
Prediction of Incomplete Response of Primary Tumour Based on Clinical and Radiomics Features in Inoperable Head and Neck Cancers after Definitive Treatment

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment and Follow Up
2.3. Endpoints
2.4. Clinical Features
2.5. Radiomic Feature Extraction
2.6. Model Training and Validation
3. Results
3.1. Patients’ Characteristics
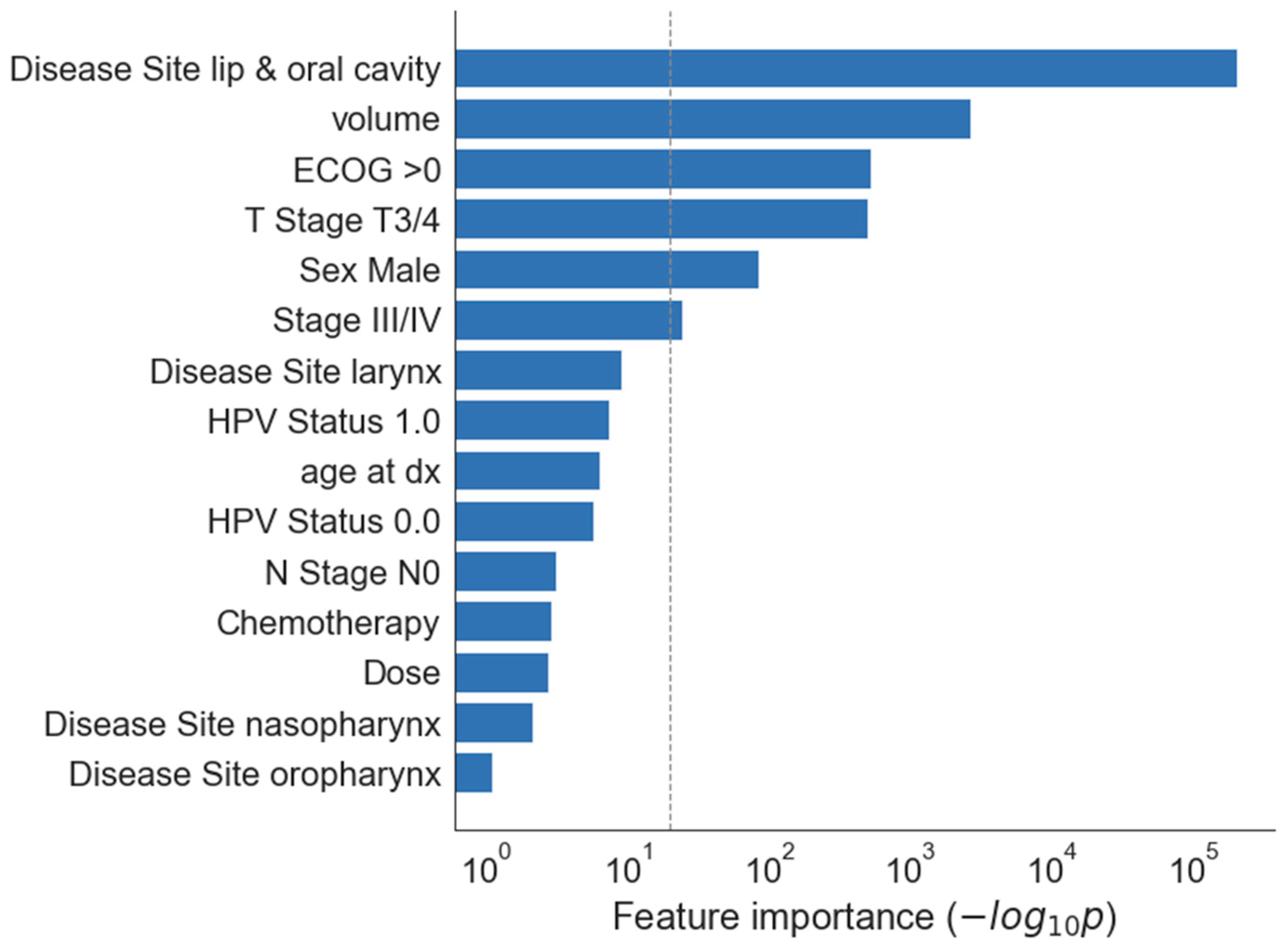
3.2. Clinical Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gouw, Z.A.R.; Jasperse, B.; Sonke, J.-J.; Heemsbergen, W.D.; Navran, A.; Hamming-Vrieze, O.; Paul de Boer, J.; van den Brekel, M.W.M.; Al-Mamgani, A. A predictive model for residual disease after (chemo) radiotherapy in oropharyngeal carcinoma: Combined radiological and clinical evaluation of tumor response. Clin. Transl. Radiat. Oncol. 2017, 6, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagh, A.; Grau, C.; Overgaard, J. Failure pattern and salvage treatment after radical treatment of head and neck cancer. Acta Oncol. 2016, 55, 625–632. [Google Scholar] [CrossRef] [Green Version]
- Diamant, A.; Chatterjee, A.; Vallières, M.; Shenouda, G.; Seuntjens, J. Deep learning in head & neck cancer outcome prediction. Sci. Rep. 2019, 9, 2764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallières, M.; Kay-Rivest, E.; Perrin, L.J.; Liem, X.; Furstoss, C.; Aerts, H.J.W.L.; Khaouam, N.; Nguyen-Tan, P.F.; Wang, C.-S.; Sultanem, K.; et al. Radiomics strategies for risk assessment of tumour failure in head-and-neck cancer. Sci. Rep. 2017, 7, 10117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.; Ma, S.J.; Farrugia, M.; Iovoli, A.J.; Wooten, K.E.; Gupta, V.; McSpadden, R.P.; Kuriakose, M.A.; Markiewicz, M.R.; Chan, J.M.; et al. Machine Learning Incorporating Host Factors for Predicting Survival in Head and Neck Squamous Cell Carcinoma Patients. Cancers 2021, 13, 4559. [Google Scholar] [CrossRef]
- Keek, S.; Sanduleanu, S.; Wesseling, F.; De Roest, R.; van den Brekel, M.; Van Der Heijden, M.; Vens, C.; Giuseppina, C.; Licitra, L.; Scheckenbach, K.; et al. Computed tomography-derived radiomic signature of head and neck squamous cell carcinoma (peri)tumoral tissue for the prediction of locoregional recurrence and distant metastasis after concurrent chemo-radiotherapy. PLoS ONE 2020, 15, e0232639. [Google Scholar] [CrossRef]
- Han, K.; Joung, J.F.; Han, M.; Sung, W.; Kang, Y.-N. Locoregional Recurrence Prediction Using a Deep Neural Network of Radiological and Radiotherapy Images. J. Pers. Med. 2022, 12, 143. [Google Scholar] [CrossRef]
- Zhai, T.-T.; Langendijk, J.A.; van Dijk, L.V.; van der Schaaf, A.; Sommers, L.; Vemer-van den Hoek, J.G.M.; Bijl, H.P.; Halmos, G.B.; Witjes, M.J.H.; Oosting, S.F.; et al. Pre-treatment radiomic features predict individual lymph node failure for head and neck cancer patients. Radiother. Oncol. 2020, 146, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Zhai, T.-T.; Wesseling, F.; Langendijk, J.A.; Shi, Z.; Kalendralis, P.; van Dijk, L.V.; Hoebers, F.; Steenbakkers, R.J.H.M.; Dekker, A.; Wee, L.; et al. External validation of nodal failure prediction models including radiomics in head and neck cancer. Oral Oncol. 2020, 112, 105083. [Google Scholar] [CrossRef]
- Grégoire, V.; Eisbruch, A.; Hamoir, M.; Levendag, P. Proposal for the delineation of the nodal CTV in the node-positive and the post-operative neck. Radiother. Oncol. 2006, 79, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Grégoire, V.; Evans, M.; Le, Q.-T.; Bourhis, J.; Budach, V.; Chen, A.; Eisbruch, A.; Feng, M.; Giralt, J.; Gupta, T.; et al. Delineation of the primary tumour Clinical Target Volumes (CTV-P) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity squamous cell carcinoma: AIRO, CACA, DAHANCA, EORTC, GEORCC, GORTEC, HKNPCSG, HNCIG, IAG-KHT, LPRHHT, NCIC CTG, NCRI, NRG Oncology, PHNS, SBRT, SOMERA, SRO, SSHNO, TROG consensus guidelines. Radiother. Oncol. 2018, 126, 3–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piotrowski, T.; Kaźmierska, J.; Sokołowski, A.; Skórska, M.; Jodda, A.; Ryczkowski, A.; Cholewiński, W.; Bąk, B. Impact of the spinal cord position uncertainty on the dose received during head and neck helical tomotherapy: Impact of the SC Position on the Dose. J. Med. Imaging Radiat. Oncol. 2013, 57, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Andrearczyk, V.; Fontaine, P.; Oreiller, V.; Castelli, J.; Jreige, M.; Prior, J.O.; Depeursinge, A. Multi-task Deep Segmentation and Radiomics for Automatic Prognosis in Head and Neck Cancer. In Predictive Intelligence in Medicine. PRIME 2021; Rekik, I., Adeli, E., Park, S.H., Schnabel, J., Eds.; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2021; Volume 12928, pp. 147–156. [Google Scholar] [CrossRef]
- Bogowicz, M.; Pavic, M.; Riesterer, O.; Finazzi, T.; Garcia Schüler, H.; Holz-Sapra, E.; Rudofsky, L.; Basler, L.; Spaniol, M.; Ambrusch, A.; et al. Targeting Treatment Resistance in Head and Neck Squamous Cell Carcinoma—Proof of Concept for CT Radiomics-Based Identification of Resistant Sub-Volumes. Front. Oncol. 2021, 11, 664304. [Google Scholar] [CrossRef]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef]
- Le, W.T.; Vorontsov, E.; Romero, F.P.; Seddik, L.; Elsharief, M.M.; Nguyen-Tan, P.F.; Roberge, D.; Bahig, H.; Kadoury, S. Cross-institutional outcome prediction for head and neck cancer patients using self-attention neural networks. Sci. Rep. 2022, 12, 3183. [Google Scholar] [CrossRef]
- Scher, E.D.; Romesser, P.B.; Chen, C.; Ho, F.; Wuu, Y.; Sherman, E.J.; Fury, M.G.; Wong, R.J.; McBride, S.; Lee, N.Y.; et al. Definitive chemoradiation for primary oral cavity carcinoma: A single institution experience. Oral Oncol. 2015, 51, 709–715. [Google Scholar] [CrossRef] [Green Version]
- Hosni, A.; Chiu, K.; Huang, S.H.; Xu, W.; Huang, J.; Bayley, A.; Bratman, S.V.; Cho, J.; Giuliani, M.; Kim, J.; et al. Non-operative management for oral cavity carcinoma: Definitive radiation therapy as a potential alternative treatment approach. Radiother. Oncol. 2020, 154, 70–75. [Google Scholar] [CrossRef]
- Foster, C.C.; Melotek, J.M.; Brisson, R.J.; Seiwert, T.Y.; Cohen, E.E.W.; Stenson, K.M.; Blair, E.A.; Portugal, L.; Gooi, Z.; Agrawal, N.; et al. Definitive chemoradiation for locally-advanced oral cavity cancer: A 20-year experience. Oral Oncol. 2018, 80, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Bøje, C.R.; Dalton, S.O.; Grønborg, T.K.; Primdahl, H.; Kristensen, C.A.; Andersen, E.; Johansen, J.; Andersen, L.J.; Overgaard, J. The impact of comorbidity on outcome in 12623 Danish Head and Neck Cancer Patients: A population based study from the DAHANCA database. Acta Oncol. 2013, 52, 285–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human Papillomavirus and Survival of Patients with Oropharyngeal Cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Doran, S.J.; Kumar, S.; Orton, M.; D’Arcy, J.; Kwaks, F.; O’Flynn, E.; Ahmed, Z.; Downey, K.; Dowsett, M.; Turner, N.; et al. “Real-world” radiomics from multi-vendor MRI: An original retrospective study on the prediction of nodal status and disease survival in breast cancer, as an exemplar to promote discussion of the wider issues. Cancer Imaging 2021, 21, 37. [Google Scholar] [CrossRef]
- De Maria Marchiano, R.; Di Sante, G.; Piro, G.; Carbone, C.; Tortora, G.; Boldrini, L.; Pietragalla, A.; Daniele, G.; Tredicine, M.; Cesario, A.; et al. Translational Research in the Era of Precision Medicine: Where We Are and Where We Will Go. J. Pers. Med. 2021, 11, 216. [Google Scholar] [CrossRef] [PubMed]
- Selim, M.; Zhang, J.; Fei, B.; Zhang, G.-Q.; Chen, J. CT Image Harmonization for Enhancing Radiomics Studies. In Proceedings of the 2021 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Houston, TX, USA, 9–12 December 2021; pp. 1057–1062. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Characteristic n = 290 | Value |
|---|---|
| Age (years) | |
| Range | 20–81 |
| Median | 58 |
| Gender | |
| Male | 217 |
| Female | 73 |
| Primary Site | |
| Nasopharynx | 17 |
| Oropharynx | 131 |
| Hypopharynx | 32 |
| Oral cavity | 28 |
| Larynx | 82 |
| Tumour classification | |
| T1 | 15 |
| T2 | 93 |
| T3 | 92 |
| T4 | 90 |
| Tumour Volume (cc) | |
| Median | 13.8 |
| Range | (0.2–91.3) |
| Stage AJCC v.7 | |
| I | 11 |
| II | 33 |
| III | 66 |
| IVA | 173 |
| IVB | 7 |
| Follow up (months) | |
| Median FU | 33.2 |
| Range | 3–112 |
| HPV status: | |
| Positive | 29 |
| Negative | 18 |
| Unknown | 243 |
| ECOG 0 | 79 |
| ECOG 1 | 211 |
| Treatment and Results, n = 290 | Number of Patients (%) |
|---|---|
| Treatment | |
| RT | 66 (22.7) |
| RTCT | 224 (77.2) |
| Residual disease | |
| All | 45 (15.6) |
| Primary site | 26 (9) |
| Lymph nodes | 11 (3.8) |
| Both | 8 (2.8) |
| Primary site | Primary site residual disease, n = 34 (% of all patients, % of all patients in corresponding primary site) |
| Oropharynx | 15 (5.2, 11.4) |
| Oral cavity | 11 (3.8, 39.3) |
| Larynx | 6 (2.1, 7.3) |
| Hypopharynx | 1 (0.3, 3.1) |
| Nasopharynx | 1 (0.3, 5.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaźmierska, J.; Kaźmierski, M.R.; Bajon, T.; Winiecki, T.; Bandurska-Luque, A.; Ryczkowski, A.; Piotrowski, T.; Bąk, B.; Żmijewska-Tomczak, M. Prediction of Incomplete Response of Primary Tumour Based on Clinical and Radiomics Features in Inoperable Head and Neck Cancers after Definitive Treatment. J. Pers. Med. 2022, 12, 1092. https://doi.org/10.3390/jpm12071092
Kaźmierska J, Kaźmierski MR, Bajon T, Winiecki T, Bandurska-Luque A, Ryczkowski A, Piotrowski T, Bąk B, Żmijewska-Tomczak M. Prediction of Incomplete Response of Primary Tumour Based on Clinical and Radiomics Features in Inoperable Head and Neck Cancers after Definitive Treatment. Journal of Personalized Medicine. 2022; 12(7):1092. https://doi.org/10.3390/jpm12071092
Chicago/Turabian StyleKaźmierska, Joanna, Michał R. Kaźmierski, Tomasz Bajon, Tomasz Winiecki, Anna Bandurska-Luque, Adam Ryczkowski, Tomasz Piotrowski, Bartosz Bąk, and Małgorzata Żmijewska-Tomczak. 2022. "Prediction of Incomplete Response of Primary Tumour Based on Clinical and Radiomics Features in Inoperable Head and Neck Cancers after Definitive Treatment" Journal of Personalized Medicine 12, no. 7: 1092. https://doi.org/10.3390/jpm12071092
APA StyleKaźmierska, J., Kaźmierski, M. R., Bajon, T., Winiecki, T., Bandurska-Luque, A., Ryczkowski, A., Piotrowski, T., Bąk, B., & Żmijewska-Tomczak, M. (2022). Prediction of Incomplete Response of Primary Tumour Based on Clinical and Radiomics Features in Inoperable Head and Neck Cancers after Definitive Treatment. Journal of Personalized Medicine, 12(7), 1092. https://doi.org/10.3390/jpm12071092