
Advancing Cancer Care in Colombia: Results of the First In Situ Implementation of Comprehensive Genomic Profiling

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Comprehensive Genomic Profiling Test
2.3. Covariates
- Personal data: Name, age, identification document, city of residence, and sex.
- Medical data: Diagnosis based on histopathologic classification of the tumor, and cancer staging based on TNM Staging System or Stages I–IV. Also, pathology report and information on previous cancer panels and microsatellite instability results.
- Therapy: Details of the response to their first and second line treatments according to the evolution of tumor size.
- Cancer type and sex are nominal categorical variables that were analyzed using absolute and relative frequencies.
2.4. DNA and RNA Extraction
2.5. TSO500 Library Preparation and Next-Generation Sequencing (NGS)
2.5.1. Library Prep DNA Workflow
2.5.2. Library Prep RNA Workflow
2.5.3. Enrichment DNA and RNA Workflow
2.6. Bioinformatic Analysis of Sequencing Data
2.7. Variant Analysis and Interpretation
2.8. PD-L1 Expression (Immunohistochemistry) Test
2.9. Ethical Considerations
2.10. Statistical Analysis
3. Results
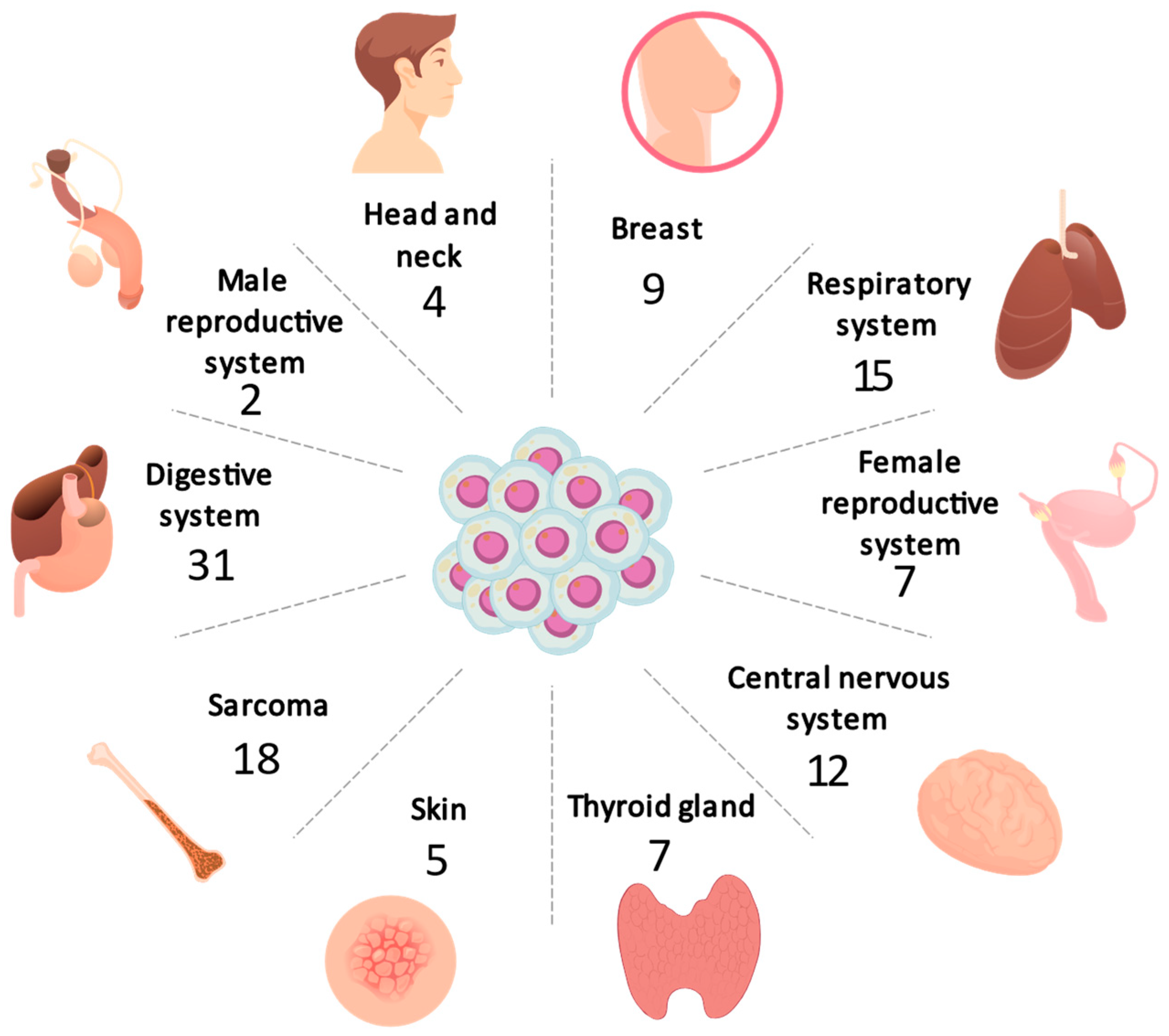
3.1. Distribution of Cancer
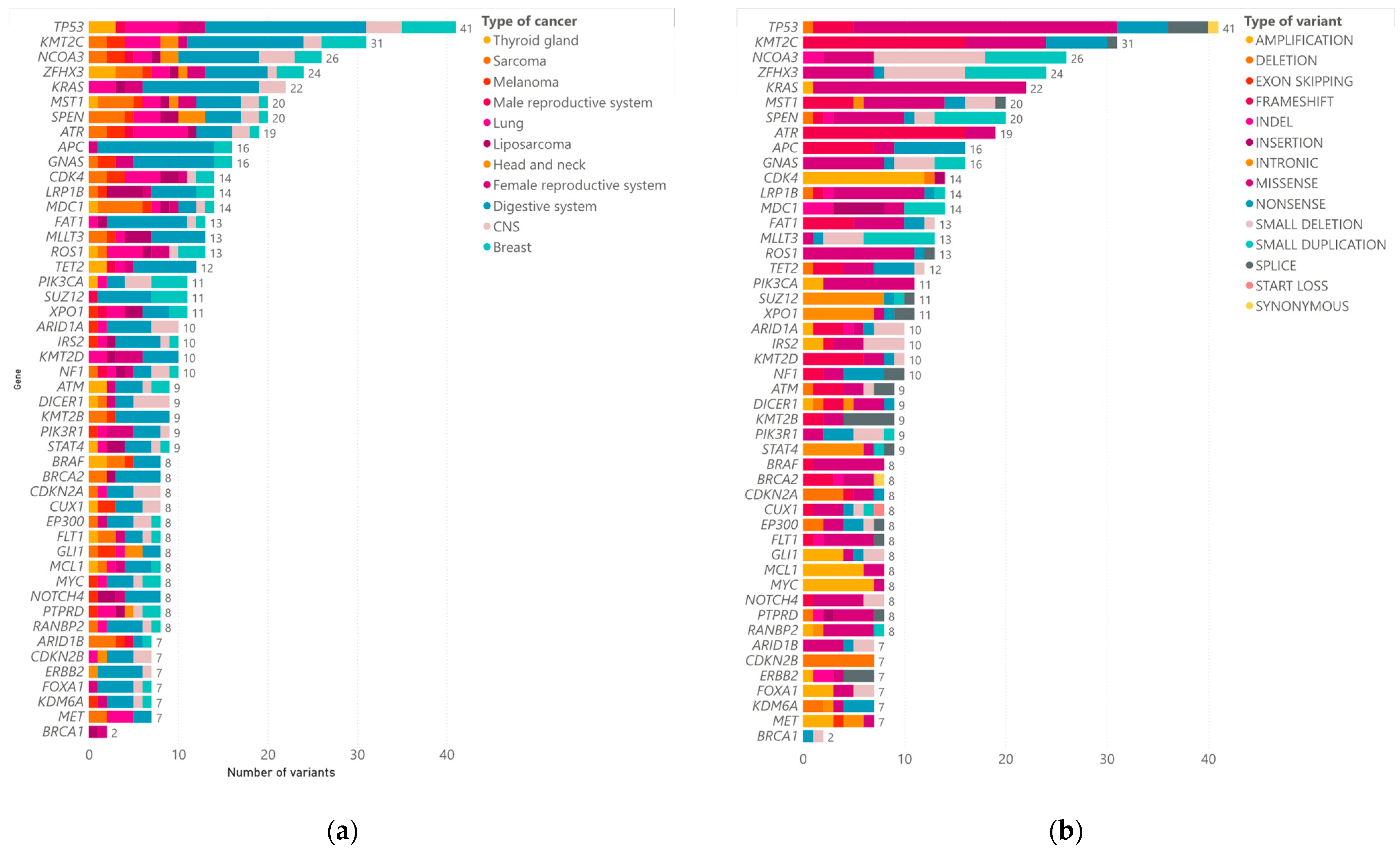
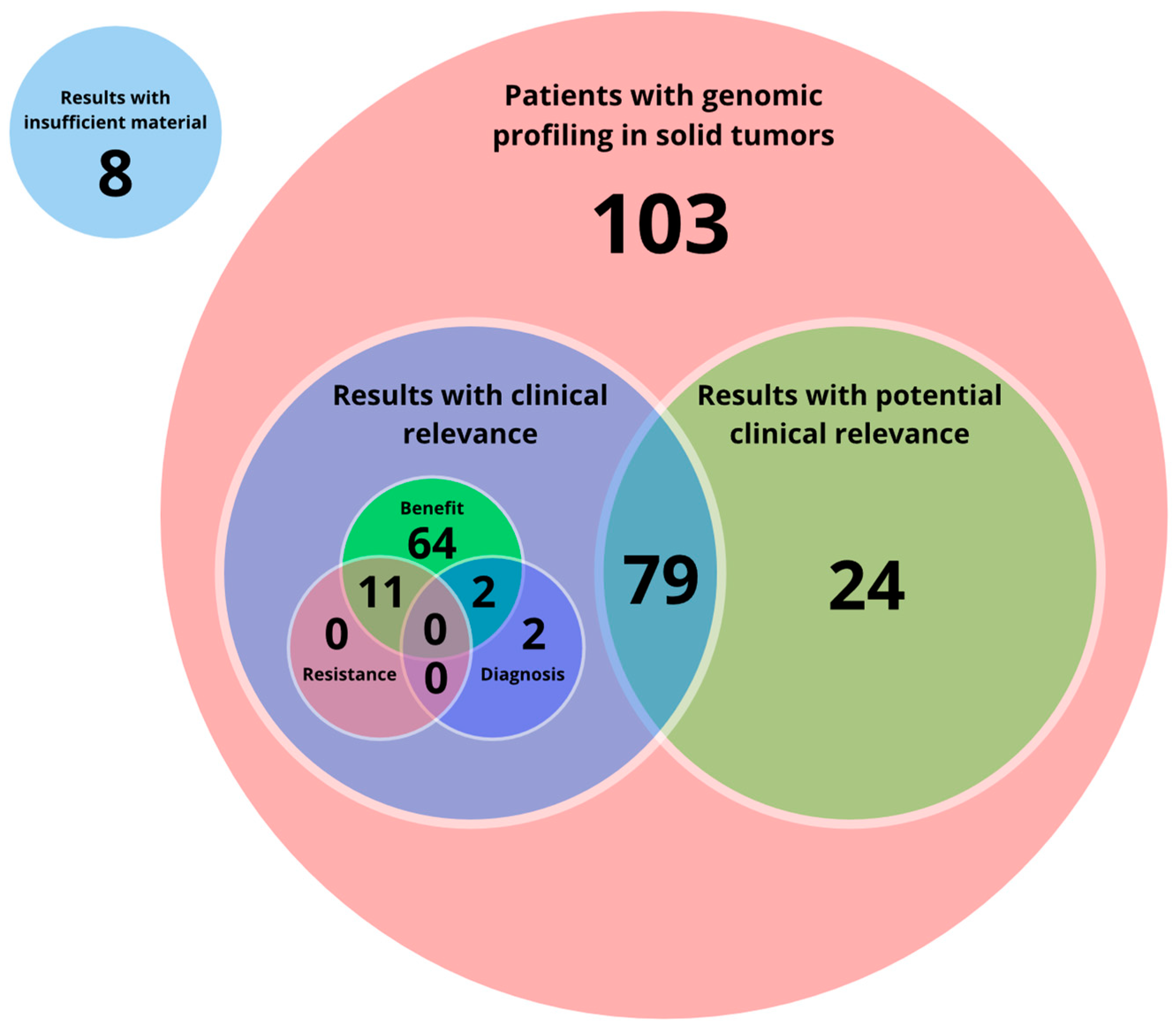
3.2. CGP Results
3.3. Actionable Alterations
- Digestive system: This group includes 31 patients, namely 14 men and 17 women with tumors of the rectum, pancreas, liver, intestine, colon and stomach. Out of 31 patients with tumors of the digestive system, positive results (Tier IA/IB) were found in 20 patients (9 men, 11 women), and 1 female patient could not be processed due to poor sample quality. The most frequently mutated genes in this type of cancer were TP53 (51.61%), KMT2C (35.48%), APC (32.25%), NCOA3 (25.80%), and KRAS (29.03%)
- Lung: Out of 14 patients with lung tumors, positive results (Tier IA/IB) were found in 8 patients (3 men, 5 women). The most frequent findings in these positive patients were MET exon 14 (METex14) skipping and EGFR exon 19 deletion. The most frequently mutated genes were ATR (33.3%), EGFR (26.6%), KMT2C (20%), and ROS1 (20%).
- CNS: A total of 12 samples from patients with central nervous system tumors, including glioblastoma, astrocytoma, medulloblastoma, glioma, and meningioma, were analyzed. Out of 12 patients with CNS tumors, positive results (Tier IA/IB) were found in 2 patients (1 men, 1 women), one of which had mutations in the IDH1 gene and the other in the NF1 gene. The most frequent mutations in this type of tumors were in DICER1 (25%) and NCOA3 (25%) genes.
- Sarcoma: Out of 14 patients with sarcoma, positive results (Tier I/II) were found in 2 patients (2 men) with BRAF p.Val600Glu. One patient could not be processed due to poor sample quality. The most frequently mutated genes in this type of cancer were SPEN (28.57%), NUTM1 (21.42%), MST1 (21.42%), and ZFHX3 (21.42%).
- Breast: Out of nine patients with breast tumors, positive results (Tier IA/IB) were found in five patients (five women). The most frequently mutated genes were TP53 (55.55%), ZFHX3 (44.4%), SPEN (55.5%), PIK3CA (33.3%), and SUZ12 (44.4%).
- Female reproductive system: Out seven patients with female reproductive system tumors, positive results (Tier IA/IB) were found in three patients (42.85%). Half of the patients with ovarian tumors had mutations in TP53 and the only patient with endometrial cancer had an oncogenic variant in BRCA1. The most frequently mutated genes in this type of cancer were TP53 and KMT2D (42.85%).
- Thyroid gland: Out of seven patients with thyroid gland tumors, positive results (Tier IA/IB) were found in four patients (two women, two men), whilst three patients could not be processed due to poor sample quality. Two patients had BRAF p.Val600Glu variant findings. ZFHX3 (42.85%) was the most frequently mutated gene.
- Melanoma: Out of five patients with thyroid gland tumors, positive results (Tier IA/IB) were found in two patients (one man, one woman) with BRAF p.Val600Glu.
- Head and neck: Out of four patients with head and neck tumors, none were found to be positive (Level I/II). However, the PAX3-FOXO fusion was found in a 17-year-old patient with an adenoid cystic carcinoma of the trachea.
- Liposarcoma: Out of five patients with liposarcoma, positive results (Tier IA/IB) were found in two patients (two women). The most frequently mutated gene was LRP1B (75%).
- Male reproductive system: Positive results (Level IA/IB) were found in two of two patients (100%) evaluated with tumors in the male reproductive system.
- Rare tumors: In this group, there is a male patient with a diagnosis of PEComa. The recommended treatment for this finding consisted of mTOR inhibitors, such as sirolimus, temsirolimus, and everolimus.
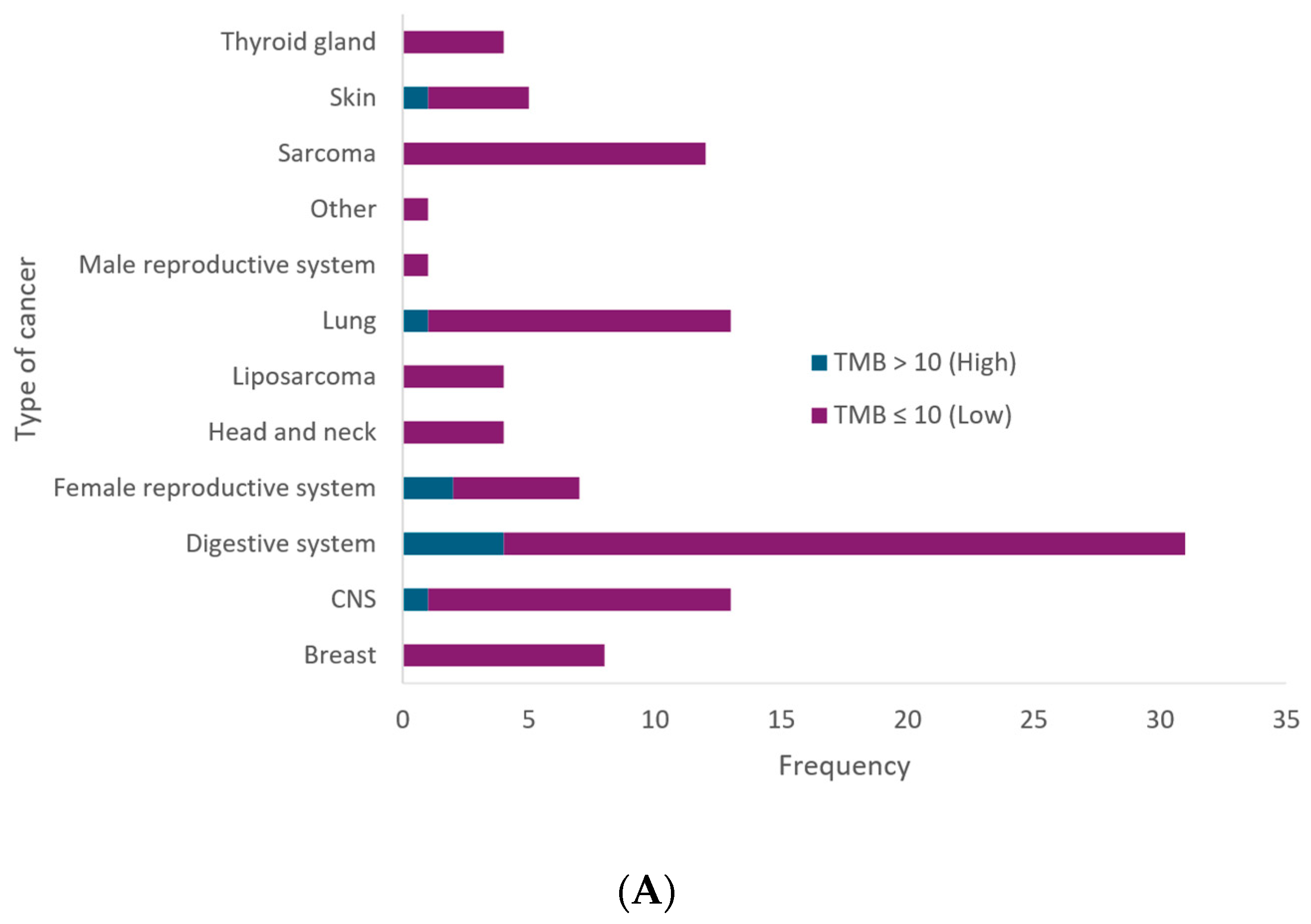
3.4. MSI and TMB
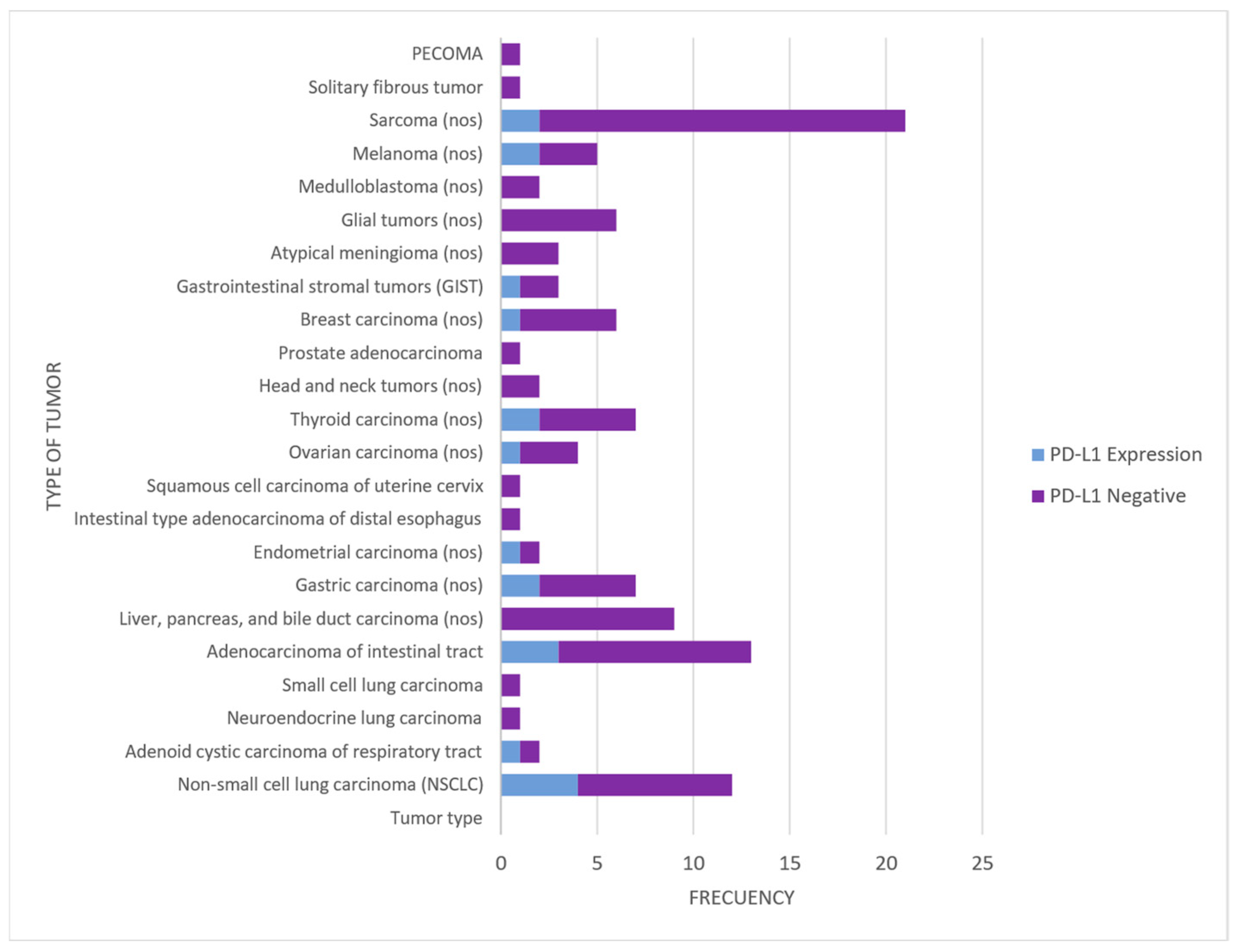
3.5. PD-L1 Expression (Immunohistochemistry)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malone, E.R.; Oliva, M.; Sabatini, P.J.B.; Stockley, T.L.; Siu, L.L. Molecular profiling for precision cancer therapies. Genome Med. 2020, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Hoeben, A.; Joosten, E.A.J.; van den Beuken-van Everdingen, M.H.J. Personalized Medicine: Recent Progress in Cancer Therapy. Cancers 2021, 13, 242. [Google Scholar] [CrossRef] [PubMed]
- Rassy, E.; Heard, J.-M.; Andre, F. The paradigm shift to precision oncology between political will and cultural acceptance. ESMO Open 2023, 8, 101622. [Google Scholar] [CrossRef] [PubMed]
- Bhai, P.; Turowec, J.; Santos, S.; Kerkhof, J.; Pickard, L.; Foroutan, A.; Breadner, D.; Cecchini, M.; Levy, M.A.; Stuart, A.; et al. Molecular profiling of solid tumors by next-generation sequencing: An experience from a clinical laboratory. Front. Oncol. 2023, 13, 1208244. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.; Barlesi, F.; Lolkema, M.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: A report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef]
- Tjota, M.Y.; Segal, J.P.; Wang, P. Clinical Utility and Benefits of Comprehensive Genomic Profiling in Cancer. J. Appl. Lab. Med. 2024, 9, 76–91. [Google Scholar] [CrossRef]
- Pujol, N.; Heeke, S.; Bontoux, C.; Boutros, J.; Ilié, M.; Hofman, V.; Marquette, C.-H.; Hofman, P.; Benzaquen, J. Molecular Profiling in Non-Squamous Non-Small Cell Lung Carcinoma: Towards a Switch to Next-Generation Sequencing Reflex Testing. J. Pers. Med. 2022, 12, 1684. [Google Scholar] [CrossRef]
- Schram, A.M.; Chang, M.T.; Jonsson, P.; Drilon, A. Fusions in solid tumours: Diagnostic strategies, targeted therapy, and acquired resistance. Nat. Rev. Clin. Oncol. 2017, 14, 735–748. [Google Scholar] [CrossRef]
- Palmeri, M.; Mehnert, J.; Silk, A.; Jabbour, S.; Ganesan, S.; Popli, P.; Riedlinger, G.; Stephenson, R.; de Meritens, A.; Leiser, A.; et al. Real-world application of tumor mutational burden-high (TMB-high) and microsatellite instability (MSI) confirms their utility as immunotherapy biomarkers. ESMO Open 2022, 7, 100336. [Google Scholar] [CrossRef]
- Marcus, L.; Lemery, S.J.; Keegan, P.; Pazdur, R. FDA Approval Summary: Pembrolizumab for the Treatment of Microsatellite Instability-High Solid Tumors. Clin. Cancer Res. 2019, 25, 3753–3758. [Google Scholar] [CrossRef]
- Tang, Q.; Chen, Y.; Li, X.; Long, S.; Shi, Y.; Yu, Y.; Wu, W.; Han, L.; Wang, S. The role of PD-1/PD-L1 andapplication of immune-checkpointinhibitors in human cancers. Front. Immunol. 2022, 13, 964442. [Google Scholar] [CrossRef] [PubMed]
- Gatalica, Z.; Snyder, C.; Maney, T.; Ghazalpour, A.; Holterman, D.A.; Xiao, N.; Overberg, P.; Rose, I.; Basu, G.D.; Vranic, S.; et al. Programmed cell death 1 (PD-1) and its ligand (PD-L1) in common cancers and their correlation with molecular cancer type. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2965–2970. [Google Scholar] [CrossRef] [PubMed]
- Cifuentes, C.; Lombana, M.; Vargas, H.; Laguado, P.; Ruiz-Patiño, A.; Rojas, L.; Navarro, U.; Vargas, C.; Ricaurte, L.; Arrieta, O.; et al. Application of Comprehensive Genomic Profiling-Based Next-Generation Sequencing Assay to Improve Cancer Care in a Developing Country. Cancer Control J. Moffitt Cancer Cent. 2023, 30, 10732748231175256. [Google Scholar] [CrossRef]
- Mantilla, W.A.; Sanabria-Salas, M.C.; Baldion, A.M.; Sua, L.F.; Gonzalez, D.M.; Lema, M. NGS in Lung, Breast, and Unknown Primary Cancer in Colombia: A Multidisciplinary Consensus on Challenges and Opportunities. JCO Glob. Oncol. 2021, 7, 1012–1023. [Google Scholar] [CrossRef]
- Vranic, S.; Gatalica, Z. PD-L1 testing by immunohistochemistry in Immuno-Oncology. Bosn. J. Basic Med. Sci. 2023, 23, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef]
- Horak, P.; Griffith, M.; Danos, A.M.; Pitel, B.A.; Madhavan, S.; Liu, X.; Chow, C.; Williams, H.; Carmody, L.; Barrow-Laing, L.; et al. Standards for the classification of pathogenicity of somatic variants in cancer (oncogenicity): Joint recommendations of Clinical Genome Resource (ClinGen), Cancer Genomics Consortium (CGC), and Variant Interpretation for Cancer Consortium (VICC). Anesth. Analg. 2022, 24, 986–998. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H., Jr.; et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: Prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. 2024. Available online: https://www.nccn.org/professionals/physician_gls/ (accessed on 12 April 2024).
- Marletta, S.; Fusco, N.; Munari, E.; Luchini, C.; Cimadamore, A.; Brunelli, M.; Querzoli, G.; Martini, M.; Vigliar, E.; Colombari, R.; et al. Atlas of PD-L1 for Pathologists: Indications, Scores, Diagnostic Platforms and Reporting Systems. J. Pers. Med. 2022, 12, 1073. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Brgfx, Macrovector, Studiogstock, and pch.vector—Freepik. Available online: https://www.freepik.com/ (accessed on 12 April 2024).
- Gamboa, O.; Bonilla, C.E.; Quitian, D.; Torres, G.F.; Buitrago, G.; Cardona, A.F. Cost-Effectiveness of Comprehensive Genomic Profiling in Patients with Non–Small Cell Lung Cancer for the Colombian Health System. Value Health Reg. Issues 2024, 39, 115–125. [Google Scholar] [CrossRef]
- Yu, D.; Ou, Z.; Zhang, W.; He, H.; Li, Y.; He, W.; Zhang, M.; Gao, Y.; Wu, F.; Chen, Q. Global and national trends in years of life lost and years lived with disability caused by three common gastrointestinal cancers from 1990 to 2019. BMC Gastroenterol. 2022, 22, 493. [Google Scholar] [CrossRef]
- Fitzmaurice, C.; Akinyemiju, T.F.; al Lami, F.H.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; Anderson, B.O.; et al. Global Burden of Disease Cancer Collaboration. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2018, 4, 1553–1568. [Google Scholar] [CrossRef]
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global burden of 5 major types of gastrointestinal cancer. Gastroenterology 2020, 159, 335–349.e15. [Google Scholar] [CrossRef] [PubMed]
- Sholl, L.M.; Do, K.; Shivdasani, P.; Cerami, E.; Dubuc, A.M.; Kuo, F.C.; Garcia, E.P.; Jia, Y.; Davineni, P.; Abo, R.P.; et al. Institutional implementation of clinical tumor profiling on an unselected cancer population. J. Clin. Investig. 2016, 1, e87062. [Google Scholar] [CrossRef] [PubMed]
- Galanina, N.; Bejar, R.; Choi, M.; Goodman, A.; Wieduwilt, M.; Mulroney, C.; Kim, L.; Yeerna, H.; Tamayo, P.; Vergilio, J.-A.; et al. Comprehensive Genomic Profiling Reveals Diverse but Actionable Molecular Portfolios across Hematologic Malignancies: Implications for Next Generation Clinical Trials. Cancers 2018, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.J.; Tang, M.; Rajaram, S.; O’Grady, S.; Crown, J. Targeting Mutant p53 for Cancer Treatment: Moving Closer to Clinical Use? Cancers 2022, 14, 4499. [Google Scholar] [CrossRef]
- Ni, C.; Wang, X.; Liu, S.; Zhang, J.; Luo, Z.; Xu, B. KMT2C mutation as a predictor of immunotherapeutic efficacy in colorectal cancer. Sci. Rep. 2024, 14, 8284. [Google Scholar] [CrossRef]
- de Semir, D.; Bezrookove, V.; Nosrati, M.; Dar, A.A.; Miller, J.R., 3rd; Leong, S.P.; Kim, K.B.; Liao, W.; Soroceanu, L.; McAllister, S.; et al. Nuclear Receptor Coactivator NCOA3 Regulates UV Radiation–Induced DNA Damage and Melanoma Susceptibility. Cancer Res. 2021, 81, 2956–2969. [Google Scholar] [CrossRef]
- Paric, A.; Karan-Krizanac, D.; Saric, I.; Vranic, S. A Chromosome 9p24.1 Amplification in Colorectal Cancer with Metastases to the Kidney and Adrenal Gland: A Case Report. Case Rep. Oncol. 2023, 16, 803–810. [Google Scholar] [CrossRef]
- Gupta, S.; Cheville, J.C.; Jungbluth, A.A.; Zhang, Y.; Zhang, L.; Chen, Y.-B.; Tickoo, S.K.; Fine, S.W.; Gopalan, A.; Al-Ahmadie, H.A.; et al. JAK2/PD-L1/PD-L2 (9p24.1) amplifications in renal cell carcinomas with sarcomatoid transformation: Implications for clinical management. Mod. Pathol. 2019, 32, 1344–1358. [Google Scholar] [CrossRef]
- Goodman, A.M.; Piccioni, D.; Kato, S.; Boichard, A.; Wang, H.-Y.; Frampton, G.; Lippman, S.M.; Connelly, C.; Fabrizio, D.; Miller, V.; et al. Prevalence of PDL1 Amplification and Preliminary Response to Immune Checkpoint Blockade in Solid Tumors. JAMA Oncol. 2018, 4, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Wardell, C.P.; Fujita, M.; Yamada, T.; Simbolo, M.; Fassan, M.; Karlic, R.; Polak, P.; Kim, J.; Hatanaka, Y.; Maejima, K.; et al. Genomic characterization of biliary tract cancers identifies driver genes and predisposing mutations. J. Hepatol. 2018, 68, 959–969. [Google Scholar] [CrossRef] [PubMed]
- Bonneville, R.; Krook, M.A.; Kautto, E.A.; Miya, J.; Wing, M.R.; Chen, H.-Z.; Reeser, J.W.; Yu, L.; Roychowdhury, S. Landscape of Microsatellite Instability Across 39 Cancer Types. JCO Precis. Oncol. 2017, 2017, PO.17.00073. [Google Scholar] [CrossRef] [PubMed]
- Ashktorab, H.; Ahuja, S.; Kannan, L.; Llor, X.; Ellis, N.A.; Xicola, R.M.; Laiyemo, A.O.; Carethers, J.M.; Brim, H.; Nouraie, M. A meta-analysis of MSI frequency and race in colorectal cancer. Oncotarget 2016, 7, 34546–34557. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef]
- Dupain, C.; Gutman, T.; Girard, E.; Kamoun, C.; Marret, G.; Castel-Ajgal, Z.; Sablin, M.-P.; Neuzillet, C.; Borcoman, E.; Hescot, S.; et al. Tumor mutational burden assessment and standardized bioinformatics approach using custom NGS panels in clinical routine. BMC Biol. 2024, 22, 43. [Google Scholar] [CrossRef]
- Sha, D.; Jin, Z.; Budczies, J.; Kluck, K.; Stenzinger, A.; Sinicrope, F.A. Tumor Mutational Burden as a Predictive Biomarker in Solid Tumors. Cancer Discov. 2020, 10, 1808–1825. [Google Scholar] [CrossRef]
- Barroso-Sousa, R.; Jain, E.; Cohen, O.; Kim, D.; Buendia-Buendia, J.; Winer, E.; Lin, N.; Tolaney, S.; Wagle, N. Prevalence and mutational determinants of high tumor mutation burden in breast cancer. Ann. Oncol. 2020, 31, 387–394. [Google Scholar] [CrossRef]
- Zhang, C.; Yang, Q. Predictive Values of Programmed Cell Death-Ligand 1 Expression for Prognosis, Clinicopathological Factors, and Response to Programmed Cell Death-1/Programmed Cell Death-Ligand 1 Inhibitors in Patients with Gynecological Cancers: A Meta-Analysis. Front. Oncol. 2021, 10, 572203. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, Y.-Z.; Wang, J.-S.; Du, J.; Tang, X.-L.; Xiao, J.-P. Clinical benefit analysis of PD-1 inhibitors in patients with advanced, recurrent or metastatic cervical cancer: A meta-analysis and systematic review. Front. Immunol. 2024, 15, 1305810. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, Y.; Aiob, A.; Kim, H.; Suh, D.H.; Kim, K.; Kim, Y.B.; No, J.H. Clinical Implication of PD-L1 Expression in Patients with Endometrial Cancer. Biomedicines 2023, 11, 2691. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Saito, H.; Kono, Y.; Murakami, Y.; Shishido, Y.; Kuroda, H.; Matsunaga, T.; Fukumoto, Y.; Osaki, T.; Ashida, K.; Fujiwara, Y. Highly Activated PD-1/PD-L1 Pathway in Gastric Cancer with PD-L1 Expression. Anticancer. Res. 2018, 38, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Guo, X.; Sun, Q.; Zhang, M.; Qi, L.; Li, Y.; Chen, L.; Gu, Y.; Guo, Z.; Zhao, W. The influence of cancer tissue sampling on the identification of cancer characteristics. Sci. Rep. 2015, 5, 15474. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Cancer | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Liver | 2 | 1.8% | 1 | 0.9% | 3 | 2.7% |
| Colorectal | 5 | 4.5% | 5 | 4.5% | 10 | 9.0% |
| Pancreas | 3 | 2.7% | 1 | 0.9% | 4 | 3.6% |
| Gastric | 3 | 2.7% | 7 | 6.3% | 10 | 9.0% |
| GIST | 1 | 0.9% | 1 | 0.9% | 2 | 1.8% |
| Bile duct | 0 | 0.0% | 2 | 1.8% | 2 | 1.8% |
| Lung | 7 | 6.3% | 8 | 7.2% | 15 | 13.5% |
| Astrocytoma | 0 | 0.0% | 2 | 1.8% | 2 | 1.8% |
| Glioblastoma | 2 | 1.8% | 0 | 0.0% | 2 | 1.8% |
| Glioma | 2 | 1.8% | 0 | 0.0% | 2 | 1.8% |
| Meningioma | 1 | 0.9% | 2 | 1.8% | 3 | 2.7% |
| Medulloblastoma | 1 | 0.9% | 1 | 0.9% | 2 | 1.8% |
| Primary CNS sarcoma | 0 | 0.0% | 1 | 0.9% | 1 | 0.9% |
| Sarcoma | 9 | 8.1% | 5 | 4.5% | 14 | 12.6% |
| Breast | 0 | 0.0% | 9 | 8.1% | 9 | 8.1% |
| Cervical | 0 | 0.0% | 1 | 0.9% | 1 | 0.9% |
| Ovarian | 0 | 0.0% | 4 | 3.6% | 4 | 3.6% |
| Endometrial | 0 | 0.0% | 1 | 0.9% | 1 | 0.9% |
| Uterus | 0 | 0.0% | 1 | 0.9% | 1 | 0.9% |
| Thyroid gland | 4 | 3.6% | 3 | 2.7% | 7 | 6.3% |
| Melanoma | 2 | 1.8% | 3 | 2.7% | 5 | 4.5% |
| Nose | 1 | 0.9% | 1 | 0.9% | 2 | 1.8% |
| Salivary gland | 1 | 0.9% | 0 | 0.0% | 1 | 0.9% |
| Trachea | 0 | 0.0% | 1 | 0.9% | 1 | 0.9% |
| Liposarcoma | 2 | 1.8% | 2 | 1.8% | 4 | 3.6% |
| Prostate | 2 | 1.8% | 0 | 0.0% | 2 | 1.8% |
| PEComa | 1 | 0.9% | 0 | 0.0% | ||
| Total | 49 | 62 | 111 | |||
| Tumor Type | Frequency | PD-L1 Expression |
|---|---|---|
| Non-small-cell lung carcinoma (NSCLC) | 12 | 4 (33%) |
| Adenoid cystic carcinoma of respiratory tract | 2 | 1 (50%) |
| Neuroendocrine lung carcinoma | 1 | 0 |
| Small-cell lung carcinoma | 1 | 0 |
| Adenocarcinoma of intestinal tract | 13 | 3 (23%) |
| Liver, pancreas, and bile duct carcinoma (nos) | 9 | 0 |
| Gastric carcinoma (nos) | 7 | 2 (29%) |
| Endometrial carcinoma (nos) | 2 | 1 (50%) |
| Intestinal type adenocarcinoma of distal esophagus | 1 | 0 |
| Squamous cell carcinoma of uterine cervix | 1 | 0 |
| Ovarian carcinoma (nos) | 4 | 1 (25%) |
| Thyroid carcinoma (nos) | 7 | 2 (29%) |
| Head and neck tumors (nos) | 2 | 0 |
| Prostate adenocarcinoma | 1 | 0 |
| Breast carcinoma (nos) | 6 | 1 (17%) |
| Gastrointestinal stromal tumors (GIST) | 3 | 1 (33%) |
| Atypical meningioma (nos) | 3 | 0 |
| Glial tumors (nos) | 6 | 0 |
| Medulloblastoma (nos) | 2 | 0 |
| Melanoma (nos) | 5 | 2 (40%) |
| Sarcoma (nos) | 21 | 2 (10%) |
| Solitary fibrous tumor | 1 | 0 |
| PECOMA | 1 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López Rivera, J.J.; Rueda-Gaitán, P.; Rios Pinto, L.C.; Rodríguez Gutiérrez, D.A.; Gomez-Lopera, N.; Lamilla, J.; Rojas Aguirre, F.A.; Bernal Vaca, L.; Isaza-Ruget, M.A. Advancing Cancer Care in Colombia: Results of the First In Situ Implementation of Comprehensive Genomic Profiling. J. Pers. Med. 2024, 14, 975. https://doi.org/10.3390/jpm14090975
López Rivera JJ, Rueda-Gaitán P, Rios Pinto LC, Rodríguez Gutiérrez DA, Gomez-Lopera N, Lamilla J, Rojas Aguirre FA, Bernal Vaca L, Isaza-Ruget MA. Advancing Cancer Care in Colombia: Results of the First In Situ Implementation of Comprehensive Genomic Profiling. Journal of Personalized Medicine. 2024; 14(9):975. https://doi.org/10.3390/jpm14090975
Chicago/Turabian StyleLópez Rivera, Juan Javier, Paula Rueda-Gaitán, Laura Camila Rios Pinto, Diego Alejandro Rodríguez Gutiérrez, Natalia Gomez-Lopera, Julian Lamilla, Fabio Andrés Rojas Aguirre, Laura Bernal Vaca, and Mario Arturo Isaza-Ruget. 2024. "Advancing Cancer Care in Colombia: Results of the First In Situ Implementation of Comprehensive Genomic Profiling" Journal of Personalized Medicine 14, no. 9: 975. https://doi.org/10.3390/jpm14090975
APA StyleLópez Rivera, J. J., Rueda-Gaitán, P., Rios Pinto, L. C., Rodríguez Gutiérrez, D. A., Gomez-Lopera, N., Lamilla, J., Rojas Aguirre, F. A., Bernal Vaca, L., & Isaza-Ruget, M. A. (2024). Advancing Cancer Care in Colombia: Results of the First In Situ Implementation of Comprehensive Genomic Profiling. Journal of Personalized Medicine, 14(9), 975. https://doi.org/10.3390/jpm14090975