
The Effect of Intermittent Pneumatic Compression on Hemodynamics and Regional Cerebral Oxygen Saturation in Laparoscopic Bariatric Surgery with Mild Hypercapnia in the Steep Reverse Trendelenburg Position


Abstract
:1. Introduction
2. Materials and Methods
3. Results
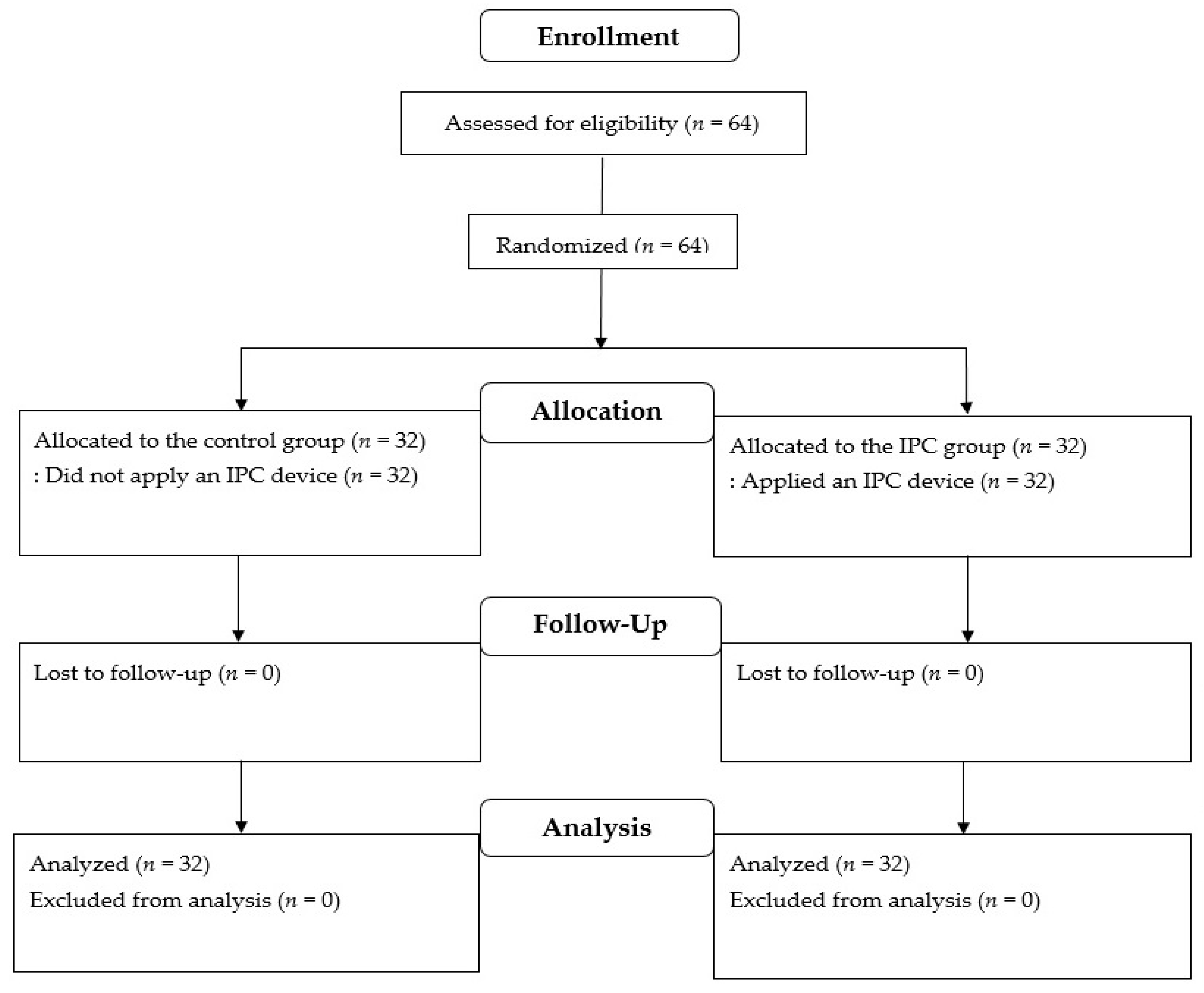
3.1. Participants
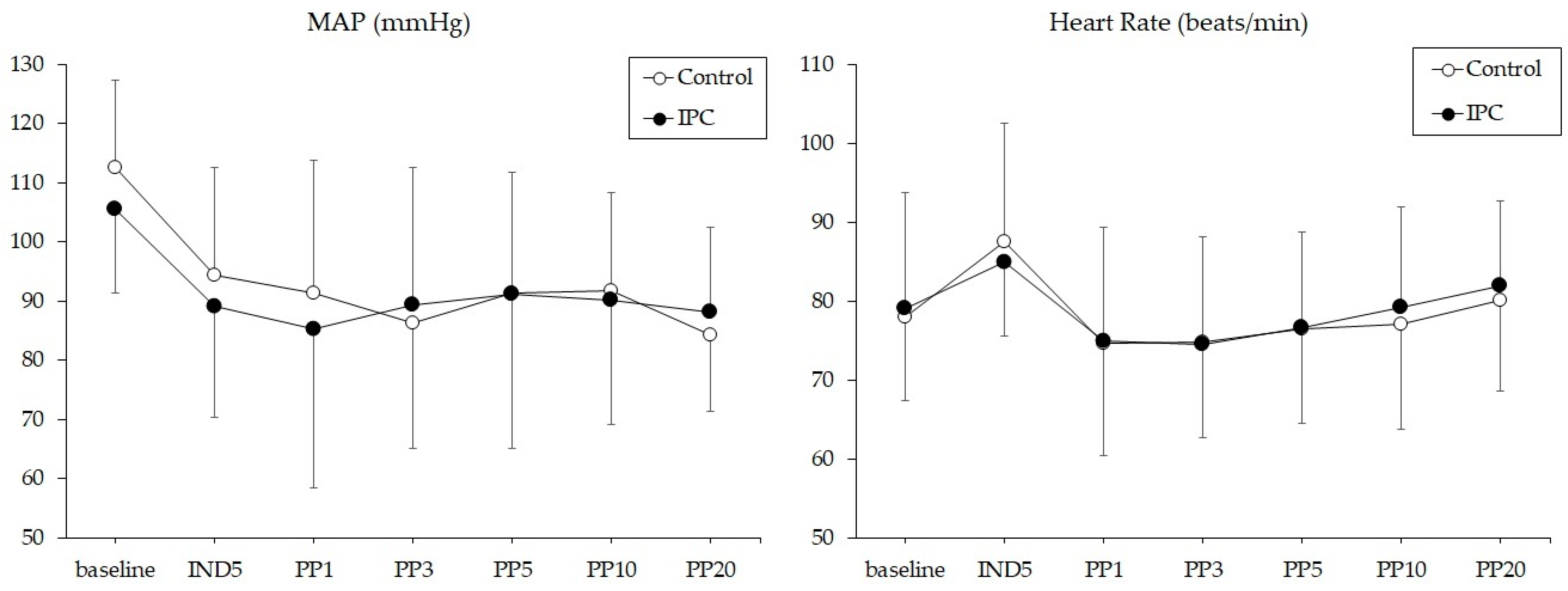
3.2. Intraoperative Hemodynamic Data
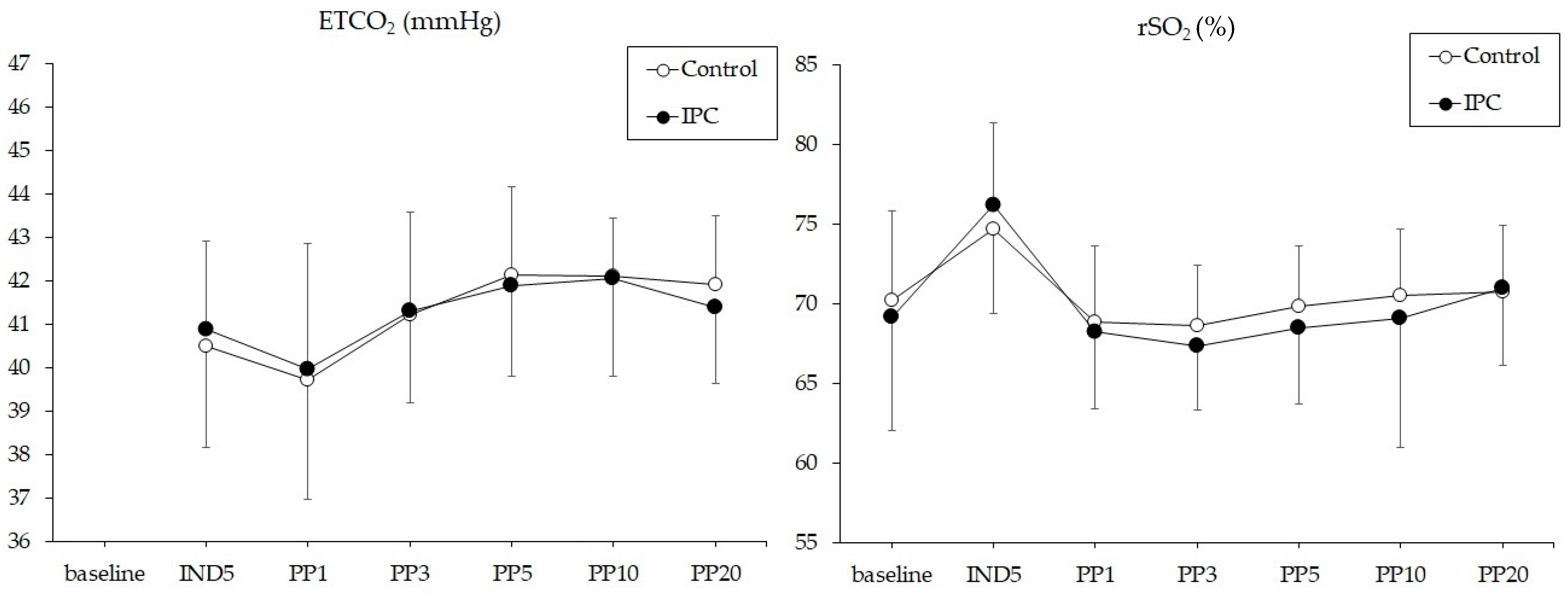
3.3. Chanages in ETCO2 and rSO2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shen, Q.; Hiebert, J.B.; Rahman, F.K.; Krueger, K.J.; Gupta, B.; Pierce, J.D. Understanding obesity-related high output heart failure and its implications. Int. J. Heart Fail. 2021, 3, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.A.; Chanderraj, R.; Gant, R.; Butler, C.; Frangos, S.; Maloney-Wilensky, E.; Faerber, J.; Kofke, W.A.; Levine, J.M.; LeRoux, P. Obesity is associated with reduced brain tissue oxygen tension after severe brain injury. Neurocrit. Care 2012, 16, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Cardim, D.; Robba, C.; Matta, B.; Tytherleigh-Strong, G.; Kang, N.; Schmidt, B.; Donnelly, J.; Calviello, L.; Smielewski, P.; Czosnyka, M. Cerebrovascular assessment of patients undergoing shoulder surgery in beach chair position using a multiparameter transcranial Doppler approach. J. Clin. Monit. Comput. 2019, 33, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.S.; Szokol, J.W.; Marymont, J.H.; Greenberg, S.B.; Avram, M.J.; Vender, J.S.; Vaughn, J.; Nisman, M. Cerebral oxygen desaturation events assessed by near-infrared spectroscopy during shoulder arthroscopy in the beach chair and lateral decubitus positions. Anesth. Analg. 2010, 111, 496–505. [Google Scholar] [CrossRef]
- Wang, L.; Yang, L.; Yang, J.; Shan, S. Effects of permissive hypercapnia on laparoscopic surgery for rectal carcinoma. Gastroenterol. Res. Pract. 2019, 2019, 3903451. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Cao, B.; Niu, L.; Cui, X.; Yu, H.; Liu, J.; Li, H.; Li, W. Effects of permissive hypercapnia on transient global cerebral ischemia-reperfusion injury in rats. Anesthesiology 2010, 112, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Khatri, A.; Davies, A.H.; Shalhoub, J. Mechanical prophylaxis for venous thromboembolism prevention in obese individuals. Phlebology 2021, 36, 768–770. [Google Scholar] [CrossRef] [PubMed]
- Kurukahvecioglu, O.; Sare, M.; Karamercan, A.; Gunaydin, B.; Anadol, Z.; Tezel, E. Intermittent pneumatic sequential compression of the lower extremities restores the cerebral oxygen saturation during laparoscopic cholecystectomy. Surg. Endosc. 2008, 22, 907–911. [Google Scholar] [CrossRef]
- Lim, H.; Kim, J.W.; Lee, K.; Seo, D.; Ko, S. Hemodynamic effects of different types of pneumatic compression of the lower extremities during anesthesia induction: A prospective randomized controlled trial. Korean J. Anesthesiol. 2018, 71, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Kiefer, N.; Theis, J.; Putensen-Himmer, G.; Hoeft, A.; Zenker, S. Peristaltic pneumatic compression of the legs reduces fluid demand and improves hemodynamic stability during surgery: A randomized, prospective study. Anesthesiology 2011, 114, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Kwak, H.J.; Lee, J.S.; Lee, D.C.; Kim, H.S.; Kim, J.Y. The effect of a sequential compression device on hemodynamics in arthroscopic shoulder surgery using beach-chair position. Arthroscopy 2010, 26, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Sorimachi, H.; Obokata, M.; Takahashi, N.; Reddy, Y.N.V.; Jain, C.C.; Verbrugge, F.H.; Koepp, K.E.; Khosla, S.; Jensen, M.D.; Borlaug, B.A. Pathophysiologic importance of visceral adipose tissue in women with heart failure and preserved ejection fraction. Eur. Heart J. 2021, 42, 1595–1605. [Google Scholar] [CrossRef]
- Shah, S.J.; Borlaug, B.A.; Kitzman, D.W.; McCulloch, A.D.; Blaxall, B.C.; Agarwal, R.; Chirinos, J.A.; Collins, S.; Deo, R.C.; Gladwin, M.T.; et al. Research priorities for heart failure with preserved ejection fraction: National Heart, Lung, and Blood Institute working group summary. Circulation 2020, 141, 1001–1026. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A.; Melenovsky, V.; Russell, S.D.; Kessler, K.; Pacak, K.; Becker, L.C.; Kass, D.A. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation 2006, 114, 2138–2147. [Google Scholar] [CrossRef]
- Comerota, A.J.; Chouhan, V.; Harada, R.N.; Sun, L.; Hosking, J.; Veermansunemi, R.; Comerota, A.J., Jr.; Schlappy, D.; Rao, A.K. The fibrinolytic effects of intermittent pneumatic compression: Mechanism of enhanced fibrinolysis. Ann. Surg. 1997, 226, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Sorimachi, H.; Burkhoff, D.; Verbrugge, F.H.; Omote, K.; Obokata, M.; Reddy, Y.N.V.; Takahashi, N.; Sunagawa, K.; Borlaug, B.A. Obesity, venous capacitance, and venous compliance in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2021, 23, 1648–1658. [Google Scholar] [CrossRef] [PubMed]
- Stepniakowski, K.; Egan, B.M. Additive effects of obesity and hypertension to limit venous volume. Am. J. Physiol. 1995, 268, R562–R568. [Google Scholar] [CrossRef]
- Alishahi, S.; Francis, N.; Crofts, S.; Duncan, L.; Bickel, A.; Cuschieri, A. Central and peripheral adverse hemodynamic changes during laparoscopic surgery and their reversal with a novel intermittent sequential pneumatic compression device. Ann. Surg. 2001, 233, 176–182. [Google Scholar] [CrossRef]
- Lv, H.; Xiong, C.; Wu, B.; Lan, Z.; Xu, D.; Duan, D.; Huang, X.; Guo, J.; Yu, S. Effects of targeted mild hypercapnia versus normocapnia on cerebral oxygen saturation in patients undergoing laparoscopic hepatectomy under low central venous pressure: A prospective, randomized controlled study. BMC Anesthesiol. 2023, 23, 257. [Google Scholar] [CrossRef] [PubMed]
- Park, C.G.; Jung, W.S.; Park, H.Y.; Kim, H.W.; Kwak, H.J.; Jo, Y.Y. Comparison of the effects of normocapnia and mild hypercapnia on the optic nerve sheath diameter and regional cerebral oxygen saturation in patients undergoing gynecological laparoscopy with total intravenous anesthesia. J. Clin. Med. 2021, 10, 4707. [Google Scholar] [CrossRef]
- Tsui, C.; Klein, R.; Garabrant, M. Minimally invasive surgery: National trends in adoption and future directions for hospital strategy. Surg. Endosc. 2013, 27, 2253–2257. [Google Scholar] [CrossRef] [PubMed]
- Kindel, T.; Latchana, N.; Swaroop, M.; Chaudhry, U.I.; Noria, S.F.; Choron, R.L.; Seamon, M.J.; Lin, M.J.; Mao, M.; Cipolla, J.; et al. Laparoscopy in trauma: An overview of complications and related topics. Int. J. Crit. Illn. Sci. 2015, 5, 196–205. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Control (n = 32) | IPC (n = 32) | p Value | |
|---|---|---|---|
| Age, years | 36 ± 8 | 32 ± 7 | 0.089 |
| Sex, M/F | 6/26 | 7/25 | 0.500 |
| Body mass index, kg/m2 | 38 ± 6 | 38 ± 5 | 0.825 |
| Anesthesia time, min | 183 ± 80 | 184 ± 81 | 0.969 |
| Operative time, min | 146 ± 74 | 146 ± 81 | 0.987 |
| Pneumoperitoneum time, min | 118 ± 71 | 120 ± 81 | 0.909 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, Y.Y.; Kim, S.M.; Park, C.G.; Kim, J.W.; Kwak, H.J. The Effect of Intermittent Pneumatic Compression on Hemodynamics and Regional Cerebral Oxygen Saturation in Laparoscopic Bariatric Surgery with Mild Hypercapnia in the Steep Reverse Trendelenburg Position. J. Pers. Med. 2024, 14, 405. https://doi.org/10.3390/jpm14040405
Jo YY, Kim SM, Park CG, Kim JW, Kwak HJ. The Effect of Intermittent Pneumatic Compression on Hemodynamics and Regional Cerebral Oxygen Saturation in Laparoscopic Bariatric Surgery with Mild Hypercapnia in the Steep Reverse Trendelenburg Position. Journal of Personalized Medicine. 2024; 14(4):405. https://doi.org/10.3390/jpm14040405
Chicago/Turabian StyleJo, Youn Yi, Seong Min Kim, Chun Gon Park, Ji Woong Kim, and Hyun Jeong Kwak. 2024. "The Effect of Intermittent Pneumatic Compression on Hemodynamics and Regional Cerebral Oxygen Saturation in Laparoscopic Bariatric Surgery with Mild Hypercapnia in the Steep Reverse Trendelenburg Position" Journal of Personalized Medicine 14, no. 4: 405. https://doi.org/10.3390/jpm14040405
APA StyleJo, Y. Y., Kim, S. M., Park, C. G., Kim, J. W., & Kwak, H. J. (2024). The Effect of Intermittent Pneumatic Compression on Hemodynamics and Regional Cerebral Oxygen Saturation in Laparoscopic Bariatric Surgery with Mild Hypercapnia in the Steep Reverse Trendelenburg Position. Journal of Personalized Medicine, 14(4), 405. https://doi.org/10.3390/jpm14040405