
T1 Mapping in Cardiovascular Magnetic Resonance—A Marker of Diffuse Myocardial Fibrosis in Patients Undergoing Hematopoietic Stem Cell Transplantation

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
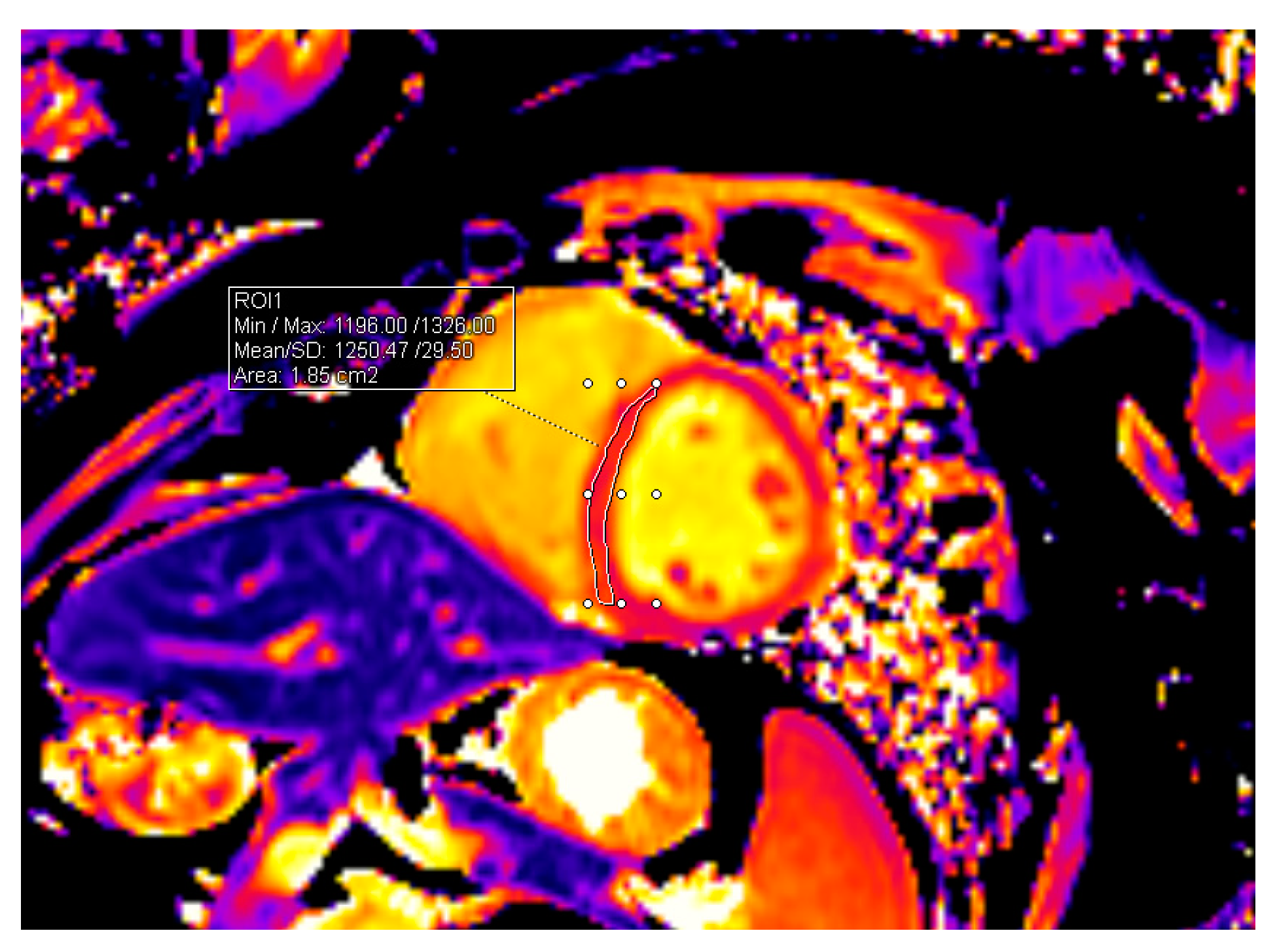
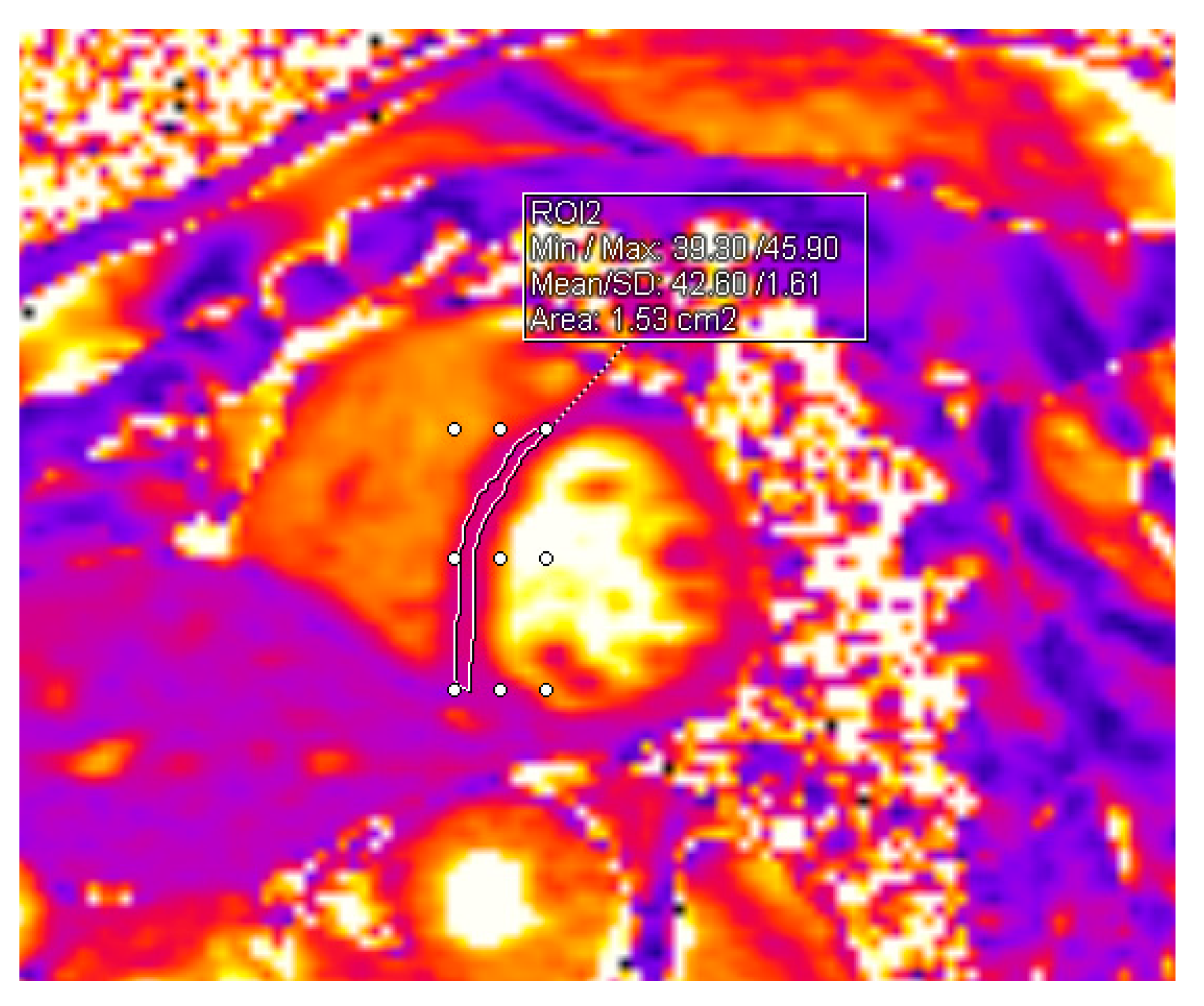
2.1. CMR Acquisition and Analysis
2.2. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardinale, D.; Biasillo, G.; Salvatici, M.; Sandri, M.T.; Cipolla, C.M. Using Biomarkers to Predict and to Prevent Cardiotoxicity of Cancer Therapy. Expert Rev. Mol. Diagn. 2017, 17, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Devine, H.; Kathryn Tierney, D.; Schmit-Pokorny, K.; McDermott, K. Mobilization of Hematopoietic Stem Cells for Use in Autologous Transplantation. Clin. J. Oncol. Nurs. 2010, 14, 212–222. [Google Scholar] [CrossRef]
- Pulte, D.; Gondos, A.; Brenner, H. Trends in 5- and 10-Year Survival after Diagnosis with Childhood Hematologic Malignancies in the United States, 1990–2004. J. Natl. Cancer Inst. 2008, 100, 1301–1309. [Google Scholar] [CrossRef]
- López-Fernández, T.; Vadillo, I.S.; de la Guía, A.L.; Barbier, K.H. Cardiovascular Issues in Hematopoietic Stem Cell Transplantation (HSCT). Curr. Treat. Options Oncol. 2021, 22, 51. [Google Scholar] [CrossRef] [PubMed]
- Carreras, E.; Dufour, C.; Mohty, M.; Kröger, N. The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies [Internet]; Springer: Cham, Switzerland, 2019; pp. 1–702. [Google Scholar] [CrossRef]
- Blank, U.; Karlsson, G.; Karlsson, S. Signaling Pathways Governing Stem-Cell Fate. Blood 2008, 111, 492–503. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.; Trumpp, A. Bone-Marrow Haematopoietic-Stem-Cell Niches. Nat. Rev. Immunol. 2006, 6, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Yanada, M.; Matsuo, K.; Emi, N.; Naoe, T. Efficacy of Allogeneic Hematopoietic Stem Cell Transplantation Depends on Cytogenetic Risk for Acute Myeloid Leukemia in First Disease Remission: A Metaanalysis. Cancer 2005, 103, 1652–1658. [Google Scholar] [CrossRef] [PubMed]
- Alter, B.P. Inherited Bone Marrow Failure Syndromes: Considerations Pre- and Posttransplant. Blood 2017, 130, 2257–2264. [Google Scholar] [CrossRef] [PubMed]
- High, K.A.; Roncarolo, M.G. Gene Therapy. N. Engl. J. Med. 2019, 381, 455–464. [Google Scholar] [CrossRef]
- Karakukcu, M.; Unal, E. Stem Cell Mobilization and Collection from Pediatric Patients and Healthy Children. Transfus. Apher. Sci. 2015, 53, 17–22. [Google Scholar] [CrossRef]
- Balassa, K.; Danby, R.; Rocha, V. Haematopoietic Stem Cell Transplants: Principles and Indications. Br. J. Hosp. Med. 2019, 80, 33–39. [Google Scholar] [CrossRef]
- Bensinger, W.; DiPersio, J.F.; McCarty, J.M. Improving Stem Cell Mobilization Strategies: Future Directions. Bone Marrow Transplant. 2009, 43, 181–195. [Google Scholar] [CrossRef] [PubMed]
- Barriga, F.; Ramírez, P.; Wietstruck, A.; Rojas, N. Hematopoietic Stem Cell Transplantation: Clinical Use and Perspectives. Biol. Res. 2012, 45, 307–316. [Google Scholar] [CrossRef]
- Juric, M.K.; Ghimire, S.; Ogonek, J.; Weissinger, E.M.; Holler, E.; van Rood, J.J.; Oudshoorn, M.; Dickinson, A.; Greinix, H.T. Milestones of Hematopoietic Stem Cell Transplantation–From First Human Studies to Current Developments. Front. Immunol. 2016, 7, 470. [Google Scholar] [CrossRef]
- Paiman, E.H.M.; Louwerens, M.; Bresters, D.; Westenberg, J.J.M.; Tao, Q.; van der Geest, R.J.; Lankester, A.C.; W Roest, A.A.; Lamb, H.J. Late Effects of Pediatric Hematopoietic Stem Cell Transplantation on Left Ventricular Function, Aortic Stiffness and Myocardial Tissue Characteristics. J. Cardiovasc. Magn. Reson. 2019, 21, 6. [Google Scholar] [CrossRef]
- Blaes, A.; Konety, S.; Hurley, P. Cardiovascular Complications of Hematopoietic Stem Cell Transplantation. Curr. Treat. Options Cardiovasc. Med. 2016, 18, 25. [Google Scholar] [CrossRef]
- Ohmoto, A.; Fuji, S. Cardiac Complications Associated with Hematopoietic Stem-Cell Transplantation. Bone Marrow Transplant. 2021, 56, 2637–2643. [Google Scholar] [CrossRef] [PubMed]
- Alizadehasl, A.; Ghadimi, N.; Hosseinifard, H.; Roudini, K.; Emami, A.H.; Ghavamzadeh, A.; khoda-Amorzideh, D. Cardiovascular Diseases in Patients after Hematopoietic Stem Cell Transplantation: Systematic Review and Meta-Analysis. Curr. Res. Transl. Med. 2023, 71, 103363. [Google Scholar] [CrossRef] [PubMed]
- Hemu, M.; Zimmerman, A.; Kalra, D.; Okwuosa, T. Pretransplant Cardiac Evaluation Using Novel Technology. J. Clin. Med. 2019, 8, 690. [Google Scholar] [CrossRef]
- Tuzovic, M.; Mead, M.; Young, P.A.; Schiller, G.; Yang, E.H. Cardiac Complications in the Adult Bone Marrow Transplant Patient. Curr. Oncol. Rep. 2019, 21, 28. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernánde, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klei, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on Cardio-Oncology Developed in Collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef] [PubMed]
- Rotz, S.J.; Ryan, T.D.; Hayek, S.S. Cardiovascular Disease and Its Management in Children and Adults Undergoing Hematopoietic Stem Cell Transplantation. J. Thromb. Thrombolysis 2021, 51, 854–869. [Google Scholar] [CrossRef] [PubMed]
- Vaitiekiene, A.; Kulboke, M.; Bieseviciene, M.; Bartnykaite, A.; Kireilis, B.; Rinkuniene, D.; Jankauskas, A.; Zemaitis, J.; Gaidamavicius, I.; Gerbutavicius, R.; et al. Early Impact of Mobilization Process on Cardiac Function and Size in Patients Undergoing Autologous Hematopoietic Stem Cell Transplantation. J. Clin. Med. 2024, 13, 773. [Google Scholar] [CrossRef] [PubMed]
- Uderzo, C.; Pillon, M.; Corti, P.; Tridello, G.; Tana, F.; Zintl, F.; Nysom, K.; Galambrun, C.; Fagioli, F.; Varotto, S.; et al. Impact of Cumulative Anthracycline Dose, Preparative Regimen and Chronic Graft-versus-Host Disease on Pulmonary and Cardiac Function in Children 5 Years after Allogeneic Hematopoietic Stem Cell Transplantation: A Prospective Evaluation on Behalf of the EBMT Pediatric Diseases and Late Effects Working Parties. Bone Marrow Transplant. 2007, 39, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Puntmann, V.O.; Peker, E.; Chandrashekhar, Y.; Nagel, E. T1 Mapping in Characterizing Myocardial Disease: A Comprehensive Review. Circ. Res. 2016, 119, 277–299. [Google Scholar] [CrossRef] [PubMed]
- Vaitiekus, D.; Muckiene, G.; Vaitiekiene, A.; Maciuliene, D.; Vaiciuliene, D.; Ambrazeviciute, G.; Sereikaite, L.; Verikas, D.; Jurkevicius, R.; Juozaityte, E. Impact of Arterial Hypertension on Doxorubicin-Based Chemotherapy-Induced Subclinical Cardiac Damage in Breast Cancer Patients. Cardiovasc. Toxicol. 2020, 20, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Vaitiekus, D.; Muckiene, G.; Vaitiekiene, A.; Sereikaite, L.; Inciuraite, R.; Insodaite, R.; Cepuliene, D.; Kupcinskas, J.; Ugenskiene, R.; Jurkevicius, R.; et al. HFE Gene Variants’ Impact on Anthracycline-Based Chemotherapy-Induced Subclinical Cardiotoxicity. Cardiovasc. Toxicol. 2021, 21, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Lin, L.; Zhang, G.; Zhou, X. Cardiovascular Magnetic Resonance Imaging in the Early Detection of Cardiotoxicity Induced by Cancer Therapies. Diagnostics 2022, 12, 1846. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.L.; Hu, P.; Ennis, D.B.; Shao, J.; Pham, K.A.; Chen, J.J. Cardiac MRI: A Translational Imaging Tool for Characterizing Anthracycline-Induced Myocardial Remodeling. Curr. Oncol. Rep. 2016, 18, 48. [Google Scholar] [CrossRef]
- Kim, P.K.; Hong, Y.J.; Im, D.J.; Suh, Y.J.; Park, C.H.; Kim, J.Y.; Chang, S.; Lee, H.J.; Hur, J.; Kim, Y.J.; et al. Myocardial T1 and T2 Mapping: Techniques and Clinical Applications. Korean J. Radiol. 2017, 18, 113–131. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1956–2041. [Google Scholar] [CrossRef]
- Park, H.S.; Hong, Y.J.; Han, K.; Kim, P.K.; An, E.; Lee, J.Y.; Park, C.H.; Lee, H.J.; Hur, J.; Kim, Y.J.; et al. Ultrahigh-Field Cardiovascular Magnetic Resonance T1 and T2 Mapping for the Assessment of Anthracycline-Induced Cardiotoxicity in Rat Models: Validation against Histopathologic Changes. J. Cardiovasc. Magn. Reson. 2021, 23, 76. [Google Scholar] [CrossRef] [PubMed]
- Rotz, S.J.; Dandoy, C.E.; Taylor, M.D.; Jodele, S.; Jefferies, J.L.; Lane, A.; El-Bietar, J.A.; Powell, A.W.; Davies, S.M.; Ryan, T.D. Long-Term Systolic Function in Children and Young Adults after Hematopoietic Stem Cell Transplant. Bone Marrow Transplant. 2017, 52, 1443–1447. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jordan, J.H.; Vasu, S.; Morgan, T.M.; D’Agostino, R.B.; Meléndez, G.C.; Hamilton, C.A.; Arai, A.E.; Liu, S.; Liu, C.Y.; Lima, J.A.C.; et al. Anthracycline-Associated T1 Mapping Characteristics Are Elevated Independent of the Presence of Cardiovascular Comorbidities in Cancer Survivors. Circ. Cardiovasc. Imaging 2016, 9, e004325. [Google Scholar] [CrossRef] [PubMed]
- Toro-Salazar, O.H.; Gillan, E.; O’Loughlin, M.T.; Burke, G.S.; Ferranti, J.; Stainsby, J.; Liang, B.; Mazur, W.; Raman, S.V.; Hor, K.N. Occult Cardiotoxicity in Childhood Cancer Survivors Exposed to Anthracycline Therapy. Circ. Cardiovasc. Imaging 2013, 6, 873–880. [Google Scholar] [CrossRef]
- Tham, E.B.; Haykowsky, M.J.; Chow, K.; Spavor, M.; Kaneko, S.; Khoo, N.S.; Pagano, J.J.; Mackie, A.S.; Thompson, R.B. Diffuse Myocardial Fibrosis by T1-Mapping in Children with Subclinical Anthracycline Cardiotoxicity: Relationship to Exercise Capacity, Cumulative Dose and Remodeling. J. Cardiovasc. Magn. Reson. 2013, 15, 48. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sex | |
| Male, n (%) | 24 (54.5) |
| Female, n (%) | 20 (45.5) |
| Age, years (median (minimum–maximum)) | 61 (18–74) |
| Autologous HSCT, n (%) | 39 (88.6) |
| Main disease | |
| Multiple Myeloma, n (%) | 27 (69.2) |
| PCNS diffuse large B cell lymphoma, n (%) | 4 (10.3) |
| Mantle cell lymphoma, n (%) | 4 (10.3) |
| Hodgkin’s lymphoma, n (%) | 2 (5.1) |
| NK/T-cell lymphoma, n (%) | 1 (2.6) |
| Ewing sarcoma, n (%) | 1 (2.6) |
| Allogeneic HSCT, n (%) | 5 (11.4) |
| Main disease | |
| Acute myeloid leukemia, n (%) | 4 (80.0) |
| Acute myelomonocytic leukemia, n (%) | 1 (20.0) |
| Cardiovascular Risk Factors | n (%) |
|---|---|
| CAD | 4 (9.1) |
| Arterial hypertension | 15 (34.1) |
| Diabetes mellitus | 3 (6.8) |
| Family history of CAD | 8 (18.2) |
| Dyslipidemia | 31 (70.5) |
| Currently smoking | 0 (0) |
| Cardiovascular Risk Factor | Mean T1 Values before HSCT | Mean T1 Values after HSCT | No. of Patients |
|---|---|---|---|
| CAD | 1212.54 ± 17.62 | 1235.27 ± 17.82 | 4 |
| Arterial hypertension | 1235.52 ± 42.24 | 1257.07 ± 50.14 | 15 |
| Diabetes mellitus | 1231.79 ± 11.35 | 1277.14 ± 47.68 | 3 |
| Family history of CAD | 1224.16 ± 34.53 | 1250.08 ± 43.54 | 8 |
| Dyslipidemia | 1227.49 ± 35.75 | 1245.69 ± 43.67 | 31 |
| CMR Values | Before HSCT (Mean ± SD) | After HSCT (Mean ± SD) | p |
|---|---|---|---|
| LV EDV, mL | 142.45 ± 35.62 | 145.29 ± 36.36 | 0.713 |
| LV EDVi, mL/m2 | 74.33 ± 15.23 | 75.64 ± 15.10 | 0.686 |
| LV ESV, mL | 60.82 ± 18.36 | 60.15 ± 17.17 | 0.860 |
| LV ESVi, mL/m2 | 31.07 ± 8.36 | 31.55 ± 8.61 | 0.791 |
| LV EF, % | 58.10 ± 7.77 | 58.58 ± 7.08 | 0.761 |
| LV mass, g | 109.22 ± 28.51 | 107.81 ± 29.44 | 0.819 |
| LV mass index, g/m2 | 56.40 ± 11.17 | 56.37 ± 12.92 | 0.991 |
| T1 mapping value, ms | 1226.13 ± 39.74 | 1248.70 ± 41.07 | 0.010 |
| T2 mapping value, ms | 38.91 ± 2.14 | 38.53 ± 2.14 | 0.412 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaitiekiene, A.; Kulboke, M.; Bieseviciene, M.; Jankauskas, A.; Bartnykaite, A.; Rinkuniene, D.; Strazdiene, I.; Lidziute, E.; Jankauskaite, D.; Gaidamavicius, I.; et al. T1 Mapping in Cardiovascular Magnetic Resonance—A Marker of Diffuse Myocardial Fibrosis in Patients Undergoing Hematopoietic Stem Cell Transplantation. J. Pers. Med. 2024, 14, 412. https://doi.org/10.3390/jpm14040412
Vaitiekiene A, Kulboke M, Bieseviciene M, Jankauskas A, Bartnykaite A, Rinkuniene D, Strazdiene I, Lidziute E, Jankauskaite D, Gaidamavicius I, et al. T1 Mapping in Cardiovascular Magnetic Resonance—A Marker of Diffuse Myocardial Fibrosis in Patients Undergoing Hematopoietic Stem Cell Transplantation. Journal of Personalized Medicine. 2024; 14(4):412. https://doi.org/10.3390/jpm14040412
Chicago/Turabian StyleVaitiekiene, Audrone, Migle Kulboke, Monika Bieseviciene, Antanas Jankauskas, Agne Bartnykaite, Diana Rinkuniene, Igne Strazdiene, Emilija Lidziute, Darija Jankauskaite, Ignas Gaidamavicius, and et al. 2024. "T1 Mapping in Cardiovascular Magnetic Resonance—A Marker of Diffuse Myocardial Fibrosis in Patients Undergoing Hematopoietic Stem Cell Transplantation" Journal of Personalized Medicine 14, no. 4: 412. https://doi.org/10.3390/jpm14040412
APA StyleVaitiekiene, A., Kulboke, M., Bieseviciene, M., Jankauskas, A., Bartnykaite, A., Rinkuniene, D., Strazdiene, I., Lidziute, E., Jankauskaite, D., Gaidamavicius, I., Bucius, P., Lapinskas, T., Gerbutavicius, R., Juozaityte, E., Vaskelyte, J. J., Vaitiekus, D., & Sakalyte, G. (2024). T1 Mapping in Cardiovascular Magnetic Resonance—A Marker of Diffuse Myocardial Fibrosis in Patients Undergoing Hematopoietic Stem Cell Transplantation. Journal of Personalized Medicine, 14(4), 412. https://doi.org/10.3390/jpm14040412