

Morphological and Optical Coherence Tomography Aspects of Non-Carious Cervical Lesions

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Teeth Prevelation and Preparation
2.2. Macroscopic Examination
2.3. OCT Examination
3. Results
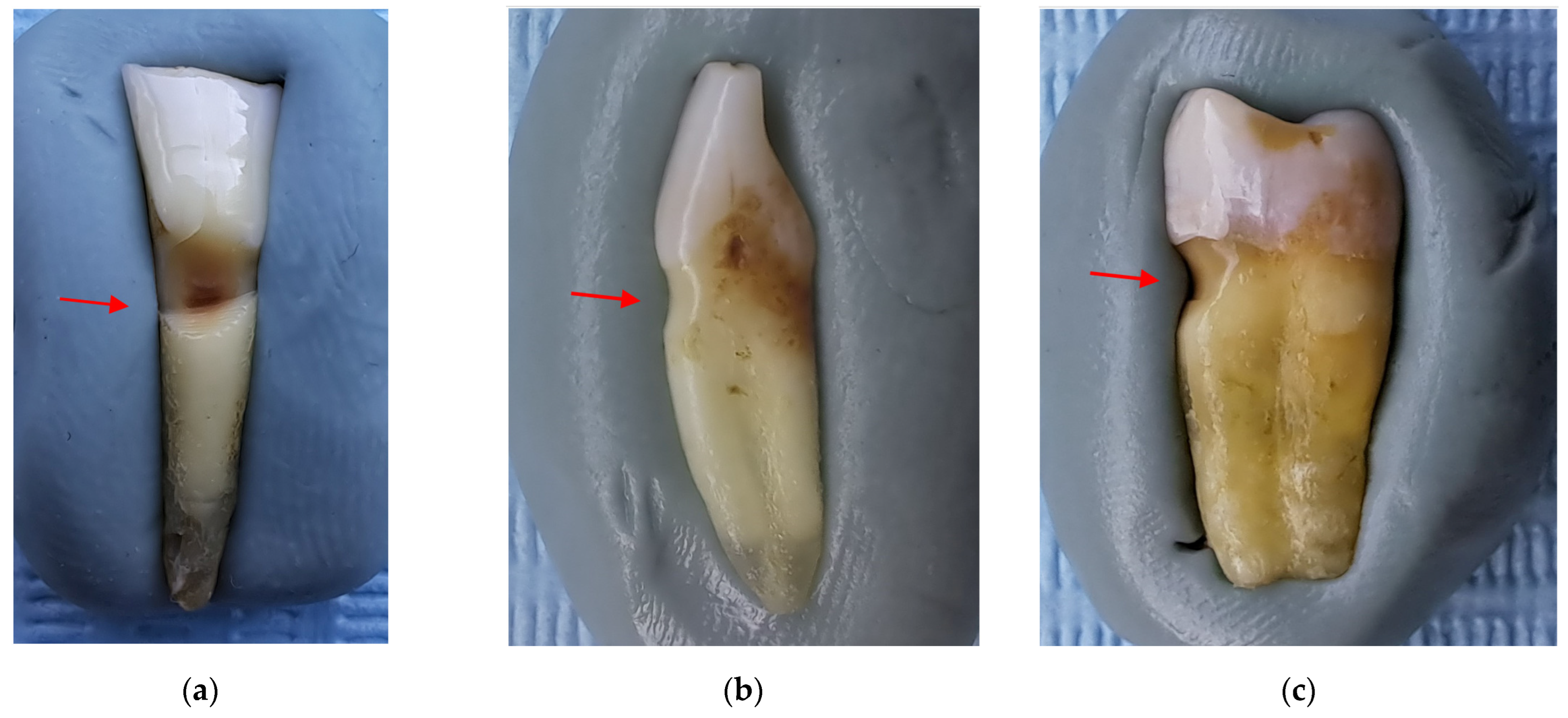
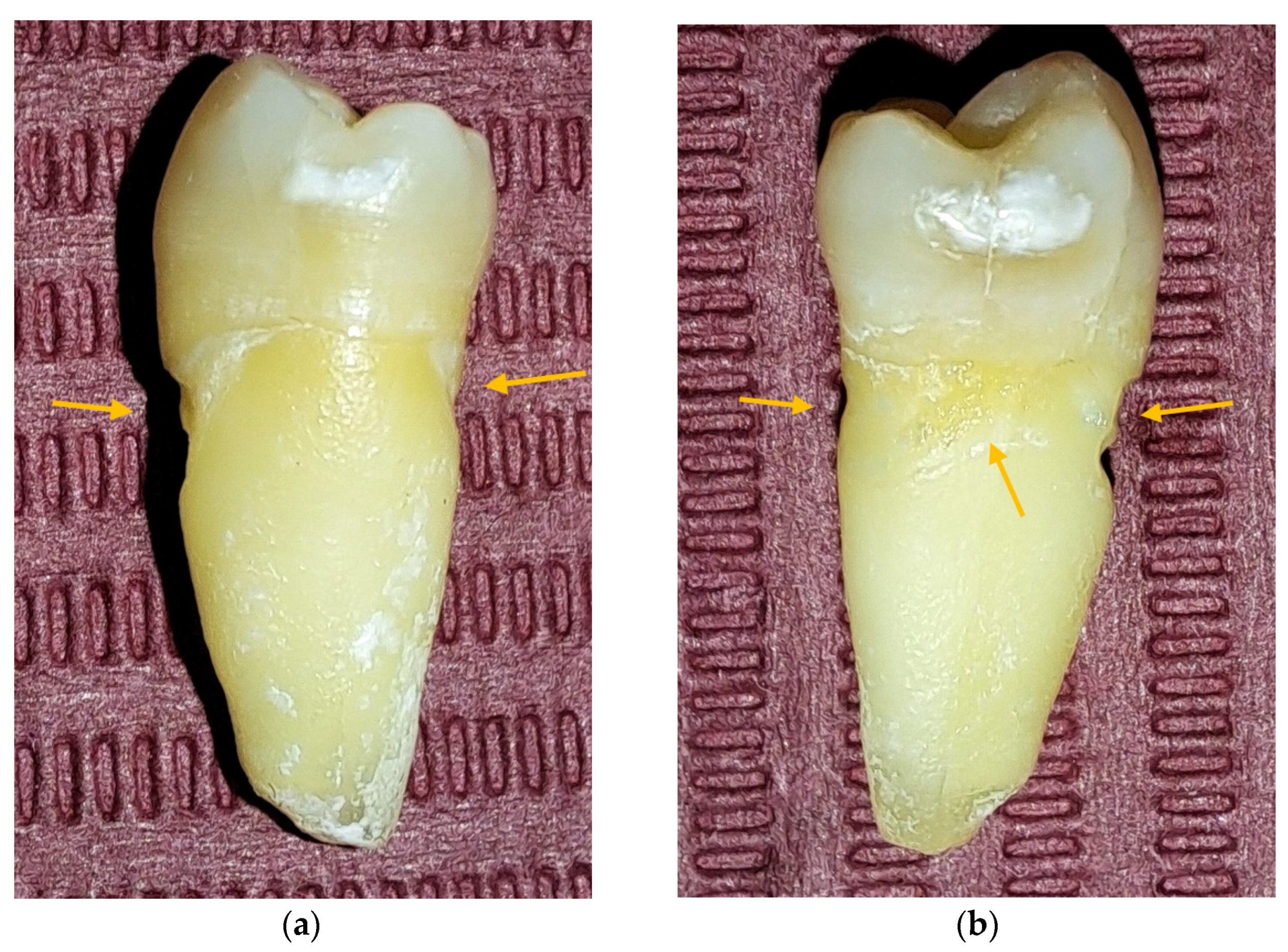
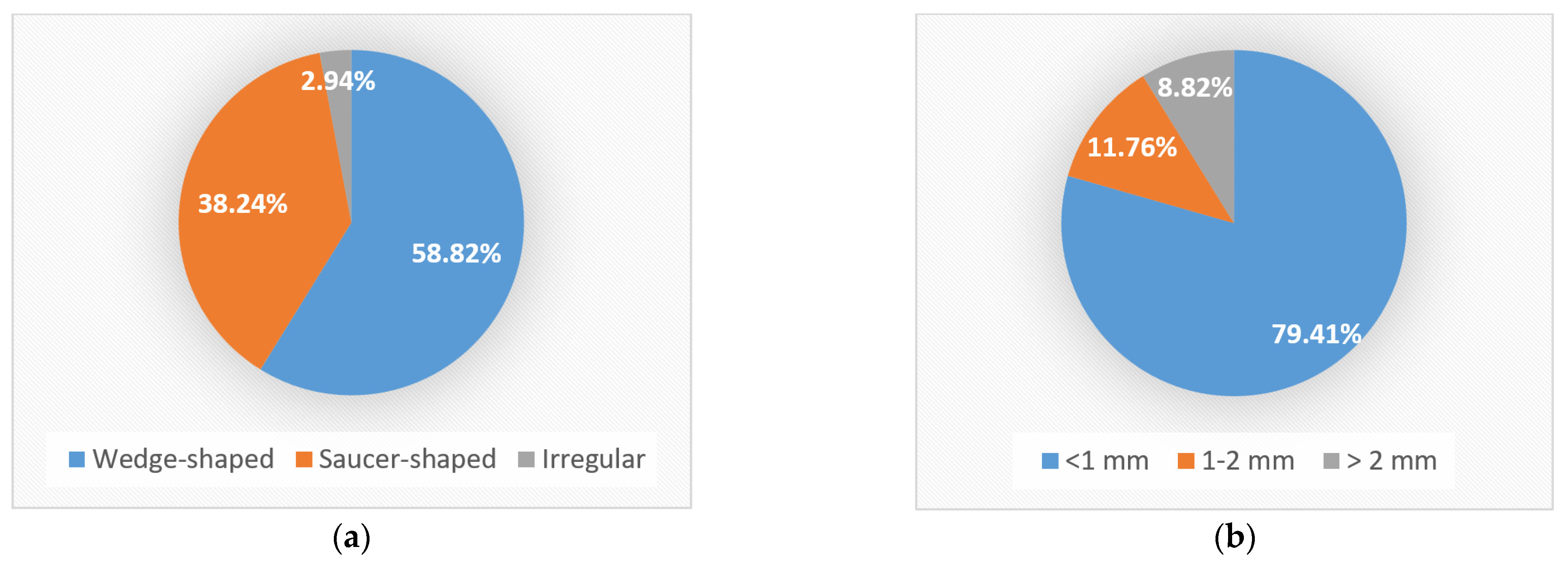
3.1. Macroscopic Examination of Teeth with NCCLs
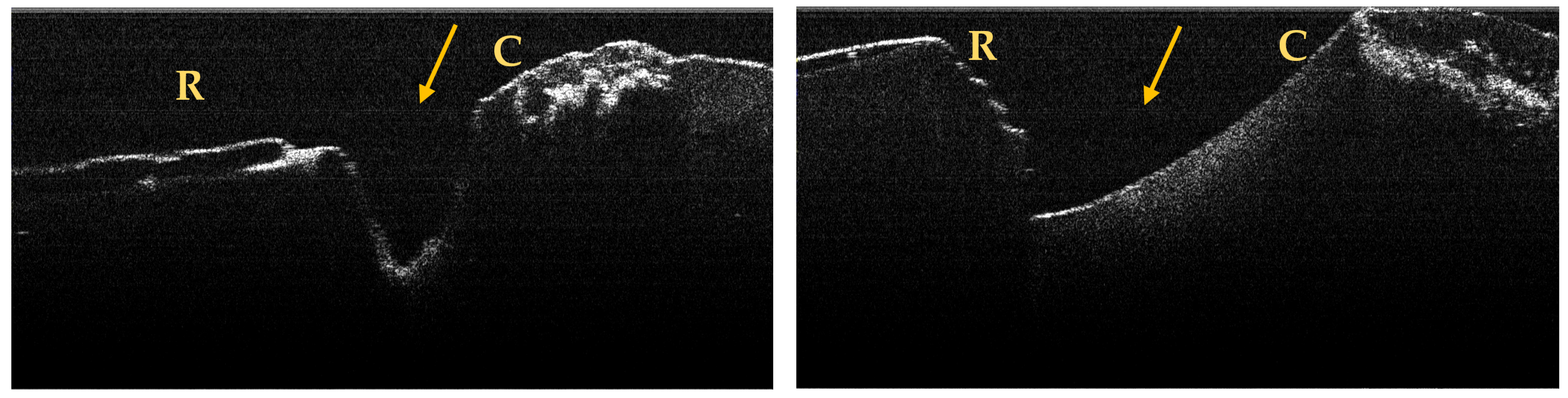
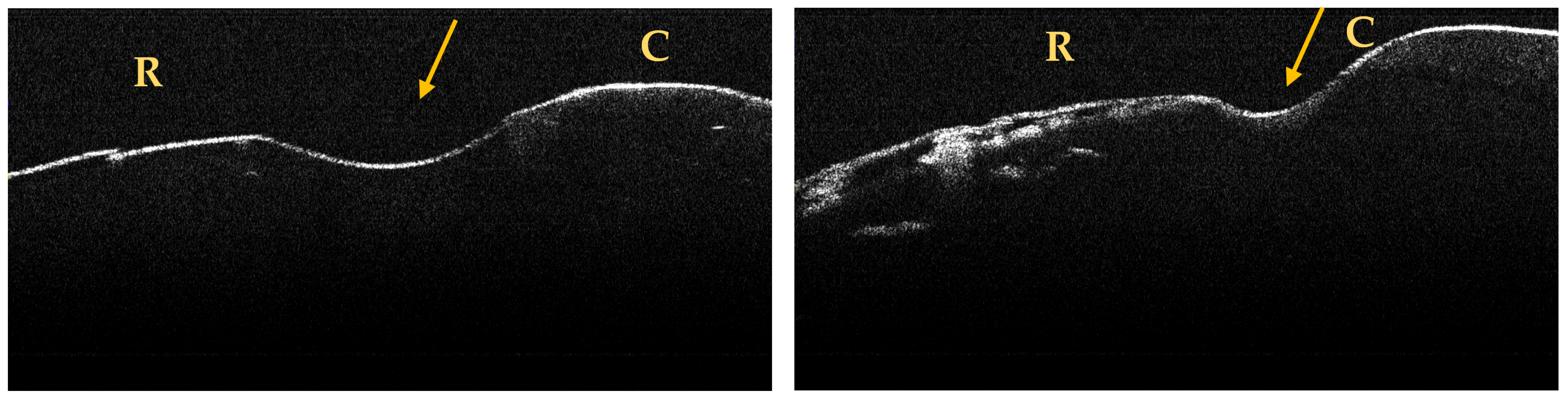
3.2. OCT Examination of Teeth Included in the Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Femiano, F.; Sorice, R.; Femiano, R.; Femiano, L.; Nucci, L.; Grassia, V.; Annunziata, M.; Baldi, A.; Scotti, N.; Nastri, L. Clinical Behavior of the Gingival Margin following Conservative “Coronally Dynamic” Restorations in the Presence of Non-Carious Cervical Lesions Associated with Gingival Recession: A Pilot Study. Dent. J. 2022, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, D.N.R.; Thomas, R.Z.; Soares, P.V.; Cune, M.S.; Gresnigt, M.M.M.; Slot, D.E. Prevalence of noncarious cervical lesions among adults: A systematic review. J. Dent. 2020, 95, 103285. [Google Scholar] [CrossRef]
- Koc Vural, U.; Meral, E.; Ergin, E.; Gürgan, S. Twenty-four-month clinical performance of a glass hybrid restorative in non-carious cervical lesions of patients with bruxism: A split-mouth, randomized clinical trial. Clin. Oral Investig. 2019, 24, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- Lührs, A.; Jacker-Guhr, S.; Günay, H.; Herrmann, P. Composite restorations placed in non-carious cervical lesions—Which cavity preparation is clinically reliable? Clin. Exp. Dent. Res. 2020, 6, 558–567. [Google Scholar] [CrossRef]
- Hunter, J. The Natural History of Human Teeth: Explaining Their Structure, Use, Formation, Growth, and Diseases; J. Johnson: London, UK, 1778; pp. 98–100. [Google Scholar]
- Zsigmondy, U. Über die keilförmigen Defekte an den Facialflächen der Zähne. Österr Ung. Vjhrschr Zahnärzte 1894, 1, 439–442. [Google Scholar]
- Grippo, J.O. Abfractions: A new classification of hard tissue lesions of teeth. J. Esthet. Dent. 1991, 3, 14–19. [Google Scholar] [CrossRef]
- Schlueter, N.; Amaechi, B.T.; Bartlett, D. Terminology of erosive tooth wear: Consensus report of a workshop organized by the ORCA and the Cariology Research Group of the IADR. Caries Res. 2020, 54, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Alves-Silva, E.G.; Arruda-Vasconcelos, R.; Mendes Louzada, L.; de-Jesus-Soares, A.; Ferraz, C.C.R.; Almeida, J.F.A.; Marciano, M.A.; Steiner-Oliveira, C.; Marques Santos, J.M.; Gomes, B.P.F.A. Effect of antimicrobial photodynamic therapy on the reduction of bacteria and virulence factors in teeth with primary endodontic infection. Photodiagnosis Photodyn. Ther. 2023, 41, 103292. [Google Scholar] [CrossRef]
- Jakupović, S.; Šehić, A.; Julardžija, F.; Gavranović-Glamoč, A.; Sofić, A.; Bajsman, A.; Kazazić, L. The Influence of Different Occlusal Loading on Six Restorative Materials for Restoration of Abfraction Lesions-Finite Element Analysis. Eur. J. Dent. 2022, 16, 886–894. [Google Scholar] [CrossRef]
- Tapia Ornelas, D.A.; Vela, M.O.R.; García Palencia, P. Abfraction: Etiopathogenesis, clinical aspect, diagnosis and treatment, a review literature. Int. J. Appl. Dent. Sci. 2022, 8, 97–100. [Google Scholar] [CrossRef]
- Rusu Olaru, A.; Popescu, M.R.; Dragomir, L.P.; Rauten, A.M. Clinical Study on Abfraction Lesions in Occlusal Dysfunction. Curr. Health Sci. J. 2019, 45, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Du, J.-K.; Wu, J.-H.; Chen, P.-H.; Ho, P.-S.; Chen, K.-K. Influence of cavity depth and restoration of non-carious cervical root lesions on strain distribution from various loading sites. BMC Oral Health. 2020, 20, 98. [Google Scholar] [CrossRef]
- Kolak, V.; Pesic, D.; Melih, I.; Lalovic, M.; Nikitovic, A.; Jakovljevic, A. Epidemiological investigation of non-carious cervical lesions and possible etiological factors. J. Clin. Exp. Dent. 2018, 10, e648–e656. [Google Scholar] [CrossRef]
- Yang, J.; Cai, D.; Wang, F.; He, D.; Ma, L.; Jin, Y.; Que, K. Noncarious cervical lesions (NCCLs) in a random sampling community population and the association of NCCLs with occlusive wear. J. Oral Rehabil. 2016, 43, 960–966. [Google Scholar] [CrossRef]
- Rees, J.S. The biomechanics of abfractions. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2006, 220, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Grippo, J.O.; Simring, M. Dental ‘erosion’ revisited. JADA 1995, 126, 619–630. [Google Scholar] [CrossRef]
- Lai, Z.Y.; Zhi, Q.H.; Zhou, Y.; Lin, H.C. Prevalence of non-carious cervical lesions and associated risk indicators in middle-aged and elderly populations in Southern China. Chin. J. Dent. Res. 2015, 18, 41–50. [Google Scholar] [PubMed]
- Que, K.; Guo, B.; Jia, Z.; Chen, Z.; Yang, J.; Gao, P. A cross-sectional study: Non-carious cervical lesions, cervical dentine hypersensitivity and related risk factors. J. Oral Rehabil. 2013, 40, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Hirata, Y.; Yamamoto, T.; Kawagoe, T.; Sasaguri, K.; Sato, S. Relationship between occlusal contact pattern and non-carious cervical lesions among male adults. Int. J. Stomatol. Occlusion Med. 2010, 3, 10–14. [Google Scholar] [CrossRef]
- Jakupovic, S.; Vukovic, A.; Korac, S.; Tahmiscija, I.; Bajsman, A. The prevalence, distribution and expression of noncarious cervical lesions (NCCL) in permanent dentition. Mater. Sociomed. 2010, 22, 200–204. [Google Scholar]
- Sakhabutdinova, L.; Kamenskikh, A.A.; Kuchumov, A.G.; Nosov, Y.; Baradina, I. Numerical Study of the Mechanical Behaviour of Wedge-Shaped Defect Filling Materials. Materials 2022, 15, 7387. [Google Scholar] [CrossRef] [PubMed]
- Stanusi, A.; Mercuţ, V.; Scrieciu, M.; Popescu, S.M.; Craitoiu-Iacov, M.M.; Daguci, L.; Castravete, S.; Vintila, D.D.; Vatu, M. Effects of occlusal loads in the genesis of non-carious cervical lesions—A finite element study. Rom. J. Oral Rehabil. 2019, 11, 73–81. [Google Scholar]
- Abdalla, R.; Mitchell, R.J.; Ren, Y. Non-carious cervical lesions imaged by focus variation microscopy. J. Dent. 2017, 63, 14–20. [Google Scholar] [CrossRef]
- Peumans, M.; Politano, G.; Van Meerbeek, B. Treatment of noncarious cervical lesions: When, why, and how. Int. J. Esthet. Dent. 2020, 15, 16–42. [Google Scholar] [PubMed]
- Nascimento, M.; Dilbone, D.; Pereira, P.; Geraldeli, S.; Delgado, A.; Duarte, W. Abfraction lesions: Etiology, diagnosis, and treatment options. Clin. Cosmet. Investig. Dent. 2016, 8, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Aldosari, M.A. Magnification Loupes: An Update of the Evidence. J. Contemp. Dent. Pract. 2021, 22, 310–315. [Google Scholar] [CrossRef]
- Pispero, A.; Marcon, M.; Ghezzi, C.; Massironi, D.; Varoni, E.M.; Tubaro, S.; Lodi, G. Posture Assessment in Dentistry for Different Visual Aids Using 2D Markers. Sensors 2021, 21, 7717. [Google Scholar] [CrossRef]
- Bud, M.; Jitaru, S.; Lucaciu, O.; Korkut, B.; Dumitrascu-Timis, L.; Ionescu, C.; Cimpean, S.; Delean, A. The advantages of the dental operative microscope in restorative dentistry. Med. Pharm. Rep. 2021, 94, 22–27. [Google Scholar] [CrossRef]
- Soares, P.V.; Grippo, J.O. Noncarious Cervical Lesions and Cervical Dentin Hypersensitivity–Etiology, Diagnosis and Treatment; Quintessesnce Publishing: Batavia, IL, USA, 2017. [Google Scholar]
- Stanusi, A.; Ionescu, M.; Cerbulescu, C.; Popescu, S.M.; Osiac, E.; Mercut, R.; Scrieciu, M.; Pascu, R.M.; Stanus, A.S.; Mercut, V. Modifications of the Dental Hard Tissues in the Cervical Area of Occlusally Overloaded Teeth Identified Using Optical Coherence Tomography. Medicina 2022, 58, 702. [Google Scholar] [CrossRef]
- Kitasako, Y.; Ikeda, M.; Takagaki, T.; Burrow, M.F.; Tagami, J. The prevalence of non-carious cervical lesions (NCCLs) with or without erosive etiological factors among adults of different ages in Tokyo. Clin. Oral Investig. 2021, 25, 6939–6947. [Google Scholar] [CrossRef] [PubMed]
- Haak, R.; Hähnel, M.; Schneider, H.; Rosolowski, M.; Park, K.-J.; Ziebolz, D.; Häfer, M. Clinical and OCT outcomes of a universal adhesive in a randomized clinical trial after 12 months. J. Dent. 2019, 90, 103200. [Google Scholar] [CrossRef] [PubMed]
- Sugita, I.; Nakashima, S.; Ikeda, A.; Burrow, M.F.; Nikaido, T.; Kubo, S.; Tagami, J.; Sumi, Y. A pilot study to assess the morphology and progression of non-carious cervical lesions. J. Dent. 2017, 57, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Mercut, V.; Popescu, S.M.; Scrieciu, M.; Amarascu, M.O.; Vatu, M.; Diaconu, O.A. Optical coherence tomography applications in tooth wear diagnosis. Rom. J. Morphol. Embryol. 2017, 58, 99–106. [Google Scholar] [PubMed]
- Surlin, P.; Didilescu, A.C.; Lazar, L.; Arsenie, C.C.; Camen, A.; Popescu, D.M.; Gheorghe, D.N.; Osiac, E.; Rogoveanu, I. Evaluation Through the Optical Coherence Tomography Analysis of the Influence of Non-Alcoholic Fatty Liver Disease on the Gingival Inflammation in Periodontal Patients. Diabetes Metab. Syndr. Obes. 2021, 14, 2935–2942. [Google Scholar] [CrossRef]
- Lim, J.; Lee, W.; Judex, S.; Mahdian, M. Optical Coherence Tomography for the Detection and Characterization of Subgingival Root Caries Lesions and Noncarious Cervical Lesions: A Quantitative Analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, e118–e119. [Google Scholar] [CrossRef]
- Wada, I.; Shimada, Y.; Ikeda, M.; Sadr, A.; Nakashima, S.; Tagami, J.; Sumi, Y. Clinical assessment of non carious cervical lesion using swept-source optical coherence tomography. J. Biophotonics 2015, 8, 846–854. [Google Scholar] [CrossRef]
- Marcauteanu, C.; Stoica, E.; Dorin, B.; Sinescu, C.; Negrutiu, M.L.; Topala, F.; Goguta, L.; Hughes, M.; Bradu, A.; Dobre, G.; et al. Microstructural characterization of non-carious cervical lesions by en face optical coherence tomography. Timis. Med. J. 2010, 60, 60–63. [Google Scholar]
- Smith, B.G.; Knight, J.K. An index for measuring the wear of teeth. Br. Dent. J. 1984, 156, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Osiac, E.; Bălşeanu, T.A.; Mogoantă, L.; Gheonea, D.I.; Pirici, I.; Iancău, M. Optical coherence tomography investigation of ischemic stroke inside a rodent model. Rom. J. Morphol. Embryol. 2014, 55, 767–772. [Google Scholar]
- Osiac, E.; Săftoiu, A.; Gheonea, D.I.; Mandrila, I.; Angelescu, R. Optical coherence tomography and Doppler optical coherence tomography in the gastrointestinal tract. World J. Gastroenterol. 2011, 17, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, B.L.; Vieira, A.R.; Bezamat, M.; Ignácio, S.A.; Souza, E.M. Occlusal problems, mental health issues and non-carious cervical lesions. Odontology 2022, 110, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.; Nguyen, D.H.; Lee, S.; Heo, S.M.; Park, J. Simulation of Non-Carious Cervical Lesions by Computational Toothbrush Model: A Novel Three-Dimensional Discrete Element Method. Sensors 2022, 22, 4183. [Google Scholar] [CrossRef]
- Huang, X.; She, L.; Liu, H.; Liu, P.; Chen, J.; Chen, Y.; Zhou, W.; Lu, Y.; Lin, J. Study of oral microorganisms contributing to non-carious cervical lesions via bacterial interaction and pH regulation. J. Cell. Mol. Med. 2021, 25, 3103–3112. [Google Scholar] [CrossRef]
- Nassar, H.M.; Hara, A.T. Effect of dentifrice slurry abrasivity and erosive challenge on simulated non-carious cervical lesions development in vitro. J. Oral Sci. 2021, 63, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, D.F.M.; Shinohara, M.S.; Carvalho, P.R.M.A.; Ramos, F.S.E.S.; Oliveira, L.C.; Omoto, É.M.; Fagundes, T.C. Three-year evaluation of different adhesion strategies in non-carious cervical lesion restorations: A randomized clinical trial. J. Appl. Oral Sci. 2021, 29, e20210192. [Google Scholar] [CrossRef]
- Schwendicke, F.; Müller, A.; Seifert, T.; Jeggle-Engbert, L.M.; Paris, S.; Göstemeyer, G. Glass hybrid versus composite for non-carious cervical lesions: Survival, restoration quality and costs in randomized controlled trial after 3 years. J. Dent. 2021, 110, 103689. [Google Scholar] [CrossRef]
- Cairo, F.; Cortellini, P.; Nieri, M.; Pilloni, A.; Barbato, L.; Pagavino, G.; Tonetti, M. Coronally advanced flap and composite restoration of the enamel with or without connective tissue graft for the treatment of single maxillary gingival recession with non-carious cervical lesion. A randomized controlled clinical trial. J. Clin. Periodontol. 2020, 47, 362–371. [Google Scholar] [CrossRef]
- Medeiros, T.L.M.; Mutran, S.C.A.N.; Espinosa, D.G.; do Carmo Freitas Faial, K.; Pinheiro, H.H.C. Prevalence and risk indicators of non-carious cervicl lesions in male footballers. BMC Oral Health 2020, 20, 215. [Google Scholar] [CrossRef]
- Zuza, A.; Racic, M.; Ivkovic, N.; Krunic, J.; Stojanovic, N.; Bozovic, D. Prevalence of non-carious cervical lesions among the general population of the Republic of Srpska, Bosnia and Herzegovina. Int. Dent. J. 2019, 69, 281–288. [Google Scholar] [CrossRef]
- Yan, W.; Yang, D. The Prevalence, characteristics and risk factors in non-carious cervical lesion: A survey on 295 people in Guangzhou Area. J. Oral Hyg. Health 2014, 2, 125. [Google Scholar]
- Caneppele, T.M.F.; Meirelles, L.C.F.; Rocha, R.S.; Gonçalves, L.L.; Ávila, D.M.S.; Gonçalves, S.E. de P.; Bresciani, E. A 2-year clinical evaluation of direct and semi-direct resin composite restorations in non-carious cervical lesions: A randomized clinical study. Clin. Oral Investig. 2020, 24, 1321–1331. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Rong, Q.; Luan, Q.; Yu, X. Effect of partial restorative treatment on stress distributions in non-carious cervical lesions: A three-dimensional finite element analysis. BMC Oral Health. 2022, 22, 607. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Kubo, S.; Pereira, P.N.R.; Ikeda, M.; Takagaki, T.; Nikaido, T.; Tagami, J. Progression of non-carious cervical lesions: 3D morphological analysis. Clin Oral Investig. 2022, 26, 575–583. [Google Scholar] [CrossRef]
- Michael, J.A.; Kaidonis, J.A.; Townsend, G.C. Non-carious cervical lesions on permanent anterior teeth: A new mrhological classification. Aust. Dent. J. 2010, 55, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Giachetti, L. A Simple Method for Treating Subgingival Class V Lesions. Oper. Dent. 2018, 44, 333–335. [Google Scholar] [CrossRef] [PubMed]
- Haripriya, S.; Ajitha, P. Importance of isolation in restoring non-carious cervical lesions. J. Adv. Pharm. Educ. Res. 2017, 7, 283–286. [Google Scholar]
- Loomba, K.; Bains, R.; Bains, V.K.; Loomba, A. Proposal for clinical classification of multifactorial noncarious cervical lesions. Gen. Dent. 2014, 62, 39–44. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | No. NCCL/Tooth | Tooth with NCCL | Surface with NCCL | Anatomical Location of NCCL | NCCL Shape | NCCL Depth |
|---|---|---|---|---|---|---|
| 1 | 2 | I6 | Buccal | Crown and root | Wedge shaped | <1 mm |
| Oral | Crown and root | Wedge shaped | <1 mm | |||
| 2 | 1 | I7 | Buccal | Crown and root | Wedge shaped | >2 mm |
| 3 | 1 | I8 | Buccal | Crown and root | Wedge shaped | <1 mm |
| 4 | 1 | I9 | Buccal | Crown and root | Wedge shaped | >2 mm |
| 5 | 1 | I13 | Buccal | Root | Saucer shaped | 1 mm |
| 6 | 1 | I14 | Buccal | Crown and root | Saucer shaped | <1 mm |
| 7 | 1 | I15 | Buccal | Root | Wedge shaped | 2 mm |
| 8 | 1 | I17 | Buccal | Crown and root | Saucer shaped | <1 mm |
| 9 | 1 | I23 | Oral | Crown and root | Wedge shaped | <1 mm |
| 10 | 1 | I25 | Buccal | Root | Saucer shaped | <1 mm |
| 11 | 1 | PM7 | Buccal | Crown | Wedge shaped | <1 mm |
| 12 | 1 | PM8 | Buccal | Crown and root | Wedge shaped | <1 mm |
| 13 | 2 | PM9 | Buccal | Crown | Wedge shaped | <1 mm |
| Oral | Crown | Wedge shaped | <1 mm | |||
| 14 | 1 | PM10 | Oral | Root | Wedge shaped | <1 mm |
| 15 | 1 | PM11 | Buccal | Crown and root | Wedge shaped | <1 mm |
| 16 | 1 | PM13 | Buccal | Root | Wedge shaped | >2 mm |
| 17 | PM15 | Buccal | Root | Saucer shaped | <1 mm | |
| 3 | PM15 | Oral | Root | Saucer shaped | <1 mm | |
| PM15 | Distal | Root | Saucer shaped | <1 mm | ||
| 18 | 1 | PM16 | Oral | Root | Wedge shaped | <1 mm |
| 19 | 1 | PM17 | Buccal | Crown and root | Wedge shaped | <1 mm |
| 20 | 2 | PM19 | Buccal | Root | Wedge shaped | <1 mm |
| PM19 | Oral | Root | Wedge shaped | <1 mm | ||
| 21 | 2 | PM20 | Buccal | Root | Saucer shaped | <1 mm |
| PM20 | Mesial | Root | Saucer shaped | <1 mm |
| No. | No. NCCL/Tooth | Tooth with NCCL | Surface with NCCL | Anatomical Location of NCCL | NCCL Shape | NCCL Depth |
|---|---|---|---|---|---|---|
| 1 | 1 | I18 | Mesial | Root | Saucer shaped | <1 mm |
| 2 | 1 | I24 | Distal | Root | Saucer shaped | <1 mm |
| 3 | 1 | I27 | Buccal | Root | Irregular | 1–2 mm |
| 4 | 2 | PM6 | Buccal | Crown and root | Wedge shaped | <1 mm |
| PM6 | Mesial | Root | Wedge shaped | <1 mm | ||
| 5 | 1 | PM14 | Distal | Root | Saucer shaped | 1–2 mm |
| 6 | 1 | PM24 | Buccal | Root | Saucer shaped | <1 mm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stănuşi, A.; Iacov-Crăițoiu, M.M.; Scrieciu, M.; Mitruț, I.; Firulescu, B.C.; Boțilă, M.R.; Vlăduțu, D.E.; Stănuşi, A.Ş.; Mercuț, V.; Osiac, E. Morphological and Optical Coherence Tomography Aspects of Non-Carious Cervical Lesions. J. Pers. Med. 2023, 13, 772. https://doi.org/10.3390/jpm13050772
Stănuşi A, Iacov-Crăițoiu MM, Scrieciu M, Mitruț I, Firulescu BC, Boțilă MR, Vlăduțu DE, Stănuşi AŞ, Mercuț V, Osiac E. Morphological and Optical Coherence Tomography Aspects of Non-Carious Cervical Lesions. Journal of Personalized Medicine. 2023; 13(5):772. https://doi.org/10.3390/jpm13050772
Chicago/Turabian StyleStănuşi, Andreea, Monica Mihaela Iacov-Crăițoiu, Monica Scrieciu, Ioana Mitruț, Bogdan Costin Firulescu, Mihaela Roxana Boțilă, Diana Elena Vlăduțu, Adrian Ştefan Stănuşi, Veronica Mercuț, and Eugen Osiac. 2023. "Morphological and Optical Coherence Tomography Aspects of Non-Carious Cervical Lesions" Journal of Personalized Medicine 13, no. 5: 772. https://doi.org/10.3390/jpm13050772
APA StyleStănuşi, A., Iacov-Crăițoiu, M. M., Scrieciu, M., Mitruț, I., Firulescu, B. C., Boțilă, M. R., Vlăduțu, D. E., Stănuşi, A. Ş., Mercuț, V., & Osiac, E. (2023). Morphological and Optical Coherence Tomography Aspects of Non-Carious Cervical Lesions. Journal of Personalized Medicine, 13(5), 772. https://doi.org/10.3390/jpm13050772