
Precision Workforce Management for Radiographers: Monitoring and Managing Competences with an Automatic Tool
 , ,
, , 
Abstract
1. Introduction
1.1. Background
1.2. Introduction to the Study’s Relevance
1.3. Aim
Subsidiary Goals
2. Methods
3. Results
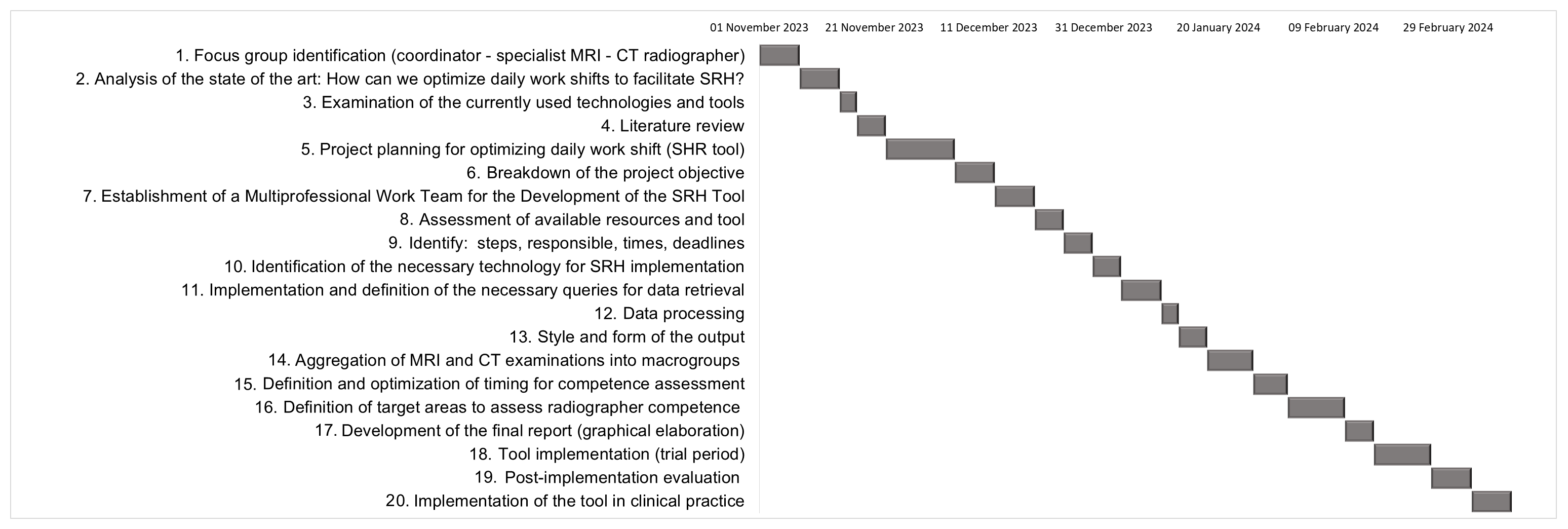
3.1. Utilization of a SRH Tool for Optimizing Daily Work Shift Planning in CT and MRI: From Development to Clinical Implementation
- -
- Aggregation of CT and MRI examinations into macro-groups (8 days). In this case, the task of the focus group was to identify the different and numerous MRI and CT examinations performed and recorded by the radiographers in the RIS and to summarize them in macro groups defined according to the anatomical district. In particular, 108 different CT examinations were categorized into five macro-groups and 137 MRI examinations into nine macro-groups.
- -
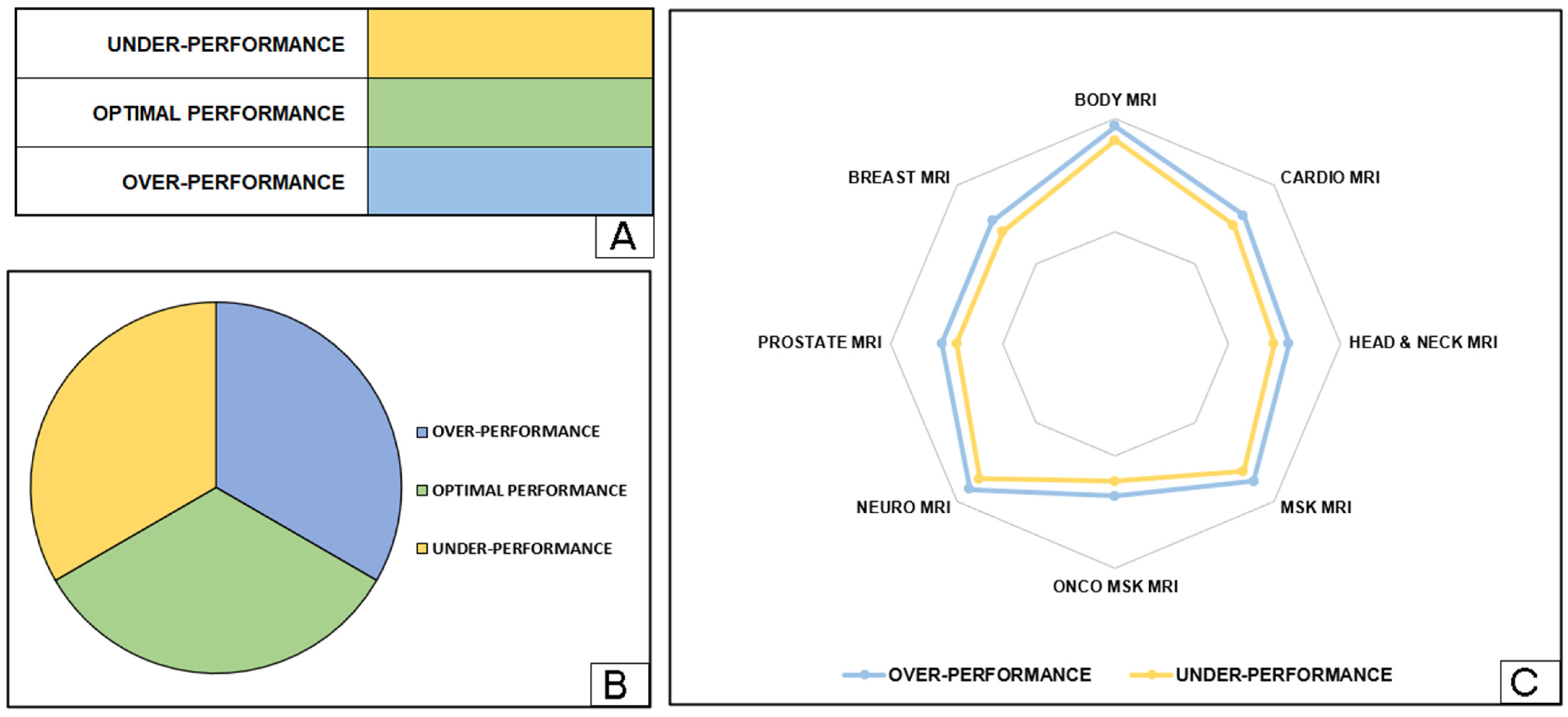
- Definition of target ranges to assess radiographer competence (10 days). In this activity, the focus group defined the “target ranges”, which represent the number of examinations (±15%) for each macro group that each radiographer must perform within a given timeframe to maintain their competence. If the number of examinations performed is below the target value, this is considered “under-performance”, while a higher value is referred to as “over-performance”.
- Figure 3A shows a table listing the competencies for each macro-group assigned to radiographers based on defined target areas. To improve readability and interpretation, different colors indicate specific target areas within the competencies.
- Figure 3B includes a comprehensive pie chart providing a holistic overview of the competencies across all macro-groups for all radiographers. This diagram offers an e-summary of the distribution of skills and expertise within the radiography team, facilitating informed decision making and resource allocation for coordinators.
- Figure 3C features a radar chart that graphically depicts the competencies of each radiographer for the different MRI macro-groups. This visualization technique provides a comprehensive overview of the professionals’ competencies and areas for improvement in their respective fields. Optimal performance is defined as the area between two lines indicating underperformance and overperformance.
3.2. Feedback from the Training Event before the SRH Tool Release
3.2.1. Insights into the Participants to the Training Event
3.2.2. Feedback and Findings from Single-Choice and Open-Ended Questions
- -
- In the field of cardiovascular perfusion, the utilization of the SRH tool in clinical practice may be restricted due to the necessity of having all colleagues present for both emergency and routine activities.
- -
- A total 71% of the medical laboratory technician coordinators are of the opinion that this tool cannot be implemented in this form but that appropriate modifications would be necessary, as there is not always a match between medical laboratory technicians and performance and not all of their activities are measurable.
3.2.3. Feedback and Findings from Likert-Scale Questions
3.2.4. Feedback from Qualitative Analysis
3.3. Comprehensive SRH Tool Release, Maintenance, Monitoring, and Transfer Plan
3.3.1. SRH Tool Release
3.3.2. SRH Tool Maintenance and Monitoring
- Implementation of Quality Control and Monitoring Procedures: This strategy involves establishing robust protocols and procedures to ensure the seamless functionality and reliability of the SRH tool. By adhering to stringent quality control measures, potential issues can be pre-emptively identified and addressed. These procedures will align closely with organizational standards, ensuring consistency and adherence to best practices. Meticulous monitoring at every stage of the SRH tool’s lifecycle will proactively safeguard against disruptions and optimize performance.
- Application of Key Performance Indicators (KPIs) Based on the Scientific Literature: Monitoring efforts will be fortified by the application of KPIs selected based on extensive research from the scientific literature. Drawing upon insights from peer-reviewed studies and industry best practices, meaningful indicators of the SRH tool’s effectiveness and efficiency will be identified and prioritized. Aligning monitoring efforts with evidence-based metrics will provide comprehensive insights into strengths and areas for improvement. This data-driven approach will empower informed decision making and drive continuous enhancements to the SRH tool’s functionality and performance.
Implementation of Quality Control and Monitoring Procedures for the SRH Tool
Application of Key Performance Indicators Used for Fostering Effective Communication and Leadership Using the SRH Tool
3.3.3. SRH Transfer Plan
4. Discussion
4.1. Highlights from the Study
- -
- Recognition of the impracticality of extending the model/product to medical laboratory technicians and cardiovascular perfusionists due to the intricacies of their shift scheduling.
- -
- The imperative need for specialized training integrated into the curriculum of Italian university degree programs.
- -
- The usefulness in the hands of the relevant professional scientific society/associations. This comprehensive evaluation mechanism not only provided concrete feedback on the SRH tool’s viability but also yielded actionable insights for refining its implementation and potential expansion into diverse healthcare sectors.
4.2. Importance and Location of the Study
5. Work in Progress
6. Takeaway Message
7. Conclusions
- Introduction of the SRH tool, a cost-effective solution leveraging existing software, tailored for radiographers.
- Highlighting the SRH tool’s ability to generate weekly reports aiding in activity management and resource allocation.
- Creation of the CAWI tool for evaluating the acceptance of the SRH tool, providing valuable feedback and insights after the training event before its release, also useful for defining a roadmap for transferring it to professions other than radiographers.
- Initial outcomes from the first implementation in clinical practice by two coordinators to optimize the work shifts of 35 radiographers for MRI examinations. After three months of tool usage, a 7% reduction in radiographer underperformance in MRI examinations was observed. This outcome on the profession of radiographers showcases the tool’s potential in routine clinical practice for monitoring competence and improving professionals in the healthcare domain.
- Definition of a roadmap for monitoring-and- maintenance and, specifically, transferring the SRH tool conducting feasibility investigations and making adaptations tailored to various healthcare professionals, with the participation of relevant scientific associations. This approach will enable the release of a customized version of the tool.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andersson, B.T.; Fridlund, B.; Elgán, C.; Axelsson, A.B. Radiographers’ areas of professional competence related to good nursing care. Scand. J. Caring Sci. 2008, 22, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.; Bleiker, J.; Hodgson, D. Compassionate communication: Keeping patients at the heart of practice in an advancing radiographic workforce. Radiography 2021, 27 (Suppl. S1), S43–S49. [Google Scholar] [CrossRef] [PubMed]
- Strudwick, R.M.; Day, J. Interprofessional working in diagnostic radiography. Radiography 2014, 20, 235–240. [Google Scholar] [CrossRef]
- Hyde, E.; Hardy, M. Patient centred care in diagnostic radiography (Part 1): Perceptions of service users and service deliverers. Radiography 2021, 27, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Al-Shemmari, A.F.; Herbland, A.; Akudjedu, T.N.; Lawal, O. Radiographer’s confidence in managing patients with claustrophobia during magnetic resonance imaging. Radiography 2022, 28, 148–153. [Google Scholar] [CrossRef] [PubMed]
- McNair, H.A.; Joyce, E.; O’Gara, G.; Jackson, M.; Peet, B.; Huddart, R.A.; Wiseman, T. Radiographer-led online image guided adaptive radiotherapy: A qualitative investigation of the therapeutic radiographer role. Radiography 2021, 27, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Brealey, S.; Scally, A.; Hahn, S.; Thomas, N.; Godfrey, C.; Coomarasamy, A. Accuracy of radiographer plain radiograph reporting in clinical practice: A meta-analysis. Clin. Radiol. 2005, 60, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Mada, M.O.; Hindmarch, P.; Stirling, J.; Davies, J.; Brian, D.; Barnes, A.; Hammers, A.; Gulliver, N.; Herholz, K.; O’Brien, J.; et al. Competencies and training of radiographers and technologists for PET/MR imaging—A study from the UK MR-PET network. Eur. J. Hybrid Imaging 2020, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef]
- Lu, L.; Ko, Y.M.; Chen, H.Y.; Chueh, J.W.; Chen, P.Y.; Cooper, C.L. Patient Safety and Staff Well-Being: Organizational Culture as a Resource. Int. J. Environ. Res. Public Health 2022, 19, 3722. [Google Scholar] [CrossRef]
- Copanitsanou, P.; Fotos, N.; Brokalaki, H. Effects of work environment on patient and nurse outcomes. Br. J. Nurs. Mark. Allen Publ. 2017, 26, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Valentine, N.M.; Nash, J.; Hughes, D.; Douglas, K. Achieving effective staffing through a shared decision-making approach to open-shift management. J. Nurs. Adm. 2008, 38, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Takano, M.; Ueno, C.; Mori, M.; Morimatsu, Y.; Matsumoto, Y.; Kushino, N.; Ishitake, T. Advantages of the Variable Shift System, and Effective Use of Break Time to Better Support the Work Engagement of Nurses on Extended Day Shifts. Kurume Med. J. 2020, 65, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Batt, A.M.; Tavares, W.; Williams, B. The development of competency frameworks in healthcare professions: A scoping review. Adv. Health Sci. Educ. Theory Pract. 2020, 25, 913–987. [Google Scholar] [CrossRef] [PubMed]
- Koruca, H.İ.; Emek, M.S.; Gulmez, E. Development of a new personalized staff-scheduling method with a work-life balance perspective: Case of a hospital. Ann. Oper. Res. 2023, 328, 793–820. [Google Scholar] [CrossRef] [PubMed]
- Loef, B.; van der Beek, A.J.; Holtermann, A.; Hulsegge, G.; van Baarle, D.; Proper, K.I. Objectively measured physical activity of hospital shift workers. Scand. J. Work. Environ. Health 2018, 44, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Yezengaw, T.Y.; Debella, A.; Animen, S.; Aklilu, A.; Feyisa, W.; Hailu, M.; Sime, B.; Mohammed, A.; Deressa, A.; Mussa, I.; et al. Clinical practice competence and associated factors among undergraduate midwifery and nursing sciences students at Bahir Dar city, Northwest Ethiopia. Ann. Med. Surg. 2023, 86, 734–741. [Google Scholar] [CrossRef]
- Budoff, M.J.; Cohen, M.C.; Garcia, M.J.; Hodgson, J.M.; Hundley, W.G.; Lima, J.A.; Manning, W.J.; Pohost, G.M.; Raggi, P.M.; Rodgers, G.P.; et al. ACCF/AHA clinical competence statement on cardiac imaging with computed tomography and magnetic resonance. Circulation 2005, 112, 598–617, Erratum in Circulation 2010, 121, e255–e256. [Google Scholar] [CrossRef]
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28healthcare+professional%5BTitle%2FAbstract%5D%29+AND+%28workload%5BTitle%2FAbstract%5D%29&sort=date&size=200 (accessed on 10 June 2024).
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28healthcare+professional%5BTitle%2FAbstract%5D%29+AND+%28competence%5BTitle%2FAbstract%5D%29&sort=date&size=200 (accessed on 10 June 2024).
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28healthcare+professional%5BTitle%2FAbstract%5D%29+AND+%28performance%5BTitle%2FAbstract%5D%29&sort=date&size=200 (accessed on 10 June 2024).
- Abujudeh, H.H.; Kaewlai, R.; Asfaw, B.A.; Thrall, J.H. Quality initiatives: Key performance indicators for measuring and improving radiology department performance. Radiographics 2010, 30, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.; Ding, A.; Mann, S.; Parsons, M.; Samei, E. Key Performance Indicators for Quality Imaging Practice: Why, What, and How. J. Am. Coll. Radiol. 2022, 19 Pt A, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Di Costanzo, D.J.; Kumaraswamy, L.K.; Shuman, J.; Pavord, D.C.; Hu, Y.; Jordan, D.W.; Waite-Jones, C.; Hsu, A. An introduction to key performance indicators for medical physicists. J. Appl. Clin. Med. Phys. 2022, 23, e13718. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- European Society of Radiology (ESR). Performance indicators for radiation protection management: Suggestions from the European Society of Radiology. Insights Imaging 2020, 11, 134. [Google Scholar] [CrossRef] [PubMed]
- Schultz, C.C.; Shaffer, S.; Fink-Bennett, D.; Winokur, K. Key Performance Indicators in the Evaluation of the Quality of Radiation Safety Programs. Health Phys. 2016, 111, S155–S165. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.A.; Petscavage-Thomas, J.M.; Fotos, J.S.; Bruno, M.A. Quality metrics currently used in academic radiology departments: Results of the QUALMET survey. Br. J. Radiol. 2017, 90, 20160827. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zeng, A.; Gu, Y.; Ma, L.; Tao, X.; Gao, L.; Li, J.; Wang, H.; Jiang, Y. Development of Quality Indicators for the Ultrasound Department through a Modified Delphi Method. Diagnostics 2023, 13, 3678. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nowik, P.; Bujila, R.; Poludniowski, G.; Fransson, A. Quality control of CT systems by automated monitoring of key performance indicators: A two-year study. J. Appl. Clin. Med. Phys. 2015, 16, 254–265. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Karami, M. A design protocol to develop radiology dashboards. Acta Inform. Med. 2014, 22, 341–346. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sreedharan, J.; Subbarayalu, A.V.; Kamalasanan, A.; Albalawi, I.; Krishna, G.G.; Alahmari, A.D.; Alsalamah, J.A.; Alkhathami, M.G.; Alenezi, M.; Alqahtani, A.S.; et al. Key Performance Indicators: A Framework for Allied Healthcare Educational Institutions. Clinicoecon Outcomes Res. 2024, 16, 173–185. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Portoghese, I.; Galletta, M.; Coppola, R.C.; Finco, G.; Campagna, M. Burnout and workload among health care workers: The moderating role of job control. Saf. Health Work. 2014, 5, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, R.; Lagarde, M. Does high workload reduce the quality of healthcare? Evidence from rural Senegal. J. Health Econ. 2022, 82, 102600. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rostami, F.; Babaei-Pouya, A.; Teimori-Boghsani, G.; Jahangirimehr, A.; Mehri, Z.; Feiz-Arefi, M. Mental Workload and Job Satisfaction in Healthcare Workers: The Moderating Role of Job Control. Front. Public Health 2021, 9, 683388. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jose, A.; Tortorella, G.L.; Vassolo, R.; Kumar, M.; Mac Cawley, A.F. Professional Competence and Its Effect on the Implementation of Healthcare 4.0 Technologies: Scoping Review and Future Research Directions. Int. J. Environ. Res. Public Health 2022, 20, 478. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yaqoob Mohammed Al Jabri, F.; Kvist, T.; Azimirad, M.; Turunen, H. A systematic review of healthcare professionals’ core competency instruments. Nurs. Health Sci. 2021, 23, 87–102. [Google Scholar] [CrossRef] [PubMed]
- Jarva, E.; Oikarinen, A.; Andersson, J.; Pramila-Savukoski, S.; Hammarén, M.; Mikkonen, K. Healthcare professionals’ digital health competence profiles and associated factors: A cross-sectional study. J. Adv. Nurs. 2024. [Google Scholar] [CrossRef] [PubMed]
- Krijgsheld, M.; Tummers, L.G.; Scheepers, F.E. Job performance in healthcare: A systematic review. BMC Health Serv. Res. 2022, 22, 149. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rana, W.; Mukhtar, S.; Mukhtar, S. Job satisfaction, performance appraisal, reinforcement and job tasks in medical healthcare professionals during the COVID-19 pandemic outbreak. Int. J. Health Plan. Manag. 2022, 37, 2345–2353. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Crawshaw, J.; Meyer, C.; Antonopoulou, V.; Antony, J.; Grimshaw, J.M.; Ivers, N.; Konnyu, K.; Lacroix, M.; Presseau, J.; Simeoni, M.; et al. Identifying behaviour change techniques in 287 randomized controlled trials of audit and feedback interventions targeting practice change among healthcare professionals. Implement. Sci. 2023, 18, 63, Erratum in Implement. Sci. 2023, 18, 73. [Google Scholar] [CrossRef] [PubMed]
- Chandramohan, A.; Krothapalli, V.; Augustin, A.; Kandagaddala, M.; Thomas, H.M.; Sudarsanam, T.D.; Jagirdar, A.; Govil, S.; Kalyanpur, A. Teleradiology and technology innovations in radiology: Status in India and its role in increasing access to primary health care. Lancet Reg. Health Southeast. Asia 2023, 23, 100195. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lepri, G.; Oddi, F.; Gulino, R.A.; Giansanti, D. Reimagining Radiology: A Comprehensive Overview of Reviews at the Intersection of Mobile and Domiciliary Radiology over the Last Five Years. Bioengineering 2024, 11, 216. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Giansanti, D.; Rossi, I.; Monoscalco, L. Lessons from the COVID-19 Pandemic on the Use of Artificial Intelligence in Digital Radiology: The Submission of a Survey to Investigate the Opinion of Insiders. Healthcare 2021, 9, 331. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Key Elements |
|---|
| Impact of the SRH tool in clinical practice |
| Applicability across various healthcare profiles |
| Value in decision making |
| Competence analysis |
| Simple understanding and training |
| Improvement in clinical risk management |
| Participants | Males/Females | Mean Age ± St.d. | Min/Max Age |
|---|---|---|---|
| 29 | 9/20 | 50.8 ± 9.5 | 32/64 |
| Key Discussion Topics | Unbiased Feedback | Responses Provided to Feedback |
|---|---|---|
| Delineation of “target areas” | “Without guidelines, how can the focus group outline the target areas?” | The focus group consists of experienced healthcare professionals who can identify specific areas of focus through a comprehensive evaluation. |
| “Are target areas customizable even after importing SRH tools into clinical practice?” | These target areas can be adjusted as needed, and the SRH tool will update evaluations accordingly based on the new target areas. | |
| Reporting of examination performed by individual healthcare professional | “We cannot implement the SRH tool because the activities and performance metrics of these professionals cannot be measured into a software platform.” | The functionality of the SRH tool is inevitably compromised if professionals are unable to provide a report of the examinations they have performed. |
| “In my clinical practice, examinations are usually performed and recorded by two healthcare professionals. Would the SRH tool have problems extracting the data in this case?” | No, the SRH tool is able to retrieve and process the data by defining specific queries, taking into account that there are multiple examiners (even more than one). | |
| The use of the SRH tool for optimizing work shift | “The SRH tool does not allow automatic management of emergency situations (e.g., employees who do not report their absence unannounced).” | The SRH tool was not developed to manage critical situations independently, but it helps the coordinator to optimize the work shift based on the skills of the individual healthcare professionals. In the event of a sudden absence, it helps the coordinator to find a replacement. |
| SRH tool improves decision-making processes | “The most common criticism of a coordinator relates to subjectivity when planning work shifts. Can the SRH tool help to make the management of work shifts more objective?” | Yes. By providing objective, data-driven insights, the SRH tool enables coordinators to make management decisions with confidence and accuracy. |
| Reference | Relevant KPIs |
|---|---|
| Abujudeh et al., 2010 [22] | Report turnaround time, quality and efficiency metrics |
| Nelson et al., 2022 [23] | Error rates, user satisfaction |
| DiCostanzo et al., 2022 [24] | Frequency and quality of communication updates |
| European Society of Radiology, 2020 [25] | Transparency and engagement levels |
| Schultz et al., 2016 [26] | Team meeting effectiveness, feedback quality |
| Walker et al., 2017 [27] | Cross-functional collaboration metrics |
| Zeng et al., 2023 [28] | Leadership skills development, decision-making efficacy |
| Nowik et al., 2015 [29] | Success of mentorship programs |
| Karami, 2014 [30] | Accountability, accuracy in KPI tracking |
| Sreedharan et al., 2024 [31] | Data accessibility, transparency metrics |
| Key Area | Insight | References |
|---|---|---|
| Defining Clear Objectives and Selecting Relevant KPIs for the SRH Tool | Aligning the objectives of the SRH tool with the overarching goals of the healthcare organization ensures that the selected KPIs accurately measure performance, quality, and outcomes. | [22,23] |
| Establishing Transparent Communication Channels for the SRH Tool | Implementing various communication channels such as team meetings, digital platforms, and email updates facilitates the timely dissemination of information within healthcare organizations, specifically tailored to the implementation of the SRH tool. | [24,25] |
| Fostering a Collaborative Environment for the SRH Tool | Regular team meetings and cross-functional teams promote open dialogue, enabling diverse perspectives on KPI results and improvement strategies that are essential for successful healthcare delivery, including the integration and utilization of the SRH tool. | [26,27] |
| Implementing Leadership Development Programs for the SRH Tool | Leadership development programs equip leaders with the necessary skills to interpret KPI data and make informed decisions, complemented by mentorship programs for guidance and support to emerging leaders, thereby driving organizational success, including the implementation and utilization of the SRH tool. | [28,29] |
| Empowering Team Members for the SRH Tool | Delegating responsibilities related to KPI tracking and providing access to data and analysis tools fosters a sense of ownership and accountability among team members is crucial for organizational effectiveness, including the successful integration and utilization of the SRH tool. | [30,31] |
| Recognizing and Rewarding Achievements for the SRH Tool | Regular recognition and rewards based on KPI progress enhance morale and motivation within the team, contributing to a positive work culture and driving overall performance, including the successful implementation and utilization of the SRH tool. | [22,23] |
| Continuous Improvement and Adaptation for the SRH Tool | Establishing feedback loops and remaining agile allow organizations to adapt strategies and KPIs in response to changing organizational goals and performance data, which is essential for continuous improvement and organizational excellence, including the ongoing refinement and adaptation of the SRH tool. | [24,25] |
| Defining Clear Objectives and Selecting Relevant KPIs for the SRH Tool | Aligning the objectives of the SRH tool with the overarching goals of the healthcare organization ensures that the selected KPIs accurately measure performance, quality, and outcomes. | [22,23] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lastrucci, A.; Wandael, Y.; Orlandi, G.; Barra, A.; Chiti, S.; Gigli, V.; Marletta, M.; Pelliccia, D.; Tonietti, B.; Ricci, R.; et al. Precision Workforce Management for Radiographers: Monitoring and Managing Competences with an Automatic Tool. J. Pers. Med. 2024, 14, 669. https://doi.org/10.3390/jpm14070669
Lastrucci A, Wandael Y, Orlandi G, Barra A, Chiti S, Gigli V, Marletta M, Pelliccia D, Tonietti B, Ricci R, et al. Precision Workforce Management for Radiographers: Monitoring and Managing Competences with an Automatic Tool. Journal of Personalized Medicine. 2024; 14(7):669. https://doi.org/10.3390/jpm14070669
Chicago/Turabian StyleLastrucci, Andrea, Yannick Wandael, Giovanni Orlandi, Angelo Barra, Stefano Chiti, Valentina Gigli, Massimo Marletta, Davide Pelliccia, Barbara Tonietti, Renzo Ricci, and et al. 2024. "Precision Workforce Management for Radiographers: Monitoring and Managing Competences with an Automatic Tool" Journal of Personalized Medicine 14, no. 7: 669. https://doi.org/10.3390/jpm14070669
APA StyleLastrucci, A., Wandael, Y., Orlandi, G., Barra, A., Chiti, S., Gigli, V., Marletta, M., Pelliccia, D., Tonietti, B., Ricci, R., & Giansanti, D. (2024). Precision Workforce Management for Radiographers: Monitoring and Managing Competences with an Automatic Tool. Journal of Personalized Medicine, 14(7), 669. https://doi.org/10.3390/jpm14070669