
Association between Pain and Frequent Physical Exercise among Adults in the United States: A Cross-Sectional Database Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and MEPS Data Source
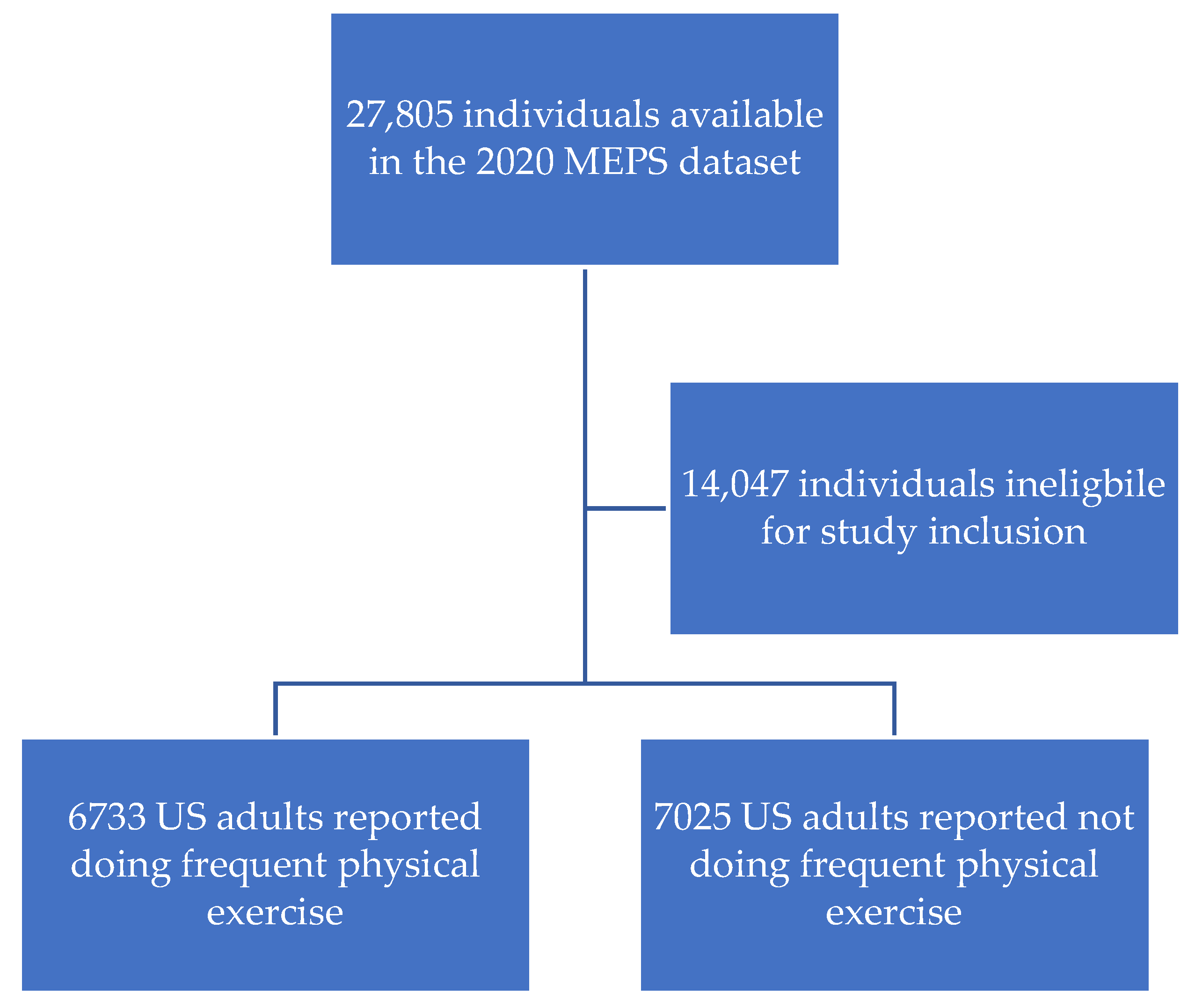
2.2. Study Inclusion Criteria
2.3. Dependent Variable
2.4. Independent Variable
2.5. Control Variables
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Summary of the Items Asked and Their Response Options in MEPS That Were Used in This Analysis
| Item | Response Options |
| Moderate/vigorous physical exercise 5x a week | Yes, no |
| Pain limits normal work | Not at all, a little bit, moderately, quite a bit, extremely |
| Age as of 12/31/20 | 0–85 (top-coded) |
| Sex | Male, female |
| Hispanic ethnicity | Hispanic, not Hispanic |
| Race | White-no other race reported, black-no other race reported, American Indian/Alaska native-no other race, Asian/native Hawaiian/pacific islander-no other race reported, multiple races reported |
| Marital status-12/31/20 | Married, widowed, divorced, separated, never married, under age 16-inapplicable |
| Years of Educ when first entered MEPS | No school/kindergarten only, elementary grades 1–8, high school grades 9–11, grade 12, 1 year college, 2 years college, 3 years college, 4 years college, 5+ years college |
| Employment status | Employed during the round, job to return to during the round, job during the round, not employed during the round |
| Family income as % of the poverty line | Poor/negative, near poor, low income, middle income, high income |
| Health insurance coverage indicator 2020 | Any private, public-only, uninsured |
| ADL screener | Yes, no |
| IADL screener | Yes, no |
| Limitations in physical functioning | Yes, no |
| Any limitation on work/housework/schoolwork | Yes, no |
| Perceived mental health status | Excellent, very good, good, fair, poor |
| Perceived health status | Excellent, very good, good, fair, poor |
| Multiple diagnoses of high blood press | Yes, no |
| Coronary heart disease diagnosis | Yes, no |
| Angina diagnosis | Yes, no |
| Heart attack (MI) diagnosis | Yes, no |
| Other heart disease diagnoses | Yes, no |
| Stroke diagnosis | Yes, no |
| Emphysema diagnosis | Yes, no |
| Chronic bronchitis last 12 months | Yes, no |
| High cholesterol diagnosis | Yes, no |
| Cancer diagnosis | Yes, no |
| Diabetes diagnosis | Yes, no |
| Joint pain last 12 months | Yes, no |
| Arthritis diagnosis | Yes, no |
| Asthma diagnosis | Yes, no |
| How often smoke cigarettes | Every day, some days, not at all |
| Adult body mass index | Continuous |
References
- International Association for the Study of Pain (IASP). Available online: https://www.iasp-pain.org/publications/iasp-news/iasp-announces-revised-definition-of-pain/ (accessed on 20 June 2023).
- Yong, R.J.; Mullins, P.M.; Bhattacharyya, N. Prevalence of chronic pain among adults in the United States. Pain 2022, 163, e328–e332. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, K.R.; Golightly, Y.M. Physical exercise as non-pharmacological treatment of chronic pain: Why and when. Best Pract. Res. Clin. Rheumatol. 2015, 29, 120–130. [Google Scholar] [CrossRef] [Green Version]
- OrthoInfo. Available online: https://orthoinfo.aaos.org/en/staying-healthy/aerobic-exercise/ (accessed on 20 June 2023).
- Cleveland Clinic. Available online: https://my.clevelandclinic.org/health/articles/7050-aerobic-exercise (accessed on 20 June 2023).
- Physical Activity Guidelines for Americans. Available online: https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition_Presentation.pdf (accessed on 20 June 2023).
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/physicalactivity/basics/pa-health/index.htm (accessed on 20 June 2023).
- Axon, D.R.; Bhattacharjee, S.; Warholak, T.L.; Slack, M.K. Xm2 scores for estimating total exposure to multimodal strategies identified by pharmacists for managing pain: Validity testing and clinical relevance. Pain Res. Manag. 2018, 2018, 2530286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Axon, D.R.; Patel, M.J.; Martin, J.R.; Slack, M.K. Use of multidomain management strategies by community dwelling adults with chronic pain: Evidence from a systematic review. Scand. J. Pain 2018, 19, 9–23. [Google Scholar] [CrossRef]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Grady, P.A.; Gough, L.L. Self-management: A comprehensive approach to management of chronic conditions. Am. J. Public Health 2014, 104, e25–e31. [Google Scholar] [CrossRef]
- Cooper, M.A.; Kluding, P.M.; Wright, D.E. Emerging relationships between exercise, sensory nerves, and neuropathic pain. Front. Neurosci. 2016, 10, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niederstrasser, N.G.; Attridge, N. Associations between pain and physical activity among older adults. PLoS ONE 2022, 17, e0263356. [Google Scholar] [CrossRef]
- Naugle, K.M.; Ohlman, T.; Naugle, K.E.; Riley, Z.A.; Keith, N.C.R. Physical activity behavior predicts endogenous pain modulation in older adults. Pain 2017, 158, 383–390. [Google Scholar] [CrossRef]
- Law, L.F.; Sluka, K.A. How does physical activity modulate pain? Pain 2016, 158, 369–370. [Google Scholar] [CrossRef] [Green Version]
- Axon, D.R.; Chien, J.; Dinh, H. Comparison of health care expenditures among U.S. older adults with pain who reported frequent exercise versus nonfrequent exercise. J. Aging Phys. Act. 2022, 30, 824–832. [Google Scholar] [CrossRef]
- Medical Expenditure Panel Survey Background. Available online: https://meps.ahrq.gov/mepsweb/about_meps/survey_back.jsp (accessed on 20 June 2023).
- Medical Expenditure Panel Survey Download Data Files. Available online: https://meps.ahrq.gov/mepsweb/data_stats/download_data_files.jsp (accessed on 20 June 2023).
- MEPS HC-224 2020 Full Year Consolidated Data File. Available online: https://meps.ahrq.gov/data_stats/download_data/pufs/h224/h224doc.shtml (accessed on 20 June 2023).
- MEPS HC-224 2020 Full Year Consolidated Data File Codebook. Available online: https://meps.ahrq.gov/data_stats/download_data/pufs/h224/h224cb.pdf (accessed on 20 June 2023).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ray, B.M.; Kelleran, K.J.; Eubanks, J.E.; Nan, N.; Ma, C.; Miles, D. Relationship between physical activity and pain in U.S. adults. Med. Sci. Sports Exerc. 2022, 55, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Zadro, J.R.; Shirley, D.; Amorim, A.; Pérez-Riquelme, F.; Ordoñana, J.R.; Ferreira, P.H. Are people with chronic low back pain meeting the physical activity guidelines? A co-twin control study. Spine J. 2017, 17, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Zhaoyang, R.; Martire, L.M. Daily sedentary behavior predicts pain and affect in knee arthritis. Ann. Behav. Med. 2019, 53, 642–651. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Public Health. Time to tackle the physical activity gender gap. Lancet Public Health 2019, 4, e360. [Google Scholar] [CrossRef] [Green Version]
- Xie, Z.; Jo, A.; Hong, Y.R. Electronic wearable device and physical activity among US adults: An analysis of 2019 hints data. Int. J. Med. Inform. 2020, 144, 104297. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/nchs/products/databriefs/db443.htm (accessed on 31 May 2023).
- Saffer, H.; Dave, D.; Grossman, M.; Leung, L.A. Racial, ethnic, and gender differences in physical activity. J. Hum. Cap. 2013, 7, 378–410. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Available online: https://blogs.cdc.gov/healthequity/2020/04/01/physical-inactivity/ (accessed on 31 May 2023).
- McMaughan, D.J.; Oloruntoba, O.; Smith, M.L. Socioeconomic status and access to Healthcare: Interrelated drivers for Healthy Aging. Front. Public Health 2020, 8, 231. [Google Scholar] [CrossRef]
- Physical Activity Tracking in Private Insurance: A Prospective Framework for the Policy Implications of the Use of Physical Activity Trackers by Private Insurers. Available online: https://www.actuaries.org.uk/system/files/field/document/Physical%20Activity%20Tracking.pdf (accessed on 31 May 2023).
- Morey, M.C.; Pieper, C.F.; Cornoni-Huntley, J. Physical fitness and functional limitations in community-dwelling older adults. Med. Sci. Sports Exerc. 1998, 30, 715–723. [Google Scholar] [CrossRef]
- Kim, B.Y.; Choi, D.H.; Jung, C.H.; Kang, S.K.; Mok, J.O.; Kim, C.H. Obesity and physical activity. J. Obes. Metab. Syndr. 2017, 26, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakicic, J.M.; Davis, K.K. Obesity and physical activity. Psychiatr. Clin. N. Am. 2014, 34, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Westerterp, K.R. Obesity and physical activity. Int. J. Obes. Relat. Metab. Disord. 1999, 23, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Atallah, N.; Adjibade, M.; Lelong, H.; Hercberg, S.; Galan, P.; Assmann, K.; Kesse-Guyot, E. How healthy lifestyle factors at midlife relate to healthy aging. Nutrients 2018, 10, 854. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Frequent Physical Exercise: Yes N = 6733 | Frequent Physical Exercise: No N = 7025 | Total N = 13,758 | p Value | |
|---|---|---|---|---|
| Percent [95% CI] | Percent [95% CI] | Percent [95% CI] | ||
| Pain: | <0.0001 | |||
| Extreme | 0.7 [0.4, 0.9] | 3.3 [2.9, 3.8] | 2.0 [1.7, 2.2] | |
| Quite a bit | 3.6 [2.9, 4.2] | 7.1 [6.4, 7.8] | 5.3 [4.9, 5.8] | |
| Moderate | 6.2 [5.5, 6.9] | 8.2 [7.4, 9.0] | 7.2 [6.7, 7.7] | |
| Little | 22.3 [21.1, 23.6] | 22.8 [21.5, 24.0] | 22.6 [21.6, 23.5] | |
| None | 67.2 [65.7, 68.8] | 58.6 [57.0, 60.1] | 62.9 [61.8, 64.1] | |
| Demographic variables: | ||||
| Age | 0.5548 | |||
| ≥65 | 21.8 [20.5, 23.1] | 22.7 [21.4, 24.0] | 22.3 [21.2, 23.3] | |
| 40–64 | 40.8 [39.3, 42.4] | 40.8 [39.2, 42.3] | 40.8 [39.6, 42.0] | |
| 18–39 | 37.4 [35.7, 39.1] | 36.5 [34.8, 38.2] | 36.9 [35.7, 38.2] | |
| Sex | <0.0001 | |||
| Male | 52.3 [51.0, 53.6] | 44.1 [42.8, 45.5] | 48.3 [47.4, 49.1] | |
| Female | 47.7 [46.4, 49.0] | 55.9 [54.5, 57.2] | 51.7 [50.9, 52.6] | |
| Hispanic | <0.0001 | |||
| Yes | 15.0 [13.0, 17.0] | 19.0 [16.6, 21.4] | 17.0 [15.0, 19.0] | |
| No | 85.0 [83.0, 87.0] | 81.0 [78.6, 83.4] | 83.0 [81.0, 85.0] | |
| White race | <0.0001 | |||
| Yes | 80.9 [79.0, 82.7] | 75.6 [73.5, 77.8] | 78.3 [76.6, 80.0] | |
| No | 19.1 [17.3, 21.0] | 24.4 [22.2, 26.5] | 21.7 [20.0, 23.4] | |
| Married | 0.0016 | |||
| Yes | 53.3 [51.5, 55.2] | 50.3 [48.7, 51.8] | 51.8 [50.4, 53.2] | |
| No | 46.7 [44.8, 48.5] | 49.7 [48.2, 51.3] | 48.2 [46.8, 49.6] | |
| Economic variables: | ||||
| More than high school education | 0.0001 | |||
| Yes | 62.1 [60.2, 64.1] | 57.7 [55.6, 59.8] | 59.9 [58.3, 61.6] | |
| No | 37.9 [35.9, 39.8] | 42.3 [40.2, 44.4] | 40.1 [38.4, 41.7] | |
| Employed | <0.0001 | |||
| Yes | 67.9 [66.3, 69.5] | 62.4 [60.8, 64.1] | 65.2 [64.0, 66.4] | |
| No | 32.1 [30.5, 33.7] | 37.6 [35.9, 39.2] | 34.8 [33.6, 36.0] | |
| Low income | <0.0001 | |||
| Yes | 21.1 [19.5, 22.7] | 28.7 [26.7, 30.6] | 24.9 [23.3, 26.4] | |
| No | 78.9 [77.3, 80.5] | 71.3 [69.4, 73.3] | 75.1 [73.6, 76.7] | |
| Health coverage | <0.0001 | |||
| Private | 71.3 [69.4, 73.2] | 64.8 [63.1, 66.4] | 68.1 [66.6, 69.5] | |
| Public | 22.1 [20.5, 23.7] | 26.4 [25.0, 27.9] | 24.3 [23.1, 25.4] | |
| None | 6.6 [5.6, 7.6] | 8.8 [7.5, 10.0] | 7.7 [6.7, 8.6] | |
| Limitation variables: | ||||
| ADL limitation | <0.0001 | |||
| Yes | 0.7 [0.5, 1.0] | 2.5 [2.0, 3.0] | 1.6 [1.3, 1.9] | |
| No | 99.3 [99.0, 99.5] | 97.5 [97.0, 98.0] | 98.4 [98.1, 98.7] | |
| IADL limitation | <0.0001 | |||
| Yes | 1.8 [1.3, 2.3] | 4.5 [3.8, 5.2] | 3.2 [2.7, 3.6] | |
| No | 98.2 [97.7, 98.7] | 95.5 [94.8, 96.2] | 96.8 [96.4, 97.3] | |
| Functional limitation | <0.0001 | |||
| Yes | 7.4 [6.7, 8.2] | 17.2 [15.9, 18.5] | 12.3 [11.5, 13.1] | |
| No | 92.6 [91.8, 93.3] | 82.8 [81.5, 84.1] | 87.7 [86.9, 88.5] | |
| Work limitation | <0.0001 | |||
| Yes | 5.7 [4.9, 6.5] | 12.7 [11.6, 13.9] | 9.2 [8.4, 10.0] | |
| No | 94.3 [93.5, 95.1] | 87.3 [86.1, 88.4] | 90.8 [90.0, 91.6] | |
| Health variables: | ||||
| Good mental health | <0.0001 | |||
| Yes | 93.3 [92.5, 94.2] | 88.0 [87.0, 89.1] | 90.7 [90.0, 91.4] | |
| No | 6.7 [5.8, 7.5] | 12.0 [10.9, 13.0] | 9.3 [8.6, 10.0] | |
| Good general health | <0.0001 | |||
| Yes | 92.7 [91.8, 93.7] | 83.3 [82.2, 84.3] | 88.0 [87.2, 88.8] | |
| No | 7.3 [6.3, 8.2] | 16.7 [15.7, 17.8] | 12.0 [11.2, 12.8] | |
| Multimorbidity | <0.0001 | |||
| Yes | 38.4 [36.8, 40.0] | 45.1 [43.5, 46.8] | 41.7 [40.6, 42.9] | |
| No | 61.6 [60.0, 63.2] | 54.9 [53.2, 56.5] | 58.3 [57.1, 59.4] | |
| Smoker | 0.0620 | |||
| Yes | 11.2 [10.0, 12.4] | 12.7 [11.6, 13.8] | 11.9 [11.1, 12.8] | |
| No | 88.8 [87.6, 90.0] | 87.3 [86.2, 88.4] | 88.1 [87.2, 88.9] | |
| Overweight/obese | <0.0001 | |||
| Yes | 61.6 [59.8, 63.5] | 71.0 [69.3, 72.7] | 66.2 [64.8, 67.6] | |
| No | 38.4 [36.5, 40.2] | 29.0 [27.3, 30.7] | 33.8 [32.4, 35.2] |
| Pain | Odds Ratio [95% CI] |
|---|---|
| Extreme vs. none | 0.2 [0.1, 0.2] |
| Quite a bit vs. none | 0.4 [0.4, 0.6] |
| Moderate vs. none | 0.7 [0.6, 0.8] |
| Little vs. none | 0.9 [0.8, 0.9] |
| Adjusted for Pain & Demographic Variables | Adjusted for Pain, Demographic & Economic Variables | Adjusted for Pain, Demographic, Economic, & Limitation Variables | Adjusted for Pain, Demographic, Economic, Limitation, & Health Variables | |
|---|---|---|---|---|
| Odds Ratio [95% CI] | Odds Ratio [95% CI] | Odds Ratio [95% CI] | Odds Ratio [95% CI] | |
| Pain: | ||||
| Pain, extreme vs. none | 0.2 [0.1, 0.2] | 0.2 [0.1, 0.3] | 0.3 [0.2, 0.5] | 0.4 [0.2, 0.7] |
| Pain, quite a bit vs. none | 0.4 [0.3, 0.5] | 0.4 [0.4, 0.6] | 0.5 [0.4, 0.7] | 0.7 [0.5, 0.9] |
| Pain, moderate vs. none | 0.6 [0.5, 0.7] | 0.6 [0.5, 0.7] | 0.7 [0.6, 0.9] | 0.8 [0.7, 1.1] |
| Pain, little vs. none | 0.8 [0.7, 0.9] | 0.8 [0.7, 0.9] | 0.8 [0.7, 1.0] | 0.9 [0.8, 1.0] |
| Demographic variables: | ||||
| Age, ≥65 vs. 18–39 | 1.1 [0.9, 1.2] | 1.1 [0.9, 1.2] | 1.2 [1.0, 1.5] | 1.3 [1.1, 1.6] |
| Age, 40–64 vs. 18–39 | 1.1 [0.9, 1.2] | 1.0 [0.9, 1.2] | 1.2 [1.0, 1.3] | 1.2 [1.1, 1.4] |
| Sex, male vs. female | 1.4 [1.3, 1.5] | 1.4 [1.3, 1.5] | 1.3 [1.2, 1.4] | 1.4 [1.2, 1.5] |
| Hispanic, yes vs. no | 0.7 [0.6, 0.8] | 0.7 [0.6, 0.8] | 0.7 [0.6, 0.8] | 0.7 [0.6, 0.9] |
| White race, yes vs. no | 1.5 [1.3, 1.7] | 1.4 [1.2, 1.6] | 1.5 [1.3, 1.8] | 1.5 [1.3, 1.8] |
| Married, yes vs. no | 1.0 [1.0, 1.1] | 1.0 [0.9, 1.1] | 1.0 [0.9, 1.1] | 1.0 [0.9, 1.1] |
| Economic variables: | ||||
| More than high school education, yes vs. no | 1.0 [0.9, 1.1] | 1.0 [0.9, 1.1] | 1.0 [0.8, 1.1] | |
| Employed, yes vs. no | 1.0 [0.9, 1.2] | 0.9 [0.8, 1.1] | 1.0 [0.8, 1.1] | |
| Low income, yes vs. no | 0.8 [0.7, 0.9] | 0.9 [0.7, 1.0] | 0.9 [0.8, 1.1] | |
| Health coverage, private vs. none | 1.3 [1.1, 1.6] | 1.3 [1.0, 1.6] | 1.3 [1.0, 1.6] | |
| Health coverage, public vs. none | 1.3 [1.1, 1.6] | 1.3 [1.0, 1.7] | 1.3 [1.0, 1.8] | |
| Limitation variables: | ||||
| ADL limitation, yes vs. no | 0.7 [0.4, 1.3] | 0.7 [0.4, 1.3] | ||
| IADL limitation, yes vs. no | 0.9 [0.6, 1.4] | 0.9 [0.6, 1.4] | ||
| Functional limitation, yes vs. no | 0.6 [0.5, 0.7] | 0.6 [0.5, 0.7] | ||
| Work limitation, yes vs. no | 0.8 [0.7, 1.1] | 0.9 [0.7, 1.2] | ||
| Health variables: | ||||
| Good mental health, yes vs. no | 1.2 [0.9, 1.5] | |||
| Good general health, yes vs. no | 1.6 [1.3, 2.0] | |||
| Multimorbidity, yes vs. no | 0.9 [0.8, 1.0] | |||
| Smoker, yes vs. no | 1.0 [0.8, 1.1] | |||
| Overweight/obese, yes vs. no | 0.7 [0.6, 0.8] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Axon, D.R.; Maldonado, T. Association between Pain and Frequent Physical Exercise among Adults in the United States: A Cross-Sectional Database Study. Sports 2023, 11, 126. https://doi.org/10.3390/sports11070126
Axon DR, Maldonado T. Association between Pain and Frequent Physical Exercise among Adults in the United States: A Cross-Sectional Database Study. Sports. 2023; 11(7):126. https://doi.org/10.3390/sports11070126
Chicago/Turabian StyleAxon, David R., and Taylor Maldonado. 2023. "Association between Pain and Frequent Physical Exercise among Adults in the United States: A Cross-Sectional Database Study" Sports 11, no. 7: 126. https://doi.org/10.3390/sports11070126
APA StyleAxon, D. R., & Maldonado, T. (2023). Association between Pain and Frequent Physical Exercise among Adults in the United States: A Cross-Sectional Database Study. Sports, 11(7), 126. https://doi.org/10.3390/sports11070126