Should Rehabilitation Specialists Use External Focus Instructions When Motor Learning Is Fostered? A Systematic Review

Abstract
:1. Introduction
2. Methods
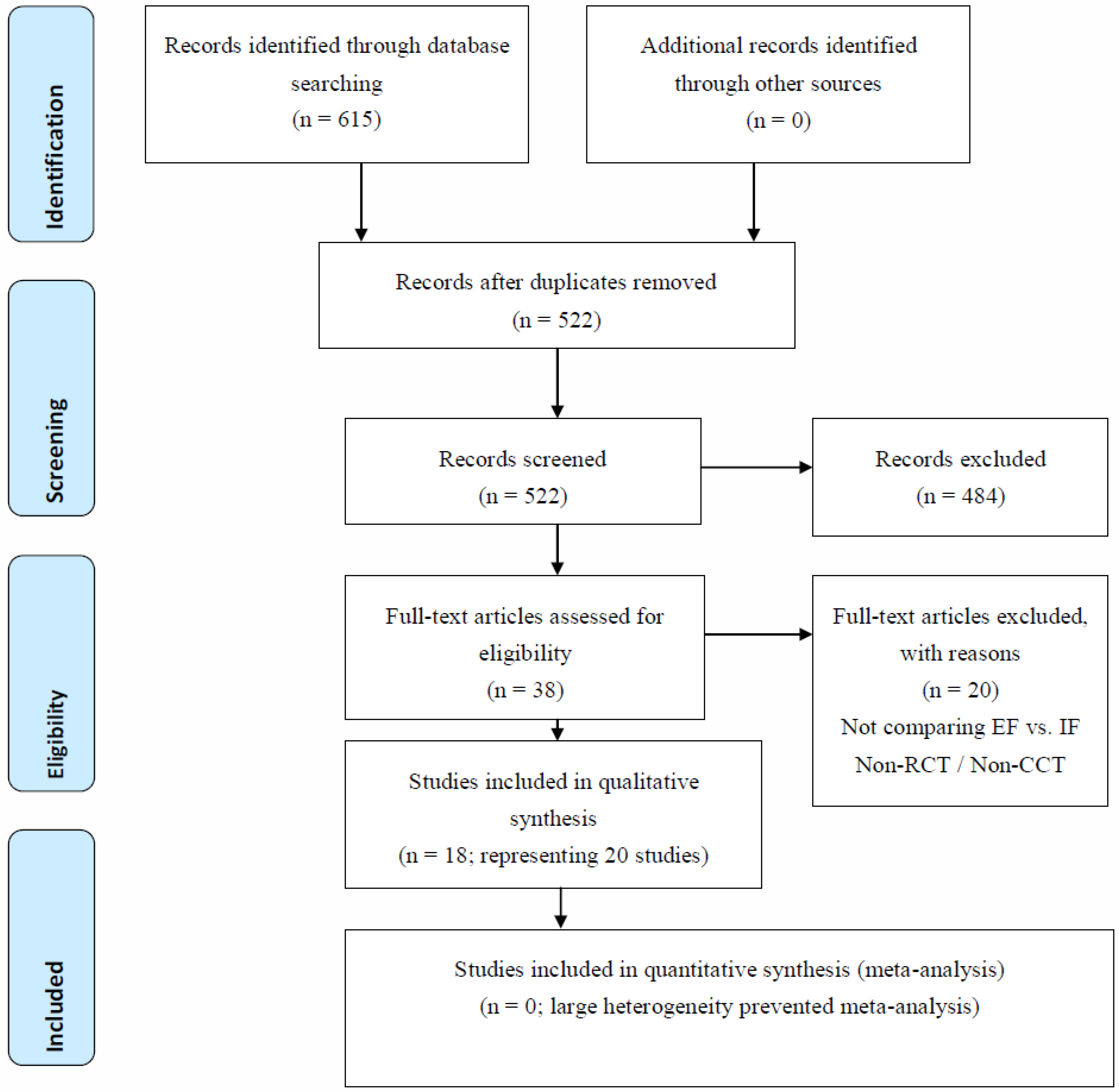
2.1. Data Sources and Searches
2.2. Criteria for Considering Studies for This Review
2.3. Data Collection and Quality Assessment
3. Analysis
4. Results

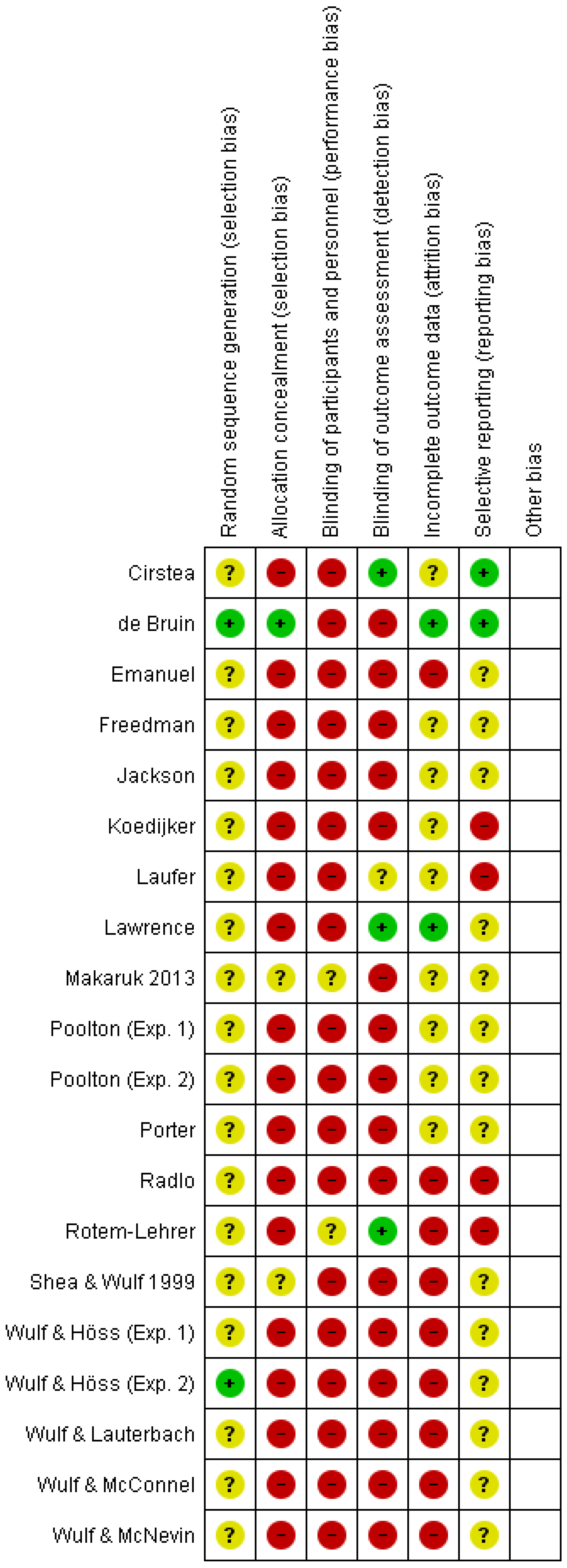
5. Methodological Quality Assessed with the Risk of Bias

6. Summary of the Studies

7. Quantitative Analyses
8. Discussion
9. Conclusion

{kind=link}
{kind=link}
{kind=link}
| Cirstea (2007) [30] | 2 IGs learn pointing movements with the impaired arm | stroke patients: 14 IF/14 EF | knowledge of performance (KP) about arm joint movements | knowledge of results (KR) about movement precision |
| de Bruin (2009) [29] | 2 IGs train dynamic balance | elderly: 26 (>70) | on a moving point on a screen, which represents their point of gravity | on a moving point on a screen, which represents an air bubble in level |
| Emanuel (2008) [32] | 2 IGs learn to throw darts | children: 34 adults: 30 | on the movements of the shoulder, arm and fingers | on the target, the dart and dart's course |
| Freedman (2007) [33] | 2 IGs learn hand and tongue impulse force control | students: 46 | on the pressure they exerted with their hand/tongue | on the pressure on a bulb |
| Jackson (2011) [40] | 4 IGs learn to balance with 2 foci of attention and 2 task objectives | adults: 36 | on feet and are told that either feet position or board position is measured | on balancing board and are told that either feet position or board position is measured |
| Koedijker (2007) [34] | 4 IGs learn implicitly, explicitly, environmental or movement oriented table tennis playing | students: 33 | movement oriented focusses on movement components of wrist, elbow and shoulder | environmentally oriented focusses on movement of the ball |
| Lawrence (2011) [31] | 3 IGs and 1 control learn new gymnastic routine | gymnasts: 40 | on feeling of pressure under feet or on feeling in the face | on the exertion of pressure under the feet |
| Laufer (2007) [26] Rotem-Lehrer (2007) [25] | 2 IGs receive balance training after ankle sprain | patients after ankle sprains: 40 | on balance by stabilizing the body | on balance by stabilizing the platform |
| Makaruk (2012) [35] | 2 IGs and 1 control have 9 weeks plyometric training | students: 36 | on the extension of the lower limbs | on the force on the ground |
| Poolton (2006) [27] first exp. | 2 IGs learn a golf putting task | adults: 30 | on the swing of the hand | on the swing of the putter head |
| Poolton (2006) [27] second exp. | 2 IGs learn golf putting task under increasing number of IF/EF rules | adults: 39 | on the mechanical processes with more and more IF rules | on the effect of the movement with more and more EF rules |
| Porter (2010) [36] | 2 IGs learn a standing long jump | young adults: 120 | on the quickest extension of the knee | as far past the line as possible |
| Radlo (2002) [37] | 2 IGs learn to throw darts | male students: 20 | on the hand and elbow | on center of the board |
| Shea & Wulf (1999) [19] | 2 IGs learn balance on stabilometer | students : 16 | try to keep the feet on the same height | try to keep the markers at the same height |
| Wulf (1998) [28] first exp. | 2 IGs and 1 control on ski-simulator | adults: 33 | on the exertion of force on outer foot | on the exertion of force on outer wheels |
| Wulf (1998) [28] second exp. | 2 IGs learn balance on stabilometer | students: 16 | try to keep the feet on the same height | try to keep the markers at the same height |
| Wulf (1999) [39] | 2 IGs hitting golf balls in a circle | students: 22 | on body movements | on club movement |
| Cirstea (2007) [30] | angular motion; inter-joint coordination trunk recruitment | with KP increase in joint range (p < 0.02); better inter-joint coordination (p <0 .05), but no trunk compensation; retention: KP better than KR (p < 0.05): no 95% CI reported | 10 1 h sessions for 2 weeks; 4 weeks later |
| de Bruin (2009) [29] | weight shifting score; dynamic balance parameters; falls efficacy; Extended Timed-Get-Up-and-Go test; 5 chair rises | all subjects improved, but no significant difference between IF and EF: no 95% confidence interval (CI) reported | 2 weekly sessions for 5 weeks no retention test |
| Emanuel (2008) [32] | accuracy and variability of throws | acquisition: adults improved more on EF than on IF (p < 0.05); children no difference; retention: no effect for age and focus of attention; transfer: EF better than IF for adults; IF better than EF for children; no 95% CI reported | 50 throws on day 1 retention: 20 throws on day 2 transfer: 20 throws on day 2 |
| Freedman (2007) [33] | absolute and variable error of the pressure bursts' peaks of hand and tongue | EF smaller absolute error (p = 0.05) for the hand and tongue; EF smaller variable error for hand and tongue (p < 0.05); no 95% CI reported | 40 contractions for hand and tongue on day 1; no retention |
| Jackson (2011) [40] | root mean square error of platform angle | acquisition: EF and external aim were most efficient (p = 0.015); retention: no interaction between focus of attention and task objective; no 95% CI reported | 6 trials on each day (1, 2) 3 trials on day 3 |
| Koedijker (2007) [34] | ball precision; stress level of subject; number of rules acquired and direction | acquisition: no difference pre- and post-learning for the 4 conditions; number of rules more important than direction of attention; no 95% CI reported | every condition 50 trials all on day 1; no retention test |
| Lawrence (2011) [31] | accurate movement form/ technique | acquisition: no significant differences between groups after two days; retention: no significant differences between groups after one week (or transfer); no 95% CI reported | 40 trials in 2 days training retention: 5 trials 1 week later |
| Laufer (2007) [26] Rotem-Lehrer (2007) [25] | variance in overall stability of platform displacement and anteroposterior and mediolateral displacement | acquisition: no group effect for any of the three stability parameters; retention: no difference between EF and IF; EF improved significantly over time; no 95% CI reported | 20 trials on 3 days (1,2,3); retention: 48 hours after day 3 |
| Makaruk (2012) [35] | standing long jump (SLJ); countermovement jump (CMJ); drop jump (DJ) | SLJ: EF better than IF and C (p < 0.000); CMJ: EF better than IF and C (p < 0.007); DJ: C better than IF (p < 0.05); no differences between EF and IF; no 95% CI reported | first 1-7 weeks 3 × 50 minutes/ week; weeks 8–9: 2 sessions |
| 1. Poolton (2006) [27] | number of successful puts | acquisition: no difference between EF and IF; retention: no difference between EF and IF; transfer (=distraction): EF better than IF (p < 0.05); no 95% CI reported | 300 trials on one day another 2 × 30 for retention |
| 2. Poolton (2006) [27] | number of successful puts | acquisition: no difference between EF and IF; retention: no difference between EF and IF; transfer (=distraction): EF and IF deteriorate (p < 0.01); no 95% CI reported | 300 trials on one day another 2 × 30 for retention |
| Porter (2010) [36] | distance jumped | EF jumped further as IF (p < 0.003); 95% CI: 3.32 - 16.74 | 5 trials on one day; no follow-up |
| Radlo (2002) [37] | magnitude of EEG alpha power; heart rate; correctness of throws | EF produced less alpha power (p < 0.0003), lower heart rate (p < 0.0001), less absolute error (p < 0.05); no 95% CI reported | 40 trials on one day no follow-up |
| Shea & Wulf (1999) [19] | RMSE of balance on stabilometer | first 7 trials: IF better than EF; second 7 trials: no difference between IF and EF; retention: EF better than IF (p < 0.05); no 95% CI reported | 7 trials on 2 following days day 3: 7 trials |
| 1. Wulf (1998) [28] | movement amplitude and frequency | movement amplitude: EF better than IF and control (p < 0.05); movement frequency: no difference (p > 0.05); retention: movement amplitude: EF better than IF and control (p < 0.05): movement frequency: no group differences; | 8 trials on each day (1,2) 6 trials on day 3 |
| 2. Wulf (1998) [28] | RMSE of balance on stabilometer | acquisition: no difference between IF and EF; retention: EF better than IF (p < 0.01); no 95% CI reported | 7 trials on 2 following days day 3: 7 trials |
| Wulf (1999) [39] | measure of success on five point scale | acquisition: EF better than IF ((p < 0.001); retention: EF better than IF (p < 0.018); no 95% CI reported | 80 trials on day 1 30 trials on day 2 |
| 2. Wulf (2002) [38] | movement accuracy on 4-point scale | acquisition: EF better than IF (p < 0.05); no main effect for frequency of feedback; retention: EF better IF (p < 0.01); no main effect for frequency of feedback; no 95% CI reported | 30 trials on day 1 10 trials one week later |
Acknowledgements
References
- Schmidt, R.A.; Lee, T.D. Motor Control and Learning, 3rd edHuman Kinetics: Champaign, IL, USA, 1999. [Google Scholar]
- Winstein, C.J. Knowledge of results and motor learning––implications for physical therapy. Phys. Ther. 1991, 71, 140–149. [Google Scholar]
- Fuhrer, M.J.; Keith, R.A. Facilitating patient learning during medical rehabilitation: a research agenda. Am. J. Phys. Med. Rehabil. 1998, 77, 557–561. [Google Scholar] [CrossRef]
- McNevin, N.H.; Wulf, G.; Carlson, C. Effects of attentional focus, self–control, and dyad training on motor learning: implications for physical rehabilitation. Phys. Ther. 2000, 80, 373–385. [Google Scholar]
- McNevin, N.H.; Wulf, G. Attentional focus on supra–postural tasks affects postural control. Hum. Mov. Sci. 2002, 21, 187–202. [Google Scholar] [CrossRef]
- Wulf, G.; Weigelt, M.; Poulter, D.; McNevin, N. Attentional focus on suprapostural tasks affects balance learning. Q. J. Exp. Psychol. A 2003, 56, 1191–1211. [Google Scholar]
- Willingham, D.B. A neuropsychological theory of motor skill learning. Psychol. Rev. 1998, 105, 558–584. [Google Scholar] [CrossRef]
- James, W. The principles of psychology, Henry Holt and Company: New York, NY, USA, 1890.
- Dayan, E.; Cohen, L.G. Neuroplasticity subserving motor skill learning. Neuron. 2011, 72, 443–454. [Google Scholar] [CrossRef]
- Floyer–Lea, A.; Matthews, P.M. Distinguishable brain activation networks for short– and long–term motor skill learning. J. Neurophysiol. 2005, 94, 512–518. [Google Scholar] [CrossRef]
- Halsband, U.; Lange, R.K. Motor learning in man: a review of functional and clinical studies. J. Physiol. Paris 2006, 99, 414–424. [Google Scholar] [CrossRef]
- Luft, A.R.; Buitrago, M.M. Stages of motor skill learning. Mol. Neurobiol. 2005, 32, 205–216. [Google Scholar] [CrossRef]
- Nielsen, J.B.; Cohen, L.G. The Olympic brain. Does corticospinal plasticity play a role in acquisition of skills required for high–performance sports? J. Physiol. 2008, 586, 65–70. [Google Scholar] [CrossRef]
- Schollhorn, W.I.; Beckmann, H.; Davids, K. Exploiting system fluctuations. Differential training in physical prevention and rehabilitation programs for health and exercise. Medicina (Kaunas) 2010, 46, 365–373. [Google Scholar]
- Wulf, G.; McNevin, N.; Shea, C.H. The automaticity of complex motor skill learning as a function of attentional focus. Q. J. Exp. Psychol. A 2001, 54, 1143–1154. [Google Scholar]
- Johnston, M.V.; Vanderheiden, G.D.; Farkas, M.D.; Rogers, E.S.; Summers, J.A.; Westbrook, J. The challenge of evidence in disability and rehabilitation research and practice: A position paper. SEDL: Austin, TX, USA, 2009. [Google Scholar]
- Peh, S.Y.; Chow, J.Y.; Davids, K. Focus of attention and its impact on movement behaviour. J. Sci. Med. Sport 2011, 14, 70–78. [Google Scholar] [CrossRef]
- Wulf, G.; Shea, C.; Lewthwaite, R. Motor skill learning and performance: a review of influential factors. Med. Educ. 2010, 44, 75–84. [Google Scholar] [CrossRef]
- Shea, C.H.; Wulf, G. Enhancing motor learning through external–focus instructions and feedback. Hum. Mov. Sci. 1999, 18, 553–571. [Google Scholar] [CrossRef]
- Wulf, G. Attentional focus and motor learning: a review of 15 years. Int. Rev. Sport. Exerc. Psychol. 2013, 6, 77–104. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Götsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta–analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Sibbald, B.; Roland, M. Understanding controlled trials. Why are randomised controlled trials important? BMJ 1998, 316, 201. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Götsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Auais, M.A.; Eilayyan, O.; Mayo, N.E. Extended exercise rehabilitation after hip fracture improves patients' physical function: a systematic review and meta–analysis. Phys. Ther. 2012, 92, 1437–1551. [Google Scholar] [CrossRef]
- Rotem–Lehrer, N.; Laufer, Y. Effect of focus of attention on transfer of a postural control task following an ankle sprain. J. Orthop. Sports Phys. Ther. 2007, 37, 564–569. [Google Scholar]
- Laufer, Y.; Rotem–Lehrer, N.; Ronen, Z.; Khayutin, G.; Rozenberg, I. Effect of attention focus on acquisition and retention of postural control following ankle sprain. Arch. Phys. Med. Rehabil. 2007, 88, 105–108. [Google Scholar] [CrossRef]
- Poolton, J.M.; Maxwell, J.P.; Masters, R.S.; Raab, M. Benefits of an external focus of attention: Common coding or conscious processing? J. Sports Sci. 2006, 24, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Wulf, G.; Hoss, M.; Prinz, W. Instructions for motor learning: Differential effects of internal versus external focus of attention. J. Mot. Behav. 1998, 30, 169–179. [Google Scholar] [CrossRef]
- de Bruin, E.D.; Swanenburg, J.; Betschon, E.; Murer, K. A randomised controlled trial investigating motor skill training as a function of attentional focus in old age. BMC Geriatr. 2009, 9, 15. [Google Scholar] [CrossRef] [Green Version]
- Cirstea, M.C.; Levin, M.F. Improvement of arm movement patterns and endpoint control depends on type of feedback during practice in stroke survivors. Neurorehabil. Neural. Repair. 2007, 21, 398–411. [Google Scholar] [CrossRef]
- Lawrence, G.R.; Gottwald, V.M.; Hardy, J.; Khan, M.A. Internal and External Focus of Attention in a Novice Form Sport. Res. Q. Exerc. Sport. 2011, 82, 431–441. [Google Scholar] [CrossRef]
- Emanuel, M.; Jarus, T.; Bart, O. Effect of focus of attention and age on motor acquisition, retention, and transfer: a randomized trial. Phys. Ther. 2008, 88, 251–260. [Google Scholar] [CrossRef]
- Freedman, S.E.; Maas, E.; Caligiuri, M.P.; Wulf, G.; Robin, D.A. Internal versus external: oral–motor performance as a function of attentional focus. J. Speech. Lang. Hear. Res. 2007, 50, 131–136. [Google Scholar] [CrossRef]
- Koedijker, J.M.; Oudejans, R.R.D.; Beek, P.J. Explicit rules and direction of attention in learning and performing the table tennis forehand. Int. J. Sport Psychol. 2007, 38, 227–244. [Google Scholar]
- Makaruk, H.; Porter, J.M.; Czaplicki, A.; Sadowski, J.; Sacewicz, T. The role of attentional focus in plyometric training. J. Sports Med. Phys. Fitness 2012, 52, 319–327. [Google Scholar]
- Porter, J.M.; Ostrowski, E.J.; Nolan, R.P.; Wu, W.F. Standing Long–Jump Performance Is Enhanced When Using an External Focus of Attention. J. Strength. Cond. Res. 2010, 24, 1746–1750. [Google Scholar] [CrossRef]
- Radlo, S.J.; Steinberg, G.; Singer, R.N.; Barba, D.A.; Melnikov, A. The influence of an attentional focus strategy on alpha brain wave activity, heart rate, and dart–throwing performance. Int. J. Sport Psychol. 2002, 33, 205–217. [Google Scholar]
- Wulf, G.; McConnel, N.; Gärtner, M.; Schwarz, A. Enhancing the learning of sport skills through external–focus feedback. J. Mot. Behav. 2002, 34, 171–182. [Google Scholar] [CrossRef]
- Wulf, G.; Lauterbach, B.; Toole, T. The learning advantages of an external focus of attention in golf. Res. Q. Exerc. Sport 1999, 70, 120–126. [Google Scholar] [CrossRef]
- Jackson, B.H.; Holmes, A.M. The Effects of Focus of Attention and Task Objective Consistency on Learning a Balancing Task. Res. Q. Exerc. Sport 2011, 82, 574–579. [Google Scholar] [CrossRef]
- Hikosaka, O.; Nakamura, K.; Sakai, K.; Nakahara, H. Central mechanisms of motor skill learning. Curr. Opin. Neurobiol. 2002, 12, 217–222. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta–analysis in clinical trials. Control. Clin. Trials. 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Bhardwaj, S.S.; Camacho, F.; Derrow, A.; Fleischer, A.B., Jr.; Feldman, S.R. Statistical significance and clinical relevance: the importance of power in clinical trials in dermatology. Arch. Dermatol. 2004, 140, 1520–1523. [Google Scholar] [CrossRef]
- Savović, J.; Jones, H.E.; Altman, D.G.; Harris, R.J.; Jüni, P.; Pildal, J.; Als–Nielsen, B.; Balk, E.M.; Gluud, C.; Gluud, L.L.; Ioannidis, J.P.; Schulz, K.F.; Beynon, R.; Welton, N.J.; Wood, L.; Moher, D.; Deeks, J.J.; Sterne, J.A. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Ann. Intern. Med. 2012, 157, 429–438. [Google Scholar]
- Herbison, P.; Hay–Smith, J.; Gillespie, W.J. Different methods of allocation to groups in randomized trials are associated with different levels of bias. A meta–epidemiological study. J. Clin. Epidemiol. 2011, 64, 1070–1075. [Google Scholar] [CrossRef]
- Kunz, R.; Vist, G.; Oxman, A.D. Randomisation to protect against selection bias in healthcare trials. Cochrane Database Syst. Rev. 2007, 2, MR000012. [Google Scholar]
- Pildal, J.; Hróbjartsson, A.; Jørgensen, K.J.; Hilden, J.; Altman, D.G.; Gøtzsche, P.C. Impact of allocation concealment on conclusions drawn from meta–analyses of randomized trials. Int. J. Epidemiol. 2007, 36, 847–857. [Google Scholar] [CrossRef]
- Ioannidis, J.P. Effectiveness of antidepressants: an evidence myth constructed from a thousand randomized trials? Philos. Ethics Humanit. Med. 2008, 3, 14. [Google Scholar] [CrossRef]
- Ioannidis, J.P. Why most published research findings are false. PLoS Med. 2005, 2, e124. [Google Scholar] [CrossRef] [Green Version]
- Kottke, F.J. From reflex to skill: the training of coordination. Arch. Phys. Med. Rehabil. 1980, 61, 551–561. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta–analyses: the PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kakebeeke, T.H.; Knols, R.H.; De Bruin, E.D. Should Rehabilitation Specialists Use External Focus Instructions When Motor Learning Is Fostered? A Systematic Review. Sports 2013, 1, 37-54. https://doi.org/10.3390/sports1020037
Kakebeeke TH, Knols RH, De Bruin ED. Should Rehabilitation Specialists Use External Focus Instructions When Motor Learning Is Fostered? A Systematic Review. Sports. 2013; 1(2):37-54. https://doi.org/10.3390/sports1020037
Chicago/Turabian StyleKakebeeke, Tanja H., Ruud H. Knols, and Eling D. De Bruin. 2013. "Should Rehabilitation Specialists Use External Focus Instructions When Motor Learning Is Fostered? A Systematic Review" Sports 1, no. 2: 37-54. https://doi.org/10.3390/sports1020037
APA StyleKakebeeke, T. H., Knols, R. H., & De Bruin, E. D. (2013). Should Rehabilitation Specialists Use External Focus Instructions When Motor Learning Is Fostered? A Systematic Review. Sports, 1(2), 37-54. https://doi.org/10.3390/sports1020037