
The Performance of a Survival Nomogram and Albumin–Bilirubin Grade as Prognostic Tools in Advanced Hepatocellular Carcinoma Treated with FOLFOX4

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Procedure
2.2. Measurement
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Treatment Information
3.3. OS
3.4. PFS
3.5. ORR
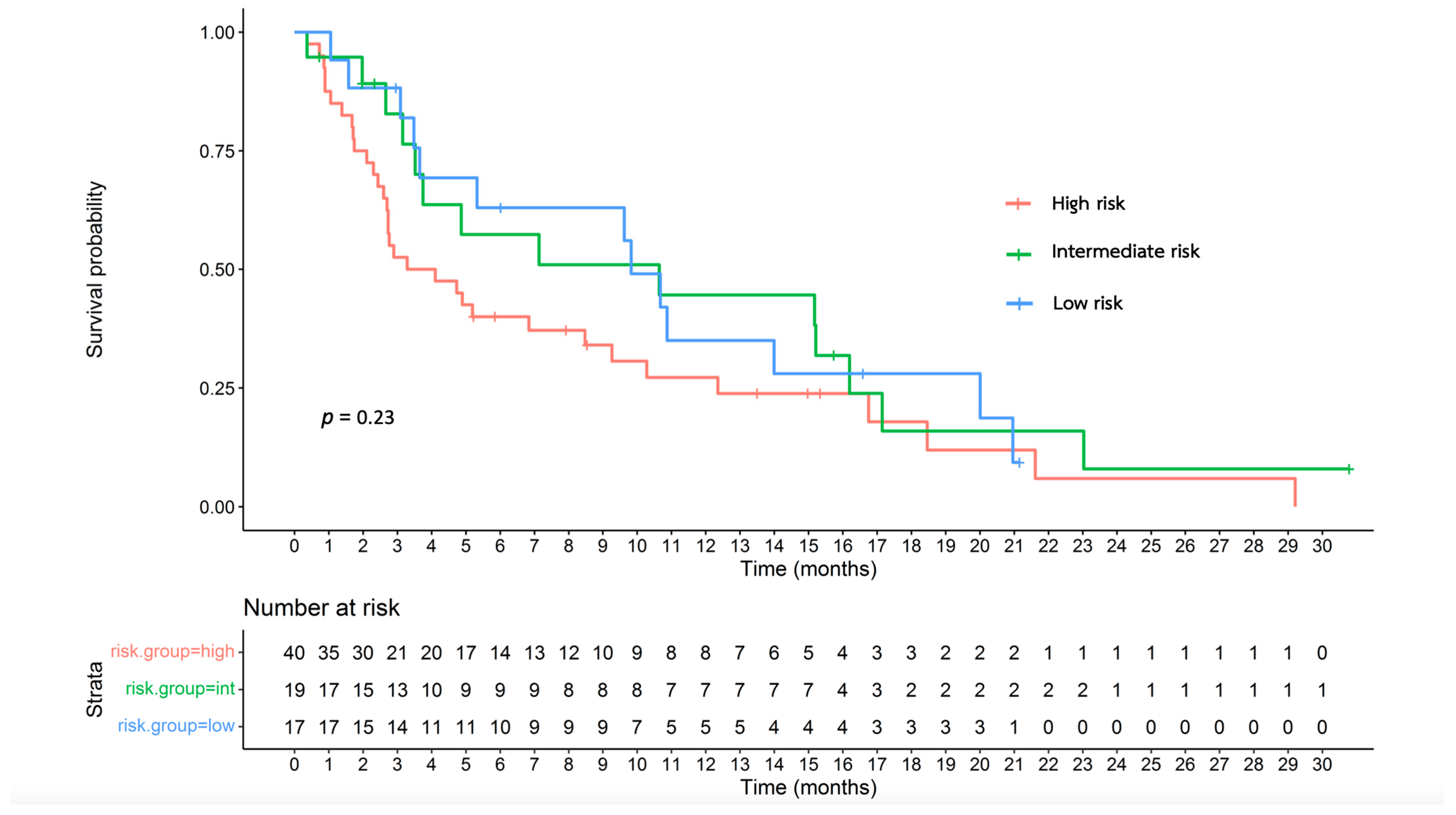
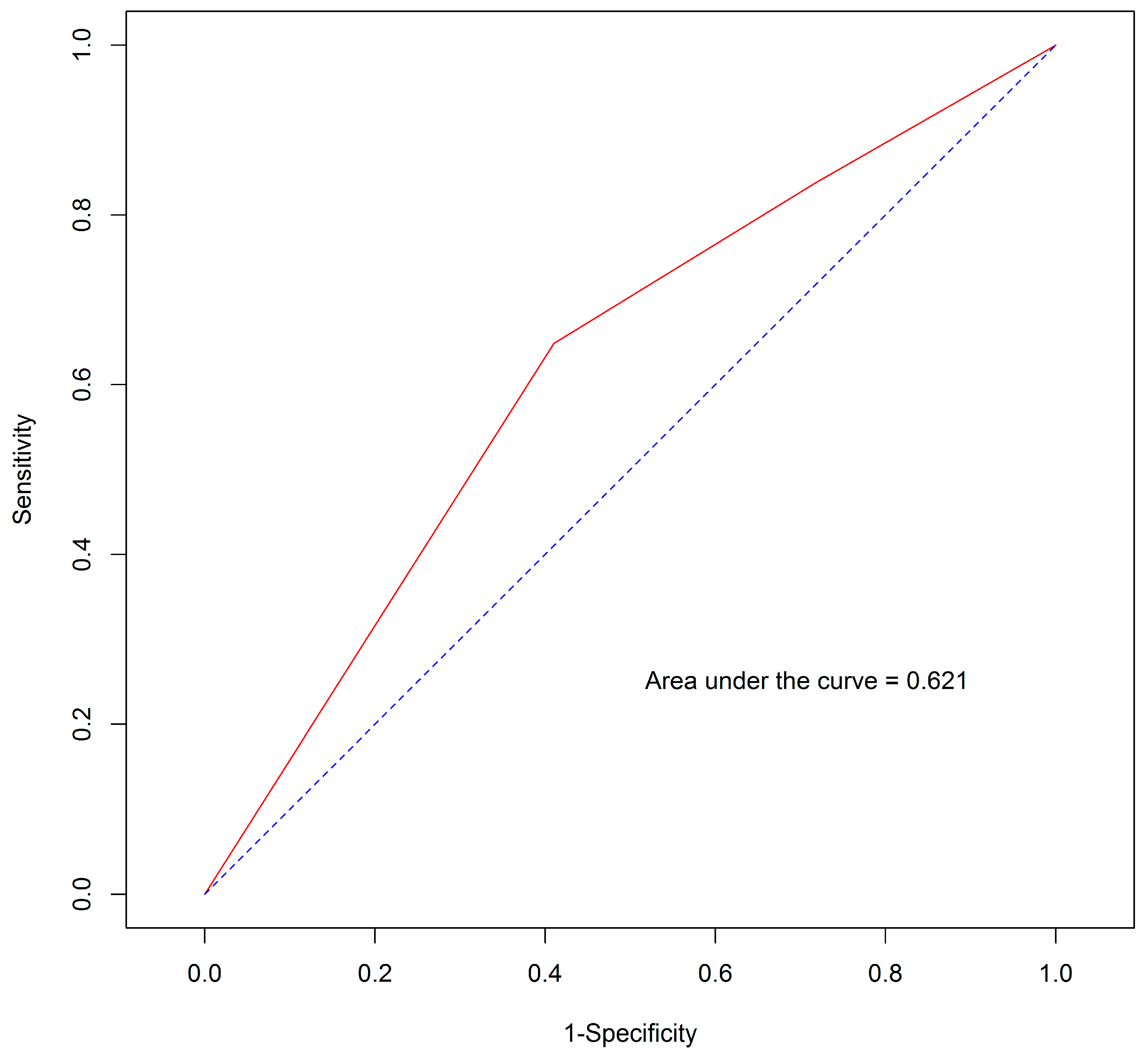
3.6. Effectiveness of the Proposed Survival Nomogram
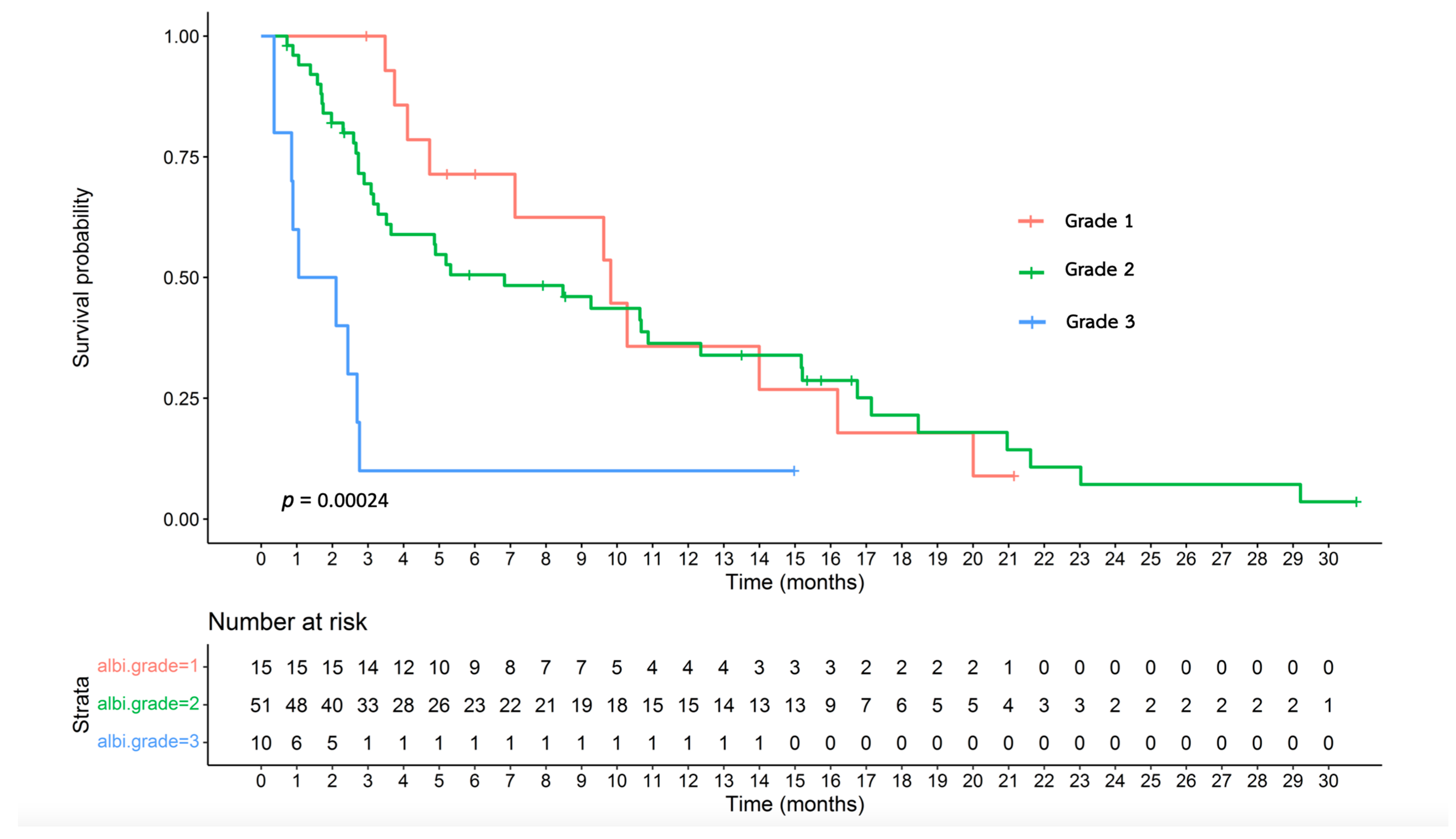
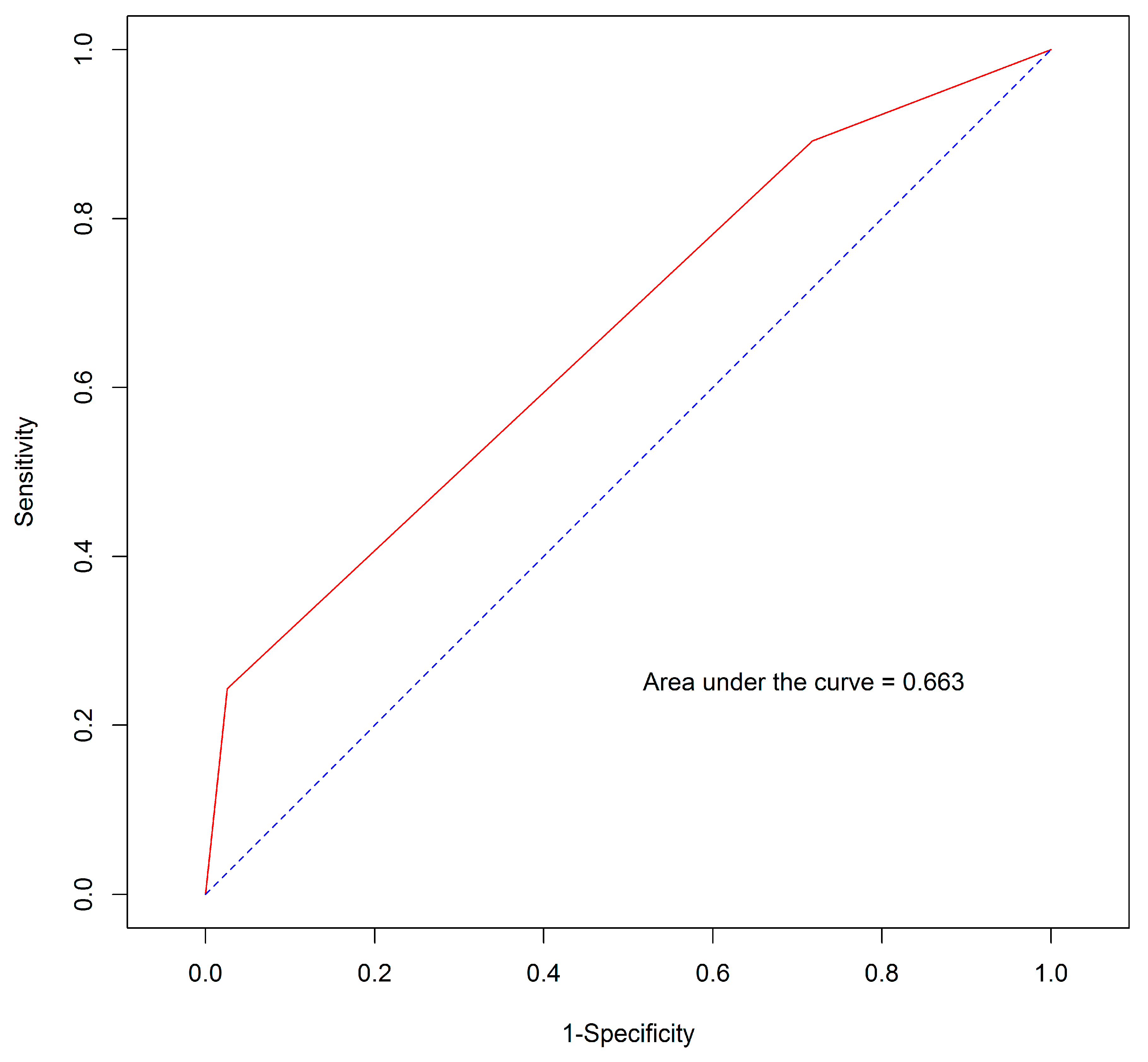
3.7. Effectiveness of the ALBI Grade
4. Discussion
- Our study is limited by a relatively small sample size, i.e., 76 patients, in contrast to a larger cohort of 187 patients in the original EACH study.
- Differences in baseline characteristics, as summarized in Supplementary Table S5, indicated that our patients exhibited more high-risk features. These differences probably reflect the differences between the clinical trial conditions and real-world scenarios.
- 3.
- The AUROC and Harrel’s C-index metrics of our study model were 0.621 and 0.589, respectively. These values signified the considerably less effective discrimination performance when compared with the values of 0.7 for both metrics in the original EACH study [15]. Importantly, the variables incorporated into the proposed survival nomogram in our study did not exhibit statistically significant associations with survival, as previously observed in the EACH study. In our cohort, only TB displayed statistical significance. This discrepancy possibly contributed to the poor performance and discriminatory capability of the nomogram in our patient population.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Imsamran, W.; Pattatang, A.; Supaattagorn, P.; Chiawiriyabunya, I.; Namthaisong, K.; Wongsena, M.; Puttawibul, P.; Chitapanarux, I.; Suwanrungruang, K.; Sangrajrang, S.; et al. Cancer in Thailand Volume IX, 2013–2015; New Thammada Press: Bangkok, Thailand, 2018. [Google Scholar]
- International Agency for Research on Cancer; World Health Organization; GLOBOCAN. Estimated Number of New Cases and Deaths from 2020 to 2030; International Agency for Research on Cancer: Lyon, France, 2020; Volume 2023, Available online: https://gco.iarc.fr/tomorrow/en/dataviz/isotype (accessed on 1 August 2023).
- Chonprasertsuk, S.; Vilaichone, R.K. Epidemiology and Treatment of Hepatocellular Carcinoma in Thailand. Jpn. J. Clin. Oncol. 2017, 47, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Sithinamsuwan, P.; Piratvisuth, T.; Tanomkiat, W.; Apakupakul, N.; Tongyoo, S. Review of 336 patients with hepatocellular carcinoma at Songklanagarind Hospital. World J. Gastroenterol. 2000, 6, 339–343. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Hepatobiliary Cancers (Version 1.2023). 2023. Available online: https://www.nccn.org/professionals/physician_gls/pdf/hcc.pdf (accessed on 1 August 2023).
- Thai. Association for the Study of the Liver. Thailand Guideline for Management of Hepatocellular Carcinoma. 2021. Available online: https://thasl.org/wp-content/uploads/2021/04/%E0%B9%81%E0%B8%99%E0%B8%A7%E0%B8%97%E0%B8%B2%E0%B8%87%E0%B8%81%E0%B8%B2%E0%B8%A3%E0%B8%94%E0%B8%B9%E0%B9%81%E0%B8%A5%E0%B8%A1%E0%B8%B0%E0%B9%80%E0%B8%A3%E0%B9%87%E0%B8%87%E0%B8%95%E0%B8%B1%E0%B8%9A%E0%B9%83%E0%B8%99%E0%B8%9B%E0%B8%A3%E0%B8%B0%E0%B9%80%E0%B8%97%E0%B8%A8%E0%B9%84%E0%B8%97%E0%B8%A2-%E0%B8%9E%E0%B8%A8-2564_25-03-64_all.pdf (accessed on 1 August 2023).
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Lau, G.; Kudo, M.; Chan, S.L.; Kelley, R.K.; Furuse, J.; Sukeepaisarnjaroen, W.; Kang, Y.K.; Van Dao, T.; De Toni, E.N.; et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 2022, 1, EVIDoa2100070. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Gong, X. Progression of systemic chemotherapy with oxaliplatin-containing regimens for advanced hepatocellular carcinoma in China. Hepat. Oncol. 2016, 3, 71–81. [Google Scholar] [CrossRef]
- Qin, S.; Bai, Y.; Lim, H.Y.; Thongprasert, S.; Chao, Y.; Fan, J.; Yang, T.S.; Bhudhisawasdi, V.; Kang, W.K.; Zhou, Y.; et al. Randomized, multicenter, open-label study of oxaliplatin plus fluorouracil/leucovorin versus doxorubicin as palliative chemotherapy in patients with advanced hepatocellular carcinoma from Asia. J. Clin. Oncol. 2013, 31, 3501–3508. [Google Scholar] [CrossRef]
- Qin, S.; Cheng, Y.; Liang, J.; Shen, L.; Bai, Y.; Li, J.; Fan, J.; Liang, L.; Zhang, Y.; Wu, G.; et al. Efficacy and safety of the FOLFOX4 regimen versus doxorubicin in Chinese patients with advanced hepatocellular carcinoma: A subgroup analysis of the EACH study. Oncologist 2014, 19, 1169–1178. [Google Scholar] [CrossRef]
- Zhang, P.; Wen, F.; Li, Q. FOLFOX4 or sorafenib as the first-line treatments for advanced hepatocellular carcinoma: A cost-effectiveness analysis. Dig. Liver Dis. 2016, 48, 1492–1497. [Google Scholar] [CrossRef]
- Qin, S.; Zhang, X.; Guo, W.; Feng, J.; Zhang, T.; Men, L.; He, J. Prognostic nomogram for advanced hepatocellular carcinoma treated with FOLFOX 4. Asian Pac. J. Cancer Prev. 2017, 18, 1225–1232. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.L.; Johnson, P.J.; Mo, F.; Berhane, S.; Teng, M.; Chan, A.W.; Poon, M.C.; Lai, P.B.; Yu, S.; Chan, A.T.; et al. International validation of the Chinese university prognostic index for staging of hepatocellular carcinoma: A joint United Kingdom and Hong Kong study. Chin. J. Cancer 2014, 33, 481–491. [Google Scholar] [CrossRef]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef]
- Vauthey, J.N.; Lauwers, G.Y.; Esnaola, N.F.; Do, K.A.; Belghiti, J.; Mirza, N.; Curley, S.A.; Ellis, L.M.; Regimbeau, J.M.; Rashid, A.; et al. Simplified staging for hepatocellular carcinoma. J. Clin. Oncol. 2002, 20, 1527–1536. [Google Scholar] [CrossRef]
- Demirtas, C.O.; D’Alessio, A.; Rimassa, L.; Sharma, R.; Pinato, D.J. ALBI grade: Evidence for an improved model for liver functional estimation in patients with hepatocellular carcinoma. JHEP Rep. 2021, 3, 100347. [Google Scholar] [CrossRef] [PubMed]
- Tandon, P.; Garcia-Tsao, G. Prognostic indicators in hepatocellular carcinoma: A systematic review of 72 studies. Liver Int. 2009, 29, 502–510. [Google Scholar] [CrossRef]
- Yen, Y.H.; Cheng, Y.F.; Wang, J.H.; Lin, C.C.; Wang, C.C. Characteristics and etiologies of hepatocellular carcinoma in patients without cirrhosis: When East meets West. PLoS ONE 2021, 16, e0244939. [Google Scholar] [CrossRef]
- Tham, J.; Goh, T.L.; Barclay, S.; Priest, M.; Forrest, E.; Fraser, A.; Stanley, A. P221 non-cirrhotic vs. Cirrhotic HCC: Comparison between patient characteristics, aetiology and outcomes. Gut 2021, 70, A157–A158. [Google Scholar] [CrossRef]
- Zipprich, A.; Garcia-Tsao, G.; Rogowski, S.; Fleig, W.E.; Seufferlein, T.; Dollinger, M.M. Prognostic indicators of survival in patients with compensated and decompensated cirrhosis. Liver Int. 2012, 32, 1407–1414. [Google Scholar] [CrossRef] [PubMed]
- Edeline, J.; Raoul, J.L.; Vauleon, E.; Guillygomac’h, A.; Boudjema, K.; Boucher, E. Systemic chemotherapy for hepatocellular carcinoma in non-cirrhotic liver: A retrospective study. World J. Gastroenterol. 2009, 15, 713–716. [Google Scholar] [CrossRef]
- Liang, B.Y.; Gu, J.; Xiong, M.; Zhang, E.L.; Zhang, Z.Y.; Chen, X.P.; Huang, Z.Y. Tumor size may influence the prognosis of solitary hepatocellular carcinoma patients with cirrhosis and without macrovascular invasion after hepatectomy. Sci. Rep. 2021, 11, 16343. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Liu, P.H.; Ho, S.Y.; Huang, Y.H.; Lee, Y.H.; Chiou, Y.Y.; Hsieh, T.H.; Fang, T.; Tsai, Y.J.; Hou, M.C.; et al. Impact of tumor burden on prognostic prediction for patients with terminal stage hepatocellular carcinoma: A nomogram study. PLoS ONE 2017, 12, e0188031. [Google Scholar] [CrossRef]
- Ho, S.Y.; Liu, P.H.; Hsu, C.Y.; Ko, C.C.; Huang, Y.H.; Su, C.W.; Lee, R.C.; Tsai, P.H.; Hou, M.C.; Huo, T.I. Tumor burden score as a new prognostic marker for patients with hepatocellular carcinoma undergoing transarterial chemoembolization. J. Gastroenterol. Hepatol. 2021, 36, 3196–3203. [Google Scholar] [CrossRef] [PubMed]
- Muscari, F.; Maulat, C. Preoperative alpha-fetoprotein (AFP) in hepatocellular carcinoma (HCC): Is this 50-year biomarker still up-to-date? Transl. Gastroenterol. Hepatol. 2020, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Yoon, E.L.; Yeon, J.E.; Lee, H.J.; Suh, S.J.; Lee, S.J.; Kang, S.H.; Kang, K.; Yoo, Y.J.; Kim, J.H.; Yim, H.J.; et al. Systemic cytotoxic chemotherapy of patients with advanced hepatocellular carcinoma in the era of sorafenib nonavailability. J. Clin. Gastroenterol. 2014, 48, e22–e29. [Google Scholar] [CrossRef] [PubMed]
- Brar, G.; Greten, T.F.; Graubard, B.I.; McNeel, T.S.; Petrick, J.L.; McGlynn, K.A.; Altekruse, S.F. Hepatocellular carcinoma survival by etiology: A SEER-Medicare database analysis. Hepatol. Commun. 2020, 4, 1541–1551. [Google Scholar] [CrossRef] [PubMed]
- Marot, A.; Henrion, J.; Knebel, J.F.; Moreno, C.; Deltenre, P. Alcoholic liver disease confers a worse prognosis than HCV infection and non-alcoholic fatty liver disease among patients with cirrhosis: An observational study. PLoS ONE 2017, 12, e0186715. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Sharma, R.; Allara, E.; Yen, C.; Arizumi, T.; Kubota, K.; Bettinger, D.; Jang, J.W.; Smirne, C.; Kim, Y.W.; et al. The ALBI grade provides objective hepatic reserve estimation across each BCLC stage of hepatocellular carcinoma. J. Hepatol. 2017, 66, 338–346. [Google Scholar] [CrossRef]
- Edeline, J.; Blanc, J.F.; Johnson, P.; Campillo-Gimenez, B.; Ross, P.; Ma, Y.T.; King, J.; Hubner, R.A.; Sumpter, K.; Darby, S.; et al. A multicentre comparison between Child Pugh and albumin-bilirubin scores in patients treated with sorafenib for hepatocellular carcinoma. Liver Int. 2016, 36, 1821–1828. [Google Scholar] [CrossRef]
- Takada, H.; Kurosaki, M.; Tsuchiya, K.; Komiyama, Y.; Itakura, J.; Takahashi, Y.; Nakanishi, H.; Yasui, Y.; Tamaki, N.; Maeyashiki, C.; et al. Baseline and early predictors of good patient candidates for second-line after sorafenib treatment in unresectable hepatocellular carcinoma. Cancers 2019, 11, 1256. [Google Scholar] [CrossRef]
- Lee, P.C.; Chao, Y.; Chen, M.H.; Lan, K.H.; Lee, C.J.; Lee, I.C.; Chen, S.C.; Hou, M.C.; Huang, Y.H. Predictors of response and survival in immune checkpoint inhibitor-treated unresectable hepatocellular carcinoma. Cancers 2020, 12, 182. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Kaneko, T.; Saeed, A.; Pressiani, T.; Kaseb, A.; Wang, Y.; Szafron, D.; Jun, T.; Dharmapuri, S.; Naqash, A.R.; et al. Immunotherapy in hepatocellular cancer patients with mild to severe liver dysfunction: Adjunctive role of the ALBI grade. Cancers 2020, 12, 1862. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Frenette, C.; Sung, M.W.; Daniele, B.; Baron, A.D.; Chan, S.L.; Blanc, J.; Tamai, T.; Ren, M.; Lim, H.J.; et al. Baseline liver function and outcomes in the phase III REFLECT study in patients with unresectable hepatocellular carcinoma (uHCC). J. Clin. Oncol. 2020, 38 (Suppl. S4), 524. [Google Scholar] [CrossRef]
- Shimose, S.; Kawaguchi, T.; Iwamoto, H.; Tanaka, M.; Miyazaki, K.; Ono, M.; Niizeki, T.; Shirono, T.; Okamura, S.; Nakano, M.; et al. Controlling nutritional status (CONUT) score is associated with overall survival in patients with unresectable hepatocellular carcinoma treated with lenvatinib: A multicenter cohort study. Nutrients 2020, 12, 1076. [Google Scholar] [CrossRef]
- Kim, H.D.; Bang, Y.; Lee, M.A.; Kim, J.W.; Kim, J.H.; Chon, H.J.; Kang, B.; Kang, M.J.; Kim, I.; Cheon, J.; et al. Regorafenib in patients with advanced Child-Pugh B hepatocellular carcinoma: A multicentre retrospective study. Liver Int. 2020, 40, 2544–2552. [Google Scholar] [CrossRef]
- Vogel, A.; Merle, P.; Verslype, C.; Finn, R.S.; Zhu, A.X.; Cheng, A.L.; Chan, S.L.; Yau, T.; Ryoo, B.Y.; Knox, J.; et al. ALBI score and outcomes in patients with hepatocellular carcinoma: Post hoc analysis of the randomized controlled trial KEYNOTE-240. Ther. Adv. Med. Oncol. 2021, 13, 17588359211039928. [Google Scholar] [CrossRef]
- Kuo, Y.H.; Wang, J.H.; Hung, C.H.; Rau, K.M.; Wu, I.P.; Chen, C.H.; Kee, K.M.; Hu, T.H.; Lu, S.N. Albumin-bilirubin grade predicts prognosis of HCC patients with sorafenib use. J. Gastroenterol. Hepatol. 2017, 32, 1975–1981. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 76) | First-Line Chemotherapy Cohort (n = 56) | Later-Line Chemotherapy Cohort (n = 20) | |
|---|---|---|---|
| Setting, n (%) | |||
| First-line treatment | 56 (73.7) | 56 (100) | - |
| Second-line treatment | 15 (19.7) | - | 15 (75.0) |
| Third-line treatment | 3 (4.0) | - | 3 (15.0) |
| Fourth-line treatment | 2 (2.6) | - | 2 (10.0) |
| Sex, n (%) | |||
| Women | 13 (17.1) | 9 (16.1) | 4 (20.0) |
| Men | 63 (82.9) | 47 (83.9) | 16 (80.0) |
| Age, mean (SD), years | 56.5 (9.8) | 55.9 (10.1) | 58.0 (8.9) |
| BMI, median (IQR), kg/m2 | 21.8 (19.4, 24.5) | 22.2 (20.1, 24.6) | 21.1 (19.2, 23.5) |
| Healthcare system, n (%) | |||
| CSMBS | 12 (15.8) | 6 (10.7) | 6 (30.0) |
| Social security | 7 (9.2) | 7 (12.5) | 0 (0) |
| Universal coverage | 53 (69.7) | 42 (75.0) | 11 (55.0) |
| Self-payment | 4 (5.3) | 1 (1.8) | 3 (15.0) |
| ECOG, n (%) | |||
| 0 | 9 (11.8) | 5 (8.9) | 4 (20.0) |
| 1 | 64 (84.2) | 49 (87.5) | 15 (75.0) |
| 2 | 3 (3.9) | 2 (3.6) | 1 (5.0) |
| Cirrhosis, n (%) | 69 (90.8) | 52 (92.9) | 17 (85.0) |
| CTP class, n (%) | |||
| A | 56 (73.7) | 39 (69.7) | 17 (85.0) |
| B | 20 (26.3) | 17 (30.3) | 3 (15.0) |
| Etiology *, n (%) | |||
| HBV | 56 (73.7) | 41 (73.2) | 15 (75.0) |
| HCV | 11 (14.5) | 8 (14.3) | 3 (15.0) |
| Alcohol | 12 (15.8) | 9 (16.1) | 3 (15.0) |
| NAFLD | 2 (2.6) | 1 (1.8) | 1 (5.0) |
| PSC | 1 (1.3) | 1 (1.8) | 0 (0) |
| Number of liver tumors, n (%) | |||
| 0 | 8 (10.5) | 4 (7.1) | 4 (20.0) |
| 1–5 | 35 (46.1) | 28 (50.0) | 7 (35.0) |
| 6–10 | 4 (5.2) | 2 (3.6) | 2 (10.0) |
| >10 | 24 (31.6) | 17 (30.4) | 7 (35.0) |
| Infiltrative | 5 (6.6) | 5 (8.9) | 0 (0) |
| Maximum tumor diameter, mean (SD), cm | 11.0 (6) | 11.0 (5.6) | 10.9 (7.5) |
| Vascular involvement, n (%) | 43 (56.6) | 34 (60.7) | 9 (45.0) |
| Ascites, n (%) | 8 (10.5) | 6 (10.7) | 2 (10.0) |
| BCLC, n (%) | |||
| B | 9 (11.8) | 6 (11.4) | 3 (15.0) |
| C | 67 (88.2) | 50 (89.3) | 17 (85.0) |
| Extrahepatic metastasis, n (%) | |||
| 1 | 28 (36.8) | 21 (37.5) | 7 (35.0) |
| 2 | 10 (13.2) | 6 (10.7) | 4 (20.0) |
| 3 | 1 (1.3) | 0 (0) | 1 (5.0) |
| 4 | 1 (1.3) | 0 (0) | 1 (5.0) |
| Metastatic site, n (%) | |||
| Lymph node | 14 (18.4) | 8 (14.3) | 6 (30.0) |
| Lungs | 19 (25.0) | 10 (17.9) | 9 (45.0) |
| Pleura | 3 (3.9) | 1 (1.8) | 2 (10.0) |
| Peritoneum | 11 (14.5) | 8 (14.3) | 3 (15.0) |
| Adrenal gland | 3 (3.9) | 2 (3.6) | 1 (5.0) |
| Bone | 3 (3.9) | 2 (3.6) | 1 (5.0) |
| Ovary | 1 (1.3) | 1 (1.8) | 0 (0) |
| Pancreas | 1 (1.3) | 1 (1.8) | 0 (0) |
| Laboratory results | |||
| TB, median (IQR), mg/dL | 1.2 (0.7, 1.8) | 1.3 (0.7, 1.8) | 1.0 (0.5, 1.6) |
| AST, median (IQR), U/L | 101.5 (61.5, 214.5) | 117 (65.0, 280.5) | 94.0 (54.5, 112) |
| ALT, median (IQR), U/L | 45 (30.0, 78.8) | 49 (29.8, 85.2) | 40.5 (30.8, 70.0) |
| ALP, median (IQR), U/L | 235 (133.0, 395.0) | 263.5 (144.5, 398.5) | 196.5 (95.5, 293.8) |
| Albumin, mean (SD), g/dL | 3.5 (0.5) | 3.4 (0.5) | 3.6 (0.5) |
| Platelet count, median (IQR), /µL | 201,500 (127,750, 261,000) | 201,500 (121,250, 256,500) | 205,000 (141,750, 262,500) |
| INR level, median (IQR) | 1.2 (1.1, 1.3) | 1.2 (1.2, 1.4) | 1.2 (1.1, 1.2) |
| Creatinine, median (IQR), mg/dL | 0.8 (0.7, 1.0) | 0.8 (0.7, 1.0) | 0.8 (0.7, 0.9) |
| AFP, median (IQR), ng/dL | 5630.5 (152.1, 30,045) | 5048.0 (135.2, 31,011) | 11,231.5 (155, 30,045) |
| Previous treatment, n (%) | |||
| Resection | 13 (17.1) | 5 (8.9) | 8 (40.0) |
| TACE | 31 (40.8) | 19 (33.9) | 12 (60.0) |
| RFA | 7 (9.2) | 6 (10.7) | 1 (5.0) |
| SBRT | 2 (2.6) | 2 (3.6) | 0 (0) |
| Doxorubicin | 4 (5.3) | 0 (0) | 4 (20.0) |
| Sorafenib | 12 (15.8) | 0 (0) | 12 (60.0) |
| Regorafenib | 2 (2.6) | 0 (0) | 2 (10.0) |
| Nivolumab | 3 (3.9) | 0 (0) | 3 (15.0) |
| Atezolizumab plus bevacizumab | 1 (1.3) | 0 (0) | 1 (5.0) |
| Durvalumab plus tremelimumab | 2 (2.6) | 0 (0) | 2 (10.0) |
| Total (n = 76) | First-Line Chemotherapy Cohort (n = 56) | Later-Line Chemotherapy Cohort (n = 20) | |
|---|---|---|---|
| Evaluable, n (%) | 40 (52.6) | 26 (46.4) | 14 (70.0) |
| Complete response, n (%) | (0) | 0 (0) | 0 (0) |
| Partial response, n (%) | 9 (11.8) | 5 (8.9) | 4 (20.0) |
| Stable disease, n (%) | 15 (19.7) | 10 (17.9) | 5 (25.0) |
| Progressive disease, n (%) | 16 (21.1) | 11 (19.6) | 5 (25.0) |
| ORR as per ITT, n (%) | 9 (11.8) | 5 (8.9) | 4 (20.0) |
| ORR as per assessable, n (%) | 9 (22.5) | 5 (19.2) | 4 (23.5) |
| DCR as per ITT, n (%) | 24 (31.5) | 15 (26.8) | 9 (45.0) |
| DCR as per assessable, n (%) | 24 (60.0) | 15 (57.7) | 9 (64.3) |
| Median OS, Months (95% CI) | Survival Nomogram | p-Value | ||
|---|---|---|---|---|
| Low Risk | Intermediate Risk | High Risk | ||
| Entire cohort (n = 76) | 9.82 (5.32, NA) | 10.64 (3.75, NA) | 3.70 (2.69, 9.26) | 0.23 |
| First-line cohort (n = 56) | 5.32 (3.48, NA) | 8.89 (3.75, NA) | 3.29 (2.43, NA) | 0.62 |
| Later-line cohort (n = 20) | 12.43 (9.82, NA) | 13.27 (2.66, NA) | 4.73 (2.69, NA) | 0.50 |
| Median OS, Months (95% CI) | ALBI Grade | p-Value | ||
|---|---|---|---|---|
| Grade 1 | Grade 2 | Grade 3 | ||
| Entire cohort (n = 76) | 9.82 (7.13, NA) | 6.83 (3.16, 15.20) | 1.58 (0.85, NA) | 0.00024 |
| First-line cohort (n = 56) | 9.63 (4.11, NA) | 5.26 (3.15, 15.20) | 1.05 (0.85, NA) | 0.0025 |
| Later-line cohort (n = 20) | 13.99 (9.82, NA) | 10.87 (2.73, NA) | 2.69 (NA, NA) | 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wonglhow, J.; Sunpaweravong, P.; Sathitruangsak, C.; Dechaphunkul, A. The Performance of a Survival Nomogram and Albumin–Bilirubin Grade as Prognostic Tools in Advanced Hepatocellular Carcinoma Treated with FOLFOX4. J. Pers. Med. 2024, 14, 403. https://doi.org/10.3390/jpm14040403
Wonglhow J, Sunpaweravong P, Sathitruangsak C, Dechaphunkul A. The Performance of a Survival Nomogram and Albumin–Bilirubin Grade as Prognostic Tools in Advanced Hepatocellular Carcinoma Treated with FOLFOX4. Journal of Personalized Medicine. 2024; 14(4):403. https://doi.org/10.3390/jpm14040403
Chicago/Turabian StyleWonglhow, Jirapat, Patrapim Sunpaweravong, Chirawadee Sathitruangsak, and Arunee Dechaphunkul. 2024. "The Performance of a Survival Nomogram and Albumin–Bilirubin Grade as Prognostic Tools in Advanced Hepatocellular Carcinoma Treated with FOLFOX4" Journal of Personalized Medicine 14, no. 4: 403. https://doi.org/10.3390/jpm14040403
APA StyleWonglhow, J., Sunpaweravong, P., Sathitruangsak, C., & Dechaphunkul, A. (2024). The Performance of a Survival Nomogram and Albumin–Bilirubin Grade as Prognostic Tools in Advanced Hepatocellular Carcinoma Treated with FOLFOX4. Journal of Personalized Medicine, 14(4), 403. https://doi.org/10.3390/jpm14040403