
Psychological Characteristics Associated with Post-Treatment Physical Status and Quality of Life in Patients with Brain Tumor Undergoing Radiotherapy

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
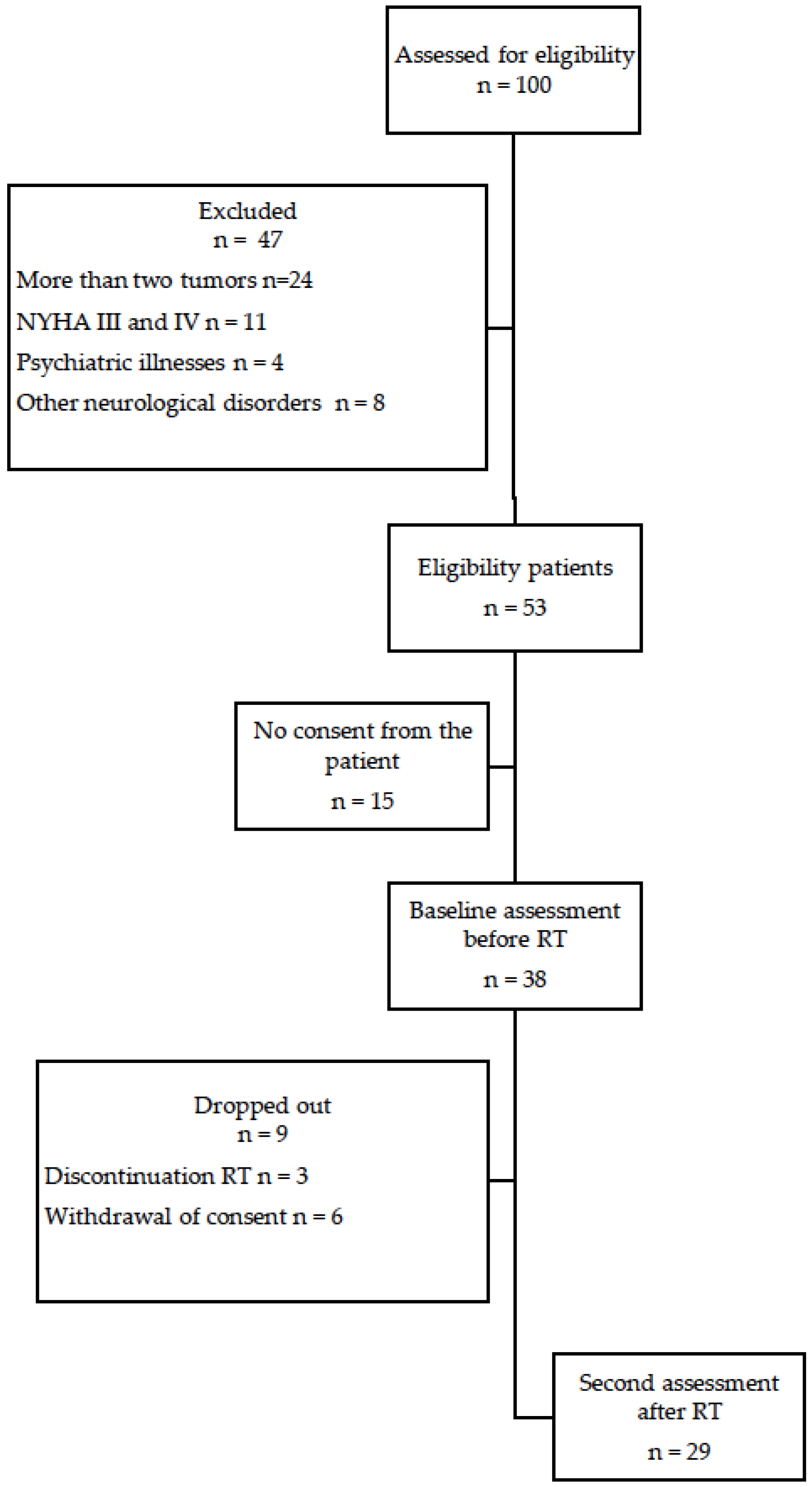
2.2. Participants
2.3. Radiotherapy Procedure
2.4. Study Data Collection
2.5. Measurements
2.5.1. Hand Grip Strength (HGS)
2.5.2. Timed Up and Go Test (TUG)
2.5.3. 6 Min Walk Test (6MWT)
2.5.4. The Functional Independence Measure (FIM)
2.5.5. Quality of Life
2.5.6. Assessment of Fatigue
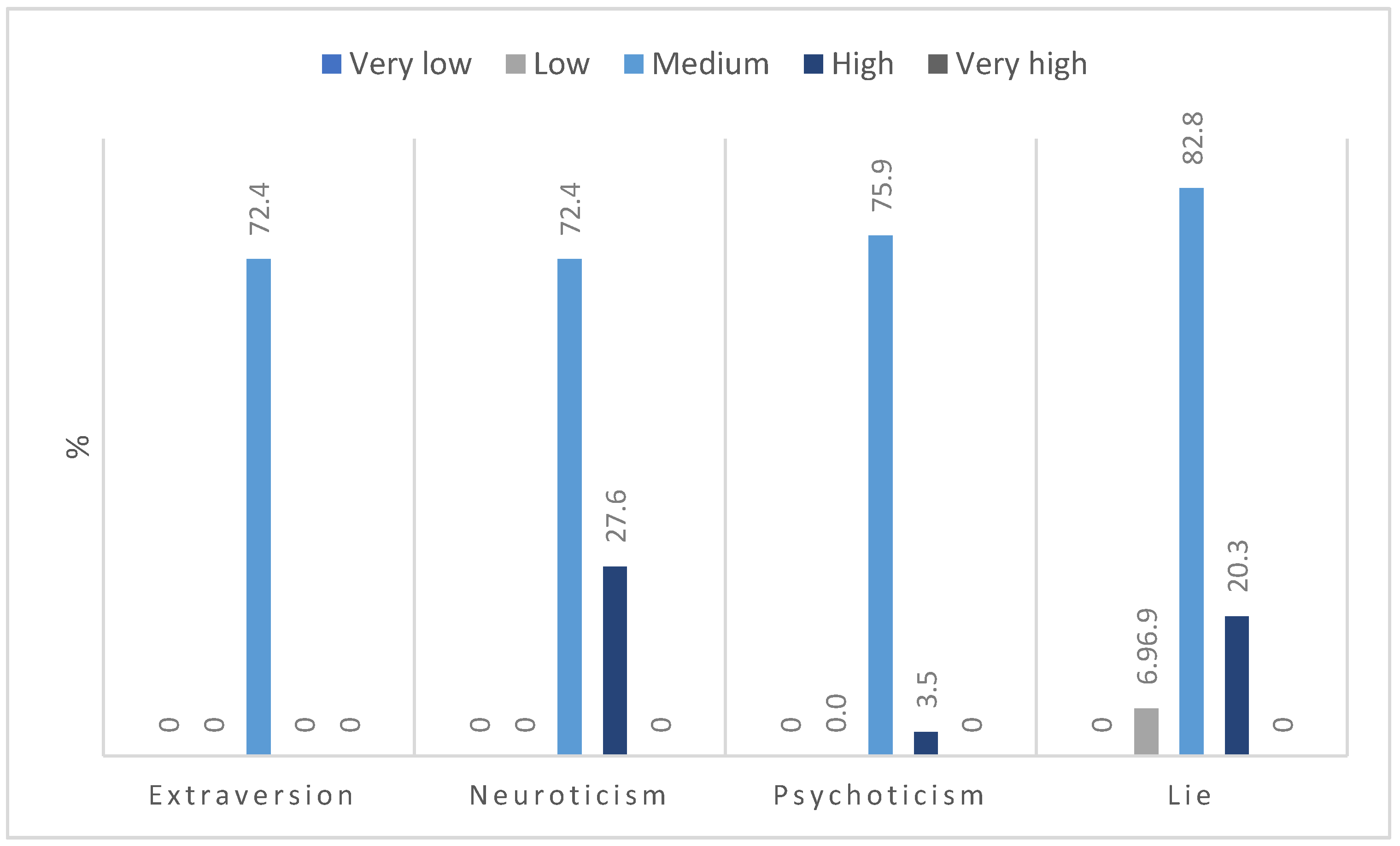
2.5.7. Personality Test
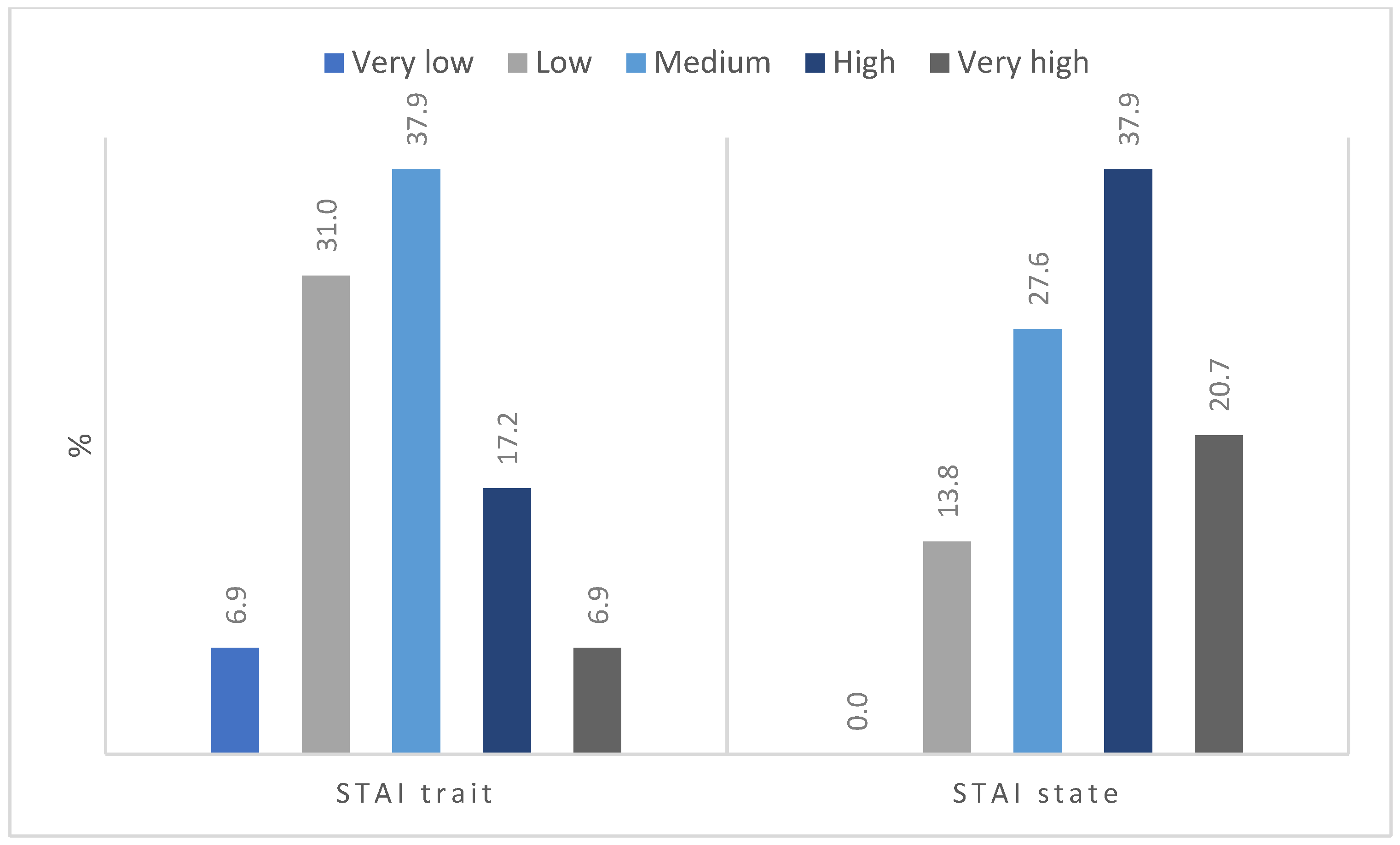
2.5.8. Anxiety Level Assessment
2.6. Statistical Analysis
3. Results
4. Discussion
5. Strength and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Perkins, A.; Liu, G. Primary Brain Tumors in Adults: Diagnosis and Treatment. Am. Fam. Physician 2016, 93, 211–217. [Google Scholar]
- Batash, R.; Asna, N.; Schaffer, P.; Francis, N.; Schaffer, M. Glioblastoma Multiforme, Diagnosis and Treatment; Recent Literature Review. Curr. Med. Chem. 2017, 24, 3002–3009. [Google Scholar] [CrossRef]
- Barisano, G.; Bergamaschi, S.; Acharya, J.; Rajamohan, A.; Gibbs, W.; Kim, P.; Zada, G.; Chang, E.; Law, M. Complications of Radiotherapy and Radiosurgery in the Brain and Spine. Neurographics (2011) 2018, 8, 167–187. [Google Scholar] [CrossRef]
- de Courcy, L.; Bezak, E.; Marcu, L.G. Gender-dependent radiotherapy: The next step in personalised medicine? Crit. Rev. Oncol. Hematol. 2020, 147, 102881. [Google Scholar] [CrossRef]
- Malicki, J.; Piotrowski, T.; Guedea, F.; Krengli, M. Treatment-integrated imaging, radiomics, and personalised radiotherapy: The future is at hand. Rep. Pr. Oncol. Radiother. 2022, 27, 734–743. [Google Scholar] [CrossRef]
- Ree, A.H.; Redalen, K.R. Personalized radiotherapy: Concepts, biomarkers and trial design. Br. J. Radiol. 2015, 88, 20150009. [Google Scholar] [CrossRef]
- Lipkova, J.; Angelikopoulos, P.; Wu, S.; Alberts, E.; Wiestler, B.; Diehl, C.; Preibisch, C.; Pyka, T.; Combs, S.E.; Hadjidoukas, P.; et al. Personalized Radiotherapy Design for Glioblastoma: Integrating Mathematical Tumor Models, Multimodal Scans, and Bayesian Inference. IEEE Trans. Med. Imaging 2019, 38, 1875–1884. [Google Scholar] [CrossRef]
- Asher, A.; Fu, J.B.; Bailey, C.; Hughes, J.K. Fatigue among patients with brain tumors. CNS Oncol. 2016, 5, 91–100. [Google Scholar] [CrossRef]
- Marker, R.J.; Ostendorf, D.M.; Leach, H.J.; Peters, J.C. Cancer-related fatigue mediates the relationships between physical fitness and attendance and quality of life after participation in a clinical exercise program for survivors of cancer. Qual. Life Res. 2022, 31, 3201–3210. [Google Scholar] [CrossRef]
- Mravec, B.; Tibensky, M.; Horvathova, L. Stress and cancer. Part II: Therapeutic implications for oncology. J. Neuroimmunol. 2020, 346, 577312. [Google Scholar] [CrossRef]
- Macina, C.; Bendel, R.; Walter, M.; Wrege, J.S. Somatization and Somatic Symptom Disorder and its overlap with dimensionally measured personality pathology: A systematic review. J. Psychosom. Res. 2021, 151, 110646. [Google Scholar] [CrossRef]
- Eysenck, H.J.; Eysenck, S.B.G. Manual of the Eysenck Personality Scales (Eps Adult): Comprising the Epq-Revised (Epq-R) (Including Addiction and Criminality Scales) Epq-R Short Scale Impulsiveness (Ive) Questionnaire; Hodder & Stoughton: London, UK, 1998. [Google Scholar]
- Hoerger, M.; Coletta, M.; Sörensen, S.; Chapman, B.P.; Kaukeinen, K.; Tu, X.; Duberstein, P.R. Personality and Perceived Health in Spousal Caregivers of Patients with Lung Cancer: The Roles of Neuroticism and Extraversion. J. Aging Res. 2016, 2016, 5659793. [Google Scholar] [CrossRef]
- Sutin, A.R.; Zonderman, A.B.; Ferrucci, L.; Terracciano, A. Personality traits and chronic disease: Implications for adult personality development. J. Gerontol. B Psychol. Sci. Soc. Sci. 2013, 68, 912–920. [Google Scholar] [CrossRef]
- Chapman, B.P.; Hampson, S.; Clarkin, J. Personality-informed interventions for healthy aging: Conclusions from a National Institute on Aging work group. Dev. Psychol. 2014, 50, 1426–1441. [Google Scholar] [CrossRef]
- Dahl, A.A.; Fosså, S.D. High Neuroticism Is Related to More Overall Functional Problems and Lower Function Scores in Men Who Had Surgery for Non-Relapsing Prostate Cancer. Curr. Oncol. 2022, 29, 459. [Google Scholar] [CrossRef]
- Ramírez-de Los Santos, M.L.; López-Navarro, A.; Ramírez-de Los Santos, S.; Guzmán-Flores, J.M.; Pereira-Suárez, A.L.; López-Pulido, E.I. Relation between personality dimensions and symptomatology of depression in skin cancer patients. Biopsychosoc. Med. 2021, 15, 18. [Google Scholar] [CrossRef]
- Bunevicius, A. Personality traits, patient-centered health status and prognosis of brain tumor patients. J. Neurooncol. 2018, 137, 593–600. [Google Scholar] [CrossRef]
- Krok, J.L.; Baker, T.A. The influence of personality on reported pain and self-efficacy for pain management in older cancer patients. J. Health Psychol. 2014, 19, 1261–1270. [Google Scholar] [CrossRef]
- Brown, R.L.; Chen, M.A.; Paoletti, J.; Dicker, E.E.; Wu-Chung, E.L.; LeRoy, A.S.; Majd, M.; Suchting, R.; Thayer, J.F.; Fagundes, C.P. Emotion Regulation, Parasympathetic Function, and Psychological Well-Being. Front. Psychol. 2022, 13, 879166. [Google Scholar] [CrossRef]
- Aprile, I.; Chiesa, S.; Padua, L.; Di Blasi, C.; Arezzo, M.F.; Valentini, V.; Di Stasio, E.; Balducci, M. Occurrence and predictors of the fatigue in high-grade glioma patients. Neurol. Sci. 2015, 36, 1363–1369. [Google Scholar] [CrossRef]
- Gonzalez-Saenz de Tejada, M.; Bilbao, A.; Baré, M.; Briones, E.; Sarasqueta, C.; Quintana, J.M.; Escobar, A. Association between social support, functional status, and change in health-related quality of life and changes in anxiety and depression in colorectal cancer patients. Psychooncology 2017, 26, 1263–1269. [Google Scholar] [CrossRef]
- Shi, C.; Lamba, N.; Zheng, L.J.; Cote, D.; Regestein, Q.R.; Liu, C.M.; Tran, Q.; Routh, S.; Smith, T.R.; Mekary, R.A.; et al. Depression and survival of glioma patients: A systematic review and meta-analysis. Clin. Neurol. Neurosurg. 2018, 172, 8–19. [Google Scholar] [CrossRef]
- Dinapoli, L.; Chiesa, S.; Dinapoli, N.; Gatta, R.; Beghella Bartoli, F.; Bracci, S.; Mazzarella, C.; Sanfilippo, M.Z.; Sabatino, G.; Gaudino, S.; et al. Personalised support of brain tumour patients during radiotherapy based on psychological profile and quality of life. Support. Care Cancer 2021, 29, 4555–4563. [Google Scholar] [CrossRef]
- Mehnert, A.; Lehmann, C.; Graefen, M.; Huland, H.; Koch, U. Depression, anxiety, post-traumatic stress disorder and health-related quality of life and its association with social support in ambulatory prostate cancer patients. Eur. J. Cancer Care 2010, 19, 736–745. [Google Scholar] [CrossRef]
- Dahl, A.A. Link between personality and cancer. Future Oncol. 2010, 6, 691–707. [Google Scholar] [CrossRef]
- Macía, P.; Gorbeña, S.; Gómez, A.; Barranco, M.; Iraurgi, I. Role of neuroticism and extraversion in the emotional health of people with cancer. Heliyon 2020, 6, e04281. [Google Scholar] [CrossRef]
- Wang, S.-H.; He, G.-P.; Jiang, P.-L.; Tang, L.-L.; Feng, X.-M.; Zeng, C.; Wang, G.-F. Relationship between cancer-related fatigue and personality in patients with breast cancer after chemotherapy. Psychooncology 2013, 22, 2386–2390. [Google Scholar] [CrossRef]
- Caudell, J.J.; Torres-Roca, J.F.; Gillies, R.J.; Enderling, H.; Kim, S.; Rishi, A.; Moros, E.G.; Harrison, L.B. The future of personalised radiotherapy for head and neck cancer. Lancet Oncol. 2017, 18, e266–e273. [Google Scholar] [CrossRef]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef]
- Sartor, L.C.A.; Luvizutto, G.J.; de Souza, J.T.; Silva Dalle Molle, E.R.; Modolo, G.P.; da Silva, T.R.; Prudente, R.A.; Ribeiro, P.W.; da Costa, R.D.M.; de Oliveira Antunes, L.C.; et al. Respiratory Function and Grip Strength in the Acute Phase of Stroke Are Associated with Stroke Severity and Disability at Hospital Discharge. Rehabil. Res. Pract. 2020, 2020, 1636540. [Google Scholar] [CrossRef]
- Esteban-Simón, A.; Díez-Fernández, D.M.; Artés-Rodríguez, E.; Casimiro-Artés, M.Á.; Rodríguez-Pérez, M.A.; Moreno-Martos, H.; Casimiro-Andújar, A.J.; Soriano-Maldonado, A. Absolute and Relative Handgrip Strength as Indicators of Self-Reported Physical Function and Quality of Life in Breast Cancer Survivors: The EFICAN Study. Cancers 2021, 13, 5292. [Google Scholar] [CrossRef]
- Cordier, D.; Gerber, M.; Brand, S. Effects of two types of exercise training on psychological well-being, sleep, quality of life and physical fitness in patients with high-grade glioma (WHO III and IV): Study protocol for a randomized controlled trial. Cancer Commun. 2019, 39, 46. [Google Scholar] [CrossRef]
- MacDermid, J.; Solomon, G.; Valdes, K. (Eds.) Clinical Assessment Recommendations, 3rd ed.; American Society of Hand Therapists: Mount Laurel, NJ, USA, 2015; ISBN 9780692525159. [Google Scholar]
- Kear, B.M.; Guck, T.P.; McGaha, A.L. Timed Up and Go (TUG) Test: Normative Reference Values for Ages 20 to 59 Years and Relationships with Physical and Mental Health Risk Factors. J. Prim. Care Community Health 2017, 8, 9–13. [Google Scholar] [CrossRef]
- Michael, C.M.; Lehrer, E.J.; Schmitz, K.H.; Zaorsky, N.G. Prehabilitation exercise therapy for cancer: A systematic review and meta-analysis. Cancer Med. 2021, 10, 4195–4205. [Google Scholar] [CrossRef]
- Agarwala, P.; Salzman, S.H. Six-Minute Walk Test: Clinical Role, Technique, Coding, and Reimbursement. Chest 2020, 157, 603–611. [Google Scholar] [CrossRef]
- Maritz, R.; Tennant, A.; Fellinghauer, C.; Stucki, G.; Prodinger, B. The Functional Independence Measure 18-item version can be reported as a unidimensional interval-scaled metric: Internal construct validity revisited. J. Rehabil. Med. 2019, 51, 193–200. [Google Scholar] [CrossRef]
- Noll, K.R.; Bradshaw, M.E.; Weinberg, J.S.; Wefel, J.S. Neurocognitive functioning is associated with functional independence in newly diagnosed patients with temporal lobe glioma. Neurooncol. Pract. 2018, 5, 184–193. [Google Scholar] [CrossRef]
- Gunn, S.; Burgess, G.H.; Maltby, J. A Factor Analysis of Functional Independence and Functional Assessment Measure Scores Among Focal and Diffuse Brain Injury Patients: The Importance of Bifactor Models. Arch. Phys. Med. Rehabil. 2018, 99, 1805–1810. [Google Scholar] [CrossRef]
- Hojan, K.; Gerreth, K. Can Multidisciplinary Inpatient and Outpatient Rehabilitation Provide Sufficient Prevention of Disability in Patients with a Brain Tumor?-A Case-Series Report of Two Programs and A Prospective, Observational Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 6488. [Google Scholar] [CrossRef]
- Kim, S.-H.; Byun, Y. Trajectories of Symptom Clusters, Performance Status, and Quality of Life During Concurrent Chemoradiotherapy in Patients with High-Grade Brain Cancers. Cancer Nurs. 2018, 41, E38–E47. [Google Scholar] [CrossRef]
- Agarwal, S.; Garg, R.; Minhas, V.; Bhatnagar, S.; Mishra, S.; Kumar, V.; Bharati, S.J.; Gupta, N.; Khan, M.A. To assess the Prevalence and Predictors of Cancer-related Fatigue and its Impact on Quality of Life in Advanced Cancer Patients Receiving Palliative Care in a Tertiary Care Hospital: A Cross-sectional Descriptive Study. Indian J. Palliat. Care 2020, 26, 523–527. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Manual for the State-Trait Anxiety Inventory (Self Evaluation Questionnaire); Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Hu, T.; Xiao, J.; Peng, J.; Kuang, X.; He, B. Relationship between resilience, social support as well as anxiety/depression of lung cancer patients: A cross-sectional observation study. J. Cancer Res. Ther. 2018, 14, 72–77. [Google Scholar] [CrossRef]
- García-Torres, F.; Alós, F.J. Eysenck personality questionnaire revised psychoticism predicts motivational-somatic symptoms of depression in breast cancer survivors. Psychooncology 2014, 23, 350–352. [Google Scholar] [CrossRef]
- Bitterlich, C.; Vordermark, D. Analysis of health-related quality of life in patients with brain tumors prior and subsequent to radiotherapy. Oncol. Lett. 2017, 14, 1841–1846. [Google Scholar] [CrossRef]
- Wujanto, C.; Vellayappan, B.; Chang, E.L.; Chao, S.T.; Sahgal, A.; Lo, S.S. Radiotherapy to the brain: What are the consequences of this age-old treatment? Ann. Palliat. Med. 2021, 10, 936–952. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Participants (n = 29) n (%) or Mean ± SD |
|---|---|
| Age, years | 52.8 ± 14.1 |
| Sex | |
| Female | 10 (34.5) |
| Male | 19 (65.5) |
| Type of tumor | |
| GBM | 26 (89.7) |
| Oligodendroglioma | 2 (6.9) |
| Ependymoma | 1 (3.5) |
| Total resection | |
| Yes | 12 (41.4) |
| No | 17 (58.6) |
| Chemotherapy | |
| Yes | 23 (79.3) |
| No | 6 (20.7) |
| Parameters Median (Range) | Before RT | After RT | p-Value |
|---|---|---|---|
| HGS (kg) | 28 (11.3–53) | 30 (13–4.5) | 0.659 |
| TUG (s) | 8.38 (5.28–12.95) | 8 (5.12–13.76) | 0.331 |
| 6MWT (m) | 405 (267–670) | 431 (243–703) | 0.666 |
| FIM (points) | 126 (7–126) | 126 (5–126) | 0.683 |
| FACT-G PWB (points) | 22 (10–28) | 21 (10–28) | 0.201 |
| FACT-G SWB (points) | 24 (9–28) | 24 (2–28) | 0.332 |
| FACT-G EWB (points) | 15 (0–24) | 15 (0–24) | 0.550 |
| FACT-G FWB (points) | 19 (2–28) | 19 (4–28) | 0.984 |
| FACT-G total (points) | 79.3 (43–105) | 77.5 (43–98) | 0.648 |
| FACIT-F (points) | 38 (11–52) | 33 (14–50) | 0.040 |
| Test | Extraversion | Neuroticism | Psychoticism | Lie | ||||
|---|---|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | r | p-Value | |
| HGS | 0.049 | 0.81 | 0.253 | 0.19 | 0.307 | 0.11 | −0.359 | 0.06 |
| TUG | −0.192 | 0.33 | 0.145 | 0.46 | −0.300 | 0.12 | −0.010 | 0.96 |
| 6MWT | 0.076 | 0.71 | −0.167 | 0.42 | 0.402 | 0.04 | −0.097 | 0.64 |
| FIM | 0.079 | 0.69 | −0.246 | 0.21 | 0.023 | 0.91 | −0.066 | 0.74 |
| FACT-G PWB | 0.087 | 0.66 | −0.399 | 0.04 | −0.117 | 0.55 | 0.373 | 0.05 |
| FACT-G SWB | 0.420 | 0.03 | −0.309 | 0.11 | −0.239 | 0.02 | −0.088 | 0.66 |
| FACT-G EWB | 0.378 | 0.05 | −0.186 | 0.34 | −0.023 | 0.91 | −0.033 | 0.87 |
| FACT-G FWB | 0.455 | 0.02 | −0.265 | 0.17 | −0.134 | 0.49 | −0.124 | 0.53 |
| FACT-G total | 0.428 | 0.02 | −0.335 | 0.08 | −0.136 | 0.49 | −0.010 | 0.96 |
| FACIT-F | 0.056 | 0.78 | −0.159 | 0.42 | −0.008 | 0.97 | 0.336 | 0.08 |
| Measurements before RT | STAI Trait | STAI State | ||
|---|---|---|---|---|
| r | p-Value | r | p-Value | |
| HGS | 0.113 | 0.57 | −0.084 | 0.67 |
| TUG | 0.236 | 0.23 | 0.36 | 0.06 |
| 6MWT | −0.233 | 0.25 | −0.343 | 0.09 |
| FIM | −0.407 | 0.03 | −0.479 | 0.01 |
| FACT-G PWB | −0.329 | 0.09 | −0.371 | 0.05 |
| FACT-G SWB | −0.379 | 0.05 | −0.351 | 0.07 |
| FACT-G EWB | −0.143 | 0.47 | −0.171 | 0.38 |
| FACT-G FWB | −0.189 | 0.33 | −0.360 | 0.06 |
| FACT-G total | −0.291 | 0.13 | −0.386 | 0.04 |
| FACIT-F | −0.267 | 0.17 | −0.280 | 0.15 |
| Measurements after RT | Extraversion | Neuroticism | Psychoticism | Lie | ||||
|---|---|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | r | p-Value | |
| HGS | 0.050 | 0.81 | 0.217 | 0.29 | 0.231 | 0.27 | −0.212 | 0.31 |
| TUG | 0.045 | 0.83 | 0.135 | 0.51 | −0.148 | 0.47 | −0.153 | 0.46 |
| 6MWT | 0.085 | 0.69 | −0.226 | 0.28 | 0.561 | 0.00 | −0.029 | 0.89 |
| FIM | −0.040 | 0.85 | −0.203 | 0.33 | 0.040 | 0.85 | −0.181 | 0.39 |
| FACT-G PWB | −0.017 | 0.93 | −0.441 | 0.02 | 0.269 | 0.18 | 0.216 | 0.29 |
| FACT-G SWB | 0.194 | 0.34 | −0.037 | 0.86 | −0.014 | 0.95 | 0.266 | 0.19 |
| FACT-G EWB | 0.267 | 0.19 | −0.198 | 0.33 | −0.078 | 0.70 | −0.128 | 0.53 |
| FACT-G FWB | 0.301 | 0.14 | −0.309 | 0.13 | 0.124 | 0.55 | −0.178 | 0.38 |
| FACT-G total | 0.304 | 0.13 | −0.362 | 0.07 | 0.147 | 0.47 | −0.026 | 0.90 |
| FACIT-F | 0.093 | 0.66 | −0.087 | 0.68 | 0.277 | 0.18 | 0.257 | 0.22 |
| Measurements after RT | STAI Trait | STAI State | ||
|---|---|---|---|---|
| r | p-Value | r | p-Value | |
| HGS | 0.038 | 0.86 | −0.190 | 0.36 |
| TUG | 0.282 | 0.16 | 0.449 | 0.02 |
| 6MWT | −0.299 | 0.16 | −0.346 | 0.09 |
| FIM | −0.397 | 0.05 | −0.506 | 0.01 |
| FACT-G PWB | −0.359 | 0.07 | −0.379 | 0.06 |
| FACT-G SWB | −0.115 | 0.58 | −0.092 | 0.66 |
| FACT-G EWB | −0.065 | 0.75 | −0.110 | 0.59 |
| FACT-G FWB | −0.230 | 0.26 | −0.490 | 0.01 |
| FACT-G total | −0.301 | 0.14 | −0.444 | 0.02 |
| FACIT-F | −0.191 | 0.36 | −0.149 | 0.48 |
| Difference in Measurements before and after RT | Extraversion | Neuroticism | Psychoticism | Lie | ||||
|---|---|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | r | p-Value | |
| HGS | 0.178 | 0.38 | −0.227 | 0.27 | −0.282 | 0.16 | 0.288 | 0.15 |
| TUG | 0.275 | 0.17 | −0.056 | 0.79 | 0.001 | 0.99 | −0.238 | 0.24 |
| 6MWT | 0.059 | 0.78 | −0.132 | 0.53 | 0.446 | 0.03 | 0.126 | 0.55 |
| FIM | −0.031 | 0.89 | −0.047 | 0.82 | −0.159 | 0.44 | −0.102 | 0.62 |
| FACT-G PWB | −0.007 | 0.97 | −0.009 | 0.97 | 0.399 | 0.04 | −0.172 | 0.40 |
| FACT-G SWB | −0.021 | 0.92 | 0.197 | 0.34 | 0.466 | 0.02 | 0.165 | 0.43 |
| FACT-G EWB | −0.141 | 0.49 | −0.070 | 0.73 | −0.133 | 0.52 | −0.019 | 0.94 |
| FACT-G FWB | −0.196 | 0.34 | −0.071 | 0.73 | 0.341 | 0.09 | −0.031 | 0.88 |
| FACT-G total | −0.156 | 0.45 | −0.035 | 0.87 | 0.412 | 0.04 | −0.093 | 0.65 |
| FACIT-F | 0.172 | 0.41 | −0.062 | 0.79 | 0.311 | 0.13 | −0.280 | 0.18 |
| Difference in Measurements before and after RT | STAI Trait | STAI State | ||
|---|---|---|---|---|
| r | p-Value | r | p-Value | |
| HGS | −0.142 | 0.49 | −0.195 | 0.34 |
| TUG | 0.060 | 0.77 | 0.132 | 0.52 |
| 6MWT | −0.102 | 0.63 | −0.183 | 0.38 |
| FIM | 0.083 | 0.69 | −0.042 | 0.84 |
| FACT-G PWB | 0.048 | 0.82 | 0.090 | 0.66 |
| FACT-G SWB | 0.082 | 0.69 | 0.054 | 0.79 |
| FACT-G EWB | 0.044 | 0.83 | −0.041 | 0.84 |
| FACT-G FWB | −0.154 | 0.45 | −0.257 | 0.21 |
| FACT-G total | −0.002 | 0.99 | −0.117 | 0.57 |
| FACIT-F | 0.043 | 0.85 | 0.071 | 0.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pieczyńska, A.; Pilarska, A.; Adamska, K.; Zasadzka, E.; Hojan, K. Psychological Characteristics Associated with Post-Treatment Physical Status and Quality of Life in Patients with Brain Tumor Undergoing Radiotherapy. J. Pers. Med. 2022, 12, 1880. https://doi.org/10.3390/jpm12111880
Pieczyńska A, Pilarska A, Adamska K, Zasadzka E, Hojan K. Psychological Characteristics Associated with Post-Treatment Physical Status and Quality of Life in Patients with Brain Tumor Undergoing Radiotherapy. Journal of Personalized Medicine. 2022; 12(11):1880. https://doi.org/10.3390/jpm12111880
Chicago/Turabian StylePieczyńska, Anna, Agnieszka Pilarska, Krystyna Adamska, Ewa Zasadzka, and Katarzyna Hojan. 2022. "Psychological Characteristics Associated with Post-Treatment Physical Status and Quality of Life in Patients with Brain Tumor Undergoing Radiotherapy" Journal of Personalized Medicine 12, no. 11: 1880. https://doi.org/10.3390/jpm12111880
APA StylePieczyńska, A., Pilarska, A., Adamska, K., Zasadzka, E., & Hojan, K. (2022). Psychological Characteristics Associated with Post-Treatment Physical Status and Quality of Life in Patients with Brain Tumor Undergoing Radiotherapy. Journal of Personalized Medicine, 12(11), 1880. https://doi.org/10.3390/jpm12111880