
Patient and Physician Preferences for Regimen Attributes for the Treatment of HIV in the United States and Canada

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Satisfaction and Stigma Questions
2.4. Discrete Choice Experiment
2.5. Demographics and Treatment Characteristics
2.6. Pilot Testing
2.7. Data Analysis
3. Results
3.1. PLWH Characteristics
3.2. Physician Characteristics
3.3. Current Treatment Satisfaction, Adherence and Stigma
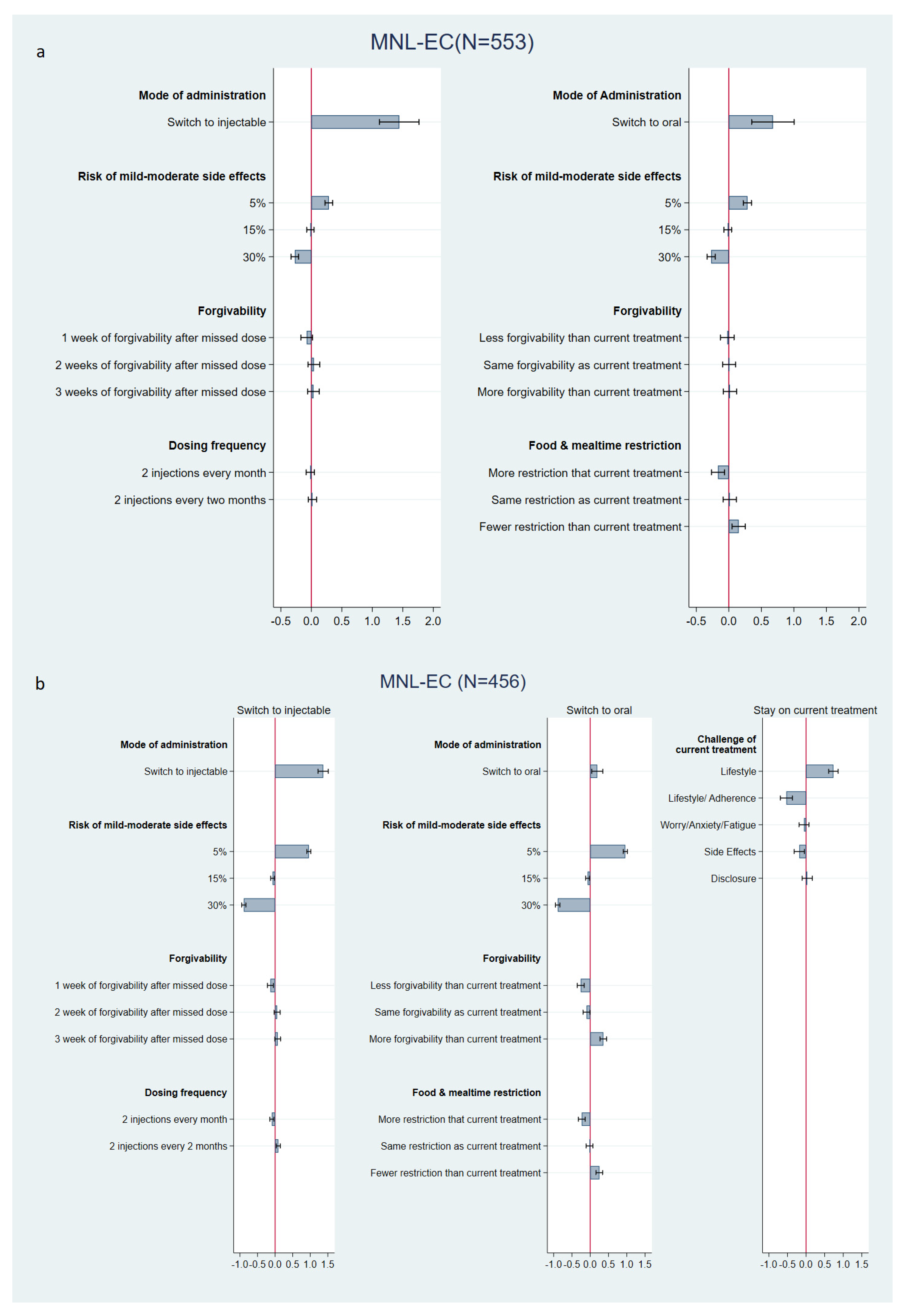
3.4. Preference Estimates
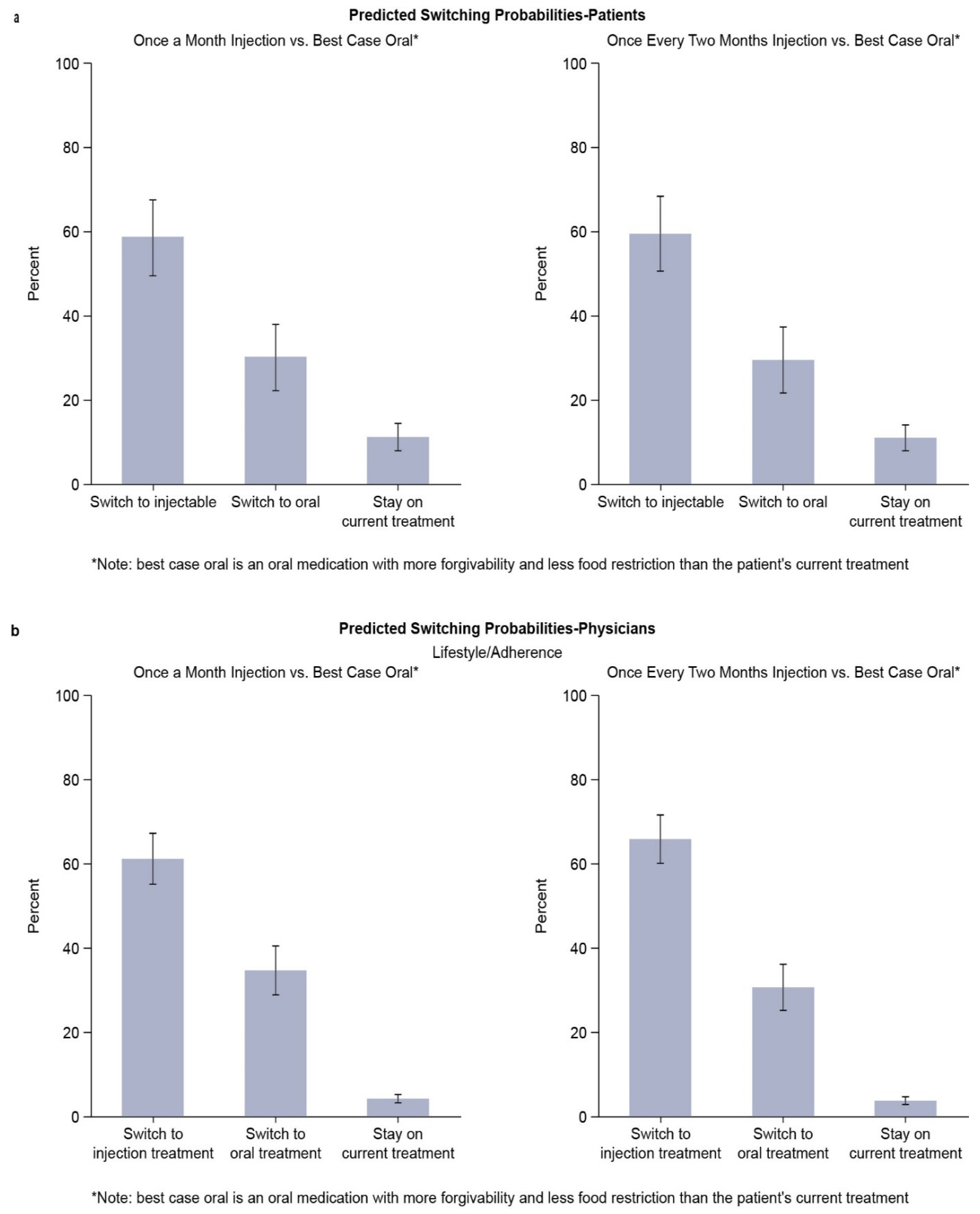
3.5. Predicted Switching Probabilities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wandeler, G.; Johnson, L.F.; Egger, M. Trends in life expectancy of HIV-positive adults on antiretroviral therapy across the globe: Comparisons with general population. Curr. Opin. HIV AIDS 2016, 11, 492–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, S.G.; Lewin, S.R.; Havlir, D.V. The end of AIDS: HIV infection as a chronic disease. Lancet 2013, 382, 1525–1533. [Google Scholar] [CrossRef] [Green Version]
- Sabin, C.A. Do people with HIV infection have a normal life expectancy in the era of combination antiretroviral therapy? BMC Med. 2013, 11, 251. [Google Scholar] [CrossRef] [Green Version]
- Teeraananchai, S.; Kerr, S.J.; Amin, J.; Ruxrungtham, K.; Law, M.G. Life expectancy of HIV-positive people after starting combination antiretroviral therapy: A meta-analysis. HIV Med. 2017, 18, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Wing, E.J. HIV and aging. Int. J. Infect Dis. 2016, 53, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DHHS. Panel on Antiretroviral Guidelines for Adults and Adolescents—A Working Group of the Office of AIDS Research Advisory Council (OARAC). Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV (2019). Available online: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/AdultandAdolescentGL.pdf (accessed on 8 November 2021).
- Beusterien, K.M.; Dziekan, K.; Flood, E.; Harding, G.; Jordan, J.C. Understanding patient preferences for HIV medications using adaptive conjoint analysis: Feasibility assessment. Value Health 2005, 8, 453–461. [Google Scholar] [CrossRef] [Green Version]
- Burch, L.S.; Smith, C.J.; Anderson, J.; Sherr, L.; Rodger, A.J.; O’Connell, R.; Geretti, A.; Gilson, R.; Fisher, M.; Elford, J.; et al. Socioeconomic status and treatment outcomes for individuals with HIV on antiretroviral treatment in the UK: Cross-sectional and longitudinal analyses. Lancet Public Health 2016, 1, e26–e36. [Google Scholar] [CrossRef] [Green Version]
- Eaton, E.F.; McDavid, C.; Banasiewicz, M.K.; Mugavero, M.J.; Knight, S.J. Patient preferences for antiretroviral therapy: Effectiveness, quality of life, access and novel delivery methods. Patient Prefer. Adherence 2017, 11, 1585–1590. [Google Scholar] [CrossRef] [Green Version]
- Fielden, S.J.; Rusch, M.L.A.; Yip, B.; Wood, E.; Shannon, K.; Levy, A.R.; Montaner, J.S.G.; Hogg, R.S. Nonadherence increases the risk of hospitalization among HIV-infected antiretroviral naive patients started on HAART. J. Int. Assoc. Physicians AIDS Care (Chic.) 2008, 7, 238–244. [Google Scholar] [CrossRef]
- Jean, B.N.; Vinvent, M.C.; Gert, U.v.Z.; Edward, M.G.; Wolfgang, P.; Steven, Y.H.; Edward, J.M.; Robert, G. HIV treatment adherence, drug resistance, virologic failure: Evolving concepts. Inf. Disord Drug Targets 2011, 11, 167–174. [Google Scholar]
- Rizzardini, G.; Overton, E.T.; Orkin, C.; Swindells, S.; Arasteh, K.; Górgolas Hernández-Mora, M.; Pokrovsky, V.; Girard, P.M.; Oka, S.; Andrade-Villanueva, J.F.; et al. Long-acting injectable cabotegravir + rilpivirine for HIV maintenance therapy: Week 48 pooled analysis of Phase 3 ATLAS and FLAIR trials. J. Acquir. Immune Defic. Syndr. 2020, 85, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Overton, E.T.; Richmond, G.; Rizzardini, G.; Jaeger, H.; Orrell, C.; Nagimova, F.; Bredeek, F.; Deltoro, M.G.; Swindells, S.; Andrade-Villanueva, J.F.; et al. Long-acting cabotegravir and rilpivirine dosed every 2 months in adults with HIV-1 infection (ATLAS-2M), 48-week results: A randomised, multicentre, open-label, phase 3b, non-inferiority study. Lancet 2020, 396, 1994–2005. [Google Scholar] [CrossRef]
- Chounta, V.; Overton, E.T.; Mills, A.; Swindells, S.; Benn, P.D.; Vanveggel, S.; van Solingen-Ristea, R.; Wang, Y.; Hudson, K.J.; Shaefer, M.S.; et al. Patient-Reported Outcomes Through 1 Year of an HIV-1 Clinical Trial Evaluating Long-Acting Cabotegravir and Rilpivirine Administered Every 4 or 8 Weeks (ATLAS-2M). Patient-Patient-Cent. Outcomes Res. 2021, 14, 849–862. [Google Scholar] [CrossRef] [PubMed]
- U.S. Prescribing Information for Cabenuva 2022. Available online: https://gskpro.com/content/dam/global/hcpportal/en_US/Prescribing_Information/Cabenuva/pdf/CABENUVA-PI-PIL-IFU2-IFU3.PDF (accessed on 17 February 2022).
- Product Monograph for CABENUVA 2021. Available online: https://viivhealthcare.com/content/dam/cf-viiv/viiv-healthcare/en_GB/medicines/CABENUVA-VOCABRIA-PM-26-Mar-2021.pdf (accessed on 2 May 2021).
- Ryan, M.; Gerard, K. Using discrete choice experiments to value health care programmes: Current practice and future research reflections. Appl. Health Econ. Health Policy. 2003, 2, 55–64. [Google Scholar]
- Soekhai, V.; de Bekker-Grob, E.W.; Ellis, A.R.; Vass, C.M. Discrete Choice Experiments in Health Economics: Past, Present and Future. Pharmacoeconomics 2019, 37, 201–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerrigan, D.; Mantsios, A.; Gorgolas, M.; Montes, M.; Pulido, F.; Brinson, C.; de Vente, J.; Richmond, G.J.; Beckham, S.W.; Hammon, P.; et al. Experiences with long acting injectable ART: A qualitative study among PLHIV participating in a Phase II study of cabotegravir + rilpivirine (LATTE-2) in the United States and Spain. PLoS ONE 2018, 13, e0190487. [Google Scholar] [CrossRef] [Green Version]
- Brégigeon-Ronot, S.; Cheret, A.; Cabié, A.; Prazuck, T.; Volny-Anne, A.; Ali, S.; Bottomley, C.; Finkielsztejn, L.; Philippe, C.; Parienti, J.J. Evaluating patient preference and satisfaction for human immunodeficiency virus therapy in France. Patient Prefer. Adherence 2017, 11, 1159–1169. [Google Scholar] [CrossRef] [Green Version]
- Gazzard, B.; Leen, C.; Morton, J.; Ali, S.; Benzie, A.; Murray, M.; Forni, J. Evaluation of patient satisfaction with antiretroviral therapy using a discrete choice experiment. HIV Med. 2015, 16, 63. [Google Scholar]
- Orme, M.; Miners, A.; Sabin, C.; Fisher, M. A discrete choice experiment to evaluate HIV patient preference for simplified treatment regimens: Results from the UK survey. HIV Med. 2015, 16, 13. [Google Scholar]
- Carlsson, F.; Raun Morkbak, M.; Boye Olsen, S. The first time is the hardest: A test of ordering effects in choice experiments. J. Choice Modelling 2012, 5, 19–37. [Google Scholar] [CrossRef] [Green Version]
- Johnson, F.R.; Yang, J.C.; Reed, S.D. The internal validity of discrete choice experiment data: A testing tool for quantitative assessments. Value Health 2019, 22, 157–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de los Rios, P.; Okoli, C.; Young, B.; Allan, B.; Castellanos, E.; Brough, G.; Eremin, A.; Corbelli, G.M.; Hardy, W.D.; Van de Velde, N. Treatment aspirations and attitudes towards innovative medications among people living with HIV in 25 countries. Popul. Med. 2020, 2, 23. [Google Scholar] [CrossRef]
- Dandachi, D.; Dang, B.N.; Lucari, B.; Swindells, S.; Giordano, T.P. Acceptability and preferences for long-acting antiretroviral formulations among people with HIV infection. AIDS Care 2020, 33, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Koren, D.E.; Fedkiv, V.; Zhao, H.; Bettiker, R.; Tedaldi, E.; Samuel, R. Perceptions of injectable antiretrovirals in an urban HIV clinic. Open Forum Infect. Dis. 2019, 6, S866. [Google Scholar] [CrossRef]
- Derrick, C.B.; Ostermann, J.; Weissman, S.B.; Hobbie, A.; Alshareef, N.; Weinhold, A.; Yelverton, V.; Thielman, N.M. Who wants to switch? Gauging patient interest in novel antiretroviral therapies. Open Forum Infect. Dis. 2018, 5, ofy247. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Estimated HIV Incidence and Prevalence in the United States, 2014–2018. HIV Surveillance Supplemental Report 2020; 25(No. 1). Available online: http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html (accessed on 2 May 2021).
- Public Health Agency of Canada. Summary: Estimates of HIV Incidence, Prevalence and Canada’s Progress on Meeting the 90-90-90 HIV Targets, 2018. 2020. Available online: https://www.canada.ca/content/dam/hc-sc/documents/services/publications/diseases-conditions/summary-estimates-hiv-incidence-prevalence-canadas-progress-90-90-90/national-hiv-estimates-report-2018-en.pdf (accessed on 2 May 2021).


{kind=link}
{kind=link}
{kind=link}
| Attributes | Attribute Description | Attribute Levels (Variable Name) |
|---|---|---|
| Dosing frequency | PLWH: How often you would receive the HIV treatment. For LAI, you would receive two injections each time at your HIV doctor’s clinic. Physicians: How often your PLWH would receive the HIV treatment. For LAI, two injections are given each time at your HIV clinic. | Oral: One pill, every day |
LAI:
| ||
| Risk of side effects | How many PLWH on a treatment develop mild to moderate bothersome side effects. | Oral and LAI:
|
| Forgivability | PLWH: The length of time that you have to take a missed dose without risking loss of viral suppression. You resume the normal dosing frequency after taking this catch-up dose. Physicians: the length of time PLWH have to take a missed dose without risking loss of viral suppression. PLWH resume the normal dosing frequency after taking this catch-up dose. | Oral:
|
LAI:
| ||
| Food and mealtime restrictions | PLWH: How much you are restricted in what and when you eat. Physicians: How much PLWH are restricted in what and when they eat. | Oral:
|
| LAI: None |
| Challenge (Variable Name) | PLWH | Physician |
|---|---|---|
| Lifestyle (Reference) | You find that your current treatment increasingly interferes with your lifestyle. While the treatment is becoming an inconvenience, you generally manage to follow your treatment dosing schedule. | The treatment increasingly interferes with the PLWH’s busy lifestyle. However, the PLWH manages to adhere to your treatment advice. |
| Lifestyle and adherence (Adhere) | You notice that you are increasingly missing a treatment dose. You are concerned that the treatment does not fit very well into your lifestyle. | You notice that the PLWH increasingly misses a treatment dose. You are concerned that the treatment does not fit very well into your PLWH’s lifestyle. |
| Worry/Fatigue (Worry) | You worry about the need to take your HIV medicine daily and you are increasingly tired of having to take the medicine. Every time you take your HIV medicine it is a reminder of your HIV. Your treatment feels like a burden to you. | You notice that the daily need to take the medicine worries your PLWH and causes anxiety. You are concerned about how the PLWH will manage the treatment in the long term. |
| Side effects (Side_effect) | You are struggling with the side effects of your medication. The side effects are becoming increasingly burdensome and you wonder how you will be able to manage them in the future. | The PLWH struggles with the management of side effects. You are concerned about how the PLWH will manage the side effects in the future. |
| Disclosure (Disclosue) | You constantly worry that a friend, family member, or co-worker might discover your HIV medicine. Not many people know you have HIV and you carefully hide your pills. | The PLWH seems to constantly worry that friends, family members, or others discover the medicine. Not many people know the PLWH has HIV, and the PLWH is hiding the pills carefully. |
| No challenge (Excluded for for physicians) | You are generally satisfied with your current treatment. However, you may be curious to learn about new HIV treatments. | Not applicable in physician DCE |
| Overall (N = 553) | US (n = 453) | Canada (n = 100) | |
|---|---|---|---|
| Gender, n (%) | |||
| Female | 183 (33.1) | 146 (32.2) | 37 (37.0) |
| Male | 365 (66.0) | 304 (67.1) | 61 (61.0) |
| Transgender | 5 (0.9) | 3 (0.7) | 2 (2.0) |
| Age, years | |||
| Mean (SD) | 39.3 (12.2) | 39.5 (12.3) | 38.4 (11.5) |
| Age group, n (%) | |||
| >55 years old | 82 (14.9) | 72 (15.9) | 10 (10.0) |
| Race a, n (%) | |||
| White/Caucasian | 311 (56.2) | 250 (55.2) | 61 (61.0) |
| Black/African American | 105 (19.0) | 96 (21.2) | 9 (9.0) |
| Hispanic/Latino | 51 (9.2) | 51 (11.3) | N/A |
| Asian | 31 (5.6) | 16 (3.5) | 15 (15.0) |
| Other/Mixed race | 54 (9.7) | 40 (8.8) | 14 (14.0) |
| Ethnicity, n (%) | |||
| Hispanic/Latino | 77 (13.9) | 77 (17.0) | N/A |
| Not Hispanic/Latino | 475 (85.9) | 376 (83.0) | N/A |
| Sexual orientation, n (%) | |||
| Straight | 344 (62.2) | 282 (62.3) | 62 (62.0) |
| Lesbian, gay, bisexual, transgender, or queer (LGBTQ) | 159 (28.8) | 132 (29.1) | 27 (27.0) |
| Men who have sex with men | 46 (8.3) | 35 (7.7) | 11 (11.0) |
| Other | 2 (0.4) | 2 (0.4) | 0 |
| Prefer not to say | 2 (0.4) | 2 (0.4) | 0 |
| Income (USD), n (%) | |||
| Less than USD 25,000 | 111 (20.1) | 99 (21.9) | 12 (12.0) |
| USD 25,000 to USD 49,999 | 82 (14.8) | 67 (14.8) | 15 (15.0) |
| USD 50,000 to USD 74,999 | 94 (17.0) | 74 (16.3) | 20 (20.0) |
| USD 75,000 to USD 99,999 | 97 (17.5) | 86 (19.0) | 11 (11.0) |
| USD 100,000 to USD 149,999 | 109 (19.7) | 79 (17.4) | 30 (30.0) |
| USD 150,000 or more | 53 (9.6) | 42 (9.3) | 11 (11.0) |
| Prefer not to answer | 7 (1.3) | 6 (1.3) | 1 (1.0) |
| Time since diagnosis (group), n (%) | |||
| <1 year | 14 (2.5) | 13 (2.9) | 1 (1.0) |
| 1–2 years | 103 (18.6) | 84 (18.5) | 19 (19.0) |
| 2–5 years | 142 (25.7) | 109 (24.1) | 33 (33.0) |
| 5–10 years | 118 (21.3) | 98 (21.6) | 20 (20.0) |
| >10 years | 176 (31.8) | 149 (32.9) | 27 (27.0) |
| Time since diagnosis, years | |||
| Mean (SD) | 9.4 (8.8) | 9.7 (9.0) | 8.3 (8.2) |
| Time since initiating therapy, n (%) | |||
| ≤1 year ago | 102 (18.4) | 76 (16.8) | 26 (26.0) |
| 1 year to 3 years ago | 152 (27.5) | 123 (27.2) | 29 (29.0) |
| 3–5 years ago | 78 (14.1) | 64 (14.1) | 14 (14.0) |
| 5–10 years ago | 96 (17.4) | 86 (19.0) | 10 (10.0) |
| 10 years ago or longer | 120 (21.7) | 102 (22.5) | 18 (18.0) |
| I do not remember | 5 (0.9) | 2 (0.4) | 3 (3.0) |
| Overall (N = 456) | US (n = 305) | Canada (n = 151) | |
|---|---|---|---|
| Time practicing medicine, years | |||
| Mean (SD) | 16.1 (8.4) | 16.8 (8.4) | 14.5 (8.1) |
| Median | 15.0 | 16.0 | 13.0 |
| Min–max | 2.0–39.0 | 2.0–37.0 | 2.0–39.0 |
| Time treating HIV | |||
| Mean (SD) | 13.2 (8.1) | 14.6 (8.2) | 10.5 (6.9) |
| Median | 12.0 | 13.0 | 9.0 |
| Min–max | 2.0–34.0 | 2.0–34.0 | 2.0–30.0 |
| % clinical time dedicated to HIV care | |||
| Mean (SD) | 35.7 (30.1) | 37.8 (31.0) | 31.3 (27.7) |
| Median | 25.0 | 30.0 | 20.0 |
| Min–max | 1.0–100.0 | 1.0–100.0 | 1.0–90.0 |
| Location, n (%) | |||
| Rural/Countryside | 29 (6.4) | 22 (7.2) | 7 (4.6) |
| Outskirts/Suburbs of a small city | 38 (8.3) | 27 (8.9) | 11 (7.3) |
| Center or close to center of a small city | 96 (21.1) | 62 (20.3) | 34 (22.5) |
| Outskirts/Suburbs of a large city | 93 (20.4) | 66 (21.6) | 27 (17.9) |
| Center or close to center of a large city | 200 (43.9) | 128 (42) | 72 (47.7) |
| Role, n (%) | |||
| Infectious disease specialist | 136 (29.8) | 120 (39.3) | 16 (10.6) |
| Internal medicine/primary care/general doctor/family practitioner | 250 (54.8) | 154 (50.5) | 96 (63.6) |
| Physician assistant/nurse practitioner | 13 (2.9) | 5 (1.6) | 8 (5.3) |
| HIV specialist | 50 (11) | 24 (7.9) | 26 (17.2) |
| Immunologist | 1 (0.2) | 0 | 1 (0.7) |
| Other | 6 (1.3) | 2 (0.7) | 4 (2.6) |
| Clinic/Facility, n (%) | |||
| Closed system/integrated network | 18 (3.9) | 14 (4.6) | 4 (2.6) |
| Large group practice | 126 (27.6) | 82 (26.9) | 44 (29.1) |
| Small group or individual practice | 145 (31.8) | 99 (32.5) | 46 (30.5) |
| Community or regional hospital | 58 (12.7) | 31 (10.2) | 27 (17.9) |
| Ryan White clinic | 19 (4.2) | 19 (6.2) | 0 |
| Academic system or hospital | 90 (19.7) | 60 (19.7) | 30 (19.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gelhorn, H.; Garris, C.; Arthurs, E.; Spinelli, F.; Cutts, K.; Chua, G.N.; Collacott, H.; Lebouché, B.; Lowman, E.; Rice, H.; et al. Patient and Physician Preferences for Regimen Attributes for the Treatment of HIV in the United States and Canada. J. Pers. Med. 2022, 12, 334. https://doi.org/10.3390/jpm12030334
Gelhorn H, Garris C, Arthurs E, Spinelli F, Cutts K, Chua GN, Collacott H, Lebouché B, Lowman E, Rice H, et al. Patient and Physician Preferences for Regimen Attributes for the Treatment of HIV in the United States and Canada. Journal of Personalized Medicine. 2022; 12(3):334. https://doi.org/10.3390/jpm12030334
Chicago/Turabian StyleGelhorn, Heather, Cindy Garris, Erin Arthurs, Frank Spinelli, Katelyn Cutts, Gin Nie Chua, Hannah Collacott, Bertrand Lebouché, Erik Lowman, Howard Rice, and et al. 2022. "Patient and Physician Preferences for Regimen Attributes for the Treatment of HIV in the United States and Canada" Journal of Personalized Medicine 12, no. 3: 334. https://doi.org/10.3390/jpm12030334
APA StyleGelhorn, H., Garris, C., Arthurs, E., Spinelli, F., Cutts, K., Chua, G. N., Collacott, H., Lebouché, B., Lowman, E., Rice, H., & Heidenreich, S. (2022). Patient and Physician Preferences for Regimen Attributes for the Treatment of HIV in the United States and Canada. Journal of Personalized Medicine, 12(3), 334. https://doi.org/10.3390/jpm12030334