
Cryoanalgesia as the Essential Element of Enhanced Recovery after Surgery (ERAS) in Children Undergoing Thoracic Surgery—Scoping Review

{kind=link}
Abstract
1. Introduction
2. Materials and Methods
- Specifying the research question: Can cryoanalgesia combined with multimodal analgesia during the peri-operative period in children improve the effectiveness of ERAS protocol?
- 2.
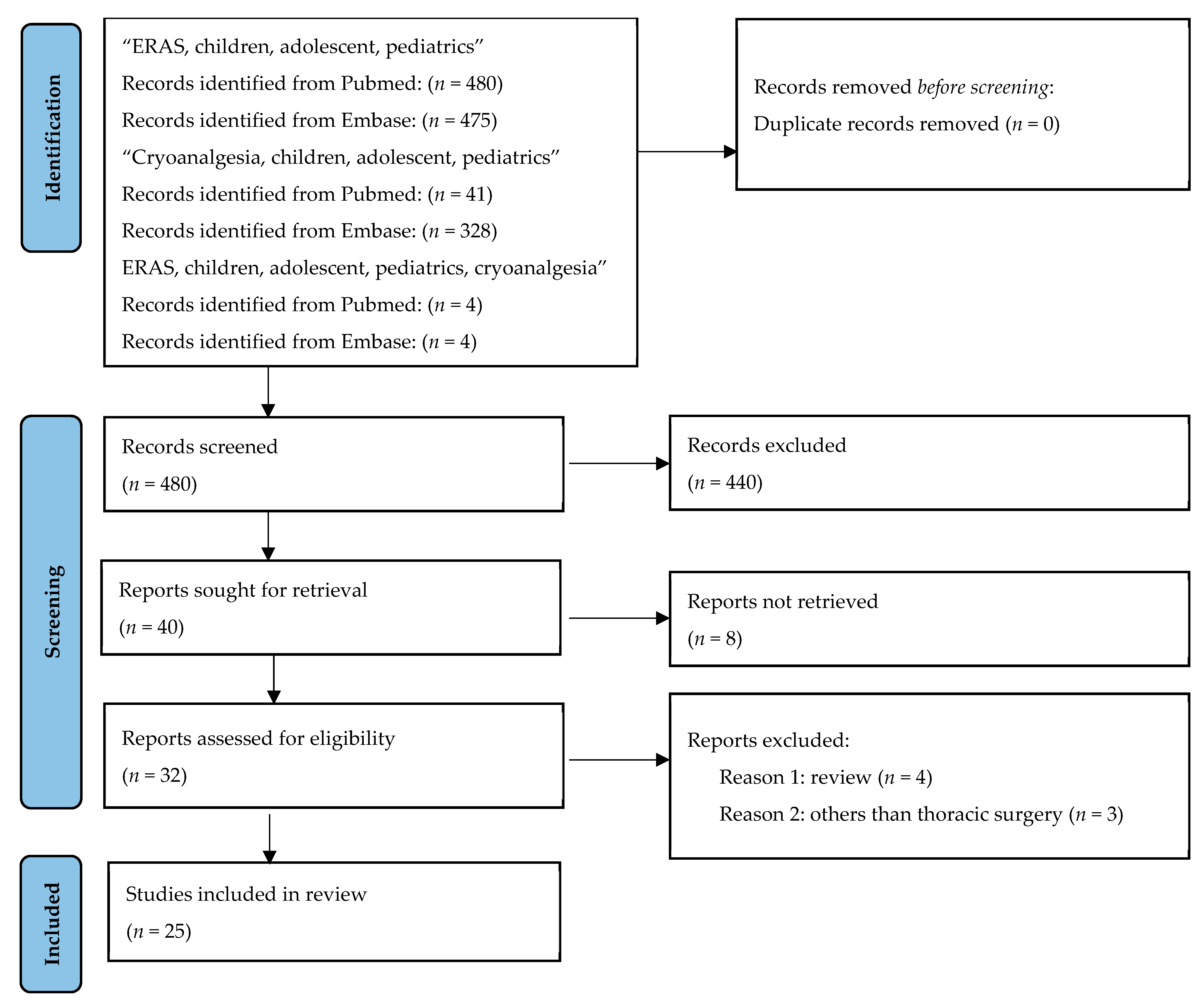
- Identifying relevant literature.
- 3.
- Selection of studies.
- 4.
- Data evaluation.
- 5.
- Summarizing, synthesizing, and describing the results.
3. Results
3.1. Foundations of Cryoanalgesia: Physical and Structural Aspects
3.2. Initiation and Duration of Cryoanalgesia
3.3. Duration of Cryoanalgesia Application
3.4. Clinical Application
3.5. Application of Cryoanalgesia in Children
3.6. Intraoperative Intrathoracic and Preoperative Percutaneous Technique
3.7. Study Endpoints for Cryoanalgesia
3.8. Cryoanalgesia as the Essential Element of ERAS in Children
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ERAS | Enhanced recovery after surgery |
| VAS | Visual analog scale |
| CWIG | Chest Wall International Group |
References
- Kehlet, H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br. J. Anaesth. 1997, 78, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Scott, M.J.; Baldini, G.; Fearon, K.C.H.; Feldheiser, A.; Feldman, L.S.; Gan, T.J.; Ljungqvist, O.; Lobo, D.N.; Rockall, T.A.; Schricker, T.; et al. Enhanced Recovery After Surgery (ERAS) for gastrointestinal surgery, part 1: Pathophysiological considerations. Acta Anaesthesiol. Scand. 2015, 59, 1212–1231. [Google Scholar] [CrossRef] [PubMed]
- Feldheiser, A.; Aziz, O.; Baldini, G.; Cox, B.P.B.W.; Fearon, K.C.H.; Feldman, L.S.; Gan, T.J.; Kennedy, R.H.; Ljungqvist, O.; Lobo, D.N.; et al. Enhanced Recovery After Surgery (ERAS) for gastrointestinal surgery, part 2: Consensus statement for anesthesia practice. Acta Anaesthesiol. Scand. 2016, 60, 289–334. [Google Scholar] [CrossRef]
- Soffin, E.M.; MacKenzie, C.R.; Cornell, C.N.; Memtsoudis, S.G. Enhanced Recovery After Surgery (ERAS) Protocols in Orthopedic Patients. In Perioperative Care of the Orthopedic Patient, 2nd ed.; Springer: New York, NY, USA, 2020; pp. 143–150. [Google Scholar]
- Wainwright, T.W.; Gill, M.; A McDonald, D.; Middleton, R.G.; Reed, M.; Sahota, O.; Yates, P.; Ljungqvist, O. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Acta Orthop. 2020, 91, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.-C.; He, L.-J.; Chen, D.; Li, X.-B.; Feng, Z.-H.; Fu, C.-W.; Xuan, J.-W.; Ni, W.-F.; Wu, A.-M. An enhanced recovery after surgery programme in orthopedic surgery: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2019, 14, 77. [Google Scholar] [CrossRef] [PubMed]
- Delande, S.; Lavand’homme, P. Acute pain management and long-term outcomes. Curr. Opin. Anaesthesiol. 2023, 36, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Van Boekel, R.L.M.; Vissers, K.C.P.; van der Sande, R.; Bronkhorst, E.; Lerou, J.G.C.; Steegers, M.A.H. Moving beyond pain scores: Multidimensional pain assessment is essential for adequate pain management after surgery. PLoS ONE 2017, 12, e0177345. [Google Scholar] [CrossRef]
- De Loos, E.; Pennings, A.; van Roozendaal, L.; Daemen, J.; van Gool, M.; Lenderink, T.; van Horck, M.; Hulsewe, K.; Vissers, Y. Nuss Procedure for Pectus Excavatum: A Comparison of Complications Between Young and Adult Patients. Ann. Thorac. Surg. 2021, 112, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Singhal, N.R.; Jones, J.; Semenova, J.; Williamson, A.; McCollum, K.; Tong, D.; Jerman, J.; Notrica, D.M.; Nguyen, H. Multimodal anesthesia with the addition of methadone is superior to epidural analgesia: A retrospective comparison of intraoperative anesthetic techniques and pain management for 124 pediatric patients undergoing the Nuss procedure. J. Pediatr. Surg. 2016, 51, 612–616. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Koucheki, R.; Koyle, M.; Ibrahim, G.M.; Nallet, J.; Lebel, D.E. Comparison of interventions and outcomes of enhanced recovery after surgery: A systematic review and meta-analysis of 2456 adolescent idiopathic scoliosis cases. Eur. Spine J. 2021, 30, 3457–3472. [Google Scholar] [CrossRef] [PubMed]
- Debono, B.; Wainwright, T.W.; Wang, M.Y.; Sigmundsson, F.G.; Yang, M.M.; Smid-Nanninga, H.; Bonnal, A.; Le Huec, J.-C.; Fawcett, W.J.; Ljungqvist, O.; et al. Consensus statement for perioperative care in lumbar spinal fusion: Enhanced Recovery After Surgery (ERAS) Society recommendations. Spine J. 2021, 21, 729–752. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Rai, S.; Ze, R.; Tang, X.; Liu, R.; Hong, P. Enhanced recovery care versus traditional non-ERAS care following osteotomies in developmental dysplasia of the hip in children: A retrospective case-cohort study. BMC Musculoskelet. Disord. 2020, 21, 234. [Google Scholar] [CrossRef] [PubMed]
- Garin, C. Enhanced recovery after surgery in pediatric orthopedics (ERAS-PO). Orthop. Traumatol. Surg. Res. 2020, 106, 101–107. [Google Scholar] [CrossRef]
- Loganathan, A.K.; Joselyn, A.S.; Babu, M.; Jehangir, S. Implementation and outcomes of enhanced recovery protocols in pediatric surgery: A systematic review and meta-analysis. Pediatr. Surg. Int. 2022, 38, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Zacha, S.; Szwed, A.; Miegoń, J.; Skonieczna-Żydecka, K.; Andrzejewska, A.; Modrzejewska, E.; Horecki, M.; Jarosz, K.; Biernawska, J. Novel Interdisciplinary Enhanced Recovery after Surgery Protocol Implementation in Paediatric Orthopaedics. J. Pers. Med. 2023, 13, 1417. [Google Scholar] [CrossRef] [PubMed]
- Zacha, S.; Andrzejewska, A.; Jastrzębska-Ligocka, B.; Szwed, A.; Modrzejewska, E.; Zacha, W.; Skonieczna-Żydecka, K.; Miegoń, J.; Jarosz, K.; Biernawska, J. Intercostal nerve cryoanalgesia in the treatment of pain in patients operated on by the modified Nuss method with the BackOnFeet application-a new strategy to improve outcomes. Front. Pediatr. 2023, 10, 1069805. [Google Scholar] [CrossRef] [PubMed]
- DiFiore, J.W.; Robertson, J.O.; Chhabada, S.; DeRoss, A.L.; Hossain, M.S.; Rincon-Cruz, L.; Sung, W. Next day discharge after the Nuss procedure using intercostal nerve cryoablation, intercostal nerve blocks, and a perioperative ERAS pain protocol. J. Pediatr. Surg. 2022, 57, 213–218. [Google Scholar] [CrossRef]
- Lai, K.; Eldredge, R.S.; Zobel, M.; Hargis-Villanueva, A.; Ostlie, A.; Padilla, B.E. Intercostal Nerve Cryoablation for Postoperative Pain Control in Pediatric Thoracic Surgery: A Scoping Review. J. Laparoendosc. Adv. Surg. Tech. A 2023, 33, 994–1004. [Google Scholar] [CrossRef]
- Gan, T.J.; Belani, K.G.; Bergese, S.; Chung, F.; Diemunsch, P.; Habib, A.S.; Jin, Z.; Kovac, A.L.; Meyer, T.A.; Urman, R.D.; et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth. Analg. 2020, 131, 411–448. [Google Scholar] [CrossRef]
- Cettler, M.; Zielińska, M.; Rosada-Kurasińska, J.; Kubica-Cielińska, A.; Jarosz, K.; Bartkowska-Śniatkowska, A. Guidelines for treatment of acute pain in children—The consensus statement of the Section of Paediatric Anaesthesiology and Intensive Therapy of the Polish Society of Anaesthesiology and Intensive Therapy. Anaesthesiol. Intensive Ther. 2022, 54, 197–218. [Google Scholar] [CrossRef]
- Maiwand, O.; Makey, A.R.; Sanmuganathan, S. Increased effectiveness of physiotherapy after cryoanalgesia following thoracotomy. Physiotherapy 1982, 68, 288–290. [Google Scholar] [PubMed]
- Frykholm, P.; Disma, N.; Andersson, H.; Beck, C.; Bouvet, L.; Cercueil, E.; Elliott, E.; Hofmann, J.; Isserman, R.; Klaucane, A.; et al. Pre-operative fasting in children. A guideline from the European Society of Anaesthesiology and Intensive Care. Eur. J. Anaesthesiol. 2022, 39, 4–25. [Google Scholar] [CrossRef] [PubMed]
- Erinjeri, J.P.; Clark, T.W. Cryoablation: Mechanism of action and devices. J. Vasc. Interv. Radiol. 2010, 21, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Graves, C.; Idowu, O.; Lee, S.; Padilla, B.; Kim, S. Intraoperative cryoanalgesia for managing pain after the Nuss procedure. J. Pediatr. Surg. 2017, 52, 920–924. [Google Scholar] [CrossRef]
- Jakubów, P.; Kościuczuk, U.; Kosel, J.; Turczynowicz, A.; Luchowski, K.; Tałałaj, M.; Kondracka, J. Zastosowanie metody kriolezji w medycynie paliatywnej. Med. Paliatywna 2020, 13, 9–18. [Google Scholar] [CrossRef]
- Hsu, M.; Stevenson, F.F. Wallerian degeneration and recovery of motor nerves after multiple focused cold therapies. Muscle Nerve 2015, 51, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.; Inge, M.; Zeineddin, S.; Linton, S.C.; Pitt, J.B.; Robson, P.; Abdullah, F.; Goldstein, S.D. Measurement and Thermodynamic Modeling of Energy Flux during Intercostal Nerve Cryoablation. J. Surg. Res. 2023, 293, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Zeineddin, S.; Goldstein, S.; Linton, S.; DeBoer, C.; Alayleh, A.; Ortiz, I.; Sands, L.; Kujawa, S.; Suresh, S.; Ghomrawi, H.; et al. Effectiveness of one minute per level intercostal nerve cryoablation for postoperative analgesia after surgical correction of pectus excavatum. J. Pediatr. Surg. 2023, 58, 34–40. [Google Scholar] [CrossRef]
- Takada, M.; Toi, M. Cryosurgery for primary breast cancers, its biological impact, and clinical outcomes. Int. J. Clin. Oncol. 2019, 24, 608–613. [Google Scholar] [CrossRef]
- Godek, P. Kriolezja i termolezja w praktyce ortopedy—Doświadczenia własne. Prakt. Ortop. Traumatol. 2018, Nr 5. [Google Scholar]
- Ilfeld, B.M.; Gabriel, R.A.; Trescot, A.M. Ultrasound-guided percutaneous cryoneurolysis for treatment of acute pain: Could cryoanalgesia replace continuous peripheral nerve blocks? Br. J. Anaesth. 2017, 119, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Torre, M.; Mameli, L.; Bonfiglio, R.; Guerriero, V.; Derosas, L.; Palomba, L.; Disma, N. A New Device for Thoracoscopic Cryoanalgesia in Pectus Excavatum Repair: Preliminary Single Center Experience. Front. Pediatr. 2021, 8, 614097. [Google Scholar] [CrossRef] [PubMed]
- Archer, V.; Robinson, T.; Kattail, D.; Fitzgerald, P.; Walton, J.M. Postoperative pain control following minimally invasive correction of pectus excavatum in pediatric patients: A systematic review. J. Pediatr. Surg. 2020, 55, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Bundrant, N.T.; Sayrs, L.W.; Ostlie, D.; Lee, J.; Egan, C.; Molitor, M.; Notrica, D.; Padilla, B. Infectious complications of intercostal nerve cryoablation mediated by perioperative hypothermia during pediatric Nuss procedure. J. Pediatr. Surg. 2022, 57, 1083–1086. [Google Scholar] [CrossRef] [PubMed]
- Sepsas, E.; Misthos, P.; Anagnostopulu, M.; Toparlaki, O.; Voyagis, G.; Kakaris, S. The role of intercostal cryoanalgesia in post-thoracotomy analgesia. Interact. Cardiovasc. Thorac. Surg. 2013, 16, 814–818. [Google Scholar] [CrossRef] [PubMed]
- Park, R.; Coomber, M.; Gilron, I.; Shanthanna, H. Cryoanalgesia for postsurgical pain relief in adults: A systematic review and meta-analysis. Ann. Med. Surg. 2021, 69, 102689. [Google Scholar] [CrossRef] [PubMed]
- Arshad, S.A.; Hatton, G.E.; Ferguson, D.M.; Li, L.T.; Austin, M.T.; Tsao, K. Cryoanalgesia enhances recovery from minimally invasive repair of pectus excavatum resulting in reduced length of stay: A case-matched analysis of NSQIP-Pediatric patients. J. Pediatr. Surg. 2021, 56, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, A.R.; Hunter, C.E.; Colgate, C.L.; Landman, M.P. Neurolysis for analgesia following pectus repair in a national cohort. J. Pediatr. Surg. 2022, 57, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Toselli, L.; Gigena, C.; Bellia-Munzon, G.; Sanjurjo, D.; Vallee, M.; Martinez-Ferro, M. Lessons Learned after 176 Patients Treated with a Standardized Procedure of Thoracoscopic Cryoanalgesia during Minimally Invasive Repair of Pectus Excavatum. J. Pediatr. Surg. 2023, 59, 372–378. [Google Scholar] [CrossRef]
- Arshad, S.A.; Garcia, E.I.; Bell, C.; Avritscher, E.B.; Kumar, M.; Brahmamdam, P.; Fraser, J.A.; Peter, S.D.S.; Aranda, A.; Hill, M.; et al. Multicenter Assessment of Cryoanalgesia Use in Minimally Invasive Repair of Pectus Excavatum: A 20-center Retrospective Cohort Study. Pediatric Surgery Research Collaborative (PedSRC). Ann. Surg. 2023, 277, e1373–e1379. [Google Scholar] [CrossRef]
- Lai, K.; Notrica, D.M.; McMahon, L.E.; Kang, P.; Molitor, M.S.; Egan, J.C.; Bae, J.-O.; Hunteman, Z.M.; Ostlie, D.J.; Lee, J.H.; et al. Cryoablation in 350 Nuss Procedures: Evolution of Hospital Length of Stay and Opioid Use. J. Pediatr. Surg. 2023, 58, 1435–1439. [Google Scholar] [CrossRef] [PubMed]
- Muhly, W.T.; Maxwell, L.G.; Cravero, J.P. Pain management following the Nuss procedure: A survey of practice and review. Acta Anaesthesiol. Scand. 2014, 58, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Idowu, O.; Palmer, B.; Lee, S.H. Use of transthoracic cryoanalgesia during the Nuss procedure. J. Thorac. Cardiovasc. Surg. 2016, 151, 887–888. [Google Scholar] [CrossRef] [PubMed]
- Keller, B.A.; Kabagambe, S.K.; Becker, J.C.; Chen, Y.J.; Goodman, L.F.; Clark-Wronski, J.M.; Furukawa, K.; Stark, R.A.; Rahm, A.L.; Hirose, S.; et al. Intercostal nerve cryoablation versus thoracic epidural catheters for postoperative analgesia following pectus excavatum repair: Preliminary outcomes in twenty-six cryoablation patients. J. Pediatr. Surg. 2016, 51, 2033–2038. [Google Scholar] [CrossRef] [PubMed]
- Graves, C.E.; Moyer, J.; Zobel, M.J.; Mora, R.; Smith, D.; O'Day, M.; Padilla, B.E. Intraoperative intercostal nerve cryoablation during the Nuss procedure reduces length of stay and opioid requirement: A randomized clinical trial. J. Pediatr. Surg. 2019, 54, 2250–2256. [Google Scholar] [CrossRef] [PubMed]
- Dekonenko, C.; Dorman, R.M.; Duran, Y.; Juang, D.; Aguayo, P.; Fraser, J.D.; Oyetunji, T.A.; Snyder, C.L.; Holcomb, G.W.; Millspaugh, D.L.; et al. Postoperative pain control modalities for pectus excavatum repair: A prospective observational study of cryoablation compared to results of a randomized trial of epidural vs. patient-controlled analgesia. J. Pediatr. Surg. 2020, 55, 1444–1447. [Google Scholar] [CrossRef] [PubMed]
- Arshad, S.A.; Ferguson, D.M.; Garcia, E.I.; Hebballi, N.B.; Buchanan, A.C.; Tsao, K. Cryoanalgesia is Associated with Decreased Postoperative Opioid Use in Minimally Invasive Repair of Pectus Excavatum. J. Surg. Res. 2022, 271, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Cadaval Gallardo, C.; Martínez, J.; Bellía-Munzon, G.; Nazar, M.; Sanjurjo, D.; Toselli, L.; Martínez-Ferro, M. Thoracoscopic cryoanalgesia: A new strategy for postoperative pain control in minimally invasive pectus excavatum repair. Cir. Pediatr. 2020, 33, 11–15. [Google Scholar] [PubMed]
- Hegde, B.N.; Avritscher, E.; Arshad, S.A.; Garcia, E.I.; Hebballi, N.B.; Broussard, M.; Tsao, K. Impact of Cryoanalgesia Use during Minimally Invasive Pectus Excavatum Repair on Hospital Days and Total Hospital Costs among Pediatric Patients. J. Pediatr. Surg. 2023, 58, 1235–1238. [Google Scholar] [CrossRef]
- Talsma, J.; Kusakavitch, M.; Lee, D.; Niederhauser, C.; Palmer, B.; Ozgediz, D.; Idowu, O.; Kim, S. Forgotten Branch of the Intercostal Nerve: Implication for Cryoablation Nerve Block for Pectus Excavatum Repair. J. Pediatr. Surg. 2023, 58, 2435–2440. [Google Scholar] [CrossRef]
- Pilkington, M.; Harbaugh, C.M.; Hirschl, R.B.; Geiger, J.D.; Gadepalli, S.K. Use of cryoanalgesia for pain management for the modified Ravitch procedure in children. J. Pediatr. Surg. 2020, 55, 1381–1384. [Google Scholar] [CrossRef] [PubMed]
- Velayos, M.; Alonso, M.; Delgado-Miguel, C.; Estefanía-Fernández, K.; Muñoz-Serrano, A.J.; Santamaría, M.V.L.; Reinoso-Barbero, F.; De La Torre, C.A. Percutaneous Cryoanalgesia: A New Strategy for Pain Management in Pectus Excavatum Surgery. Eur. J. Pediatr. Surg. 2022, 32, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Gologorsky, R.; Ewbank, C.; Idowu, O.; Kim, S. Use of cryoanalgesia as a postoperative pain management for open pectus carinatum repair. Pediatr. Surg. Int. 2021, 37, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, N.; Laferriere, N.; Koo, S.; Johnson, S.; Woo, R.; Puapong, D. Cryoanalgesia in Patients Undergoing Nuss Repair of Pectus Excavatum: Technique Modification and Early Results. J. Laparoendosc. Adv. Surg. Tech. A 2018, 28, 1148–1151. [Google Scholar] [CrossRef] [PubMed]
- Aiken, T.J.; Stahl, C.C.; Lemaster, D.; Casias, T.W.; Walker, B.J.; Nichol, P.F.; Leys, C.M.; Abbott, D.E.; Brinkman, A.S. Intercostal nerve cryoablation is associated with lower hospital cost during minimally invasive Nuss procedure for pectus excavatum. J. Pediatr. Surg. 2021, 56, 1841–1845. [Google Scholar] [CrossRef] [PubMed]
- Rettig, R.L.; Rudikoff, A.G.; Lo, H.Y.A.; Lee, C.W.; Vazquez, W.D.; Rodriguez, K.; Shaul, D.B.; Conte, A.H.; Banzali, F.M.; Sydorak, R.M. Same-day discharge following the Nuss repair: A comparison. J. Pediatr. Surg. 2022, 57, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Akinboro, S.; John, R.; Reyna, T.; Davis, R.; Ayoub, C.; Sangster, R.; Kim, J.; Nguyen, H.; Moreno, C.; Guner, Y.; et al. A pilot study of multi-modal pain management for same-day discharge after minimally invasive repair of pectus excavatum (Nuss procedure) in children. Pediatr. Surg. Int. 2023, 39, 159. [Google Scholar] [CrossRef] [PubMed]
- Downing, L.; Ramjist, J.K.; Tyrrell, A.; Tsang, M.; Isaac, L.; Fecteau, A. Development of the five points enhanced recovery protocol for pectus excavatum surgery. J. Pediatr. Surg. 2023, 58, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Sujka, J.; Benedict, L.A.; Fraser, J.D.; Aguayo, P.; Millspaugh, D.L.; Peter, S.D.S. Outcomes using cryoablation for postoperative pain control in children following minimally invasive pectus excavatum repair. J. Laparoendosc. Adv. Surg. Tech. A 2018, 28, 1383–1386. [Google Scholar] [CrossRef]
- Harbaugh, C.M.; Johnson, K.N.; Kein, C.E.; Jarboe, M.D.; Hirschl, R.B.; Geiger, J.D.; Gadepalli, S.K. Comparing outcomes with thoracic epidural and intercostal nerve cryoablation after Nuss procedure. J. Surg. Res. 2018, 231, 217–223. [Google Scholar] [CrossRef]
- Song, S.H.; Moon, D.H.; Shim, Y.H.; Jung, H.; Lee, S. Limited cryoablation reduces hospital stay and opioid consumption compared to thoracic epidural analgesia after minimally invasive repair of pectus excavatum. Medicine 2022, 101, E29773. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.A.; Briggs, K.B.; Svetanoff, W.J.; Aguayo, P.; Juang, D.; Fraser, J.D.; Snyder, C.L.; Oyetunji, T.A.; Peter, S.D.S. Short and long term outcomes of using cryoablation for postoperative pain control in patients after pectus excavatum repair. J. Pediatr. Surg. 2022, 57, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Cockrell, H.C.; Hrachovec, J.; Schnuck, J.; Nchinda, N.; Meehan, J. Implementation of a cryoablation-based pain management protocol for pectus excavatum. J. Pediatr. Surg. 2023, 58, 1239–1245. [Google Scholar] [CrossRef]
- Parrado, R.; Lee, J.; McMahon, L.E.; Clay, C.; Powell, J.; Kang, P.; Notrica, D.M.; Ostlie, D.J.; Bae, J.-O. The Use of Cryoanalgesia in Minimally Invasive Repair of Pectus Excavatum: Lessons Learned. Laparoendosc. Adv. Surg. Tech. A 2019, 29, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.C.; Mehl, S.C.; Anbarasu, C.R.; Portuondo, J.I.; Espinoza, A.F.; Whitlock, R.; Mazziotti, M.V. Intercostal cryoablation during Nuss procedure: A large volume single surgeon’s experience and outcomes. J. Pediatr. Surg. 2021, 56, 2229–2234. [Google Scholar] [CrossRef] [PubMed]
- A Clark, R.; Jacobson, J.C.; Singhal, A.B.; Alder, A.C.M.; Chung, D.H.M.; Pandya, S.R.M. Impact of cryoablation on pectus excavatum repair in pediatric patients. J. Am. Coll. Surg. 2022, 234, 484–492. [Google Scholar] [CrossRef]
- Holguin, R.A.P.; DeAngelo, N.; Sinha, A.; Shen, C.; Tsai, A.Y. Cost and outcomes of intercostal nerve cryoablation versus thoracic epidural following the Nuss procedure. J. Pediatr. Surg. 2023, 58, 608–612. [Google Scholar] [CrossRef]
- Zobel, M.J.; Ewbank, C.; Mora, R.; Idowu, O.; Kim, S.; Padilla, B.E. The incidence of neuropathic pain after intercostal cryoablation during the Nuss procedure. Pediatr. Surg. Int. 2020, 36, 317–324. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zacha, S.; Biernawska, J. Cryoanalgesia as the Essential Element of Enhanced Recovery after Surgery (ERAS) in Children Undergoing Thoracic Surgery—Scoping Review. J. Pers. Med. 2024, 14, 411. https://doi.org/10.3390/jpm14040411
Zacha S, Biernawska J. Cryoanalgesia as the Essential Element of Enhanced Recovery after Surgery (ERAS) in Children Undergoing Thoracic Surgery—Scoping Review. Journal of Personalized Medicine. 2024; 14(4):411. https://doi.org/10.3390/jpm14040411
Chicago/Turabian StyleZacha, Sławomir, and Jowita Biernawska. 2024. "Cryoanalgesia as the Essential Element of Enhanced Recovery after Surgery (ERAS) in Children Undergoing Thoracic Surgery—Scoping Review" Journal of Personalized Medicine 14, no. 4: 411. https://doi.org/10.3390/jpm14040411
APA StyleZacha, S., & Biernawska, J. (2024). Cryoanalgesia as the Essential Element of Enhanced Recovery after Surgery (ERAS) in Children Undergoing Thoracic Surgery—Scoping Review. Journal of Personalized Medicine, 14(4), 411. https://doi.org/10.3390/jpm14040411