
Data on Ocrelizumab Treatment Collected by MS Patients in Germany Using Brisa App


Abstract
1. Introduction
2. Methods
2.1. Ethical Approval
2.2. Data Source
2.3. Inclusion Criteria of Study Cohort
2.4. Data Processing and Analysis
2.5. Statistical Methodology
3. Results
3.1. Demographic Characteristics of Users
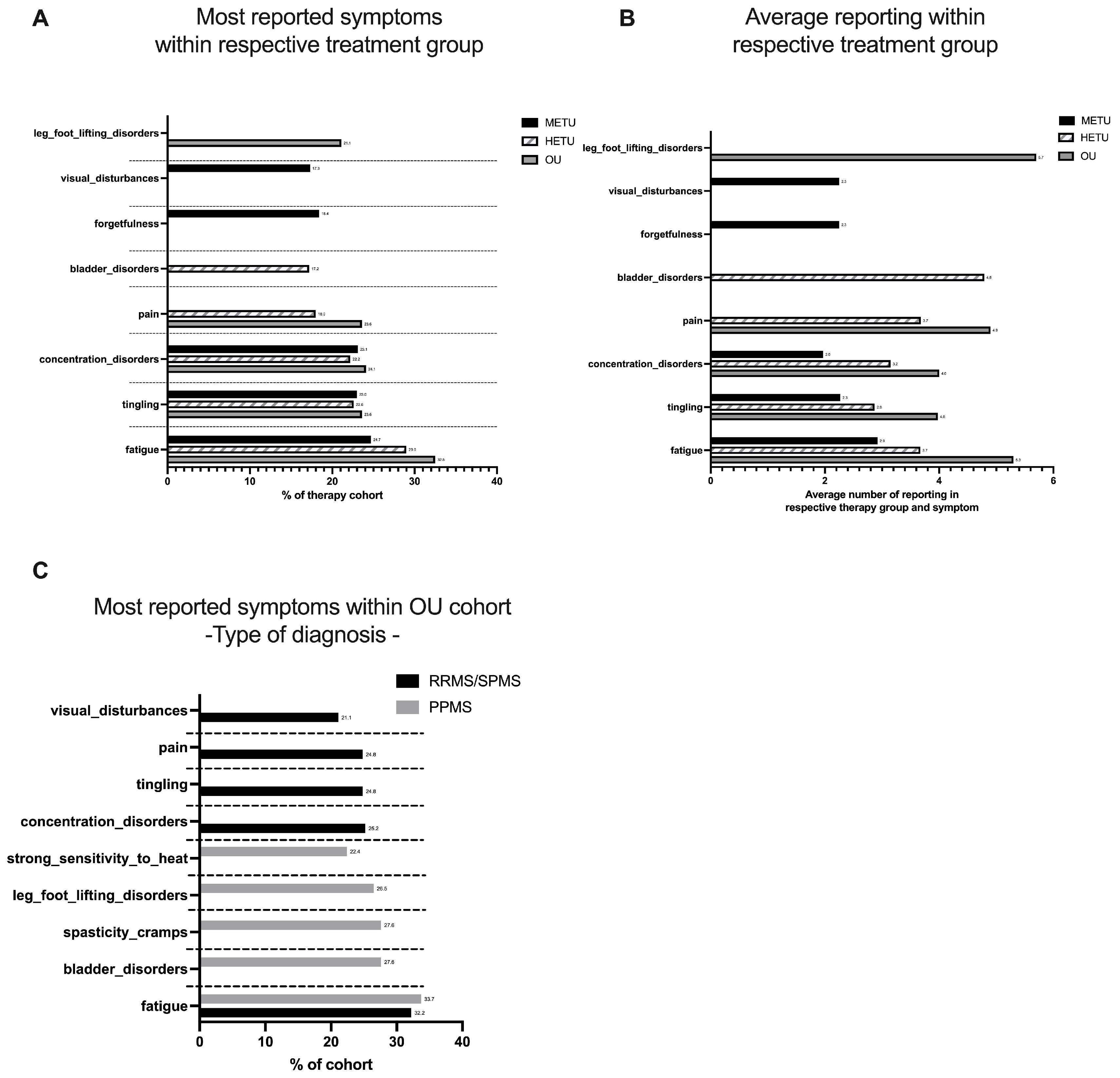
3.2. Symptoms Reported by the Different Treatment Groups
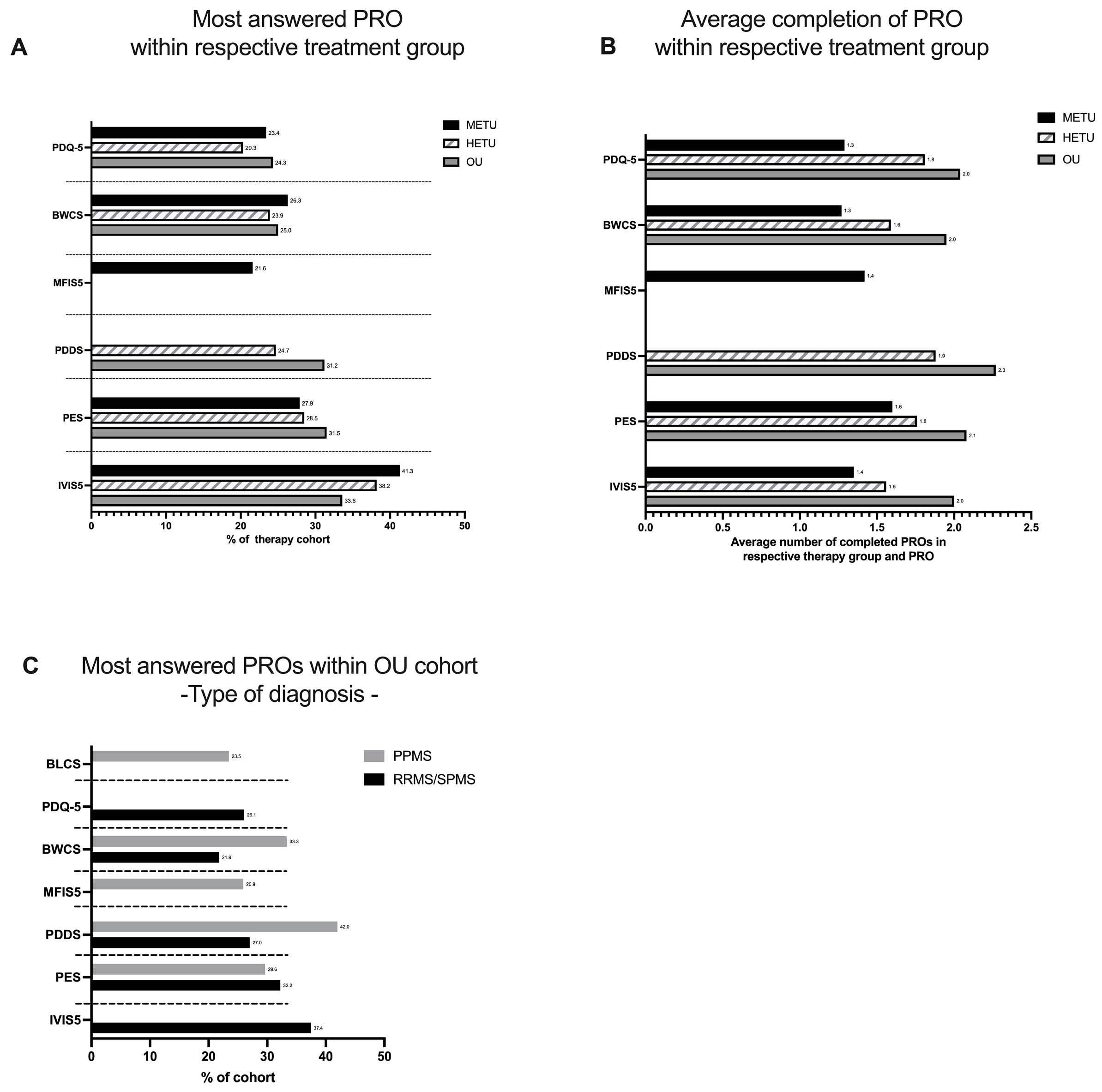
3.3. Top Five Completed Patient Reported Outcomes (PROs)
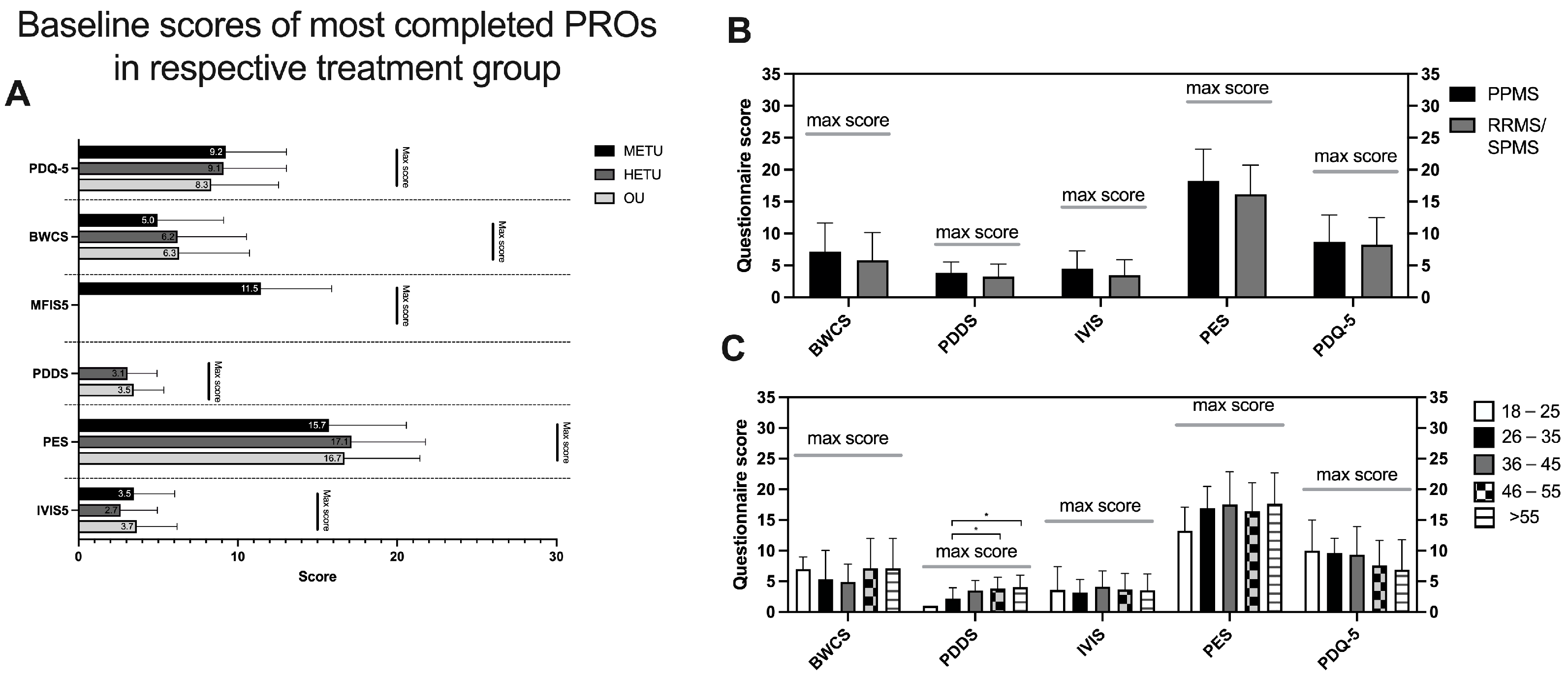
3.4. Baseline PRO Scores—All Patients vs. Ocrelizumab Users
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BDI-FS | Beck Depression Inventory—Fast Screen |
| BLCS | Bladder Control Scale |
| BWCS | Bowel Control Scale |
| DMT | disease-modifying therapy |
| EBV | Epstein–Barr virus |
| GDPR | General Data Protection Regulation |
| IVIS | Impact of Visual Impairment Scale |
| MFIS-5 | Modified Fatigue Impact Scale—5-Item Version |
| MS | multiple sclerosis |
| PDDS | Patient-Determined Disease Steps |
| PDQ-5 | Perceived Deficits Questionnaire—5-Item Version |
| PRO | patient-reported outcome |
| PES | MOS Pain Effects Scale |
| PPMS | primary progressive MS |
| RRMS | relapsing–remitting MS |
| RWE | real-world evidence |
| SPMS | secondary progressive MS |
| SSS | Sexual Satisfaction Scale |
References
- MS-in-EU-Access.pdf. Available online: https://emsp.org/wp-content/uploads/2021/06/MS-in-EU-access.pdf (accessed on 5 March 2022).
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. J. 2020, 26, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Scholz, M.; Haase, R.; Schriefer, D.; Voigt, I.; Ziemssen, T. Electronic Health Interventions in the Case of Multiple Sclerosis: From Theory to Practice. Brain Sci. 2021, 11, 180. [Google Scholar] [CrossRef] [PubMed]
- Dillenseger, A.; Weidemann, M.L.; Trentzsch, K.; Inojosa, H.; Haase, R.; Schriefer, D.; Voigt, I.; Scholz, M.; Akgün, K.; Ziemssen, T. Digital Biomarkers in Multiple Sclerosis. Brain Sci. 2021, 11, 1519. [Google Scholar] [CrossRef] [PubMed]
- Voigt, I.; Inojosa, H.; Wenk, J.; Akgün, K.; Ziemssen, T. Building a monitoring matrix for the management of multiple sclerosis. Autoimmun. Rev. 2023, 22, 103358. [Google Scholar] [CrossRef] [PubMed]
- Ziemssen, T.; Giovannoni, G.; Alvarez, E.; Bhan, V.; Hersh, C.; Hoffmann, O.; Oreja-Guevara, C.; Robles-Cedeño, R.R.; Trojano, M.; Vermersch, P.; et al. Multiple Sclerosis Progression Discussion Tool Usability and Usefulness in Clinical Practice: Cross-sectional, Web-Based Survey. J. Med. Internet Res. 2021, 23, e29558. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, E.; Haase, R.; Ziemssen, T. Review: Patient-reported outcomes in multiple sclerosis care. Mult. Scler. Relat. Disord. 2019, 33, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Rotstein, D.; Montalban, X. Reaching an evidence-based prognosis for personalized treatment of multiple sclerosis. Nat. Rev. Neurol. 2019, 15, 287–300. [Google Scholar] [CrossRef] [PubMed]
- Giovannoni, G. Disease-modifying treatments for early and advanced multiple sclerosis: A new treatment paradigm. Curr. Opin. Neurol. 2018, 31, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Simpson, A.; Mowry, E.M.; Newsome, S.D. Early Aggressive Treatment Approaches for Multiple Sclerosis. Curr. Treat. Options Neurol. 2021, 23, 19. [Google Scholar] [CrossRef] [PubMed]
- Tintoré, M. Early MS treatment. Int. MS J. 2007, 14, 5–10. [Google Scholar] [PubMed]
- Ziemssen, T.; Derfuss, T.; de Stefano, N.; Giovannoni, G.; Palavra, F.; Tomic, D.; Vollmer, T.; Schippling, S. Optimizing treatment success in multiple sclerosis. J. Neurol. 2016, 263, 1053–1065. [Google Scholar] [CrossRef] [PubMed]
- Inojosa, H.; Schriefer, D.; Ziemssen, T. Clinical outcome measures in multiple sclerosis: A review. Autoimmun. Rev. 2020, 19, 102512. [Google Scholar] [CrossRef] [PubMed]
- Hauser, S.L.; Cree, B.A.C. Treatment of Multiple Sclerosis: A Review. Am. J. Med. 2020, 133, 1380–1390. [Google Scholar] [CrossRef]
- Schriefer, D.; Haase, R.; Ettle, B.; Ziemssen, T. Patient- versus physician-reported relapses in multiple sclerosis: Insights from a large observational study. Eur. J. Neurol. 2020, 27, 2531–2538. [Google Scholar] [CrossRef]
- DGN One|Leitlinien Details. Available online: https://dgn.org/leitlinie/176 (accessed on 21 November 2022).
- Weber, M.S.; Buttmann, M.; Meuth, S.G.; Dirks, P.; Muros-Le Rouzic, E.; Eggebrecht, J.C.; Hieke-Schulz, S.; Leemhuis, J.; Ziemssen, T. Safety, Adherence and Persistence in a Real-World Cohort of German MS Patients Newly Treated With Ocrelizumab: First Insights From the CONFIDENCE Study. Front. Neurol. 2022, 13, 863105. [Google Scholar] [CrossRef]
- Balakrishnan, P.; Groenberg, J.; Jacyshyn-Owen, E.; Eberl, M.; Friedrich, B.; Joschko, N.; Ziemssen, T. Demographic Patterns of MS Patients Using BRISA: An MS-Specific App in Germany. J. Pers. Med. 2022, 12, 1100. [Google Scholar] [CrossRef] [PubMed]
- Mountford, S.; Kahn, M.; Balakrishnan, P.; Jacyshyn-Owen, E.; Eberl, M.; Friedrich, B.; Joschko, N.; Ziemssen, T. Correlation and differences of patient-reported outcomes vs. Likert-Rating of MS symptoms in a real-world cohort using a digital patient app. Digit. Health 2023, 9, 20552076231173520. [Google Scholar] [CrossRef]
- Wiendl, H.; Gold, R.; Berger, T.; Derfuss, T.; Linker, R.; Mäurer, M.; Aktas, O.; Baum, K.; Berghoff, M.; Bittner, S.; et al. Multiple Sclerosis Therapy Consensus Group (MSTCG): Position statement on disease-modifying therapies for multiple sclerosis (white paper). Ther. Adv. Neurol. Disord. 2021, 14, 17562864211039648. [Google Scholar] [CrossRef] [PubMed]
- Montalban, X.; Hauser, S.L.; Kappos, L.; Arnold, D.L.; Bar-Or, A.; Comi, G.; de Seze, J.; Giovannoni, G.; Hartung, H.-P.; Hemmer, B.; et al. Ocrelizumab versus Placebo in Primary Progressive Multiple Sclerosis. N. Engl. J. Med. 2017, 376, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Hauser, S.L.; Bar-Or, A.; Comi, G.; Giovannoni, G.; Hartung, H.-P.; Hemmer, B.; Lublin, F.; Montalban, X.; Rammohan, K.W.; Selmaj, K.; et al. Ocrelizumab versus Interferon Beta-1a in Relapsing Multiple Sclerosis. N. Engl. J. Med. 2017, 376, 221–234. [Google Scholar] [CrossRef]
- Buttmann, M.; Meuth, S.; Weber, M.; Dirks, P.; Eggebrecht, J.; Hieke-Schulz, S.; Leemhuis, J.; Ziemssen, T. The Real World Safety and Effectiveness of Ocrelizumab in Patients with Primary Progressive Multiple Sclerosis a CONFIDENCE Study Interim Analysis. Available online: https://medically.gene.com/global/en/unrestricted/neuroscience/ECTRIMS-2022/ectrims-2022-poster-buttmann-the-real-world-safety-and-.html (accessed on 28 February 2023).
- MS-Register Deutschland. Available online: https://www.msregister.de/ms-register/das-ms-register/ (accessed on 28 February 2023).
- Reber, S.; Scheel, J.; Stoessel, L.; Schieber, K.; Jank, S.; Lüker, C.; Vitinius, F.; Grundmann, F.; Eckardt, K.-U.; Prokosch, H.-U.; et al. Mobile Technology Affinity in Renal Transplant Recipients. Transplant. Proc. 2018, 50, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Miclea, A.; Salmen, A.; Zoehner, G.; Diem, L.; Kamm, C.P.; Chaloulos-Iakovidis, P.; Miclea, M.; Briner, M.; Kilidireas, K.; Stefanis, L.; et al. Age-dependent variation of female preponderance across different phenotypes of multiple sclerosis: A retrospective cross-sectional study. CNS Neurosci. Ther. 2019, 25, 527–531. [Google Scholar] [CrossRef] [PubMed]
- National MS Society. Available online: https://www.nationalmssociety.org/What-is-MS/Types-of-MS/Primary-progressive-MS (accessed on 28 March 2023).
- Ford, H. Clinical presentation and diagnosis of multiple sclerosis. Clin. Med. 2020, 20, 380–383. [Google Scholar] [CrossRef] [PubMed]
- MS Symptoms. National Multiple Sclerosis Society. Available online: https://www.nationalmssociety.org/Symptoms-Diagnosis/MS-Symptoms (accessed on 4 March 2022).
- Allen-Philbey, K.; Middleton, R.; Tuite-Dalton, K.; Baker, E.; Stennett, A.; Albor, C.; Schmierer, K. Can We Improve the Monitoring of People With Multiple Sclerosis Using Simple Tools, Data Sharing, and Patient Engagement? Front. Neurol. 2020, 11, 464. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, Y.C.; Motl, R.W.; Sandroff, B.M.; Pula, J.H.; Cadavid, D. Validation of patient determined disease steps (PDDS) scale scores in persons with multiple sclerosis. BMC Neurol. 2013, 13, 37. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Moderate-Efficacy Treatment Users (METUs) | High-Efficacy Treatment Users (HETUs) | Ocrelizumab Users (OUs) |
|---|---|---|
| Dimethylfumarate | Alemtuzumab | Ocrelizumab |
| Diroximelfumarate | Cladribine | |
| Glatirameracetate | Natalizumab | |
| Teriflunomide | Ofatumumab | |
| Interferons | S1P Modulators (Fingolimod, Ozanimod, Ponesimod) |
| Brisa Users (n = 1593) | Non-Ocrelizumab Users (n = 1188) | Ocrelizumab Users (n = 405) | ||||
|---|---|---|---|---|---|---|
| Gender | Female | Male | Divers | Female | Male | Divers |
| 1021 | 167 | 0 | 306 | 98 | 1 | |
| MS Type | SP | PP | RR | SP | PP | RR |
| 53 | 0 | 1135 | 42 | 108 | 255 | |
| OUs (n = 405) | HETUs (n = 884) | METUs (n = 709) | |
|---|---|---|---|
| Age group | |||
| 18–25 | 24 (5.9%) | 68 (7.7%) | 57 (8.0%) |
| 26–35 | 113 (27.9%) | 275(31.1%) | 241 (34.0%) |
| 36–45 | 105 (25.9%) | 251 (28.4%) | 207 (39.2%) |
| 46–55 | 105 (25.9%) | 204 (23.1%) | 143 (20.2%) |
| >55 | 58 (14.3%) | 86 (9.7%) | 61 (8.6%) |
| Time since diagnosis | |||
| 0–1 | 9 (2.2%) | 28 (3.2%) | 45 (6.3%) |
| 2–5 | 142 (35.1%) | 280 (31.7%) | 286 (40.3%) |
| 6–10 | 108 (26.7%) | 246 (27.8%) | 176 (24.8%) |
| 11–20 | 91 (22.5%) | 225 (25.5%) | 128 (18.1%) |
| 21–30 | 55 (13.6%) | 105 (11.9%) | 74 (10.4%) |
| RRMS | PPMS | |
|---|---|---|
| Age group | ||
| 18–25 | 22 (7.4%) | 2 (1.9%) |
| 26–35 | 104 (35.0%) | 9 (8.3%) |
| 36–45 | 81(27.3%) | 24 (22.2%) |
| 46–55 | 64 (21.5%) | 41(38.0%) |
| >55 | 26 (8.8%) | 32 (29.6%) |
| Time since diagnosis | ||
| 0–1 | 6 (2.0%) | 3 (2.8%) |
| 2–5 | 112 (37.7%) | 56 (51.9%) |
| 6–10 | 75 (25.3%) | 24 (22.2) |
| 11–20 | 64 (21.5%) | 15 (13.9) |
| 21–30 | 40 (13.5%) | 10 (9.3) |
| Age Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Symptom | 18–25 (n = 23) | 26–35 (n = 103) | 36–45 (n = 96) | 46–55 (n = 98) | >56 (n = 48) | |||||
| n | % of Age Group | n | % of Age Group | n | % of Age Group | n | % of Age Group | n | % of Age Group | |
| Fatigue | 10 | 43.5 | 26 | 25.2 | 34 | 35.4 | 33 | 33.7 | 17 | 35.4 |
| Numbness | 7 | 30.4 | ||||||||
| Pain | 7 | 30.4 | 21 | 20.4 | 23 | 24.0 | 26 | 26.5 | ||
| Bladder disorder | 5 | 21.7 | 12 | 25.0 | ||||||
| Depression | 5 | 21.4 | ||||||||
| Tingling | 22 | 21.4 | 28 | 28.6 | 12 | 25.0 | ||||
| Concentration disorder | 29 | 28.2 | 24 | 25.0 | ||||||
| Visual disturbances | 20 | 19.4 | ||||||||
| Strong sensitivity to heat | 28 | 29.2 | ||||||||
| Spasticity/cramps | 25 | 26.0 | 26 | 26.5 | 14 | 29.2 | ||||
| Leg foot lifting disorder | 25 | 25.5 | 15 | 31.3 | ||||||
| Age Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PRO | 18–25 (n = 18) | 26–35 (n = 79) | 36–45 (n = 73) | 46–55 (n = 76) | >56 (n = 48) | |||||
| n | % of Age Group | n | % of Age Group | n | % of Age Group | n | % of Age Group | n | % of Age Group | |
| PES (pain) | 8 | 44.4 | 16 | 20.3 | 26 | 35.6 | 30 | 39.5 | 12 | 25.0 |
| IVIS (vision) | 5 | 27.8 | 28 | 35.4 | 33 | 45.2 | 21 | 27.6 | 11 | 22.9 |
| BDI-FS (depression) | 4 | 22.2 | ||||||||
| PDQ-5 (Cognition) | 4 | 22.2 | 17 | 21.5 | 21 | 28.8 | 20 | 26.3 | ||
| BLWS (bladder control) | 3 | 16.7 | ||||||||
| BWCS (bowel control | 19 | 24.1 | 18 | 37.5 | ||||||
| MF5I (fatigue) | 16 | 20.3 | 20 | 27.4 | 17 | 22.4 | 10 | 20.8 | ||
| PDDS (disability) | 24 | 32.9 | 29 | 38.2 | 21 | 43.8 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papukchieva, S.; Kahn, M.; Eberl, M.; Friedrich, B.; Joschko, N.; Ziemssen, T. Data on Ocrelizumab Treatment Collected by MS Patients in Germany Using Brisa App. J. Pers. Med. 2024, 14, 409. https://doi.org/10.3390/jpm14040409
Papukchieva S, Kahn M, Eberl M, Friedrich B, Joschko N, Ziemssen T. Data on Ocrelizumab Treatment Collected by MS Patients in Germany Using Brisa App. Journal of Personalized Medicine. 2024; 14(4):409. https://doi.org/10.3390/jpm14040409
Chicago/Turabian StylePapukchieva, Steffeni, Maria Kahn, Markus Eberl, Benjamin Friedrich, Natalie Joschko, and Tjalf Ziemssen. 2024. "Data on Ocrelizumab Treatment Collected by MS Patients in Germany Using Brisa App" Journal of Personalized Medicine 14, no. 4: 409. https://doi.org/10.3390/jpm14040409
APA StylePapukchieva, S., Kahn, M., Eberl, M., Friedrich, B., Joschko, N., & Ziemssen, T. (2024). Data on Ocrelizumab Treatment Collected by MS Patients in Germany Using Brisa App. Journal of Personalized Medicine, 14(4), 409. https://doi.org/10.3390/jpm14040409