
Role of Cardiovascular Magnetic Resonance in Cardiac Amyloidosis: A Narrative Review

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Purpose of Review
3. Types of Cardiac Amyloidosis
4. Prevalence of Cardiac Amyloidosis
5. Diagnosis of Cardiac Amyloidosis
5.1. Invasive Diagnostic Criteria
5.2. Non-Invasive Diagnostic Criteria
6. Role of CMR
7. CMR Protocol
8. Semiotics of CMR
8.1. T1 Mapping
8.2. Extracellular Volume (ECV)
8.3. T2 Mapping
8.4. Late Gadolinium Enhancement (LGE)
8.4.1. LGE Acquisition Technique
8.4.2. CMR Sequences for LGE
- Two-dimensional segmented inversion recovery gradient echo (GRE) or b-SSFP, PSIR, or 3D sequences are preferred for patients with satisfactory breath-holding ability and adequate signal-to-noise ratio (SNR);
- Single-shot imaging (b-SSFP readout) can be performed as an optional second set or as a backup for patients with irregular heartbeat or difficulty holding their breath.
8.4.3. LGE Pattern
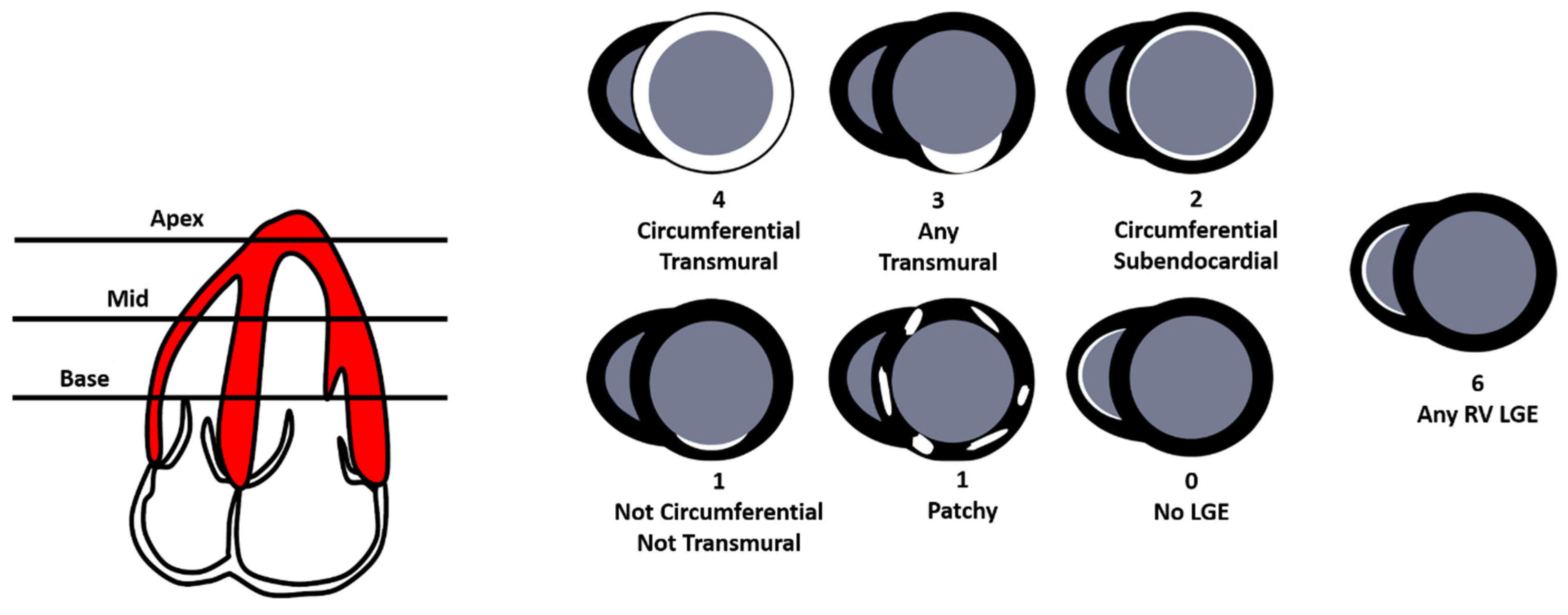
8.4.4. QALE Score
9. Assessment of Prognosis
10. Limitations of CMR
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Aimo, A.; Merlo, M.; Porcari, A.; Georgiopoulos, G.; Pagura, L.; Vergaro, G.; Sinagra, G.; Emdin, M.; Rapezzi, C. Redefining the epidemiology of cardiac amyloidosis. A systematic review and meta-analysis of screening studies. Eur. J. Heart Fail. 2022, 24, 2342–2351. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Hawkins, P.N.; Fontana, M. Cardiac amyloidosis. Clin. Med. 2018, 18, s30–s35. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis. A position statement of the European Society of Cardiology Working Group on myocardial and Pericardial Diseases. Eur. J. Heart Fail. 2021, 23, 512–526. [Google Scholar] [CrossRef]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.W.J.M.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: Part 1 of 2-evidence base and standardized methods of imaging. J. Nucl. Cardiol. 2019, 26, 2065–2123. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Yilmaz, A.; Bauersachs, J.; Bengel, F.; Büchel, R.; Kindermann, I.; Klingel, K.; Knebel, F.; Meder, B.; Morbach, C.; Nagel, E.; et al. Diagnosis and treatment of cardiac amyloidosis: Position statement of the German Cardiac Society (DGK). Clin. Res. Cardiol. 2021, 110, 479–506. [Google Scholar] [CrossRef]
- Fine, N.M.; Davis, M.K.; Anderson, K.; Delgado, D.H.; Giraldeau, G.; Kitchlu, A.; Massie, R.; Narayan, J.; Swiggum, E.; Venner, C.P.; et al. Canadian Cardiovascular Society/Canadian Heart Failure Society Joint Position Statement on the Evaluation and Management of Patients with Cardiac Amyloidosis. Can. J. Cardiol. 2020, 36, 322–334. [Google Scholar] [CrossRef]
- O’meara, E.; McDonald, M.; Chan, M.; Ducharme, A.; Ezekowitz, J.A.; Giannetti, N.; Grzeslo, A.; Heckman, G.A.; Howlett, J.G.; Koshman, S.L.; et al. CCS/CHFS Heart Failure Guidelines: Clinical Trial Update on Functional Mitral Regurgitation, SGLT2 Inhibitors, ARNI in HFpEF, and Tafamidis in Amyloidosis. Can. J. Cardiol. 2020, 36, 159–169. [Google Scholar] [CrossRef]
- Kittleson, M.M.; Maurer, M.S.; Ambardekar, A.V.; Bullock-Palmer, R.P.; Chang, P.P.; Eisen, H.J.; Nair, A.P.; Nativi-Nicolau, J.; Ruberg, F.L. Cardiac Amyloidosis: Evolving Diagnosis and Management: A Scientific Statement from the American Heart Association. Circulation 2020, 142, e7–e22. [Google Scholar] [CrossRef] [PubMed]
- Kittleson, M.M.; Maurer, M.S.; Ambardekar, A.V.; Bullock-Palmer, R.P.; Chang, P.P.; Eisen, H.J.; Nair, A.P.; Nativi-Nicolau, J.; Ruberg, F.L. Addendum to: Cardiac Amyloidosis: Evolving Diagnosis and Management: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e10. [Google Scholar]
- Kitaoka, H.; Izumi, C.; Izumiya, Y.; Inomata, T.; Ueda, M.; Kubo, T.; Koyama, J.; Sano, M.; Sekijima, Y.; Tahara, N.; et al. JCS 2020 Guideline on Diagnosis and Treatment of Cardiac Amyloidosis. Circ. J. 2020, 84, 1610–1671. [Google Scholar] [CrossRef]
- Rapezzi, C.; Aimo, A.; Serenelli, M.; Barison, A.; Vergaro, G.; Passino, C.; Panichella, G.; Sinagra, G.; Merlo, M.; Fontana, M.; et al. Critical Comparison of Documents from Scientific Societies on Cardiac Amyloidosis: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 79, 1288–1303. [Google Scholar] [CrossRef] [PubMed]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar] [CrossRef] [PubMed]
- Razvi, Y.; Patel, R.K.; Fontana, M.; Gillmore, J.D. Cardiac Amyloidosis: A Review of Current Imaging Techniques. Front. Cardiovasc. Med. 2021, 8, 751293. [Google Scholar] [CrossRef]
- Boretto, P.; Patel, N.H.; Patel, K.; Rana, M.; Saglietto, A.; Soni, M.; Ahmad, M.; Ying Ho, J.S.; De Filippo, O.; Providencia, R.A.; et al. Prognosis prediction in cardiac amyloidosis by cardiac magnetic resonance imaging: A systematic review with meta-analysis. Eur. Heart J. Open 2023, 3, oead092. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J Cardiovasc. Magn. Reson. 2020, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Aquaro, G.D.; Camastra, G.; Monti, L.; Lombardi, M.; Pepe, A.; Castelletti, S.; Maestrini, C.; Todiere, G.; Masci, P.; di Giovine, G.; et al. Reference values of cardiac volumes, dimensions, and new functional parameters by MR: A multicenter, multivendor study. J. Magn. Reson. Imaging 2017, 45, 1055–1067. [Google Scholar] [CrossRef] [PubMed]
- Peretto, G.G.; Barison, A.; Forleo, C.; Di Resta, C.; Esposito, A.; Aquaro, G.D.; Scardapane, A.; Palmisano, A.; Emdin, M.; Resta, N.; et al. Late gadolinium enhancement role in arrhythmic risk stratification of patients with LMNA cardiomyopathy: Results from a long-term follow-up multicentre study. Europace 2020, 22, 1864–1872. [Google Scholar] [CrossRef]
- Fattori, R.; Rocchi, G.; Celletti, F.; Bertaccini, P.; Rapezzi, C.; Gavelli, G. Contribution of magnetic resonance imaging in the differential diagnosis of cardiac amyloidosis and symmetric hypertrophic cardiomyopathy. Am. Heart J. 1998, 136, 824–830. [Google Scholar] [CrossRef]
- Vanden Driesen, R.I.; Slaughter, R.E.; Strugnell, W.E. MR findings in cardiac amyloidosis. AJR Am. J. Roentgenol. 2006, 186, 1682–1685. [Google Scholar] [CrossRef]
- Fontana, M.; Banypersad, S.M.; Treibel, T.A.; Maestrini, V.; Sado, D.M.; White, S.K.; Pica, S.; Castelletti, S.; Piechnik, S.K.; Robson, M.D.; et al. Native T1 mapping in transthyretin amyloidosis. J. Am. Coll. Cardiol. Imaging 2014, 7, 157–165. [Google Scholar] [CrossRef]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75, Erratum in J. Cardiovasc. Magn. Reson. 2018, 20, 9. [Google Scholar] [CrossRef] [PubMed]
- Karamitsos, T.D.; Piechnik, S.K.; Banypersad, S.M.; Fontana, M.; Ntusi, N.B.; Ferreira, V.M.; Whelan, C.K.; Myerson, S.G.; Robson, M.D.; Hawkins, P.N.; et al. Noncontrast T1 mapping for the diagnosis of cardiac Amyloidosis. J. Am. Coll. Cardiol. Imaging 2013, 6, 488–497. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Abdel-Gadir, A.; Treibel, T.A.; Zumbo, G.; Knight, D.S.; Rosmini, S.; Lane, T.; Mahmood, S.; Sachchithanantham, S.; Whelan, C.J.; et al. CMR-verified regression of cardiac AL amyloid after chemotherapy. J. Am. Coll. Cardiol. Imaging 2018, 11, 152–154. [Google Scholar] [CrossRef]
- Fontana, M.; Banypersad, S.M.; Treibel, T.A.; Abdel-Gadir, A.; Maestrini, V.; Lane, T.; Gilbertson, J.A.; Hutt, D.F.; Lachmann, H.J.; Whelan, C.J.; et al. Differential myocyte responses in patients with cardiac transthyretin amyloidosis and light-chain amyloidosis: A cardiac MR imaging study. Radiology 2015, 277, 388–397. [Google Scholar] [CrossRef]
- Banypersad, S.M.; Fontana, M.; Maestrini, V.; Sado, D.M.; Captur, G.; Petrie, A.; Piechnik, S.K.; Whelan, C.J.; Herrey, A.S.; Gillmore, J.D.; et al. T1 mapping and survival in systemic light-chain amyloidosis. Eur. Heart J. 2015, 36, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Mongeon, F.P.; Jerosch-Herold, M.; Coelho-Filho, O.R.; Blankstein, R.; Falk, R.H.; Kwong, R.Y. Quantification of extracellular matrix expansion by CMR in infiltrative heart disease. J. Am. Coll. Cardiol. Imaging 2012, 5, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Ridouani, F.; Damy, T.; Tacher, V.; Derbel, H.; Legou, F.; Sifaoui, I.; Audureau, E.; Bodez, D.; Rahmouni, A.; Deux, J.F. Myocardial native T2 measurement to differentiate light-chain and transthyretin cardiac amyloidosis and assess prognosis. J. Cardiovasc. Magn. Reson. 2018, 20, 58. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, T.; Martinez-Naharro, A.; Treibel, T.A.; Francis, R.; Nordin, S.; Abdel-Gadir, A.; Knight, D.S.; Zumbo, F.; Rosmini, S.; Maestrini, V.; et al. Myocardial edema and prognosis in amyloidosis. J. Am. Coll. Cardiol. 2018, 71, 2919–2931. [Google Scholar] [CrossRef]
- Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; Verani, M.S.; et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 2002, 105, 539–542. [Google Scholar] [PubMed]
- Maceira, A.M.; Joshi, J.; Prasad, S.K.; Moon, J.C.; Perugini, E.; Harding, I.; Sheppart, M.N.; Poole-Wilson, P.A.; Nigel Hawkins, P.; Pennell, D.J. Cardiovascular magnetic resonance in cardiac amyloidosis. Circulation 2005, 111, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Pica, S.; Reant, P.; Abdel-Gadir, A.; Treibel, T.A.; Banypersad, S.M.; Maestrini, V.; Barcella, W.; Rosmini, S.; Bulluck, H.; et al. Prognostic value of late gadolinium enhancement cardiovascular magnetic resonance in cardiac amyloidosis. Circulation 2015, 132, 1570–1579. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Treibel, T.A.; Abdel-Gadir, A.; Bulluck, H.; Zumbo, G.; Knight, D.S.; Kotecha, T.; Fancis, E.; Hutt, D.F.; Rezk, T.; et al. Magnetic resonance in transthyretin cardiac amyloidosis. J. Am. Coll. Cardiol. 2017, 70, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Tian, Z.; Fang, Q. Diagnostic accuracy of cardiovascular magnetic resonance for patients with suspected cardiac amyloidosis: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2016, 16, 129. [Google Scholar] [CrossRef] [PubMed]
- Vermes, E.; Carbone, I.; Friedrich, M.G.; Merchant, N. Patterns of myocardial late enhancement: Typical and atypical features. Arch. Cardiovasc. Dis. 2012, 105, 300–308. [Google Scholar] [CrossRef]
- Dungu, J.N.; Valencia, O.; Pinney, J.H.; Gibbs, S.D.; Rowczenio, D.; Gilbertson, J.A.; Lachmann, H.J.; Wechalekar, A.; Gillmore, J.D.; Whelan, C.J.; et al. CMR-based differentiation of AL and ATTR cardiac amyloidosis. JACC Cardiovasc. Imaging 2014, 7, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Chatzantonis, G.; Bietenbeck, M.; Elsanhoury, A.; Tschöpe, C.; Pieske, B.; Tauscher, G.; Vietheer, J.; Shomanova, Z.; Mahrholdt, H.; Rolf, A.; et al. Diagnostic value of cardiovascular magnetic resonance in comparison to endomyocardial biopsy in cardiac amyloidosis: A multi-centre study. Clin. Res. Cardiol. 2021, 110, 555–568. [Google Scholar] [CrossRef] [PubMed]
- Abulizi, M.; Sifaoui, I.; Wuliya-Gariepy, M.; Kharoubi, M.; Israël, J.M.; Emsen, B.; Bodez, D.; Monnet, A.; Didierlaurent, D.; Tacher, V.; et al. 18F-sodium fluoride PET/MRI myocardial imaging in patients with suspected cardiac amyloidosis. J. Nucl. Cardiol. 2021, 28, 1586–1595. [Google Scholar] [CrossRef]
- Wan, K.; Sun, J.; Han, Y.; Liu, H.; Yang, D.; Li, W.; Wang, J.; Cheng, W.; Zhang, Q.; Zeng, Z.; et al. Increased Prognostic Value of Query Amyloid Late Enhancement Score in Light-Chain Cardiac Amyloidosis. Circ. J. 2018, 82, 739–746. [Google Scholar] [CrossRef]
- Kwong, R.Y.; Jerosch-Herold, M. CMR and amyloid cardiomyopathy: Are we getting closer to the biology? JACC Cardiovasc. Imaging 2014, 7, 166–168. [Google Scholar] [CrossRef]
- Raina, S.; Lensing, S.Y.; Nairooz, R.S.; Pothineni, N.V.K.; Hakeem, A.; Bhatti, S.; Pandey, T. Prognostic value of late gadolinium enhancement CMR in systemic amyloidosis. JACC Cardiovasc. Imaging 2016, 9, 1267–1277. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Naharro, A.; Kotecha, T.; Norrington, K.; Boldrini, M.; Rezk, T.; Quarta, C.; Treibel, T.A.; Whelan, C.J.; Knight, D.S.; Kellman, P.; et al. Native T1 and extracellular volume in transthyretin amyloidosis. JACC Cardiovasc. Imaging 2019, 12, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-6/Clinical-Utilities-of-cardiac-MRI (accessed on 16 March 2024).
- Available online: https://www.esur.org/esur-guidelines-on-contrast-agents/ (accessed on 16 March 2024).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis Criteria for Cardiac Amyloidosis | |||
|---|---|---|---|
| All types | Only ATTR (with absent monoclonal protein) | ||
| Positive cardiac biopsy | Positive extracardiac biopsy + Echocardiographic/CMR features | Grade 2 or 3 cardiac uptake at scintigraphy + Echocardiographic/CMR features | |
| * | |||
| Echocardiography Criteria | |
|---|---|
| Unexplained LV Thickness (>_12 mm) | |
| At least 2 of: -Grade 2 or worse diastolic dysfunction -sI, eI and aI waves velocities <5 cm/s at tissue Doppler -Global longitudinal LV strain absolute value < −15% | Score ≥ 8 points: -(IVS wall thickness + PWT)/LVEDD > 0.6 3 points -Doppler E wave/eI wave velocities > 11 1 point -TAPSE ≤ 19 mm 2 points -LV global longitudinal strain absolute value ≤ −13% 1 point -Systolic longitudinal strain apex to base ratio > 2.9 3 points |
| CMR Criteria |
|---|
| Characteristic CMR findings (a and b have to be present): |
|
| CMR PROTOCOL | ||
|---|---|---|
| Sequence technique | Note | |
| Cine function | b-SSFP ECG gated | Short-axis, 2-chamber, 3-chamber, 4-chamber |
| T1 mapping pre-contrast (Native T1) | Quality controlled T1 mapping sequence | Mid and basal short-axis and apical 4-chamber views |
| Myocardial edema | STIR | Short-axis |
| Gadolinium-based non-protein bound cyclic contrast agent (0.1–0.2 mmol/kg) | ||
| T1 mapping post-contrast (ECV estimation) | Quality controlled T1 mapping sequence | Mid and basal short-axis and apical 4-chamber Should be acquired at least 10-min postcontrast |
| LGE | TI scout + PSIR | Short-axis, 2-chamber, 3-chamber, 4-chamber |
| CMR FINDINGS | |
|---|---|
| LV Function and Morphology | |
| LV function | Preserved or reduced LV systolic function |
| (LV ejection fraction < 60%) | |
| LV wall thickening | LV global wall thickening |
| (>12 mm) | |
| LV end-diastolic volume | Reduced end-diastolic volume |
| (<90 mL) | |
| LV stroke volume index | Reduced LV stroke volume index |
| (<35 mL/m2) | |
| Atrial size | Biatrial enlargement |
| (left atrium > 41 mm, right atrium > 44 mm) | |
| Atrial septum thickening | atrial septum thickening |
| (≥6 mm) | |
| Pericardial effusion | Pericardial effusion |
| Amyloid imaging | |
| LGE imaging | Abnormal LGE Pattern |
| Diffuse LGE | |
| Subendocardial LGE | |
| Patchy LGE | |
| Dark blood pool signal * | |
| Amyloid quantification | |
| T1 mapping pre-contrast (Native T1) | Abnormal T1 mapping. Native T1 values are increased in areas of amyloid infiltration |
| T1 mapping post-contrast (ECV estimation) | Values of ECV > 40% are highly suggestive of CA. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maggialetti, N.; Torrente, A.; Lorusso, G.; Villanova, I.; Ficco, M.; Gravina, M.; Ferrari, C.; Giordano, L.; Granata, V.; Rubini, D.; et al. Role of Cardiovascular Magnetic Resonance in Cardiac Amyloidosis: A Narrative Review. J. Pers. Med. 2024, 14, 407. https://doi.org/10.3390/jpm14040407
Maggialetti N, Torrente A, Lorusso G, Villanova I, Ficco M, Gravina M, Ferrari C, Giordano L, Granata V, Rubini D, et al. Role of Cardiovascular Magnetic Resonance in Cardiac Amyloidosis: A Narrative Review. Journal of Personalized Medicine. 2024; 14(4):407. https://doi.org/10.3390/jpm14040407
Chicago/Turabian StyleMaggialetti, Nicola, Andrea Torrente, Giovanni Lorusso, Ilaria Villanova, Michele Ficco, Matteo Gravina, Cristina Ferrari, Luca Giordano, Vincenza Granata, Dino Rubini, and et al. 2024. "Role of Cardiovascular Magnetic Resonance in Cardiac Amyloidosis: A Narrative Review" Journal of Personalized Medicine 14, no. 4: 407. https://doi.org/10.3390/jpm14040407
APA StyleMaggialetti, N., Torrente, A., Lorusso, G., Villanova, I., Ficco, M., Gravina, M., Ferrari, C., Giordano, L., Granata, V., Rubini, D., Lucarelli, N. M., Stabile Ianora, A. A., & Scardapane, A. (2024). Role of Cardiovascular Magnetic Resonance in Cardiac Amyloidosis: A Narrative Review. Journal of Personalized Medicine, 14(4), 407. https://doi.org/10.3390/jpm14040407