2.2.1. Cardiorespiratory Model
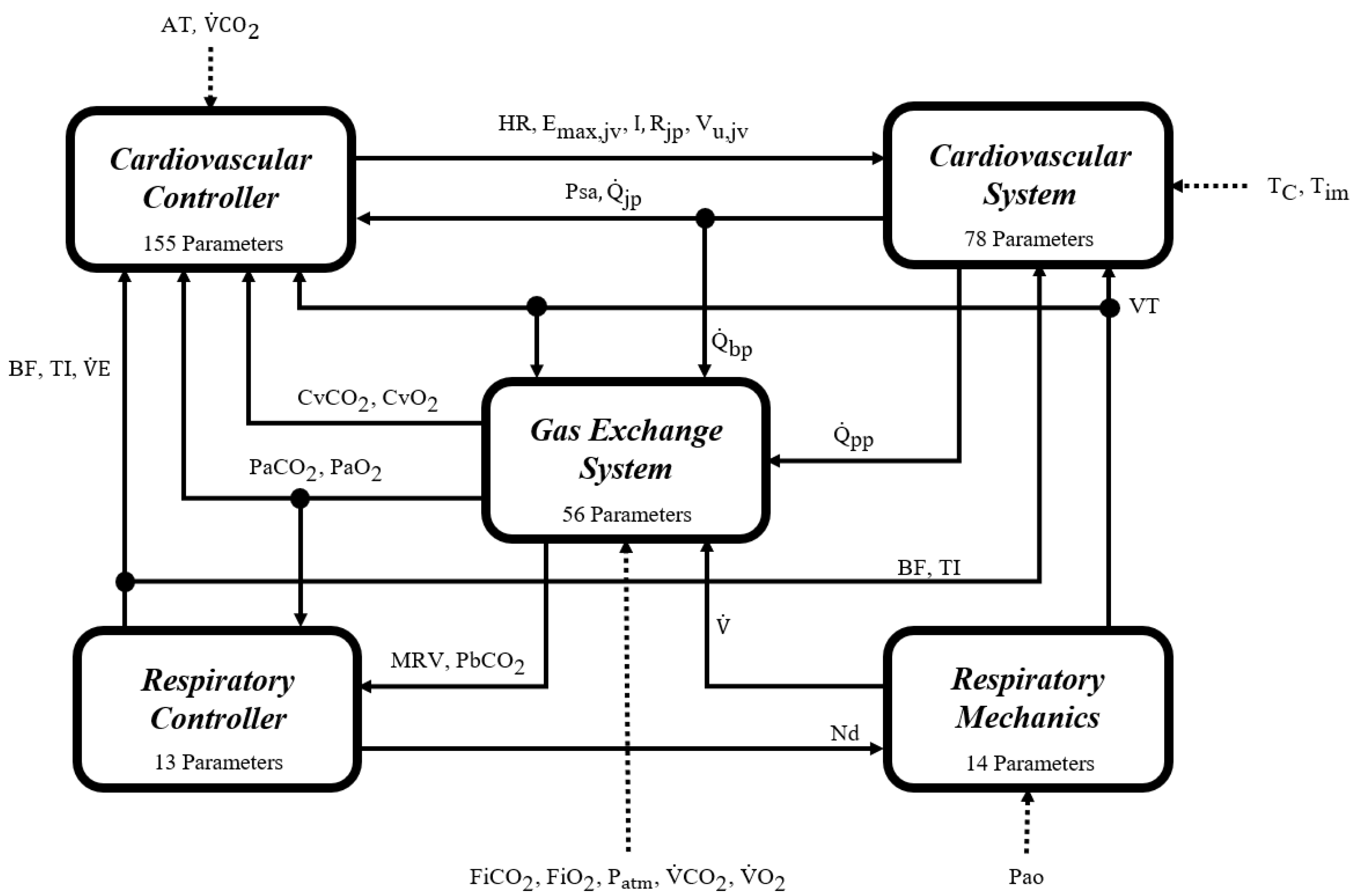
The mathematical cardiorespiratory model (CR model) used as a case study is a multi-compartmental self-regulated model of the cardiorespiratory system. It comprises 316 parameters and 170 equations distributed across different integrated mechanisms to represent the cardiovascular circulation system, the respiratory mechanic system, the gas exchange system, and the respiratory and cardiovascular controllers [
33]. It is the result of adapting previous models reported of systems, controllers, and mechanisms. It has been fitted and validated using experimental data from healthy adult individuals during rest and progressive aerobic exercise [
28].
Figure 3 delineates a schematic representation of the CR model, while
Table 1 provides detailed descriptions of the symbols utilized within the model diagram. These references constitute essential instruments for facilitating a deep and comprehensive exploration of the model’s framework.
The cardiovascular portion of the CR model encompasses a detailed representation of the heart and the circulatory system, including both pulmonary and systemic circulation. Its sophistication lies in the incorporation of various physiological aspects, such as the dynamics of blood flow through different valves and vascular beds. Notably, it incorporates modifications to accurately simulate moderate aerobic exercise, detailing the effects of muscle contractions and respiration on venous return.
The cardiovascular controller focuses on facilitating reflex control through a complex network of neural pathways and effector mechanisms. It adeptly responds to a range of stimuli, including changes in oxygen and carbon dioxide levels, thereby modulating cardiovascular responses during aerobic exercise.
The respiratory module of the CR model outlines the mechanics of the pulmonary and upper airway systems. This model segment has been enhanced to simulate the intricacies of muscle pressure waves and air movement during the respiratory cycle, effectively representing both the inspiratory and expiratory phases.
The gas exchange system provides a comprehensive depiction of the mechanisms governing the interaction between the cardiovascular system and respiratory mechanics, focusing on the regulation of blood gas concentrations. This system intricately details the processes involved in gas exchange, both at the cerebral and tissue levels, incorporating essential mechanisms that are particularly significant during exercise.
The respiratory controller in the CR1 model integrates the central and peripheral chemoreceptors and a metabolically related neural drive component. This setup, which utilizes inputs from the gas exchange system, facilitates precise estimation of the ventilatory demand, maintaining optimal arterial blood gas levels during physical activity. Additionally, it employs an optimization approach to adjust the breathing pattern each cycle, minimizing the work of breathing (WOB) and fine-tuning variables such as VT, BF, and inspiratory and expiratory times (TI and TE), thus ensuring nuanced regulation of respiratory control during exercise.
For a more in-depth understanding and exploration of the CR1 model, readers are encouraged to refer to the
Supplementary Materials. This material provides a comprehensive insight into the model, facilitating a deeper comprehension of its complexity and functionalities.
2.2.2. Experimental Data
The experimental data used to evaluate the strategy corresponded to signals and measurements from cardiorespiratory variables recorded in an observational and longitudinal study. This was based on an incremental, submaximal, and multistate cardiopulmonary exercise test performed using a programmable cycle ergometer under controlled environmental conditions. The test lasted for a total of 45 min, segmented into five distinct phases: rest (2 min), warm-up (4 min), active exercise (25 min), recovery phase (9 min), and concluding with a final resting period (5 min). During the exercise stage, five consecutive steps were carried out with load increments of 25 W every five minutes and at a constant pedaling speed of 60 RPM.
The recorded information was divided into two databases to analyze the usefulness of the dynamic fitting strategy from population-wide and personalized perspectives. The first database (DB1) corresponds to the longitudinal record of twenty-seven male adult volunteers at three different instants with more than six months of difference between them. The second database (DB2) corresponds to the records of three male adult volunteers matched by degree of consanguinity, medical history, and lifestyle but with different ages, which are proposed as an approximation of the longitudinal records of one same subject at six different stages of his life, consistent with the approach of stratified medicine [
42,
43]. These subjects are male members of the same family, corresponding to a father and his two sons who live together and have similar habits. The first two records correspond to the youngest subject, the next three to his brother, and the last to his father.
All the participants registered during the study were deemed healthy, encompassing individuals with diverse physical fitness levels, from sedentary to those regularly engaging in physical training. They were non-smokers and had no history or present symptoms of cardiovascular, pulmonary, metabolic, or neurological disorders. Additionally, none had pacemakers or any other types of implanted electrical stimulators. The records were composed of the signals of , TI, VT, BF, HR, oxygen uptake (), carbon dioxide output (), alveolar oxygen partial pressure () and alveolar carbon dioxide partial pressure () and measurements of systolic blood pressure (PS), diastolic blood pressure (PD), and mean arterial blood pressure (PM). The records also comprised characteristics of the environment, such as , , and .
Quantifiable information related to factors other than age reported significantly influencing the cardiorespiratory system was also recorded. These data accounted for habits such as diet [
35,
36], physical activity [
38,
39], and quality of sleep [
37,
44], related to measures of body mass index, average hours of weekly physical activity, and average hours of daily sleep, respectively. Other relevant factors, such as accidents or illnesses, habits such as smoking, or family history of diseases, were not reported, considering that they were regarded as exclusion criteria. Medication use was only reported by the oldest subject of the DB2 and was related to blood pressure control.
Table 2 presents the information recorded for each database related to the environmental conditions, the characteristics of the volunteers, and the factors mentioned above. The data shown for DB1 correspond to the mean and standard deviation of the measurements.
All the methods received authorization from the Ethical Committee for Human Research of the University Research Department (SIU) of the University of Antioquia (approval certificates 16-59-711, 17-59-711, and 18-59-711). These procedures adhered to the standards set by the Declaration of Helsinki. Written agreements were secured for every participant following a briefing on the experiment’s procedure and the associated risks.
2.2.3. Computational Implementation and Data Analysis
The measured values of
and
served as the model inputs to simulate exercise intensity levels. This method has been previously employed in simulating aerobic exercise within physiological models [
20,
45]. The rationale behind this approach is that the physiological response to such a stimulus is intrinsically linked to the metabolic rates of
uptake and
production, which are directly affected by the workload during exercise (the physiological model does not consider the workload as a model input).
The average of each measurement during the last minute for each subject (except for PS, PM, and PD) was used as a representative sample of each phase of the exercise test under steady-state conditions. The experimental data were constrained using as a reference, starting at 0.3 L/min, which corresponds to the resting state and consists of the minimum value observed across all the subjects’ records, and ending at the respective calculated value of AT because the model was defined only for aerobic exercise.
Each temporal fitting of the model parameter values references the parameter values from the most recent optimization result, except for the first fit of each database. In this case, the nominal values reported in [
33] are used, reflecting a traditional single-time fit approach.
Each stimulus level was simulated for 2000 s to guarantee steady-state conditions for all the evaluated variables, as reported in [
33]. The model’s steady-state responses were determined by calculating the mean values of each variable during the final minute of each simulated stimulus level.
The model simulations, data processing, and statistical tests were performed using SIMULINK/MATLAB® version R2023a. The computational specifics of the simulation were aligned with those documented for the model’s validation, utilizing the numerical solver ODE23 (Bogacki and Shampine BS23 algorithm for the solution of ordinary non-rigid differential equations) and a variable step size between and seconds. The simulations were conducted only once, as all the model equations are deterministic. Below, the specific implementation details for each procedure are outlined.
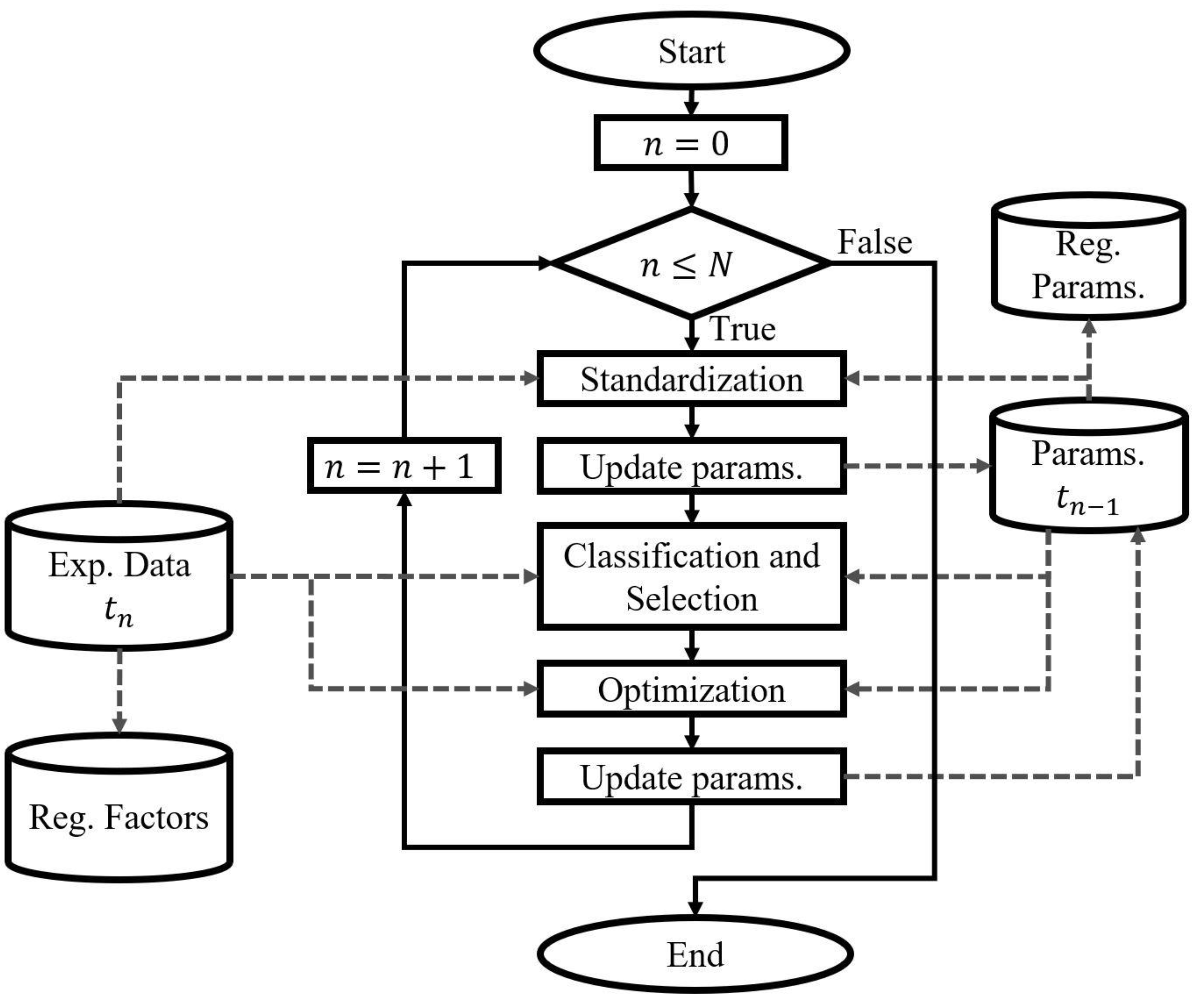
Time-Specific Fitting of the Physiological Model
Standardization of the simulation conditions
The parameters of the physiological model that were assigned according to the experimental data included
,
,
, basal respiratory tidal volume (
),
, total blood volume (
), and constant values of unstressed blood volume.
,
, and
, accounting for the environmental conditions, were considered constant in all the records and equal to 21.0379%, 0.0421%, and 640 mmHg, respectively. The values of
,
,
, and unstressed blood volume are associated with the distinct characteristics of the subjects. The value of
was determined from the VT measurements;
was calculated using the noninvasive technique v-slope [
23,
46].
in ml was also estimated for each record in relation to the body surface area (BSA) in
according to Equations (1) and (2) [
47]. Finally, the parameters related to the unstressed blood volumes were calculated using the proportion of their reported nominal values regarding
[
33].
The values of
,
, and
used for the standardization of each fit are presented in
Table 3. The data presented for DB1 correspond to the mean and standard deviation, except for
, whose value corresponds to the median and interquartile range considering the data distribution.
Classification and Selection of Parameters
Classification and selection of the parameters were performed based on the steady-state simulation results by applying changes in stimulus level and parameter value variations. Identical stimulus levels and parameter variations as those reported for the static fitting strategy previously applied to the same model were used [
28]. Three exercise stimulus levels were simulated using
and
as the model inputs, corresponding to states of rest, an intermediate level of exercise, and
. The identifiability and sensitivity of the model parameters selected by role (gain and thresholds) were evaluated throughout five uniformly distributed percentage variations in a range of ±5% of the reference value. The number of parameters selected was the same as that reported for the model according to the static fitting strategy.
The fitting approach related to the stimulus was not applied because it did not significantly decrease the prediction error, and the exercise mechanisms had already been fitted to the model [
28].
Parameter Optimization
The optimization algorithm implemented corresponds to the Covariance Matrix and Adaptation Evolution Strategy (CMA-ES). This stochastic global optimization algorithm is grounded in adaptive and evolutionary principles [
48,
49]. Its selection was based on its favorable outcomes in terms of the convergence speed, precision, and accuracy when fitting the case study model [
28] and other related ones [
27]. The parameter values applied in the implementation of the CMA-ES algorithm align with those reported for the model according to the static fitting strategy [
28].
The evaluation ranges for the parameter optimizations were defined in accordance with the static fitting strategy [
28]. The parameter values reported as nominal for the model were used as the variation references [
33]. A general evaluation range of ±30% regarding the nominal value was established and expanded to ±50% for weighting parameters unrelated to direct physiological measures. These ranges were modified according to the information reported about the optimization results or physiological sense (values with physiological justification).
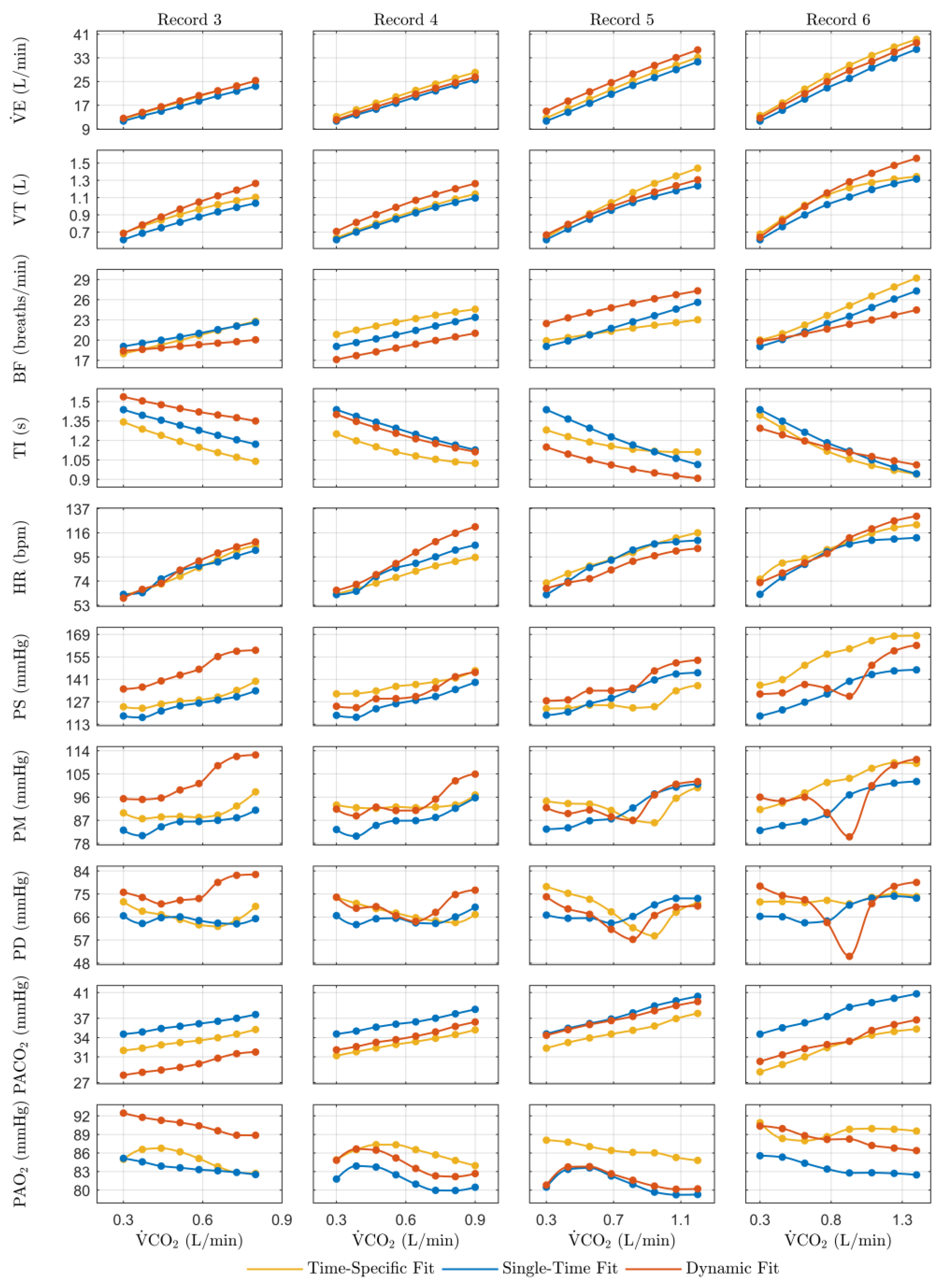
Steady-state model predictions of
, TI, VT, BF, HR,
,
, PS, PD, and PM for eight consecutive, equidistant, and incremental step values of
and
, spanning from rest to AT as the experimental data, were used for the parameter optimization. The cost function (CF) employed corresponds to Equation (3), utilizing the same root mean squared error (RMSE)-based metric as applied in the reported fitting of the case study model [
28].
where
and
correspond to the experimental and simulated values of the variable, respectively;
and K represent the number of variables and stimuli levels; and the subscripts i and k designate each specific variable and stimulus level.
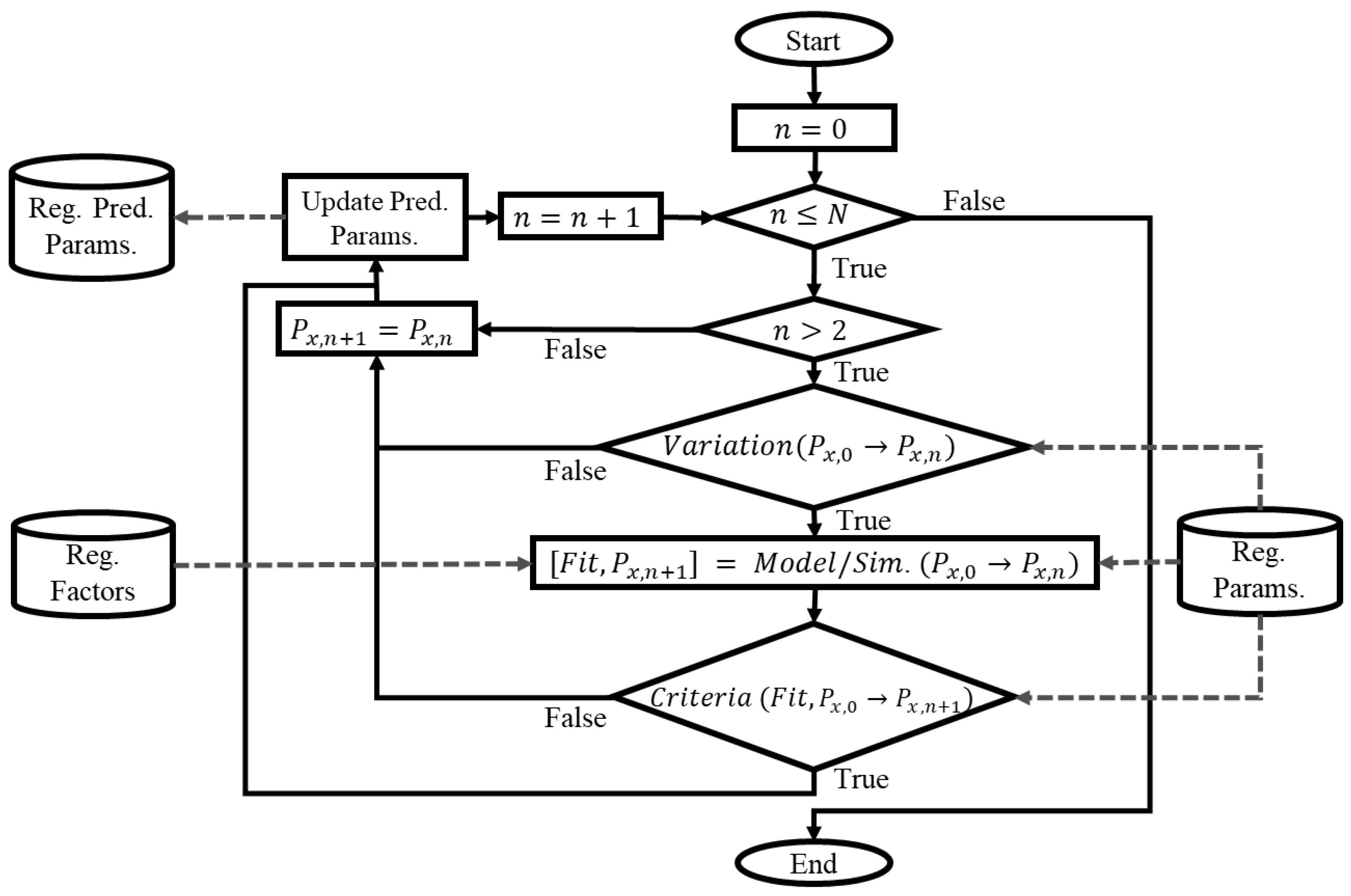
Dynamic Parameter Modeling
To effectively model a dynamic parameter, it is essential that the parameter has been optimized at least twice at two consecutive instants of time. Thus, for DB1, only the optimized parameter values of record three were predicted, while for DB2, the predictions encompassed the optimized parameter values from records three to six. Specifically, only the parameters demonstrating significant variations in their value during the optimization procedure were modeled as dynamic parameters. The remaining parameters retained their previous values, whether they were nominal, standardized, or previously optimized.
Deterministic and parametric MISO models were implemented for each dynamic parameter. The implemented model structure corresponded to an ARX model (autoregressive with exogenous input), selected to consider the effect of the past values of the outputs and inputs on the current value [
32]. Equation (4) corresponds to a representation of the model structure.
where
represents the parameter’s value at each instant of time;
is the
th input, which is associated with the factors evaluated; A and B are polynomials expressed in the time-shift operator
and are related to the parameter and the inputs, respectively;
is the total number of inputs;
is the input delay; and
is considered random noise.
For each model, the following inputs were used: the time elapsed between records, the average weekly physical activity, the average daily sleep hours (
Table 2), and AT (
Table 3). To calculate the time, the difference in age between each record was accumulated, and a value of zero for the first record was assigned. AT values have been used because they account for the metabolic response of the subject to cardiorespiratory changes [
46,
50]. Except for time, the values of the previous record’s inputs were considered equivalent to the values in the record to be predicted.
Different model orders associated with the polynomials were evaluated for each parameter, and the model with the best fit was selected. The past values of the parameters and the inputs were interpolated, considering that the design of the models requires constant sampling times. Sampling times between 0.1 and 0.4 years were evaluated in this work, considering the temporal difference between records for each fit. The orders of polynomials A and B were evaluated from zero to the maximum number of samples available.
, the input delay, was considered zero regarding all the inputs due to the limited number of available records. The coefficients of the polynomials for each model were estimated using the least-squares method. The best-order selection was based on applying Akaike’s Information Criterion (AIC) according to Equation (5).
where
is the loss function (normalized sum of squared prediction errors),
is the total number of parameters in the structure in question, and
is the number of data points used for the estimation.
Criteria based on the goodness of fit of the models and the variation in the predicted value regarding a bounded range were applied to evaluate the physiological justification for the predictions. Models with a goodness of fit of less than 60%, sign changes, or variations greater than 50% regarding the range of recorded values were discarded, and the values corresponding to the immediately previous record were used instead.
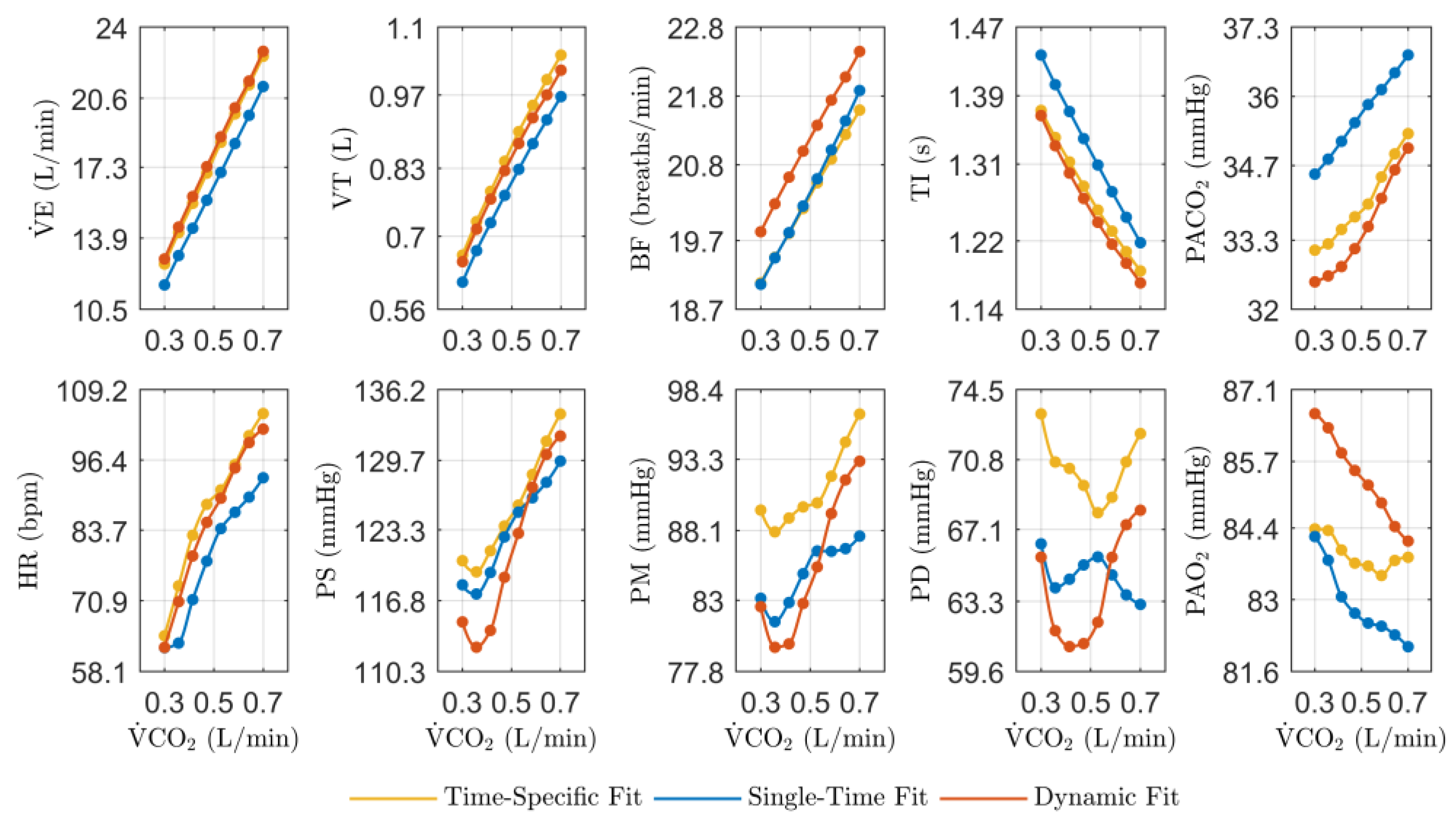
Validation
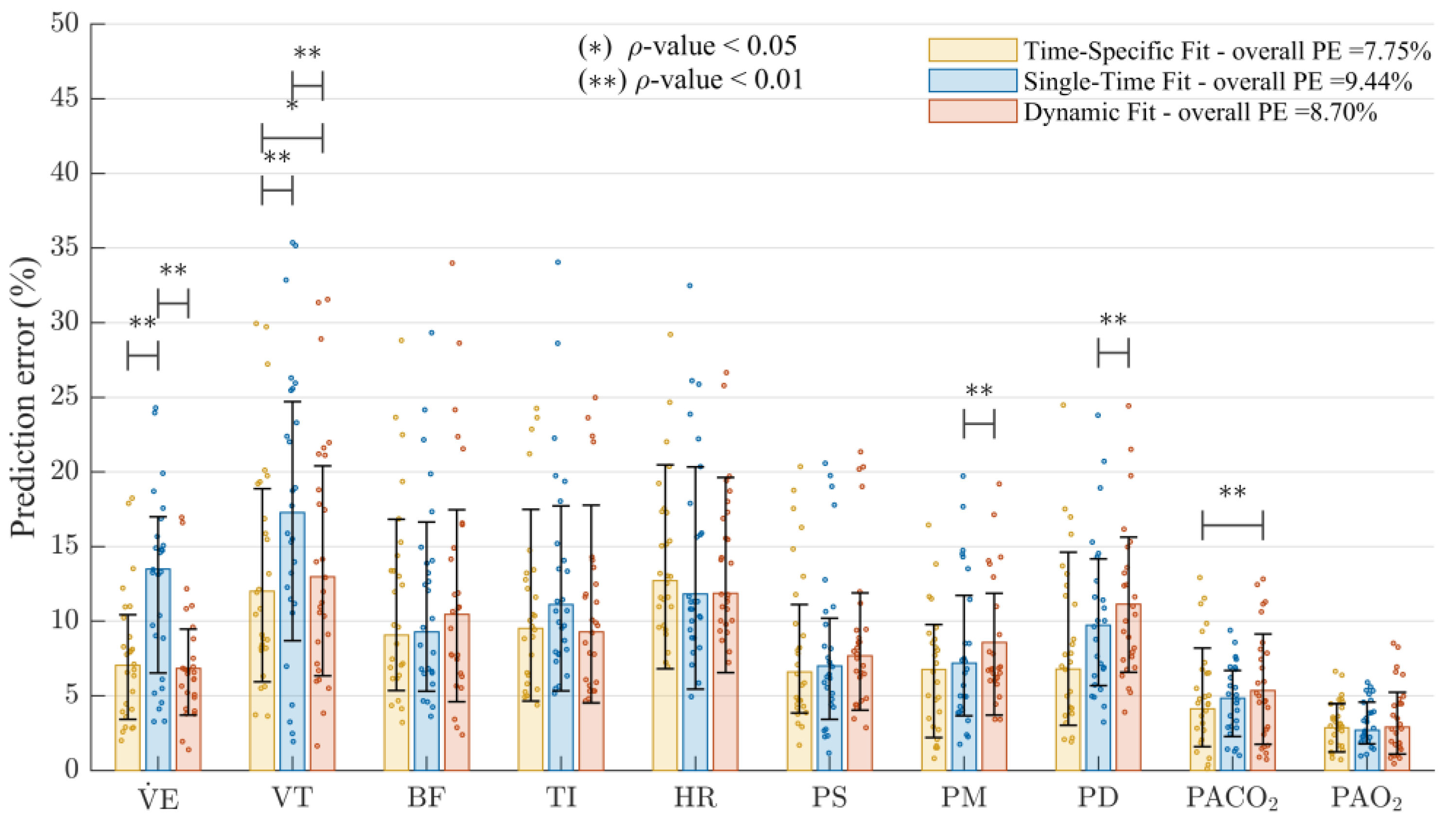
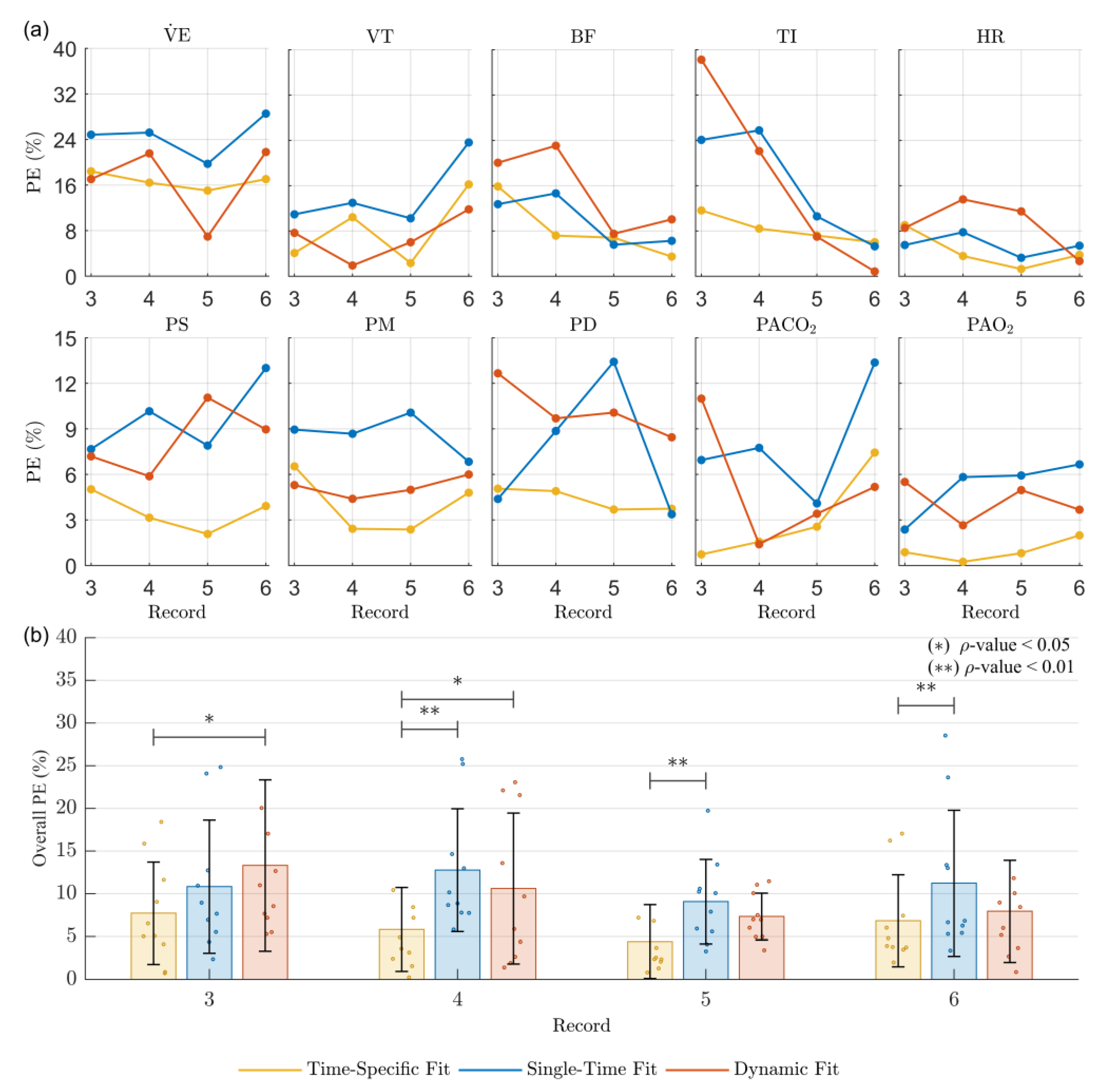
Validation consisted of comparing the simulation results of the case study model using (1) optimized parameter values for each record (time-specific fit approach), (2) nominal parameter values (single-time fit approach), and (3) predicted parameter values from the identified dynamic parameter models (dynamic parameter fit approach). These comparisons aimed to demonstrate the usefulness of the dynamic fitting strategy from the perspective of predicting the future state of the modeled system against the traditional approach of using the traditional population fit results at a single instant of time.
Prediction Error
For each approach, the effectiveness of the model performance was assessed by calculating the prediction error (PE) in relation to the steady-state experimental measures of the recorded cardiorespiratory variables (
, TI, VT, BF, HR,
,
, PS, PD, and PM) for eight incremental step values of
and
from rest to AT, as in the optimization process. The metric used to calculate the PE corresponds to Equation (6), a modification of the Mean Absolute Error (MAE) that allows an interpretation of the differences as a proportion of the experimental data. It considers the error for each subject, variable, and level of stimulus as follows:
where
is the experimental variable value;
is the simulation prediction value;
denotes the number of variables; and the subscripts i, j, and k are indexes that represent each subject, variable, and stimulus level, respectively.
Statistical Analysis
The Wilcoxon signed-rank statistical test was applied to evaluate whether the distributions of the PE results of the used fitting approaches were different. As a non-parametric test, the Wilcoxon signed-rank test is widely recommended for two populations when observations are paired [
51]. The test was applied between the PE results for all pairs of different approaches. The results were considered statistically significant for
values less than 0.01 (strong differences) and less than 0.05 (mild differences).
value results greater than 0.05 were not considered statistically different.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}