
Surgeon Dominated Design Can Improve the Accuracy of Patient-Specific Instruments in Kinematically Aligned TKA


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients
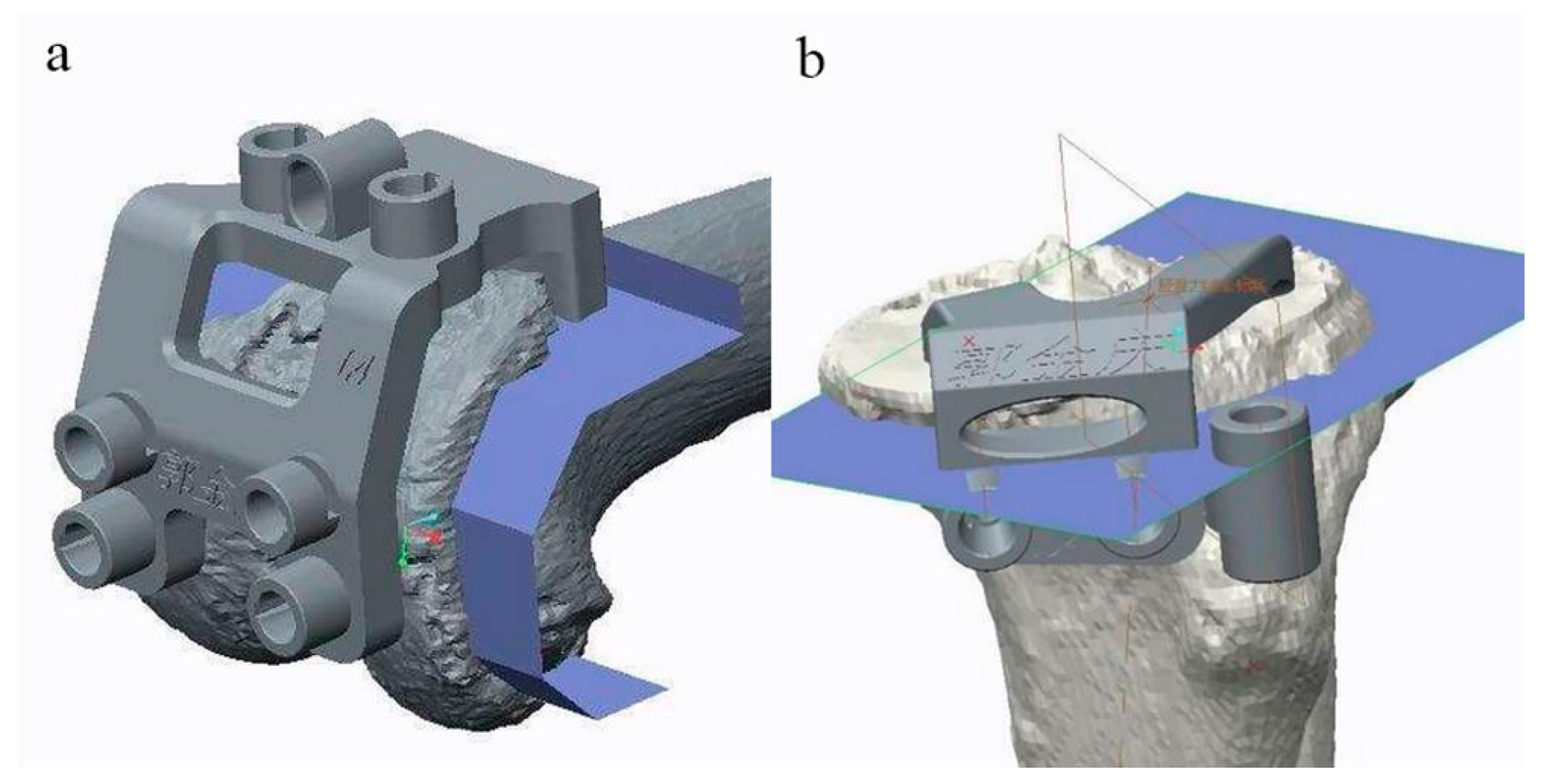
2.2. Design and Manufacturing of PSI
2.3. Grouping of Patients
2.4. Intraoperative Positioning of PSI
2.5. Assessment of the Accuracy of PSI
2.6. Statistical Analysis
3. Results
3.1. Descriptive Statistics of Patient Demographics
3.2. Accuracy of Bone Resection
3.3. Accuracy of Joint Line Restoration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Konan, S.; Howell, S.; Oussedik, S. Alignment targets in total knee arthroplasty. In Total Knee Arthroplasty; Springer: Cham, Switzerland, 2015; pp. 145–159. [Google Scholar]
- Koh, I.J.; Lin, C.C.; Patel, N.A.; Chalmers, C.E.; Maniglio, M.; Bin Han, S.; McGarry, M.H.; Lee, T.Q. Kinematically aligned total knee arthroplasty reproduces more native rollback and laxity than mechanically aligned total knee arthroplasty: A matched pair cadaveric study. Orthop. Traumatol. Surg. Res. 2019, 105, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Blakeney, W.; Clément, J.; Desmeules, F.; Hagemeister, N.; Rivière, C.; Vendittoli, P.-A. Kinematic alignment in total knee arthroplasty better reproduces normal gait than mechanical alignment. Knee Surg. Sports Traumatol. Arthrosc. 2018, 27, 1410–1417. [Google Scholar] [CrossRef] [PubMed]
- Shelton, T.J.; Gill, M.; Athwal, G.; Howell, S.M.; Hull, M.L. Outcomes in Patients with a Calipered Kinematically Aligned TKA That Already Had a Contralateral Mechanically Aligned TKA. J. Knee Surg. 2019, 34, 087–093. [Google Scholar] [CrossRef]
- An, V.V.; Twiggs, J.; Leie, M.; Fritsch, B.A. Kinematic alignment is bone and soft tissue preserving compared to mechanical alignment in total knee arthroplasty. Knee 2019, 26, 466–476. [Google Scholar] [CrossRef] [Green Version]
- Howell, S.M.; Shelton, T.J.; Hull, M.L. Implant Survival and Function Ten Years After Kinematically Aligned Total Knee Arthroplasty. J. Arthroplast. 2018, 33, 3678–3684. [Google Scholar] [CrossRef]
- Howell, S.M.; Papadopoulos, S.; Kuznik, K.T.; Hull, M.L. Accurate alignment and high function after kinematically aligned TKA performed with generic instruments. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2271–2280. [Google Scholar] [CrossRef]
- Patil, S.; Bunn, A.; Bugbee, W.D.; Colwell, C.W.; D’Lima, D.D. Patient-specific implants with custom cutting blocks better approximate natural knee kinematics than standard TKA without custom cutting blocks. Knee 2015, 22, 624–629. [Google Scholar] [CrossRef]
- Laende, E.K.; Richardson, C.G.; Dunbar, M.J. A randomized controlled trial of tibial component migration with kinematic alignment using patient-specific instrumentation versus mechanical alignment using computer-assisted surgery in total knee arthroplasty. Bone Jt. J. 2019, 101-B, 929–940. [Google Scholar] [CrossRef]
- Kim, K.-K.; Howell, S.M.; Won, Y.-Y. Kinematically Aligned Total Knee Arthroplasty with Patient-Specific Instrument. Yonsei Med. J. 2020, 61, 201–209. [Google Scholar] [CrossRef]
- Hutt, J.; LeBlanc, M.-A.; Massé, V.; Lavigne, M.; Vendittoli, P.-A. Kinematic TKA using navigation: Surgical technique and initial results. Orthop. Traumatol. Surg. Res. 2016, 102, 99–104. [Google Scholar] [CrossRef]
- Yeo, J.-H.; Seon, J.-K.; Lee, D.-H.; Song, E.-K. No difference in outcomes and gait analysis between mechanical and kinematic knee alignment methods using robotic total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2018, 27, 1142–1147. [Google Scholar] [CrossRef] [PubMed]
- Sassoon, A.; Nam, D.; Nunley, R.; Barrack, R. Systematic Review of Patient-specific Instrumentation in Total Knee Arthroplasty: New but Not Improved. Clin. Orthop. Relat. Res. 2015, 473, 151–158. [Google Scholar] [CrossRef] [Green Version]
- Cavaignac, E.; Pailhé, R.; Laumond, G.; Murgier, J.; Reina, N.; Laffosse, J.M.; Bérard, E.; Chiron, P. Evaluation of the accuracy of patient-specific cutting blocks for total knee arthroplasty: A meta-analysis. Int. Orthop. 2014, 39, 1541–1552. [Google Scholar] [CrossRef]
- Thienpont, E.; Schwab, P.-E.; Fennema, P. Efficacy of Patient-Specific Instruments in Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. J. Bone Jt. Surg. 2017, 99, 521–530. [Google Scholar] [CrossRef]
- Teeter, M.G.; Marsh, J.D.; Howard, J.L.; Yuan, X.; Vasarhelyi, E.M.; McCalden, R.W.; Naudie, D.D.R. A randomized controlled trial investigating the value of patient-specific instrumentation for total knee arthroplasty in the Canadian healthcare system. Bone Jt. J. 2019, 101-B, 565–572. [Google Scholar] [CrossRef]
- Parratte, S.; Blanc, G.; Boussemart, T.; Ollivier, M.; Le Corroller, T.; Argenson, J.-N. Rotation in total knee arthroplasty: No difference between patient-specific and conventional instrumentation. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2213–2219. [Google Scholar] [CrossRef]
- Huijbregts, H.J.T.A.M.; Khan, R.J.K.; Sorensen, E.; Fick, D.P.; Haebich, S. Patient-specific instrumentation does not improve radiographic alignment or clinical outcomes after total knee arthroplasty. Acta Orthop. 2016, 87, 386–394. [Google Scholar] [CrossRef] [Green Version]
- Levengood, G.A.; Dupee, J. Accuracy of Coronal Plane Mechanical Alignment in a Customized, Individually Made Total Knee Replacement with Patient-Specific Instrumentation. J. Knee Surg. 2017, 31, 792–796. [Google Scholar] [CrossRef] [Green Version]
- Pauzenberger, L.; Munz, M.; Brandl, G.; Frank, J.K.; Heuberer, P.R.; Laky, B.; Schwameis, E.; Anderl, W. Patient-specific instrumentation improved three-dimensional accuracy in total knee arthroplasty: A comparative radiographic analysis of 1257 total knee arthroplasties. J. Orthop. Surg. Res. 2019, 14, 1–7. [Google Scholar] [CrossRef]
- Tammachote, N.; Panichkul, P.; Kanitnate, S. Comparison of Customized Cutting Block and Conventional Cutting Instrument in Total Knee Arthroplasty: A Randomized Controlled Trial. J. Arthroplast. 2018, 33, 746–751.e3. [Google Scholar] [CrossRef]
- Kim, K.; Kim, J.; Lee, D.K.; Lim, S.; Eom, A.J. The Accuracy of Alignment Determined by Patient-Specific Instrumentation System in Total Knee Arthroplasty. Knee Surg. Relat. Res. 2019, 31, 19–24. [Google Scholar] [CrossRef]
- Hafez, M.A.; Moholkar, K. Patient-specific instruments: Advantages and pitfalls. SICOT-J 2017, 3, 66. [Google Scholar] [CrossRef] [PubMed]
- Pietsch, M.; Djahani, O.; Hochegger, M.; Plattner, F.; Hofmann, S. Patient-specific total knee arthroplasty: The importance of planning by the surgeon. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2220–2226. [Google Scholar] [CrossRef] [PubMed]
- Zambianchi, F.; Colombelli, A.; Digennaro, V.; Marcovigi, A.; Mugnai, R.; Fiacchi, F.; Sandoni, D.; Belluati, A.; Catani, F. Assessment of patient-specific instrumentation precision through bone resection measurements. Knee Surg. Sports Traumatol. Arthrosc. 2015, 25, 2841–2848. [Google Scholar] [CrossRef]
- Thienpont, E.; Bellemans, J.; Delport, H.; Van Overschelde, P.; Stuyts, B.; Brabants, K.; Victor, J. Patient-specific instruments: Industry’s innovation with a surgeon’s interest. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2227–2233. [Google Scholar] [CrossRef]
- An, V.V.; Sivakumar, B.S.; Phan, K.; Levy, Y.D.; Bruce, W.J. Accuracy of MRI-based vs. CT-based patient-specific instrumentation in total knee arthroplasty: A meta-analysis. J. Orthop. Sci. 2017, 22, 116–120. [Google Scholar] [CrossRef]
- Schotanus, M.G.M.; Thijs, E.; Heijmans, M.; Vos, R.; Kort, N.P. Favourable alignment outcomes with MRI-based patient-specific instruments in total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 2659–2668. [Google Scholar] [CrossRef]
- Kwon, O.-R.; Kang, K.-T.; Son, J.; Suh, D.-S.; Heo, D.B.; Koh, Y.-G. Patient-specific instrumentation development in TKA: 1st and 2nd generation designs in comparison with conventional instrumentation. Arch. Orthop. Trauma. Surg. 2016, 137, 111–118. [Google Scholar] [CrossRef]
- Yamamura, K.; Minoda, Y.; Sugama, R.; Ohta, Y.; Nakamura, S.; Ueyama, H.; Nakamura, H. Design improvement in patient-specific instrumentation for total knee arthroplasty improved the accuracy of the tibial prosthetic alignment in the coronal and axial planes. Knee Surg. Sports Traumatol. Arthrosc. 2019, 28, 1560–1567. [Google Scholar] [CrossRef]
- Woolson, S.T.; Harris, A.H.; Wagner, D.W.; Giori, N.J. Component Alignment During Total Knee Arthroplasty with Use of Standard or Custom Instrumentation: A randomized clinical trial using computed tomography for postoperative alignment measurement. J. Bone Jt. Surg. 2014, 96, 366–372. [Google Scholar] [CrossRef] [Green Version]
- Victor, J.; Dujardin, J.; Vandenneucker, H.; Arnout, N.; Bellemans, J. Patient-specific Guides Do Not Improve Accuracy in Total Knee Arthroplasty: A Prospective Randomized Controlled Trial. Clin. Orthop. Relat. Res. 2014, 472, 263–271. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Engineer Group (n = 10) | Surgeon Group (n = 14) | t | Sig. | |
|---|---|---|---|---|
| Age (years) | 66.8 ± 6.5 | 67.1 ± 4.1 | −0.126 | 0.901 |
| Side (Left/Right) | 6/4 | 8/6 | NA | NA |
| Gender (Male/Female) | 5/5 | 4/10 | NA | NA |
| Height (cm) | 165.5 ± 8.1 | 163.7 ± 5.8 | 0.631 | 0.534 |
| Weight (kg) | 72.1 ± 13.9 | 67.6 ± 11.1 | 0.886 | 0.385 |
| BMI (kg/m2) | 25.1 ± 3.2 | 25.1 ± 2.6 | 0.892 | 0.382 |
| Preop. Alignment (Varus/Valgus) | 9/1 | 14/0 | NA | NA |
| OP time (min) | 78.8 ± 9.9 | 75.9 ± 10.9 | 0.677 | 0.505 |
| Femoral component size (#2/#3/#4/#5) | 5/2/2/1 | 8/4/2/0 | NA | NA |
| Tibial component size (#2/#3/#4/#5) | 5/2/2/1 | 8/4/2/0 | NA | NA |
| Thicker (+2 mm) liner (Y/N) | 1/9 | 1/13 | NA | NA |
| Lateral patellar retinaculum release (Y/N) | 2/8 | 2/12 | NA | NA |
| Intraoperative tibial extracut (Y/N) | 2 medial side/8 | 1 medial side/13 | NA | NA |
| PSI Group | Facet | Distal Femur (mm) | Post. Condyle (mm) | Tibial Plateau (mm) | AVONA | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Side | Medial | Lateral | Medial | Lateral | Medial | Lateral | Main Effect | p Value | Interaction | p Value | |
| Engineer group | 0.5 ± 0.6 | 0.5 ± 0.4 | 0.8 ± 0.8 | 0.8 ± 0.6 | −0.28 ± 0.9 | 0.2 ± 0.8 | PSI Facets Side | <0.001 <0.001 0.608 | PSI * Facet PSI * Side Facet * Side PSI * Facet * Side | 0.325 0.326 0.101 0.925 | |
| Surgeon group | 0.1 ± 0.3 | 0.1 ± 0.3 | 0.4 ± 0.5 | 0.2 ± 0.5 | −0.3 ± 0.3 | −0.1 ± 0.3 | |||||
| PSI Group | Side of Joint Line (deg.) | ANOVA (p Value) | |||
|---|---|---|---|---|---|
| mLDFA | MPTA | PSI | Side | PSI * Parameters | |
| Engineer group | 1.40 ± 1.18 | 1.78 ± 1.44 | 0.010 | 0.466 | 0.576 |
| Surgeon group | 0.77 ± 0.66 | 0.82 ± 0.71 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, L.; Wang, Z.; Ma, D.; Qu, T. Surgeon Dominated Design Can Improve the Accuracy of Patient-Specific Instruments in Kinematically Aligned TKA. J. Pers. Med. 2022, 12, 1192. https://doi.org/10.3390/jpm12081192
Wen L, Wang Z, Ma D, Qu T. Surgeon Dominated Design Can Improve the Accuracy of Patient-Specific Instruments in Kinematically Aligned TKA. Journal of Personalized Medicine. 2022; 12(8):1192. https://doi.org/10.3390/jpm12081192
Chicago/Turabian StyleWen, Liang, Zhiwei Wang, Desi Ma, and Tiebing Qu. 2022. "Surgeon Dominated Design Can Improve the Accuracy of Patient-Specific Instruments in Kinematically Aligned TKA" Journal of Personalized Medicine 12, no. 8: 1192. https://doi.org/10.3390/jpm12081192