury after Radical Cystectomy among Elderly Patients: A Propensity Score-Matched Analysis. Dis. Markers 2020, 2020, 8818445. [Google Scholar] [CrossRef]
- Okusa, M.D.; Davenport, A. Reading between the (guide)lines--the KDIGO practice guideline on acute kidney injury in the individual patient. Kidney Int. 2014, 85, 39–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kork, F.; Balzer, F.; Spies, C.D.; Wernecke, K.D.; Ginde, A.A.; Jankowski, J.; Eltzschig, H.K. Minor Postoperative Increases of Creatinine Are Associated with Higher Mortality and Longer Hospital Length of Stay in Surgical Patients. Anesthesiology 2015, 123, 1301–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakar, C.V.; Christianson, A.; Freyberg, R.; Almenoff, P.; Render, M.L. Incidence and outcomes of acute kidney injury in intensive care units: A Veterans Administration study. Crit. Care Med. 2009, 37, 2552–2558. [Google Scholar] [CrossRef]
- Botros, M.; Sikaris, K.A. The de ritis ratio: The test of time. Clin. Biochem. Rev. 2013, 34, 117–130. [Google Scholar] [PubMed]
- Lee, H.; Lee, S.E.; Byun, S.S.; Kim, H.H.; Kwak, C.; Hong, S.K. De Ritis ratio (aspartate transaminase/alanine transaminase ratio) as a significant prognostic factor after surgical treatment in patients with clear-cell localized renal cell carcinoma: A propensity score-matched study. BJU Int. 2017, 119, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Tarantino, G.; Crocetto, F.; Di Vito, C.; Creta, M.; Martino, R.; Pandolfo, S.D.; Pesce, S.; Napolitano, L.; Capone, D.; Imbimbo, C. Association of NAFLD and Insulin Resistance with Non Metastatic Bladder Cancer Patients: A Cross-Sectional Retrospective Study. J. Clin. Med. 2021, 10, 346. [Google Scholar] [CrossRef]
- Yuk, H.D.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. De Ritis Ratio (Aspartate Transaminase/Alanine Transaminase) as a Significant Prognostic Factor in Patients Undergoing Radical Cystectomy with Bladder Urothelial Carcinoma: A Propensity Score-Matched Study. Dis. Markers 2019, 2019, 6702964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canat, L.; Ataly, H.A.; Agalarov, S.; Alkan, I.; Altunrende, F. The effect of AST/ALT (De Ritis) ratio on survival and its relation to tumor histopathological variables in patients with localized renal cell carcinoma. Int. Braz. J. Urol. 2018, 44, 288–295. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Chen, L.; Wang, Y.; Tan, W.; Huang, Z. Prognostic value of aspartate transaminase to alanine transaminase (De Ritis) ratio in solid tumors: A pooled analysis of 9,400 patients. Onco Targets Ther. 2019, 12, 5201–5213. [Google Scholar] [CrossRef] [Green Version]
- Ewid, M.; Sherif, H.; Allihimy, A.S.; Alharbi, S.A.; Aldrewesh, D.A.; Alkuraydis, S.A.; Abazid, R. AST/ALT ratio predicts the functional severity of chronic heart failure with reduced left ventricular ejection fraction. BMC Res. Notes 2020, 13, 178. [Google Scholar] [CrossRef] [PubMed]
- Greco, F.; Hoda, M.R.; Wagner, S.; Reichelt, O.; Inferrera, A.; Fischer, K.; Fornara, P. Adipocytokine: A new family of inflammatory and immunologic markers of invasiveness in major urologic surgery. Eur. Urol. 2010, 58, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Homburger, J.A.; Meiler, S.E. Anesthesia drugs, immunity, and long-term outcome. Curr. Opin. Anaesthesiol. 2006, 19, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Dupré, A.; Malik, H.Z. Inflammation and cancer: What a surgical oncologist should know. Eur. J. Surg. Oncol. 2018, 44, 566–570. [Google Scholar] [CrossRef]
- Sfanos, K.S.; De Marzo, A.M. Prostate cancer and inflammation: The evidence. Histopathology 2012, 60, 199–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, C.; Olivieri, O.; Girelli, D.; Faccini, G.; Zenari, M.L.; Lombardi, S.; Corrocher, R. Anti-oxidant status and lipid peroxidation in patients with essential hypertension. J. Hypertens. 1998, 16, 1267–1271. [Google Scholar] [CrossRef]
- Lenda, D.M.; Sauls, B.A.; Boegehold, M.A. Reactive oxygen species may contribute to reduced endothelium-dependent dilation in rats fed high salt. Am. J. Physiol. Heart Circ. Physiol. 2000, 279, H7–H14. [Google Scholar] [CrossRef]
- Xu, J.; Xia, Y.; Li, S.; Cheng, X.; Hu, S.; Gao, Y.; Zhou, X.; Wang, G.; Zheng, Q. A retrospective pilot study to examine the potential of aspartate aminotransferase to alanine aminotransferase ratio as a predictor of postoperative acute kidney injury in patients with hepatocellular carcinoma. Ann. Clin. Biochem. 2019, 56, 357–366. [Google Scholar] [CrossRef]
- George, T.J.; Arnaoutakis, G.J.; Beaty, C.A.; Pipeling, M.R.; Merlo, C.A.; Conte, J.V.; Shah, A.S. Acute kidney injury increases mortality after lung transplantation. Ann. Thorac. Surg. 2012, 94, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Margarson, M.P.; Soni, N. Serum albumin: Touchstone or totem? Anaesthesia 1998, 53, 789–803. [Google Scholar] [CrossRef]
- Gibbs, J.; Cull, W.; Henderson, W.; Daley, J.; Hur, K.; Khuri, S.F. Preoperative serum albumin level as a predictor of operative mortality and morbidity: Results from the National VA Surgical Risk Study. Arch. Surg. 1999, 134, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Karas, P.L.; Goh, S.L.; Dhital, K. Is low serum albumin associated with postoperative complications in patients undergoing cardiac surgery? Interact. Cardiovasc. Thorac. Surg. 2015, 21, 777–786. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 1415) | Non-AKI (n = 1338) | AKI (n = 77) | p-Value |
|---|---|---|---|---|
| Body mass index, kg/m2 | 24.8 ± 2.7 | 24.8 ± 2.7 | 25.1 ± 2.7 | 0.353 |
| Age, years | 67 ± 6 | 67 ± 6 | 70 ± 6 | <0.001 |
| ASA physical status | <0.001 | |||
| ≤2 | 379 (86.1%) | 351 (88.2%) | 28 (66.7%) | |
| 3 | 61 (13.9%) | 47 (11.8%) | 14 (33.3%) | |
| History of abdominal surgery | 268 (18.9%) | 252 (18.8%) | 16 (20.8%) | 0.672 |
| Comorbidities | ||||
| Diabetes mellitus | 252 (17.8%) | 234 (17.5%) | 18 (23.4%) | 0.189 |
| Hypertension | 679 (48.0%) | 635 (47.5%) | 44 (57.1%) | 0.098 |
| Coronary artery disease | 93 (6.6%) | 91 (6.8%) | 2 (2.6%) | 0.148 |
| Chronic kidney disease | 13 (0.9%) | 6 (0.4%) | 7 (9.1%) | <0.001 |
| Cerebrovascular accident | 45 (3.2%) | 42 (3.1%) | 3 (3.9%) | 0.732 |
| COPD | 223 (15.8%) | 211 (15.8%) | 12 (15.6%) | 0.965 |
| Medications | ||||
| Aspirin | 145 (11.0%) | 140 (11.1%) | 5 (7.6%) | 0.367 |
| Clopidogrel | 38 (3.0%) | 36 (3.0%) | 2 (3.4%) | 0.695 |
| Calcium channel blocker | 310 (23.1%) | 295 (23.2%) | 15 (22.1%) | 0.832 |
| ACEi or ARB | 325 (22.9%) | 301 (22.5%) | 24 (30.0%) | 0.121 |
| Beta blocker | 89 (6.6%) | 83 (6.5%) | 6 (8.8%) | 0.447 |
| Gleason score, points | 6.9 ± 1.0 | 6.9 ± 1.0 | 7.0 ± 1.1 | 0.788 |
| Tumor stage | 0.108 | |||
| 1 | 862 (60.8%) | 819 (61.2%) | 43 (53.8%) | |
| 2 | 37 (2.6%) | 35 (2.6%) | 2 (2.5%) | |
| 3 | 469 (33.1%) | 439 (32.7%) | 32 (40.0%) | |
| 4 | 50 (3.5%) | 47 (3.5%) | 3 (3.8%) | |
| Preoperative laboratory values | ||||
| PSA, ng/mL | 13.5 ± 27.4 | 13.6 ± 28.0 | 11.0 ± 10.9 | 0.076 |
| Hemoglobin, g/dL | 14.2 ± 2.9 | 14.1 ± 1.3 | 14.7 ± 11.1 | 0.580 |
| Platelet, 103/μL | 223.0 ± 53.4 | 223.6 ± 52.5 | 213.7 ± 65.7 | 0.200 |
| White blood cell, /mm3 | 6.3 ± 1.7 | 6.3 ± 1.7 | 6.8 ± 1.7 | 0.009 |
| Neutrophil, % | 56.5 ± 9.3 | 56.4 ± 9.3 | 57.8 ± 8.3 | 0.258 |
| Lymphocyte, % | 32.7 ± 8.5 | 32.9 ± 8.5 | 30.6 ± 7.7 | 0.021 |
| Platelet/lymphocyte ratio | 121.4 ± 59.6 | 121.8 ± 60.2 | 115.2 ± 47.9 | 0.331 |
| Neutrophil/lymphocyte ratio | 2.0 ± 1.2 | 2.0 ± 1.2 | 2.1 ± 1.0 | 0.346 |
| eGFR, mL/min/1.73 m2 | 80 ± 13 | 81 ± 11 | 69 ± 23 | <0.001 |
| Uric acid, mmol/L | 5.5 ± 1.3 | 5.5 ± 1.3 | 6.1 ± 1.7 | 0.005 |
| Albumin, g/dL | 4.0 ± 0.5 | 4.0 ± 0.5 | 3.8 ± 0.3 | <0.001 |
| AST, U/L | 24 ± 11 | 23 ± 8 | 30 ± 37 | 0.131 |
| ALT, U/L | 23 ± 11 | 23 ± 11 | 21 ± 10 | 0.072 |
| C-reactive protein, mg/L | 0.23 ± 0.57 | 0.24 ± 0.59 | 0.22 ± 0.27 | 0.838 |
| De Ritis ratio | 1.1 ± 0.5 | 1.1 ± 0.4 | 1.5 ± 1.4 | 0.008 |
| Variables | All Patients (n = 1415) | Non-AKI (n = 1338) | AKI (n = 77) | p-Value |
|---|---|---|---|---|
| Intraoperative variables | ||||
| Operation duration, minutes | 159 ± 39 | 158 ± 38 | 163 ± 45 | 0.317 |
| Crystalloid amount, mL | 1644 ± 700 | 1650 ± 703 | 1535 ± 642 | 0.159 |
| 6% hydroxyethyl starch amount, mL | 259 ± 330 | 258 ± 331 | 276 ± 320 | 0.637 |
| 5% albumin administration | 56 (4.0%) | 53 (4.0%) | 3 (3.9%) | >0.999 |
| Red blood cell transfusion | 156 (11.0%) | 143 (10.7%) | 13 (16.9%) | 0.091 |
| Extracapsular extension | 645 (45.6%) | 604 (45.1%) | 41 (53.2%) | 0.165 |
| Seminal vesical invasion | 192 (13.6%) | 180 (13.5%) | 12 (15.6%) | 0.597 |
| Positive surgical margins | 523 (37.0%) | 494 (36.9%) | 29 (37.7%) | 0.896 |
| Pelvic lymph node dissection | 1259 (89.0%) | 1187 (88.7%) | 72 (93.5%) | 0.192 |
| Laboratory data at postoperative 1 day | ||||
| Hemoglobin, g/dL | 11.2 ± 1.8 | 11.2 ± 1.9 | 10.7 ± 1.3 | 0.020 |
| Platelet, 103/μL | 184.7 ± 58.4 | 184.8 ± 56.5 | 183.9 ± 85.6 | 0.900 |
| Platelet/lymphocyte ratio | 210.4 ± 920.4 | 212.9 ± 940.5 | 156.5 ± 160.6 | 0.648 |
| Neutrophil/lymphocyte ratio | 6.8 ± 7.4 | 6.8 ± 7.5 | 7.2 ± 3.4 | 0.502 |
| Albumin, g/dL | 2.9 ± 0.3 | 2.9 ± 0.3 | 2.8 ± 0.4 | 0.115 |
| AST, U/L | 29 ± 77 | 27 ± 18 | 61 ± 317 | 0.330 |
| ALT, U/L | 28 ± 30 | 28 ± 25 | 27 ± 75 | 0.910 |
| De Ritis ratio | 1.1 ± 0.4 | 1.1 ± 0.3 | 1.5 ± 0.7 | <0.001 |
| Variables | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Body mass index | 1.038 (0.956–1.127) | 0.370 | ||
| Age | 1.092 (1.045–1.142) | <0.001 | ||
| ASA physical status | ||||
| ≤2 | 1.000 | |||
| 3 | 1.909 (0.845–4.313) | 0.120 | ||
| History of abdominal surgery | 1.077 (0.613–1.895) | 0.796 | ||
| Diabetes mellitus | 1.470 (0.862–2.506) | 0.158 | ||
| Hypertension | 1.498 (0.949–2.363) | 0.083 | ||
| Coronary artery disease | 0.351 (0.085–1.453) | 0.149 | ||
| Aspirin | 0.654 (0.258–1.655) | 0.370 | ||
| Clopidogrel | 1.145 (0.270–4.888) | 0.852 | ||
| ACEi or ARB | 1.390 (0.842–2.294) | 0.197 | ||
| Calcium channel blocker | 0.982 (0.554–1.742) | 0.951 | ||
| Beta blocker | 1.354 (0.570–3.219) | 0.492 | ||
| Tumor stage | ||||
| 1 | 1.000 | |||
| 2 | 1.088 (0.253–4.675)) | 0.909 | ||
| 3 | 1.395 (0.870–2.236) | 0.167 | ||
| 4 | 1.216 (0.364–4.064) | 0.751 | ||
| Gleason score | 1.030 (0.829–1.280) | 0.788 | ||
| Preoperative laboratory test | ||||
| PSA | 0.992 (0.977–1.008) | 0.330 | ||
| Hemoglobin | 1.027 (0.987–1.068) | 0.191 | ||
| Platelet | 0.996 (0.992–1.001) | 0.107 | ||
| White blood cell | 1.154 (1.030–1.293) | 0.014 | ||
| Platelet/lymphocyte ratio | 0.997 (0.992–1.002) | 0.287 | ||
| Neutrophil/lymphocyte ratio | 1.070 (0.936–1.223) | 0.323 | ||
| eGFR | 0.948 (0.935–0.962) | <0.001 | 0.961 (0.946–0.977) | < 0.001 |
| Uric acid | 1.367 (1.153–1.620) | <0.001 | ||
| Albumin | 0.087 (0.042–0.178) | <0.001 | 0.249 (0.109–0.572) | 0.001 |
| C-reactive protein | 0.955 (0.598–1.526) | 0.848 | ||
| Operation duration | 1.002 (0.997–1.008) | 0.429 | ||
| Crystalloid amount | 1.000 (0.999–1.000) | 0.110 | ||
| 6% hydroxyethyl starch | 1.000 (0.999–1.001) | 0.844 | ||
| Red blood cell transfusion | 1.928 (1.072–3.471) | 0.028 | ||
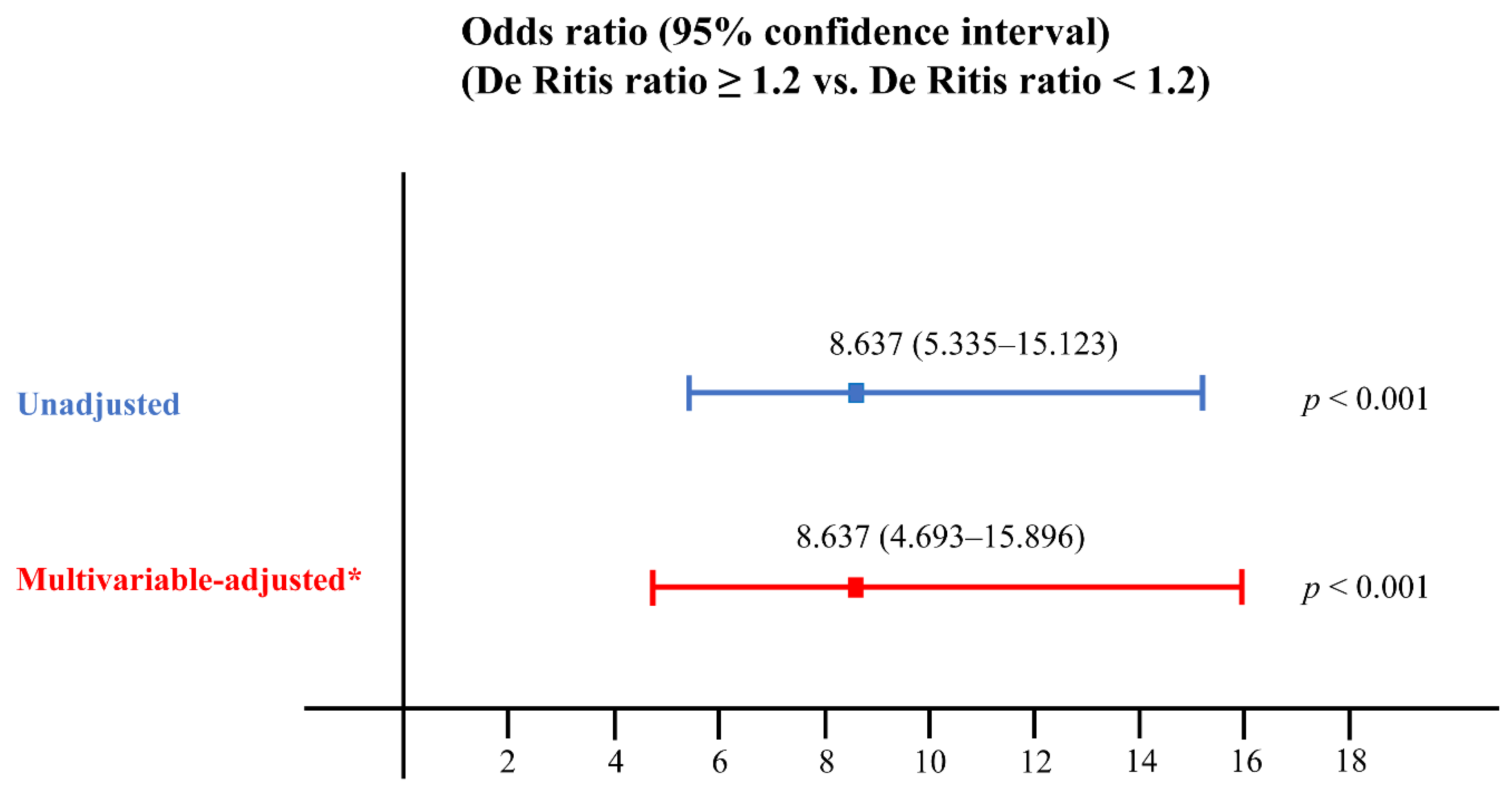
| De Ritis ratio at postoperative 1 day | 9.405 (5.504–16.071) | < 0.001 | 7.353 (3.967–13.630) | <0.001 |
| Outcomes | All Patients (n = 1415) | Non-AKI (n = 1338) | AKI (n = 77) | p-Value |
|---|---|---|---|---|
| Hospitalization duration, days | 10 ± 4 | 10 ± 4 | 11 ± 5 | 0.002 |
| Intensive care unit admission | 20 (1.4%) | 17 (1.3%) | 3 (3.8%) | 0.099 |
| Death within 30 days after surgery | 2 (0.1%) | 1 (0.1%) | 1 (1.3%) | 0.110 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-Y.; Yu, J.; Hong, J.H.; Lim, B.; Kim, Y.; Hwang, J.-H.; Kim, Y.-K. Elevated De Ritis Ratio as a Predictor for Acute Kidney Injury after Radical Retropubic Prostatectomy. J. Pers. Med. 2021, 11, 836. https://doi.org/10.3390/jpm11090836
Park J-Y, Yu J, Hong JH, Lim B, Kim Y, Hwang J-H, Kim Y-K. Elevated De Ritis Ratio as a Predictor for Acute Kidney Injury after Radical Retropubic Prostatectomy. Journal of Personalized Medicine. 2021; 11(9):836. https://doi.org/10.3390/jpm11090836
Chicago/Turabian StylePark, Jun-Young, Jihion Yu, Jun Hyuk Hong, Bumjin Lim, Youngdo Kim, Jai-Hyun Hwang, and Young-Kug Kim. 2021. "Elevated De Ritis Ratio as a Predictor for Acute Kidney Injury after Radical Retropubic Prostatectomy" Journal of Personalized Medicine 11, no. 9: 836. https://doi.org/10.3390/jpm11090836
APA StylePark, J.-Y., Yu, J., Hong, J. H., Lim, B., Kim, Y., Hwang, J.-H., & Kim, Y.-K. (2021). Elevated De Ritis Ratio as a Predictor for Acute Kidney Injury after Radical Retropubic Prostatectomy. Journal of Personalized Medicine, 11(9), 836. https://doi.org/10.3390/jpm11090836