

Factors Positively Correlated with Hepatitis B Surface Antigen Seroconversion in Chronic Hepatitis B

 ,
,  and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Information and Ethical Considerations
2.2. Data Collection, Laboratory Parameters, Antiviral Therapy and Definition of Seroconversion
2.3. Statistical Analysis
3. Results
3.1. Demographic and Laboratory Data
3.2. HCC Incidence, Liver Elastography and CAP
3.3. Antiviral Therapy
3.4. Factors Associated with Seroconversion
3.4.1. Antiviral Therapy
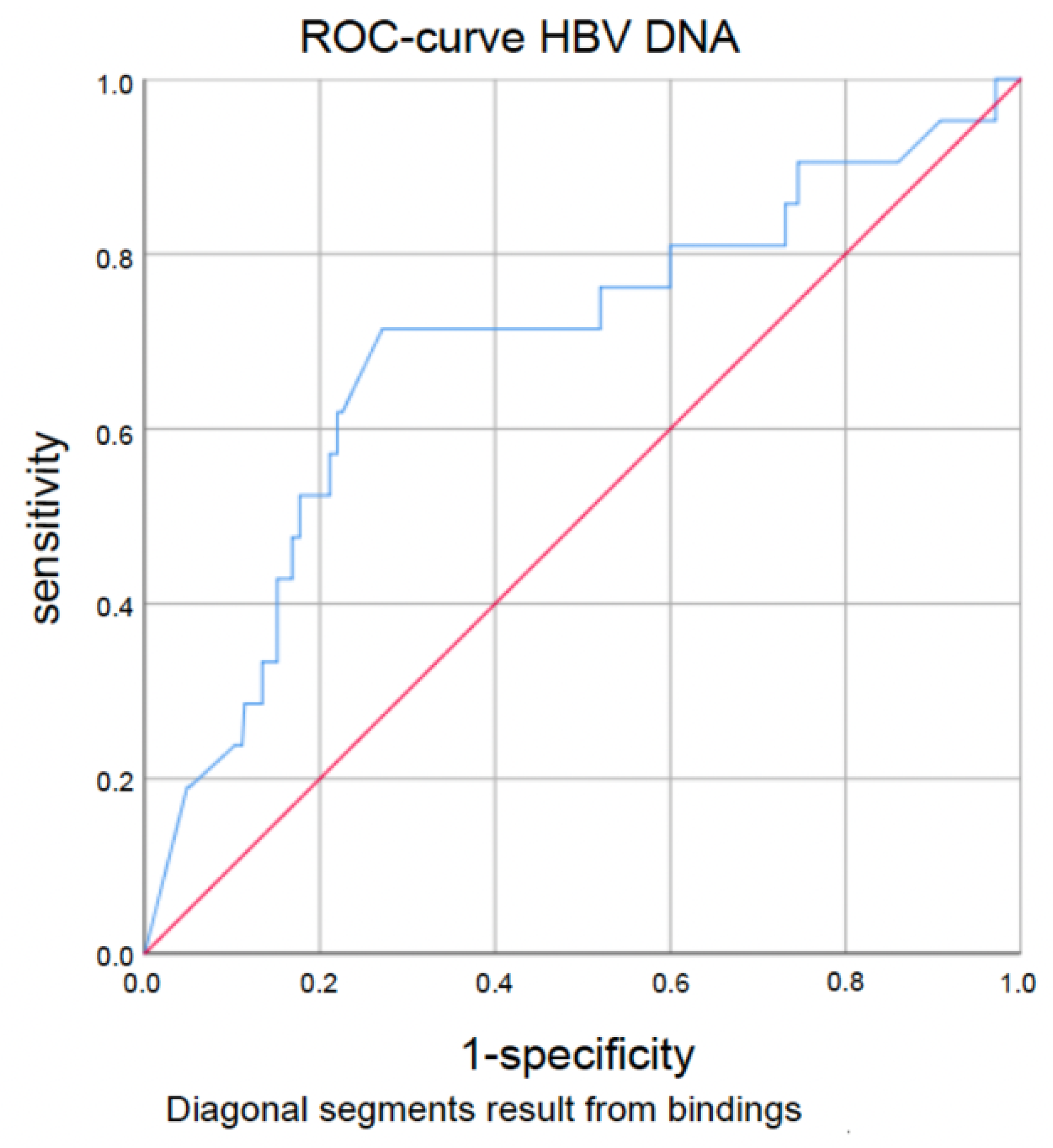
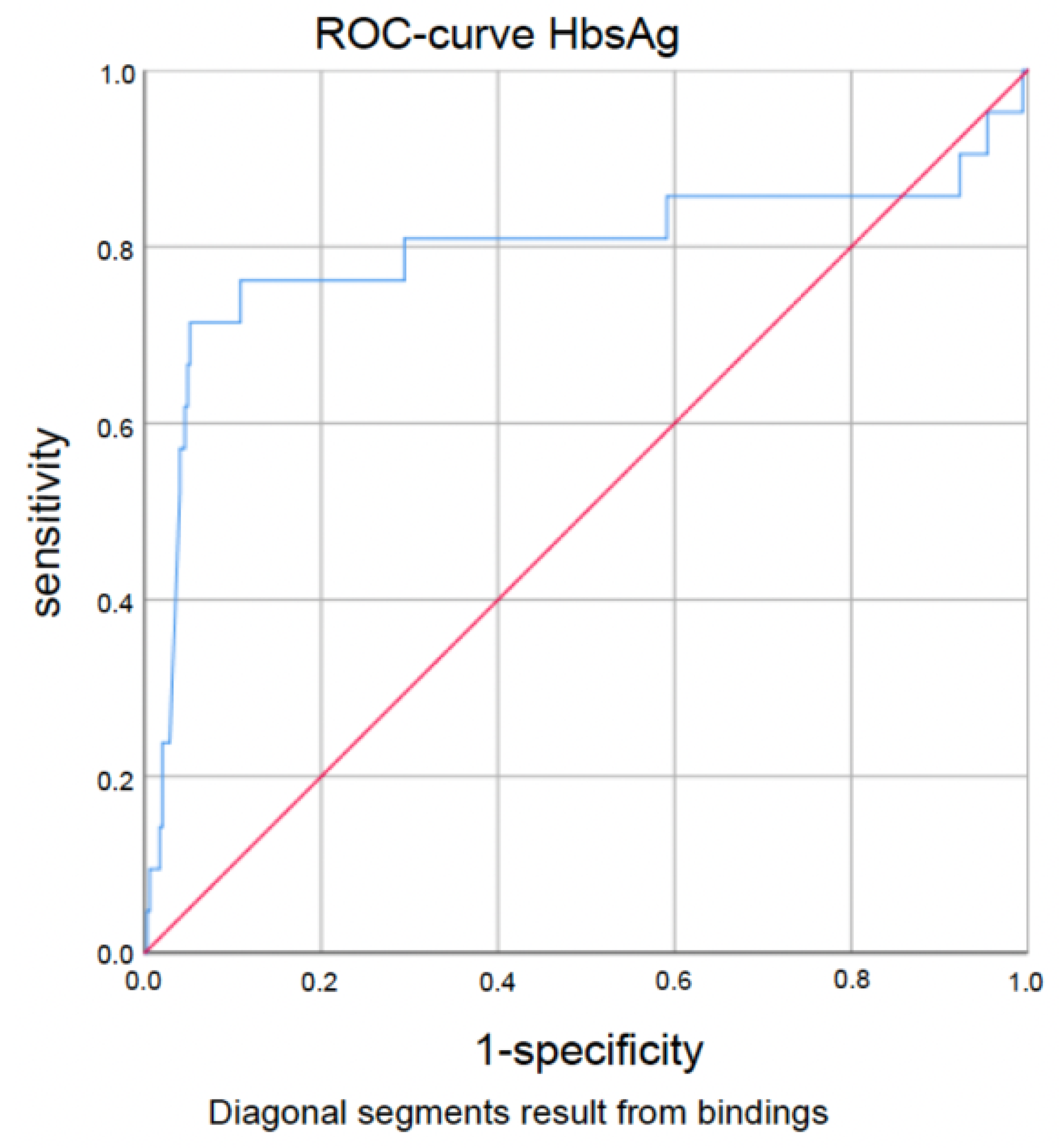
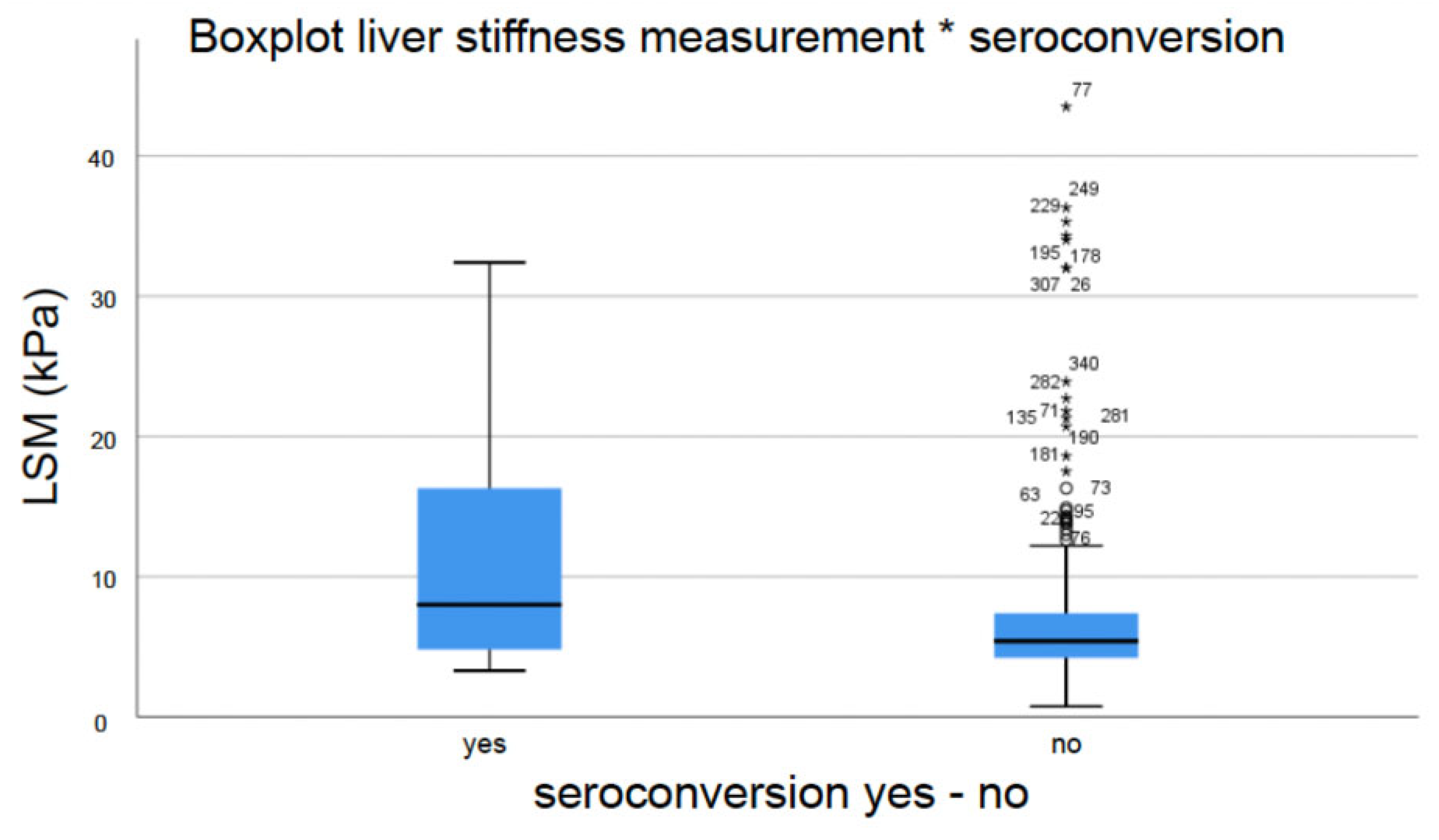
3.4.2. HBV-Specific and Liver-Specific Laboratory Parameters and Liver Fibrosis Measured by Transient Elastography (TE)
3.4.3. Steatosis, Lipid Metabolism, Diabetes Mellitus and Obesity Were Not Associated with Seroconversion
3.4.4. Gender, GGT and Antiviral Therapy Were Independently Associated with Seroconversion
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Dudareva, S.; Faber, M.; Zimmermann, R.; Bock, C.T.; Offergeld, R.; Steffen, G.; Enkelmann, J. Epidemiology of viral hepatitis A to E in Germany. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2022, 65, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Ligat, G.; Schuster, C.; Baumert, T.F. Hepatitis B Virus Core Variants, Liver Fibrosis, and Hepatocellular Carcinoma. Hepatol. Baltim. Md. 2019, 69, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Ott, J.; Stevens, G.; Groeger, J.; Wiersma, S. Global epidemiology of hepatitis B virus infection: New estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine 2012, 30, 2212–2219. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet Lond Engl. 2015, 386, 1546–1555. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.-W.; Shi, Y.-M.; Chu, F.; Liu, J.; Shi, C.; Xu, J.-J.; Liu, P.; Bai, Y.-J.; Xiao, X.-H.; Zhang, X.-C.; et al. Prediction for HBsAg seroconversion in children with chronic hepatitis B. BMC Infect. Dis. 2021, 21, 1211. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.; Chakraborty, A.; Chou, W.-M.; Hasreiter, J.; Wettengel, J.M.; Stadler, D.; Bester, R.; Asen, T.; Zhang, K.; Wisskirchen, K.; et al. Hepatitis B virus genome recycling and de novo secondary infection events maintain stable cccDNA levels. J. Hepatol. 2018, 69, 1231–1241. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liao, H.; Deng, Z.; Liu, Y.; Bian, D.; Ren, Y.; Yu, G.; Jiang, Y.; Bai, L.; Liu, S.; et al. Serum HBV RNA predicts HBeAg clearance and seroconversion in patients with chronic hepatitis B treated with nucleos(t)ide analogues. J. Viral Hepat. 2022, 29, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Wang, J.; Chen, X.; Xu, D.; Xia, N. Potential use of serum HBV RNA in antiviral therapy for chronic hepatitis B in the era of nucleos(t)ide analogs. Front. Med. 2017, 11, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Zhang, X.-X.; Cao, L.-H.; Tan, N.; Kang, Q.; Xi, H.-L.; Yu, M.; Xu, X.-Y. Serum hepatitis B virus RNA is a predictor of HBeAg seroconversion and virological response with entecavir treatment in chronic hepatitis B patients. World J. Gastroenterol. 2019, 25, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Dusheiko, G. Treatment of HBeAg positive chronic hepatitis B: Interferon or nucleoside analogues. Liver Int. Off. J. Int. Assoc. Study Liver 2013, 33 (Suppl. S1), 137–150. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Chen, J. Interferon and Hepatitis B: Current and Future Perspectives. Front. Immunol. 2021, 12, 733364. [Google Scholar] [CrossRef] [PubMed]
- Hui, A.Y.; Chan, H.L.; Cheung, A.Y.; Cooksley, G.; Sung, J.J. Systematic review: Treatment of chronic hepatitis B virus infection by pegylated interferon. Aliment. Pharmacol. Ther. 2005, 22, 519–528. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatol Baltim Md. 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.G.; Ferraioli, G.; Palmeri, M.L.; Goodman, Z.D.; Garcia-Tsao, G.; Rubin, J.; Garra, B.; Myers, R.P.; Wilson, S.R.; Rubens, D.; et al. Elastography Assessment of Liver Fibrosis: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology 2015, 276, 845–861. [Google Scholar] [CrossRef] [PubMed]
- Buechter, M.; Gerken, G. Liver Function-How to Screen and to Diagnose: Insights from Personal Experiences, Controlled Clinical Studies and Future Perspectives. J. Pers. Med. 2022, 12, 1657. [Google Scholar] [CrossRef] [PubMed]
- Castera, L. Noninvasive methods to assess liver disease in patients with hepatitis B or C. Gastroenterology 2012, 142, 1293–1302.e4. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wu, D.; Wang, M.; Chen, E.; Bai, L.; Liu, C.; Liao, J.; Tang, H. Controlled attenuation parameter for the detection of hepatic steatosis in patients with chronic hepatitis B. Infect. Dis. 2016, 48, 670–675. [Google Scholar] [CrossRef] [PubMed]
- De Franchis, R. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J. Hepatol. 2015, 63, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L. EFSUMB Guidelines and Recommendations on the Clinical Use of Liver Ultrasound Elastography, Update 2017 (Long Version). Ultraschall Med.-Eur. J. Ultrasound 2017, 38, e16–e47. [Google Scholar]
- Fang, C.; Lim, A.; Sidhu, P.S. Ultrasound-based liver elastography in the assessment of fibrosis. Clin. Radiol. 2020, 75, 822–831. [Google Scholar] [CrossRef]
- Ferraioli, G. Review of Liver Elastography Guidelines. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2019, 38, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli, G. Ultrasound Techniques for the Assessment of Liver Stiffness: A Correct Terminology. Hepatol. Baltim. Md. 2019, 69, 461. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Adams, L.A. Advances in non-invasive assessment of hepatic fibrosis. Gut 2020, 69, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Cornberg, M.; Sandmann, L.; Protzer, U. Not Available. Z. Gastroenterol. 2021, 59, 691–776. [Google Scholar] [PubMed]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.Y.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- Lee, H.W.; Lee, J.S.; Ahn, S.H. Hepatitis B Virus Cure: Targets and Future Therapies. Int. J. Mol. Sci. 2020, 22, 213. [Google Scholar] [CrossRef]
- Nassal, M. HBV cccDNA: Viral persistence reservoir and key obstacle for a cure of chronic hepatitis B. Gut 2015, 64, 1972–1984. [Google Scholar] [CrossRef]
- Trépo, C.; Chan, H.L.Y.; Lok, A. Hepatitis B virus infection. Lancet Lond. Engl. 2014, 384, 2053–2063. [Google Scholar] [CrossRef] [PubMed]
- Wan, M.B.; Weng, X.H. Expert recommendations on the application of interferon for chronic hepatitis B. J. Dig. Dis. 2013, 14, 626–637. [Google Scholar] [CrossRef]
- Viganò, M.; Grossi, G.; Loglio, A.; Lampertico, P. Treatment of hepatitis B: Is there still a role for interferon? Liver Int. Off. J. Int. Assoc. Study Liver 2018, 38 (Suppl. S1), 79–83. [Google Scholar] [CrossRef] [PubMed]
- Konerman, M.A.; Lok, A.S. Interferon Treatment for Hepatitis B. Clin. Liver Dis. 2016, 20, 645–665. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, B.; Wang, L.; Chi, J.; Song, S.; Liu, M.; Zhao, Z. HBsAg seroclearance or seroconversion induced by peg-interferon alpha and lamivudine or adefovir combination therapy in chronic hepatitis B treatment: A meta-analysis and systematic review. Rev. Esp. Enferm. Dig. 2016, 108, 263–270. [Google Scholar] [CrossRef]
- Ferreira, S.C.; Chachá, S.G.F.; Souza, F.F.; Teixeira, A.C.; Santana, R.C.; Villanova, M.G.; Zucoloto, S.; Ramalho, L.N.; Perdoná, G.S.; Passos, A.D.; et al. Factors associated with spontaneous HBsAg clearance in chronic hepatitis B patients followed at a university hospital. Ann. Hepatol. 2014, 13, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Song, A.; Lin, X.; Chen, X. Functional cure for chronic hepatitis B: Accessibility, durability, and prognosis. Virol. J. 2021, 18, 114. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.; Contag, C.; Whitaker, E.; Terrault, N. Spontaneous loss of surface antigen among adults living with chronic hepatitis B virus infection: A systematic review and pooled meta-analyses. Lancet Gastroenterol. Hepatol. 2019, 4, 227–238. [Google Scholar] [CrossRef]
- Yeo, Y.H.; Ho, H.J.; Yang, H.-I.; Tseng, T.C.; Hosaka, T.; Trinh, H.N. Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection: A Systematic Review and Meta-analysis. Gastroenterology 2019, 156, 635–646.e9. [Google Scholar] [CrossRef]
- Tseng, T.-C.; Liu, C.-J.; Yang, H.-C.; Su, T.-H.; Wang, C.-C.; Chen, C.-L.; Kuo, S.F.-T.; Liu, C.-H.; Chen, P.-J.; Chen, D.-S.; et al. Determinants of spontaneous surface antigen loss in hepatitis B e antigen-negative patients with a low viral load. Hepatol. Baltim. Md. 2012, 55, 68–76. [Google Scholar] [CrossRef]
- Liu, J.; Yang, H.-I.; Lee, M.-H.; Lu, S.; Jen, C.; Wang, L.; You, S.; Iloeje, U.H.; Chen, C. Incidence and determinants of spontaneous hepatitis B surface antigen seroclearance: A community-based follow-up study. Gastroenterology 2010, 139, 474–482. [Google Scholar] [CrossRef]
- Yuen, M.-F.; Wong, D.K.-H.; Sablon, E.; Tse, E.; Ng, I.O.-L.; Yuan, H.-J.; Siu, C.-W.; Sander, T.J.; Bourne, E.J.; Hall, J.G.; et al. HBsAg seroclearance in chronic hepatitis B in the Chinese: Virological, histological, and clinical aspects. Hepatol. Baltim. Md. 2004, 39, 1694–1701. [Google Scholar] [CrossRef] [PubMed]
- Arai, M.; Togo, S.; Kanda, T.; Fujiwara, K.; Imazeki, F.; Yokosuka, O. Quantification of hepatitis B surface antigen can help predict spontaneous hepatitis B surface antigen seroclearance. Eur. J. Gastroenterol. Hepatol. 2012, 24, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-C.; Jeng, W.-J.; Chu, C.-M.; Liaw, Y.F. Decreasing levels of HBsAg predict HBsAg seroclearance in patients with inactive chronic hepatitis B virus infection. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2012, 10, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.-W.; Hu, T.-H.; Wang, J.-H.; Hung, C.H.; Lu, S.N.; Chen, C.H. Post-treatment HBsAg decline predicts high rate of HBsAg loss after stopping entecavir or tenofovir in HBeAg-negative patients without retreatment. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2023, 55, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.S.J.; Hirode, G.; Chen, C.-H.; Su, T.-H.; Seto, W.-K.; Van Hees, S.; Papatheodoridi, M.; Lens, S.; Wong, G.L.; Brakenhoff, S.M.; et al. Differential Relapse Patterns After Discontinuation of Entecavir vs Tenofovir Disoproxil Fumarate in Chronic Hepatitis B. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2023, 21, 1513–1522.e4. [Google Scholar] [CrossRef] [PubMed]
- van Bömmel, F.; Stein, K.; Heyne, R.; Petersen, J.; Buggisch, P.; Berg, C. A multicenter randomized-controlled trial of nucleos(t)ide analogue cessation in HBeAg-negative chronic hepatitis B. J. Hepatol. 2023, 78, 926–936. [Google Scholar] [CrossRef] [PubMed]
- Liaw, Y.F.; Sheen, I.S.; Chen, T.J.; Chu, C.M.; Pao, C.C. Incidence, determinants and significance of delayed clearance of serum HBsAg in chronic hepatitis B virus infection: A prospective study. Hepatol. Baltim. Md. 1991, 13, 627–631. [Google Scholar] [CrossRef]
- Gish, R.G.; Given, B.D.; Lai, C.-L.; Locarnini, S.A.; Lau, J.Y.; Lewis, D.L.; Schluep, T. Chronic hepatitis B: Virology, natural history, current management and a glimpse at future opportunities. Antiviral Res. 2015, 121, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-C.; Su, T.-H.; Tseng, T.-C.; Chen, C.-L.; Hsu, S.-J.; Liu, C.-H.; Liao, S.-H.; Hong, C.-M.; Lan, T.-Y.; Yang, H.-C.; et al. Metabolic Dysfunction-Associated Steatotic Liver Disease Facilitates Hepatitis B Surface Antigen Seroclearance and Seroconversion. Clin. Gastroenterol. Hepatol. 2024, 22, 581–590.e6. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yang, H.I.; Yeh, M.L.; Le, M.H.; Le, A.K.; Yeo, Y.H.; Dai, C.-Y.; Barnett, S.; Zhang, J.Q.; Huang, J.-F.; et al. Association Between Fatty Liver and Cirrhosis, Hepatocellular Carcinoma, and Hepatitis B Surface Antigen Seroclearance in Chronic Hepatitis B. J. Infect. Dis. 2021, 224, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Yang, H.-I.; Trinh, H.; Jeong, D.; Li, J.; Zhang, J.; Le, A.; Hoang, J.; Nguyen, P.; Henry, L.; et al. Antiviral therapy and hepatocellular carcinoma risk in hepatitis B patients with cirrhosis. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1207–1211. [Google Scholar] [CrossRef]
- Gnyawali, B.; Pusateri, A.; Nickerson, A.; Jalil, S.; Mumtaz, K. Epidemiologic and socioeconomic factors impacting hepatitis B virus and related hepatocellular carcinoma. World J. Gastroenterol. 2022, 28, 3793–3802. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhao, T.; Zhang, Y.; Zhang, A.-M.; Geng, J.; Xia, X. The incidence of hepatocellular carcinoma and clearance of hepatitis B surface for CHB patients in the indeterminate phase: A systematic review and meta-analysis. Front. Cell Infect. Microbiol. 2023, 13, 1226755. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Lampertico, P.; Manolakopoulos, S.; Lok, A. Incidence of hepatocellular carcinoma in chronic hepatitis B patients receiving nucleos(t)ide therapy: A systematic review. J. Hepatol. 2010, 53, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.K.; Majeed, A.; Kemp, W. Controversies in the Management of Hepatitis B: Hepatocellular Carcinoma. Clin. Liver Dis. 2021, 25, 785–803. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-W.; Yang, F.-C.; Lu, H.-Q.; Zhang, J.-S. Hepatocellular carcinoma and hepatitis B surface protein. World J. Gastroenterol. 2016, 22, 1943–1952. [Google Scholar] [CrossRef] [PubMed]
- Yeh, M.L.; Hung, C.H.; Huang, J.F.; Liu, C.-J.; Lee, C.-M.; Dai, C.-Y.; Wang, J.-H.; Lin, Z.-Y.; Lu, S.-N.; Hu, T.-H.; et al. Long-term effect of interferon plus ribavirin on hepatitis B surface antigen seroclearance in patients dually infected with hepatitis B and C viruses. PLoS ONE 2011, 6, e20752. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Value (Median; IQR) | Reference Value |
|---|---|---|
| HBV DNA [IU/mL] | 3329 (356; 759626) | <10 IU/mL |
| HBsAg [IU/mL] | 3823 (729; 12502) | <5 IU/mL |
| ꙋGT [U/L] | 23 (14; 43) | <60 U/L |
| AST [U/L] | 29 (22; 42) | <35 U/L |
| ALT [U/L] | 37 (24; 65) | <45 U/L |
| bilirubin [mg/dL] | 0.6 (0.5; 0.8) | 0.1–1.2 mg/dL |
| cholesterol [mg/dL] | 186 (161; 215) | <250 mg/dL |
| HDL [mg/dL] | 50 (40; 63) | 40–60 mg/dL |
| LDL [mg/dL] | 114 (91; 139) | <150 mg/dL |
| triglycerides [mg/dL] | 96 (71; 141) | <150 mg/dL |
| glucose [mg/dL] | 88 (81; 95) | 60–99 mg/dL |
| HbA1c [%] | 5.5 (5.2; 5.8) | <5.7% |
| Genotype | Frequency (n) | Proportion (%) |
|---|---|---|
| A | 43 | 11.6 |
| B | 9 | 2.4 |
| C | 4 | 1.1 |
| D | 110 | 29.6 |
| E | 9 | 2.4 |
| F | 1 | 0.3 |
| G | 1 | 0.3 |
| H | 1 | 0.3 |
| Unknown | 193 | 52.0 |
| Total | 371 | 100.0 |
| Therapy | Number of Patients Achieving Seroconversion | Number of Patients under That Specific Therapy | Fraction of Patients Achieving Seroconversion | Mean Timespan from Initial Diagnosis to Seroconversion in Months | Standard Deviation in Months |
|---|---|---|---|---|---|
| No therapy | 11 | 111 (29.9%) | 9.9% | 167.5 | 148.2 |
| Interferone | 4 | 58 (15.6%) | 6.9% | 198 | 51.2 |
| Telbivudine | 2 | 29 (7.8%) | 6.9% | 93 | 48.1 |
| Lamivudine | 3 | 63 (17%) | 4.8% | 174.3 | 60.1 |
| Any therapy (**NRTI+ *NNRTI+ Interferone) | 10 | 260 (70.1%) | 3.8% | 152.7 | 78 |
| Adefovir | 2 | 55 (14.8%) | 3.6% | 140.5 | 19.1 |
| **NRTI + *NNRTI | 8 | 237 (63.9%) | 3.3% | 143.3 | 81.7 |
| Entecavir | 3 | 93 (25.1%) | 3.2% | 106.3 | 86.6 |
| Tenofovir | 4 | 165 (44.5%) | 2.4% | 146.3 | 77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buechter, M.; Günther, A.M.; Manka, P.; Gerken, G.; Kahraman, A. Factors Positively Correlated with Hepatitis B Surface Antigen Seroconversion in Chronic Hepatitis B. J. Pers. Med. 2024, 14, 390. https://doi.org/10.3390/jpm14040390
Buechter M, Günther AM, Manka P, Gerken G, Kahraman A. Factors Positively Correlated with Hepatitis B Surface Antigen Seroconversion in Chronic Hepatitis B. Journal of Personalized Medicine. 2024; 14(4):390. https://doi.org/10.3390/jpm14040390
Chicago/Turabian StyleBuechter, Matthias, Arne Maria Günther, Paul Manka, Guido Gerken, and Alisan Kahraman. 2024. "Factors Positively Correlated with Hepatitis B Surface Antigen Seroconversion in Chronic Hepatitis B" Journal of Personalized Medicine 14, no. 4: 390. https://doi.org/10.3390/jpm14040390
APA StyleBuechter, M., Günther, A. M., Manka, P., Gerken, G., & Kahraman, A. (2024). Factors Positively Correlated with Hepatitis B Surface Antigen Seroconversion in Chronic Hepatitis B. Journal of Personalized Medicine, 14(4), 390. https://doi.org/10.3390/jpm14040390