
The Assessment of Ankle Range-of-Motion and Its Relationship with Overall Muscle Strength in a Cross-Section of Soccer Players

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
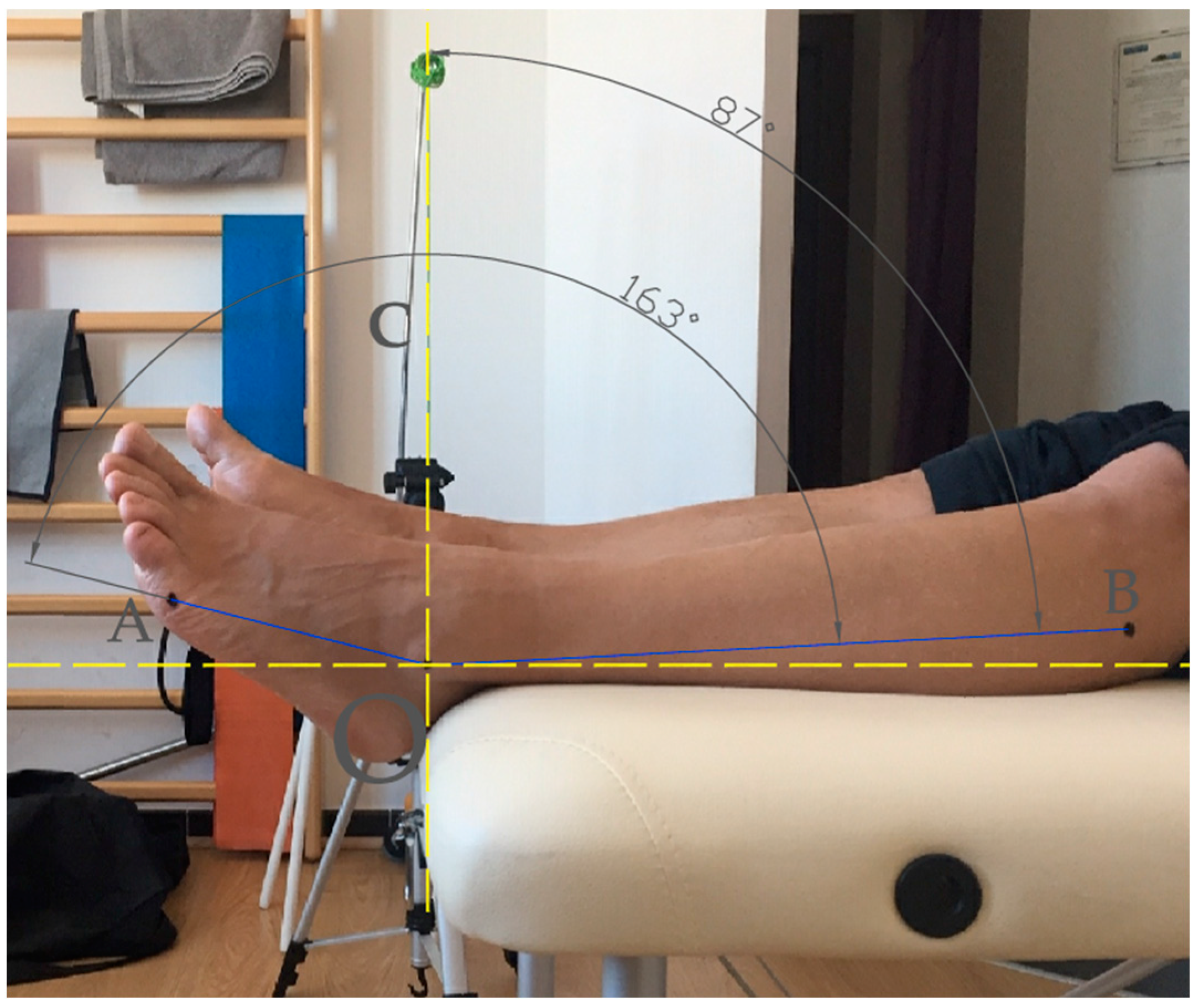
2.1. Determination of Joint Range of Motion
2.2. Determination of Hand Grip Strength
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| Adult APF | Players of Under 17 Teams |
| Adult BSP | Adult players non-Under 17 Teams |
| APF | Ankle Plantar Flexion |
| ADF | Ankle Dorsiflexion |
| ATOT | Total Ankle Joint Mobility |
| BMI | Body Mass Index |
| SP | Soccer Players |
| HGS | Hand Strength |
| R-L | Right-Left |
| ROM | Range of Motion |
| rs | Spearman’s rho |
References
- FIFA Communications Division. FIFA Big Count 2006; Statistical Summary Report. 2007. Available online: https://digitalhub.fifa.com/m/55621f9fdc8ea7b4/original/mzid0qmguixkcmruvema-pdf.pdf (accessed on 10 October 2022).
- Study Center FIGC. Report Calcio 2017. 2017. Available online: https://www.pwc.com/it/it/publications/assets/docs/reportcalcio-2017.pdf (accessed on 10 October 2022).
- Merkel, D.L. Youth sport: Positive and negative impact on young athletes. Open Access. J. Sport. Med. 2013, 4, 151–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krustrup, P.; Krustrup, B.R. Football is medicine: It is time for patients to play! Br. J. Sport. Med. 2018, 52, 1412–1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergeron, M.F.; Mountjoy, M.; Armstrong, N.; Chia, M.; Côté, J.; Emery, C.A.; Faigenbaum, A.; Hall, G., Jr.; Kriemler, S.; Léglise, M.; et al. International Olympic Committee consensus statement on youth athletic development. Br. J. Sport. Med. 2015, 49, 843–851. [Google Scholar] [CrossRef] [Green Version]
- Armenis, E.; Pefanis, N.; Tsiganos, G.; Karagounis, P.; Baltopoulos, P. Osteoarthritis of the ankle and foot complex in former Greek soccer players. Foot Ankle Spec. 2011, 4, 338–343. [Google Scholar] [CrossRef]
- Golanó, P.; Dalmau-Pastor, M.; Vega, J.; Batista, J.P. Anatomy of the Ankle. In The Ankle in Football. Sports and Traumatology; d’Hooghe, P., Kerkhoffs, G., Eds.; Springer: Paris, France, 2014; pp. 1–24. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.; Myer, G.D.; Lloyd, R.S. Neuromuscular Risk Factors for Knee and Ankle Ligament Injuries in Male Youth Soccer Players. Sports Med. 2016, 46, 1059–1066. [Google Scholar] [CrossRef] [Green Version]
- Travers, P.R.; Evans, G.P. Annotation limitation of mobility in major joints of 231 sportsmen. Br. J. Sport. Med. 1976, 10, 35–36. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, J.; Gillquist, J. The frequency of muscle tightness and injuries in soccer players. Am. J. Sport. Med. 1982, 10, 75–78. [Google Scholar] [CrossRef]
- Rein, S.; Fabian, T.; Weindel, S.; Schneiders, W.; Zwipp, H. The influence of playing level on functional ankle stability in soccer players. Arch. Orthop. Trauma Surg. 2011, 131, 1043–1052. [Google Scholar] [CrossRef] [PubMed]
- Francia, P.; Ferri Marini, C.; Toni, S.; Mencarelli, A.; Iannone, G.; Lucertini, F.; Brandoni, G.; Monteiro-Soares, M.; Federici, A.; Piccini, B. The effect of an adapted training protocol on ankle joint mobility of young soccer players. Med. Sport. 2020, 73, 271–281. [Google Scholar] [CrossRef]
- de Noronha, M.; Refshauge, K.M.; Herbert, R.D.; Kilbreath, S.L.; Hertel, J. Do voluntary strength, proprioception, range of motion, or postural sway predict occurrence of lateral ankle sprain? Br. J. Sport. Med. 2006, 40, 824–828. [Google Scholar] [CrossRef] [Green Version]
- Terada, M.; Pietrosimone, B.G.; Gribble, P.A. Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: A systematic review. J. Athl. Train. 2013, 48, 696–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaumeyer, G.; Malone, T.R. Ankle injuries: Anatomical and biomechanical considerations necessary for the development of an injury prevention program. J. Orthop. Sports Phys. Ther. 1980, 1, 171–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason-Mackay, A.R.; Whatman, C.; Reid, D. The effect of reduced ankle dorsiflexion on lower extremity mechanics during landing: A systematic review. J. Sci. Med. Sport 2017, 20, 451–458. [Google Scholar] [CrossRef]
- Kaufman, K.R.; Brodine, S.K.; Shaffer, R.A.; Johnson, C.W.; Cullison, T.R. The effect of foot structure and range of motion on musculoskeletal overuse injuries. Am. J. Sports Med. 1999, 27, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Sahillioglu, A.; Cerrahoglu, L. The relationship of the foot and ankle structure with overuse injuries in licensed footballers: A prospective cohort study. J. Sports Med. Phys. Fit. 2021, 61, 1499–1508. [Google Scholar] [CrossRef]
- Mahieu, N.N.; Witvrouw, E.; Stevens, V.; Van Tiggelen, D.; Roget, P. Intrinsic risk factors for the development of achilles tendon overuse injury: A prospective study. Am. J. Sports Med. 2006, 34, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Brockett, C.L.; Chapman, G.J. Biomechanics of the ankle. Orthop. Trauma 2016, 30, 232–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, J.Y.; Lee, H.M.; Luo, H.J.; Leu, C.C.; Cheng, P.G.; Wu, S.K. Gastrocnemius tightness on joint angle and work of lower extremity during gait. Clin. Biomech. 2009, 24, 744–750. [Google Scholar] [CrossRef]
- Drewes, L.K.; McKeon, P.O.; Kerrigan, D.C.; Hertel, J. Dorsiflexion deficit during jogging with chronic ankle instability. J. Sci. Med. Sport 2009, 12, 685–687. [Google Scholar] [CrossRef]
- Aronow, M.S.; Diaz-Doran, V.; Sullivan, R.J.; Adams, D.J. The effect of triceps surae contracture force on plantar foot pressure distribution. Foot Ankle Int. 2006, 27, 43–52. [Google Scholar] [CrossRef]
- Basnett, C.R.; Hanish, M.J.; Wheeler, T.J.; Miriovsky, D.J.; Danielson, E.L.; Barr, J.B.; Grindstaff, T.L. Ankle dorsiflexion range of motion influences dynamic balance in individuals with chronic ankle instability. Int. J. Sports Phys. Ther. 2013, 8, 121–128. [Google Scholar] [PubMed]
- Trajković, N.; Kozinc, Ž.; Smajla, D.; Šarabon, N. Relationship between ankle strength and range of motion and postural stability during single-leg quiet stance in trained athletes. Sci. Rep. 2021, 11, 11749. [Google Scholar] [CrossRef]
- Francia, P.; Ferri Marini, C.; Toni, S.; Lucertini, F.; Federici, A.; Iannone, G.; Paternostro, F.; Piccini, B. Lower limb posture and joint mobility in young Soccer players. Italian J. Anat. Embryol. 2022, 125, 83–94. [Google Scholar] [CrossRef]
- Ribeiro, C.Z.P.; Akashi, P.M.H.; Sacco, I.D.C.N.; Pedrinelli, A. Relationship between postural changes and injuries of the locomotor system in indoor soccer athletes. Rev. Bras. Med. Esporte 2003, 9, 98–103. [Google Scholar] [CrossRef]
- Hoch, M.C.; Staton, G.S.; Medina McKeon, J.M.; Mattacola, C.G.; McKeon, P.O. Dorsiflexion and dynamic postural control deficits are present in those with chronic ankle instability. J. Sci. Med. Sport 2012, 15, 574–579. [Google Scholar] [CrossRef]
- Xue, X.; Ma, T.; Li, Q.; Song, Y.; Hua, Y. Chronic ankle instability is associated with proprioception deficits: A systematic review and meta-analysis. J. Sport Health Sci. 2021, 10, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Azuma, N.; Someya, F. Injury prevention effects of stretching exercise intervention by physical therapists in male high school soccer players. Scand. J. Med. Sci. Sports 2020, 30, 2178–2192. [Google Scholar] [CrossRef] [PubMed]
- Paterno, M.V.; Taylor-Haas, J.A.; Myer, G.D.; Hewett, T.E. Prevention of overuse sports injuries in the young athlete. Orthop. Clin. N. Am. 2013, 44, 553–564. [Google Scholar] [CrossRef] [Green Version]
- Hattori, K.; Ohta, S. Ankle joint flexibility in college soccer players. J. Hum. Ergol. 1986, 15, 85–89. [Google Scholar]
- Walls, R.J.; Ross, K.A.; Fraser, E.J.; Hodgkins, C.W.; Smyth, N.A.; Egan, C.J.; Calder, J.; Kennedy, J.G. Football injuries of the ankle: A review of injury mechanisms, diagnosis and management. World J. Orthop. 2016, 7, 8–19. [Google Scholar] [CrossRef]
- Kim, S.G.; Kim, W.S. Effect of Ankle Range of Motion (ROM) and Lower-Extremity Muscle Strength on Static Balance Control Ability in Young Adults: A Regression Analysis. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2018, 24, 3168–3175. [Google Scholar] [CrossRef] [PubMed]
- Beynnon, B.D.; Murphy, D.F.; Alosa, D.M. Predictive Factors for Lateral Ankle Sprains: A Literature Review. J. Athl. Train. 2002, 37, 376–380. [Google Scholar]
- Lees, A.; Asai, T.; Andersen, T.B.; Nunome, H.; Sterzing, T. The biomechanics of kicking in soccer: A review. J. Sports Sci. 2010, 28, 805–817. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, Y.; Takahashi, M.; Shinkoda, K. Differences of muscle co-contraction of the ankle joint between young and elderly adults during dynamic postural control at different speeds. J. Physiol. Anthropol. 2017, 36, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellis, E.; Katis, A. Biomechanical characteristics and determinants of instep soccer kick. J. Sports Sci. Med. 2007, 6, 154–165. [Google Scholar]
- Ghouchani, A.; Tabatabai, F.; Nejad, S.K.A.; Rahimnejad, M. Analysis of Torques and Forces Applied on Limbs and Joints of Lower Extremities in Free Kick in Football. Procedia Eng. 2010, 2, 3269–3274. [Google Scholar] [CrossRef] [Green Version]
- Youdas, J.W.; McLean, T.J.; Krause, D.A.; Hollman, J.H. Changes in active ankle dorsiflexion range of motion after acute inversion ankle sprain. J. Sport Rehabil. 2009, 18, 358–374. [Google Scholar] [CrossRef] [Green Version]
- Corso, M. Developmental changes in the youth athlete: Implications for movement, skills acquisition, performance and injuries. J. Can. Chiropr. Assoc. 2018, 62, 150–160. [Google Scholar]
- Houghton, K.M. Review for the generalist: Evaluation of pediatric foot and ankle pain. Pediatr. Rheumatol. Online J. 2008, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Robles-Palazón, F.J.; Ayala, F.; Cejudo, A.; De Ste Croix, M.; Sainz de Baranda, P.; Santonja, F. Effects of Age and Maturation on Lower Extremity Range of Motion in Male Youth Soccer Players. J. Strength Cond. Res. 2022, 36, 1417–1425. [Google Scholar] [CrossRef]
- Hogrel, J.Y. Grip strength measured by high precision dynamometry in healthy subjects from 5 to 80 years. BMC Musculoskelet. Disord. 2015, 16, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ploegmakers, J.J.W.; Hepping, A.M.; Geertzen, J.H.B.; Bulstra, S.K.; Stevens, M. Strength Is Strongly Associated With Height, Weight and Gender in Childhood: A Cross Sectional Study of 2241 Children and Adolescents Providing Reference Values. J. Physiother. 2013, 5, 255–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molenaar, H.M.; Selles, R.W.; Zuidam, J.M.; Willemsen, S.P.; Stam, H.J.; Hovius, S.E. Growth diagrams for grip strength in children. Clin. Orthop. Relat. Res. 2010, 468, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Strandkvist, V.; Larsson, A.; Pauelsen, M.; Nyberg, L.; Vikman, I.; Lindberg, A.; Gustafsson, T.; Röijezon, U. Hand grip strength is strongly associated with lower limb strength but only weakly with postural control in community-dwelling older adults. Arch. Gerontol. Geriatr. 2021, 94, 104345. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Santos, R.; Amaral, T.F. Differences in handgrip strength protocols to identify sarcopenia and frailty—A systematic review. BMC Geriatr. 2017, 17, 238. [Google Scholar] [CrossRef] [Green Version]
- Benfica, P.; Aguiar, L.T.; Brito, S.; Bernardino, L.; Teixeira-Salmela, L.F.; Faria, C. Reference values for muscle strength: A systematic review with a descriptive meta-analysis. Braz. J. Phys. Ther. 2018, 22, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Francia, P.; Toni, S.; Iannone, G.; Seghieri, G.; Piccini, B.; Vittori, A.; Santosuosso, U.; Casalini, E.; Gulisano, M. Type 1 diabetes, sport practiced, and ankle joint mobility in young patients: What is the relationship? Pediatr. Diabetes 2018, 19, 801–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francia, P.; Bocchi, L.; Santosuosso, U.; Iannone, G.; Vittori, A.; Toni, S. The effect of different sports specialization on ankle joint mobility of young players. J. Hum. Sport Exerc. 2021, 16, 63–73. [Google Scholar] [CrossRef]
- Clarkson, H.M. Musculoskeletal Assessment: Joint Motion and Muscle Testing, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; pp. 350–352. [Google Scholar]
- Francia, P.; Sorelli, M.; Piccini, B.; Iannone, G.; Capirchio, L.; Toni, S.; Gulisano, M.; Bocchi, L. Glycemic Control Maintained over Time and Joint Stiffness in Young Type 1 Patients: What Is the Mathematical Relationship? J. Diabetes Sci. Technol. 2019, 13, 728–733. [Google Scholar] [CrossRef]
- DeLang, M.D.; Kondratek, M.; DiPace, L.J.; Hew-Butler, T. Collegiate male soccer players exhibit between-limb symmetry in body composition muscle strength and range of motion. Int. J. Sports Phys. Ther. 2017, 12, 1087–1094. [Google Scholar] [CrossRef] [Green Version]
- De, S.; Sengupta, P.; Maity, P.; Pal, A.; Dhara, P.C. Effect of body posture on hand grip strength in adult Bengalee population. J. Exerc. Sci. Physiother. 2011, 7, 79–88. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Weber, K.; Volland, G.; Kashman, N. Reliability and validity of grip and pinch strength evaluations. Surg. Am. 1984, 9, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Madaleno, F.O.; Verhagen, E.; Ferreira, T.V.; Ribeiro, T.; Ocarino, J.M.; Resende, R.A. Normative reference values for handgrip strength, shoulder and ankle range of motion and upper-limb and lower limb stability for 137 youth judokas of both sexes. J. Sci. Med. Sport 2021, 24, 41–45. [Google Scholar] [CrossRef] [PubMed]
- McQuiddy, V.A.; Scheerer, C.R.; Lavalley, R.; McGrath, T.; Lin, L. Normative Values for Grip and Pinch Strength for 6- to 19-Year-Olds. Arch. Phys. Med. Rehabil. 2015, 96, 1627–1633. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge Academic: New York, NY, USA, 1988. [Google Scholar] [CrossRef]
- Boone, D.C.; Azen, S.P. Normal range of motion of joints in male subjects. J. Bone Joint Surg. Am. 1979, 61, 756–759. [Google Scholar] [CrossRef]
- Russell, J.A.; McEwan, I.M.; Koutedakis, Y.; Wyon, M.A. Clinical anatomy and biomechanics of the ankle in dance. J. Dance Med. Sci. 2008, 12, 75–82. [Google Scholar]
- Kumar, S.; Sharma, R.; Gulati, D.; Dhammi, I.K.; Aggarwal, A.N. Normal range of motion of hip and ankle in Indian population. Acta Orthop. Traumatol. Turc. 2011, 45, 421–424. [Google Scholar] [CrossRef]
- Zakas, A. The effect of stretching duration on the lower-extremity flexibility of adolescent soccer players. J. Bodyw. Mov. Ther. 2005, 9, 220–225. [Google Scholar] [CrossRef]
- Brown, K.A.; Patel, D.R.; Darmawan, D. Participation in Sports in Relation to Adolescent Growth and Development. Transl. Pediatr. 2017, 6, 150–159. [Google Scholar] [CrossRef] [Green Version]
- Korff, T.; Horne, S.L.; Cullen, S.J.; Blazevich, A.J. Development of lower limb stiffness and its contribution to maximum vertical jumping power during adolescence. J. Exp. Biol. 2009, 212, 3737–3742. [Google Scholar] [CrossRef] [Green Version]
- Hansen, L.; Bangsbo, J.; Twisk, J.; Klausen, K. Development of muscle strength in relation to training level and testosterone in young male soccer players. J. Appl. Physiol. 1999, 87, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Limony, Y.; Kozieł, S.; Friger, M. Age of onset of a normally timed pubertal growth spurt affects the final height of children. Pediatr. Res. 2015, 78, 351–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soliman, A.; De Sanctis, V.; Elalaily, R.; Bedair, S. Advances in pubertal growth and factors influencing it: Can we increase pubertal growth? Indian J. Endocrinol. Metab. 2014, 18, S53–S62. [Google Scholar] [CrossRef]
- Blazevich, A.; Waugh, C.; Korff, T. Development of musculoskeletal stiffness. In Paediatric Biomechanics and Motor Control Theory and Application; De Ste Croix, M., Korff, T., Eds.; Routledge: Abingdon/Oxon, UK, 2013. [Google Scholar]
- Croix, M. Advances in paediatric strength assessment: Changing our perspective on strength development. J. Sports Sci. Med. 2007, 6, 292–304. [Google Scholar] [PubMed]
- Vänttinen, T.; Blomqvist, M.; Nyman, K.; Häkkinen, K. Changes in body composition, hormonal status, and physical fitness in 11-, 13-, and 15-year-old Finnish regional youth soccer players during a two-year follow-up. J. Strength Cond. Res. 2011, 25, 3342–3351. [Google Scholar] [CrossRef]
- Viru, A.; Loko, J.; Volver, A.; Laaneots, L.; Karelson, K.; Viru, M. Age periods of accelerated improvement of muscle strength, power, speed and endurance in the age interval 6–18 years. Biol. Sport 1998, 15, 211–227. [Google Scholar]
- Cejudo, A.; Robles-Palazón, F.J.; Ayala, F.; De Ste Croix, M.; Ortega-Toro, E.; Santonja-Medina, F.; Sainz de Baranda, P. Age-related differences in flexibility in soccer players 8–19 years old. PeerJ 2019, 7, e6236. [Google Scholar] [CrossRef]
- Wind, A.E.; Takken, T.; Helders, P.J.M.; Engelbert, R.H.H. Is grip strength a predictor for total muscle strength in healthy children, adolescents, and young adults? Eur. J. Pediatr. 2010, 169, 281–287. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| All SP (n = 204) | All Controls (n = 87) | p Value | Cohen’s d | |
|---|---|---|---|---|
| Age (years) | 15.5 ± 7.5 | 15.9 ± 9.9 | 0.962 * | −0.06 |
| BMI (kg/m2) | 19.9 ± 2.9 | 20.1 ± 3.7 | 0.427 * | −0.16 |
| HGS (kg) | 27.8 ± 12.9 | 27.9 ± 11.4 | 0.182 * | −0.10 |
| APF (degrees) | 26.3 ± 7.2 | 32.6 ± 7.4 | <0.001 | −0.90 |
| ADF (degrees) | 95.5 ± 15.6 | 105.5 ± 15.8 | <0.001 * | −0.66 |
| ATOT (degrees) | 121.8 ± 18.0 | 138.1 ± 19.2 | <0.001 * | −0.92 |
| ∆ R-L (degrees) | 5.3 ± 4.6 | 5.6 ± 5.0 | 0.655 * | −0.08 |
| Adult SP (n = 61) | Adult Controls (n = 23) | p Value | Cohen’s d | Young SP (n = 143) | Young Controls (n = 64) | p Value | Cohen’s d | |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 25.2 ± 6.9 | 28.0 ± 8.7 | 0.204 * | −0.39 | 11.3 ± 1.9 | 11.6 ± 1.8 | 0.594 * | 0.17 |
| BMI (kg/m2) | 22.5 ± 2.1 | 23.4 ± 2.3 | 0.108 | −0.41 | 18.6 ± 2.4 | 19.3 ± 3.6 | 0.380 * | 0.26 |
| HGS (kg) | 44.2 ± 7.5 | 47.5 ± 8.8 | 0.125 | −0.43 | 20.7 ± 6.7 | 23.8 ± 7.3 | 0.005 * | 0.46 |
| APF (degrees) | 26.0 ± 5.7 | 33.5 ± 7.0 | <0.001 | −1.23 | 26.4 ± 7.8 | 32.5 ± 7.7 | <0.001 | 0.79 |
| ADF (degrees) | 89.0 ± 10.5 ^ | 104.2 ± 13.1 | <0.001 | −1.36 | 98.3 ± 16.6 ^ | 106.4 ± 16.5 | 0.003 * | 0.49 |
| ATOT (degrees) | 115.0 ± 12.9 ^ | 137.8 ± 13.9 | <0.001 * | −1.73 | 124.7 ± 19.1 ^ | 138.9 ± 20.5 | <0.001 * | 0.73 |
| ∆ R-L (degrees) | 4.4 ± 3.5 | 5.4 ± 5.2 | 0.252 * | −0.41 | 5.7 ± 4.9 | 5.6 ± 5.0 | 0.789 * | −0.03 |
| Adult APF (n = 19) (Under 17 Teams) | Adult BSP (n = 42) (Non-Under 17 Teams) | p-Value | Cohen’s d | |
|---|---|---|---|---|
| Age (years) | 16.6 ± 0.4 | 29.0 ± 4.5 | - | |
| BMI (kg/m2) | 21.2 ± 1.5 | 23.1 ± 2.0 | <0.001 | −0.99 |
| HGS (kg) | 42.9 ± 5.9 | 44.7 ± 8.1 | 0.381 | −0.24 |
| APF (degrees) | 27.1 ± 6.3 | 25.5 ± 5.5 | 0.322 | 0.28 |
| ADF (degrees) | 83.6 ± 9.0 | 91.4 ± 10.3 | 0.006 | −0.79 |
| ATOT (degrees) | 110.7 ± 12.6 | 116.9 ± 12.7 | 0.131 * | 0.49 |
| . | APF | ADF | ATOT | |||
|---|---|---|---|---|---|---|
| rs | p-Value | rs | p-Value | rs | p-Value | |
| SP (204) | ||||||
| Age | 0.03 | 0.674 | −0.20 | 0.005 | −0.17 | 0.015 |
| BMI | −0.16 | 0.029 | −0.29 | <0.001 | −0.30 | <0.001 |
| HGS | 0.05 | 0.452 | −0.27 | <0.001 | −0.22 | 0.002 |
| Controls (87) | ||||||
| Age | −0.11 | 0.328 | −0.12 | 0.282 | −0.16 | 0.129 |
| BMI | −0.11 | 0.333 | −0.18 | 0.100 | −0.22 | 0.039 |
| HGS | −0.05 | 0.667 | −0.12 | 0.282 | −0.15 | 0.196 |
| Adult SP (61) | Young SP (143) | |||||
|---|---|---|---|---|---|---|
| ß-Reg. Coef. | p-Value | p-Model | ß-Reg. Coef. | p-Value | p-Model | |
| APF | ||||||
| 0.312 | 0.266 | |||||
| Intercept | 36.383 | <0.001 | 34.326 | <0.001 | ||
| BMI | −0.585 | 0.162 | −0.558 | 0.091 | ||
| AGE | −0.074 | 0.523 | −0.076 | 0.903 | ||
| HGS | 0.103 | 0.332 | 0.170 | 0.288 | ||
| ADF | ||||||
| 0.102 | 0.469 | |||||
| Intercept | 72.649 | <0.001 | 115.736 | <0.0001 | ||
| BMI | −0.126 | 0.864 | −0.974 | 0.131 | ||
| AGE | 0.427 | 0.042 | −0.138 | 0.910 | ||
| HGS | 0.197 | 0.296 | 0.150 | 0.631 | ||
| ATOT | ||||||
| 0.348 | 0.158 | |||||
| Intercept | 109.032 | <0.001 | 150.062 | <0.0001 | ||
| BMI | −0.712 | 0.451 | −1.531 | 0.034 | ||
| AGE | 0.352 | 0.184 | −0.215 | 0.875 | ||
| HGS | 0.300 | 0.215 | 0.320 | 0.360 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francia, P.; Ferri Marini, C.; Bocchi, L.; Piccini, B.; Seghieri, G.; Federici, A.; Toni, S.; Lucertini, F. The Assessment of Ankle Range-of-Motion and Its Relationship with Overall Muscle Strength in a Cross-Section of Soccer Players. Sports 2023, 11, 12. https://doi.org/10.3390/sports11010012
Francia P, Ferri Marini C, Bocchi L, Piccini B, Seghieri G, Federici A, Toni S, Lucertini F. The Assessment of Ankle Range-of-Motion and Its Relationship with Overall Muscle Strength in a Cross-Section of Soccer Players. Sports. 2023; 11(1):12. https://doi.org/10.3390/sports11010012
Chicago/Turabian StyleFrancia, Piergiorgio, Carlo Ferri Marini, Leonardo Bocchi, Barbara Piccini, Giuseppe Seghieri, Ario Federici, Sonia Toni, and Francesco Lucertini. 2023. "The Assessment of Ankle Range-of-Motion and Its Relationship with Overall Muscle Strength in a Cross-Section of Soccer Players" Sports 11, no. 1: 12. https://doi.org/10.3390/sports11010012
APA StyleFrancia, P., Ferri Marini, C., Bocchi, L., Piccini, B., Seghieri, G., Federici, A., Toni, S., & Lucertini, F. (2023). The Assessment of Ankle Range-of-Motion and Its Relationship with Overall Muscle Strength in a Cross-Section of Soccer Players. Sports, 11(1), 12. https://doi.org/10.3390/sports11010012