

Histopathological Clues of Enhanced Inflammation in the Placental Tissue of Women with Chronic Venous Disease in Lower Limbs during Pregnancy
 , ,
, , 
 , , ,
, , ,  ,
,  and
and 
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design and Participants
2.2. Sample Processing
2.3. Gene Analysis through Real-Time Quantitative PCR (RT-qPCR)
2.4. Immunohistochemical Analysis
2.5. Histopathological Examination
2.6. Statistical Analysis
3. Results
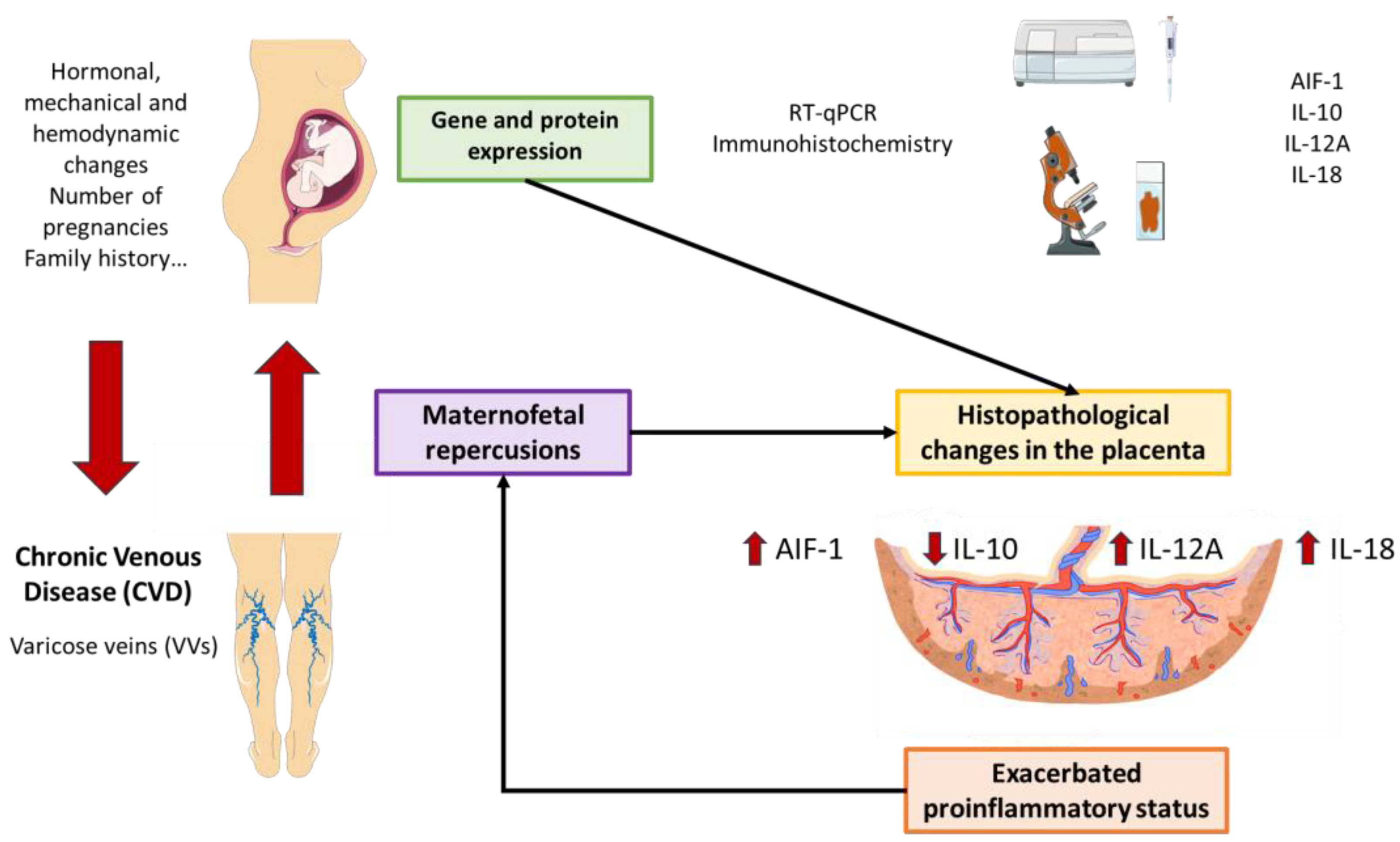
3.1. The Placenta of Women with CVD Exhibits Increased Expression of Proinflammatory Markers AIF-1, IL-12A, and IL-18
3.2. The Placental Tissue of Women with CVD Shows a Decreased Expression of IL-10
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ligi, D.; Croce, L.; Mannello, F. Chronic Venous Disorders: The Dangerous, the Good, and the Diverse. Int. J. Mol. Sci. 2018, 19, 2544. [Google Scholar] [CrossRef] [PubMed]
- Raju, S.; Knight, A.; Lamanilao, L.; Pace, N.; Jones, T. Peripheral Venous Hypertension in Chronic Venous Disease. J. Vasc. Surg. Venous Lymphat. Disord. 2019, 7, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Smetanina, M.A.; Shevela, A.I.; Gavrilov, K.A.; Filipenko, M.L. The Genetic Constituent of Varicose Vein Pathogenesis as a Key for Future Treatment Option Development. Vessel Plus 2021, 5, 2544. [Google Scholar] [CrossRef]
- Raffetto, J.D.; Mannello, F. Pathophysiology of Chronic Venous Disease. Int. Angiol. 2014, 33, 212–221. [Google Scholar] [PubMed]
- Ortega, M.A.; Fraile-Martínez, O.; García-Montero, C.; Álvarez-Mon, M.A.; Chaowen, C.; Ruiz-Grande, F.; Pekarek, L.; Monserrat, J.; Asúnsolo, A.; García-Honduvilla, N.; et al. Understanding Chronic Venous Disease: A Critical Overview of Its Pathophysiology and Medical Management. J. Clin. Med. 2021, 10, 3239. [Google Scholar] [CrossRef]
- Taylor, J.; Hicks, C.W.; Heller, J.A. The Hemodynamic Effects of Pregnancy on the Lower Extremity Venous System. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Lohr, J.M.; Bush, R.L. Venous Disease in Women: Epidemiology, Manifestations, and Treatment. J. Vasc. Surg. 2013, 57, 37S–45S. [Google Scholar] [CrossRef] [PubMed]
- Cornu-Thenard, A.; Boivin, P. Chronic Venous Disease during Pregnancy—Servier—PhlebolymphologyServier—Phlebolymphology. Phlebolymphology 2014, 21, 138–145. [Google Scholar]
- García-Montero, C.; Fraile-Martinez, O.; Rodriguez-Martín, S.; Funes Moñux, R.M.; Saz, J.V.; Bravo, C.; De Leon-Luis, J.A.; Ruiz-Minaya, M.; Pekarek, L.; Saez, M.A.; et al. Irregular Expression of Cellular Stress Response Markers in the Placenta of Women with Chronic Venous Disease. Antioxidants 2022, 11, 2277. [Google Scholar] [CrossRef]
- Ortega, M.A.; Sánchez-Trujillo, L.; Bravo, C.; Fraile-Martinez, O.; García-Montero, C.; Saez, M.A.; Alvarez-Mon, M.A.; Sainz, F.; Alvarez-Mon, M.; Bujan, J.; et al. Newborns of Mothers with Venous Disease during Pregnancy Show Increased Levels of Lipid Peroxidation and Markers of Oxidative Stress and Hypoxia in the Umbilical Cord. Antioxidants 2021, 10, 980. [Google Scholar] [CrossRef]
- Sikora, M.; Kopeć, B.; Piotrowska, K.; Pawlik, A. Role of Allograft Inflammatory Factor-1 in Pathogenesis of Diseases. Immunol. Lett. 2020, 218, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Leon-Oliva, D.; Garcia, D.; De Leon-Oliva, D.; Garcia-Montero, C.; Fraile-Martinez, O.; Liviu Boaru, D.; García-Puente, L.; Rios-Parra, A.; Garrido-Gil, M.J.; Casanova-Martín, C.; et al. AIF1: Function and Connection with Inflammatory Diseases. Biology 2023, 12, 694. [Google Scholar] [CrossRef]
- Zhao, Y.Y.; Yan, D.J.; Chen, Z.W. Role of AIF-1 in the Regulation of Inflammatory Activation and Diverse Disease Processes. Cell. Immunol. 2013, 284, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Trujillo, L.; Fraile-Martinez, O.; García-Montero, C.; García-Puente, L.M.; Guijarro, L.G.; De Leon-Oliva, D.; Boaru, D.L.; Gardón-Alburquerque, D.; del Val Toledo Lobo, M.; Royuela, M.; et al. Chronic Venous Disease during Pregnancy Is Related to Inflammation of the Umbilical Cord: Role of Allograft Inflammatory Factor 1 (AIF-1) and Interleukins 10 (IL-10), IL-12 and IL-18. J. Pers. Med. 2023, 13, 956. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Gómez-Lahoz, A.M.; Sánchez-Trujillo, L.; Fraile-Martinez, O.; García-Montero, C.; Guijarro, L.G.; Bravo, C.; De Leon-Luis, J.A.; Saz, J.V.; Bujan, J.; et al. Chronic Venous Disease during Pregnancy Causes a Systematic Increase in Maternal and Fetal Proinflammatory Markers. Int. J. Mol. Sci. 2022, 23, 8976. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Fraile-Martínez, O.; Saez, M.A.; Álvarez-Mon, M.A.; Gómez-Lahoz, A.M.; Bravo, C.; De León Luis, J.A.; Sainz, F.; Coca, S.; Asúnsolo, Á.; et al. Abnormal Proinflammatory and Stressor Environmental with Increased the Regulatory Cellular IGF-1/PAPP-A/STC and Wnt-1/β-Catenin Canonical Pathway in Placenta of Women with Chronic Venous Disease during Pregnancy. Int. J. Med. Sci. 2021, 18, 2814–2827. [Google Scholar] [CrossRef] [PubMed]
- Lurie, F.; Passman, M.; Meisner, M.; Dalsing, M.; Masuda, E.; Welch, H.; Bush, R.L.; Blebea, J.; Carpentier, P.H.; De Maeseneer, M.; et al. The 2020 Update of the CEAP Classification System and Reporting Standards. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 342–352. [Google Scholar] [CrossRef]
- Chomczynski, P.; Sacchi, N. The Single-Step Method of RNA Isolation by Acid Guanidinium Thiocyanate–Phenol–Chloroform Extraction: Twenty-Something Years On. Nat. Protoc. 2006, 1, 581–585. [Google Scholar] [CrossRef]
- Ye, J.; Coulouris, G.; Zaretskaya, I.; Cutcutache, I.; Rozen, S.; Madden, T.L. Primer-BLAST: A Tool to Design Target-Specific Primers for Polymerase Chain Reaction. BMC Bioinform. 2012, 13, 134. [Google Scholar] [CrossRef]
- Vallone, P.M.; Butler, J.M. AutoDimer: A Screening Tool for Primer-Dimer and Hairpin Structures. Biotechniques 2004, 37, 226–231. [Google Scholar] [CrossRef]
- Jang, S.J.; Jeon, R.H.; Kim, H.D.; Hwang, J.C.; Lee, H.J.; Bae, S.G.; Lee, S.L.; Rho, G.J.; Kim, S.J.; Lee, W.J. TATA Box Binding Protein and Ribosomal Protein 4 Are Suitable Reference Genes for Normalization during Quantitative Polymerase Chain Reaction Study in Bovine Mesenchymal Stem Cells. Asian-Australas. J. Anim. Sci. 2020, 33, 2021. [Google Scholar] [CrossRef]
- Gatto, F.; Feelders, R.A.; Van Der Pas, R.; Kros, J.M.; Waaijers, M.; Sprij-Mooij, D.; Neggers, S.J.C.M.M.; Van Der Lelij, A.J.; Minuto, F.; Lamberts, S.W.J.; et al. Immunoreactivity Score Using an Anti-Sst2A Receptor Monoclonal Antibody Strongly Predicts the Biochemical Response to Adjuvant Treatment with Somatostatin Analogs in Acromegaly. J. Clin. Endocrinol. Metab. 2013, 98, E66–E71. [Google Scholar] [CrossRef]
- Kotulak-Chrzaszcz, A.; Kiezun, J.; Czajkowski, M.; Matuszewski, M.; Klacz, J.; Krazinski, B.E.; Godlewski, J.; Kmiec, Z.; Wierzbicki, P.M. The Immunoreactivity of GLI1 and VEGFA Is a Potential Prognostic Factor in Kidney Renal Clear Cell Carcinoma. BMC Cancer 2023, 23, 1110. [Google Scholar] [CrossRef] [PubMed]
- Ives, C.W.; Sinkey, R.; Rajapreyar, I.; Tita, A.T.N.; Oparil, S. Preeclampsia-Pathophysiology and Clinical Presentations: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 1690–1702. [Google Scholar] [CrossRef] [PubMed]
- Heerema-McKenney, A. Defense and Infection of the Human Placenta. APMIS 2018, 126, 570–588. [Google Scholar] [CrossRef] [PubMed]
- Yockey, L.J.; Iwasaki, A. Interferons and Proinflammatory Cytokines in Pregnancy and Fetal Development. Immunity 2018, 49, 397–412. [Google Scholar] [CrossRef]
- Aggarwal, R.; Jain, A.K.; Mittal, P.; Kohli, M.; Jawanjal, P.; Rath, G. Association of Pro- and Anti-Inflammatory Cytokines in Preeclampsia. J. Clin. Lab. Anal. 2019, 33, e22834. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Cardenas, I.; Abrahams, V.; Guller, S. Inflammation and Pregnancy: The Role of the Immune System at the Implantation Site. Ann. N. Y. Acad. Sci. 2011, 1221, 80–87. [Google Scholar] [CrossRef]
- Ortega, M.A.; Fraile-Martínez, O.; García-Montero, C.; Sáez, M.A.; Álvarez-Mon, M.A.; Torres-Carranza, D.; Álvarez-Mon, M.; Bujan, J.; García-Honduvilla, N.; Bravo, C.; et al. The Pivotal Role of the Placenta in Normal and Pathological Pregnancies: A Focus on Preeclampsia, Fetal Growth Restriction, and Maternal Chronic Venous Disease. Cells 2022, 11, 568. [Google Scholar] [CrossRef]
- Grudzinska, E.; Lekstan, A.; Szliszka, E.; Czuba, Z.P. Cytokines Produced by Lymphocytes in the Incompetent Great Saphenous Vein. Mediat. Inflamm. 2018, 2018, 7161346. [Google Scholar] [CrossRef]
- García-Honduvilla, N.; Asúnsolo, Á.; Ortega, M.A.; Sainz, F.; Leal, J.; Lopez-Hervas, P.; Pascual, G.; Buján, J. Increase and Redistribution of Sex Hormone Receptors in Premenopausal Women Are Associated with Varicose Vein Remodelling. Oxid. Med. Cell. Longev. 2018, 2018, 3974026. [Google Scholar] [CrossRef] [PubMed]
- Kadoya, M.; Yamamoto, A.; Hamaguchi, M.; Obayashi, H.; Mizushima, K.; Ohta, M.; Seno, T.; Oda, R.; Fujiwara, H.; Kohno, M.; et al. Allograft Inflammatory Factor-1 Stimulates Chemokine Production and Induces Chemotaxis in Human Peripheral Blood Mononuclear Cells. Biochem. Biophys. Res. Commun. 2014, 448, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Iyer, S.S.; Cheng, G. Role of Interleukin 10 Transcriptional Regulation in Inflammation and Autoimmune Disease. Crit. Rev. Immunol. 2012, 32, 23–63. [Google Scholar] [CrossRef] [PubMed]
- Hanna, N.; Hanna, I.; Hleb, M.; Wagner, E.; Dougherty, J.; Balkundi, D.; Padbury, J.; Sharma, S. Gestational Age-Dependent Expression of IL-10 and Its Receptor in Human Placental Tissues and Isolated Cytotrophoblasts. J. Immunol. 2000, 164, 5721–5728. [Google Scholar] [CrossRef]
- Cheng, S.B.; Sharma, S. Interleukin-10: A Pleiotropic Regulator in Pregnancy. Am. J. Reprod. Immunol. 2015, 73, 487–500. [Google Scholar] [CrossRef]
- Obut, M.; Oğlak, S.C. Expression of CD44 and IL-10 in Normotensive and Preeclamptic Placental Tissue. Ginekol. Pol. 2020, 91, 334–341. [Google Scholar] [CrossRef]
- Wang, H.; Wang, L.L.; Zhao, S.J.; Lin, X.X.; Liao, A.H. IL-10: A Bridge between Immune Cells and Metabolism during Pregnancy. J. Reprod. Immunol. 2022, 154, 103750. [Google Scholar] [CrossRef]
- Ketut Suwiyoga, I.; Nyoman, I.; Astawa, M.; Jawi, M.; Wayan, I.; Putra, A. Low Expression of Calcitriol Level and Interleukin-10 and Hypoxia-Inducible Factor-1 Alpha Expression on Placenta. Open Access Maced. J. Med. Sci. 2023, 11, 599–607. [Google Scholar] [CrossRef]
- Lai, Z.; Kalkunte, S.; Sharma, S. A Critical Role of Interleukin-10 in Modulating Hypoxia-Induced Preeclampsia-Like Disease in Mice. Hypertension 2011, 57, 505–514. [Google Scholar] [CrossRef]
- Santana-Garrido, Á.; Reyes-Goya, C.; Espinosa-Martín, P.; Sobrevia, L.; Beltrán, L.M.; Vázquez, C.M.; Mate, A. Oxidative and Inflammatory Imbalance in Placenta and Kidney of SFlt1-Induced Early-Onset Preeclampsia Rat Model. Antioxidants 2022, 11, 1608. [Google Scholar] [CrossRef]
- Roth, I.; Fisher, S.J. IL-10 Is an Autocrine Inhibitor of Human Placental Cytotrophoblast MMP-9 Production and Invasion. Dev. Biol. 1999, 205, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, P.; Behzadi, E.; Ranjbar, R. Il-12 Family Cytokines: General Characteristics, Pathogenic Microorganisms, Receptors, and Signalling Pathways. Acta Microbiol. Immunol. Hung. 2016, 63, 1–25. [Google Scholar] [CrossRef]
- Kaplanski, G. Interleukin-18: Biological Properties and Role in Disease Pathogenesis. Immunol. Rev. 2018, 281, 138–153. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, K.; Nakanishi, K.; Tsutsui, H. Interleukin-18 in Health and Disease. Int. J. Mol. Sci. 2019, 20, 649. [Google Scholar] [CrossRef] [PubMed]
- Zourbas, S.; Dubanchet, S.; Martal, J.; Chaouat, G. Localization of Pro-Inflammatory (IL-12, IL-15) and Anti-Inflammatory (IL-11, IL-13) Cytokines at the Foetomaternal Interface during Murine Pregnancy. Clin. Exp. Immunol. 2001, 126, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Amash, A.; Huleihel, M.; Eyal, S.; Maor, E.; Myatt, L.; Holcberg, G. The Expression of Interleukin-15 and Interleukin-18 by Human Term Placenta Is Not Affected by Lipopolysaccharide. Eur. Cytokine Netw. 2007, 18, 188–194. [Google Scholar] [CrossRef]
- Löb, S.; Ochmann, B.; Ma, Z.; Vilsmaier, T.; Kuhn, C.; Schmoeckel, E.; Herbert, S.L.; Kolben, T.; Wöckel, A.; Mahner, S.; et al. The Role of Interleukin-18 in Recurrent Early Pregnancy Loss. J. Reprod. Immunol. 2021, 148, 103432. [Google Scholar] [CrossRef]
- Huang, X.; Huang, H.; Dong, M.; Yao, Q.; Wang, H. Serum and Placental Interleukin-18 Are Elevated in Preeclampsia. J. Reprod. Immunol. 2005, 65, 77–87. [Google Scholar] [CrossRef]
- Benyo, D.F.; Smarason, A.; Redman, C.W.G.; Sims, C.; Conrad, K.P. Expression of Inflammatory Cytokines in Placentas from Women with Preeclampsia. J. Clin. Endocrinol. Metab. 2001, 86, 2505–2512. [Google Scholar] [CrossRef]
- Alfian, I.; Chakraborty, A.; Yong, H.E.J.; Saini, S.; Lau, R.W.K.; Kalionis, B.; Dimitriadis, E.; Alfaidy, N.; Ricardo, S.D.; Samuel, C.S.; et al. The Placental NLRP3 Inflammasome and Its Downstream Targets, Caspase-1 and Interleukin-6, Are Increased in Human Fetal Growth Restriction: Implications for Aberrant Inflammation-Induced Trophoblast Dysfunction. Cells 2022, 11, 1413. [Google Scholar] [CrossRef]
- Wu, W.; Tan, Q.-Y.; Xi, F.-F.; Ruan, Y.; Wang, J.; Luo, Q.; Dou, X.-B.; Hu, T.-X. NLRP3 Inflammasome Activation in Gestational Diabetes Mellitus Placentas Is Associated with Hydrogen Sulfide Synthetase Deficiency. Exp. Ther. Med. 2022, 23, 94. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CVD (n = 62) | HC (n = 52) | |
|---|---|---|
| Median age (IQR), years | 33 (22–40) | 34 (27–41) |
| Median gestational age (IQR), weeks | 40.5 (39–41.5) | 41 (39–42) |
| C-section delivery, n (%) | 12 (19.4) | 9 (17.3) |
| Delivery via vagina, n (%) | 50 (80.6) | 43 (82.7) |
| CVD (CEAP), n (%) | ||
| CEAP 1 | 37 (59.7) | 0 (0) |
| CEAP 2 | 21 (33.8) | 0 (0) |
| CEAP 3 | 4 (6.5) | 0 (0) |
| Prior pregnancies, n (%) | 33 (53.2) | 19 (36.5) |
| Prior abortions, n (%) | 14 (22.6) | 9 (17.3) |
| Regular periods of menstruation, n (%) | 50 (80.6) | 42 (80.7) |
| Profession of inactivity, n (%) | 41 (66.1) | 40 (76.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Gil, M.A.; Fraile-Martinez, O.; García-Montero, C.; Toledo, M.D.V.; Guijarro, L.G.; De León-Luis, J.A.; Bravo, C.; Díaz-Pedrero, R.; López-Gonzalez, L.; Saez, M.A.; et al. Histopathological Clues of Enhanced Inflammation in the Placental Tissue of Women with Chronic Venous Disease in Lower Limbs during Pregnancy. J. Pers. Med. 2024, 14, 87. https://doi.org/10.3390/jpm14010087
Sánchez-Gil MA, Fraile-Martinez O, García-Montero C, Toledo MDV, Guijarro LG, De León-Luis JA, Bravo C, Díaz-Pedrero R, López-Gonzalez L, Saez MA, et al. Histopathological Clues of Enhanced Inflammation in the Placental Tissue of Women with Chronic Venous Disease in Lower Limbs during Pregnancy. Journal of Personalized Medicine. 2024; 14(1):87. https://doi.org/10.3390/jpm14010087
Chicago/Turabian StyleSánchez-Gil, María Asunción, Oscar Fraile-Martinez, Cielo García-Montero, María Del Val Toledo, Luis G. Guijarro, Juan A. De León-Luis, Coral Bravo, Raúl Díaz-Pedrero, Laura López-Gonzalez, Miguel A. Saez, and et al. 2024. "Histopathological Clues of Enhanced Inflammation in the Placental Tissue of Women with Chronic Venous Disease in Lower Limbs during Pregnancy" Journal of Personalized Medicine 14, no. 1: 87. https://doi.org/10.3390/jpm14010087
APA StyleSánchez-Gil, M. A., Fraile-Martinez, O., García-Montero, C., Toledo, M. D. V., Guijarro, L. G., De León-Luis, J. A., Bravo, C., Díaz-Pedrero, R., López-Gonzalez, L., Saez, M. A., Álvarez-Mon, M., García-Honduvilla, N., & Ortega, M. A. (2024). Histopathological Clues of Enhanced Inflammation in the Placental Tissue of Women with Chronic Venous Disease in Lower Limbs during Pregnancy. Journal of Personalized Medicine, 14(1), 87. https://doi.org/10.3390/jpm14010087