Injuries and Persistent Pain in Elite Adolescent Archery Athletes: A Cross-Sectional Epidemiological Study

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
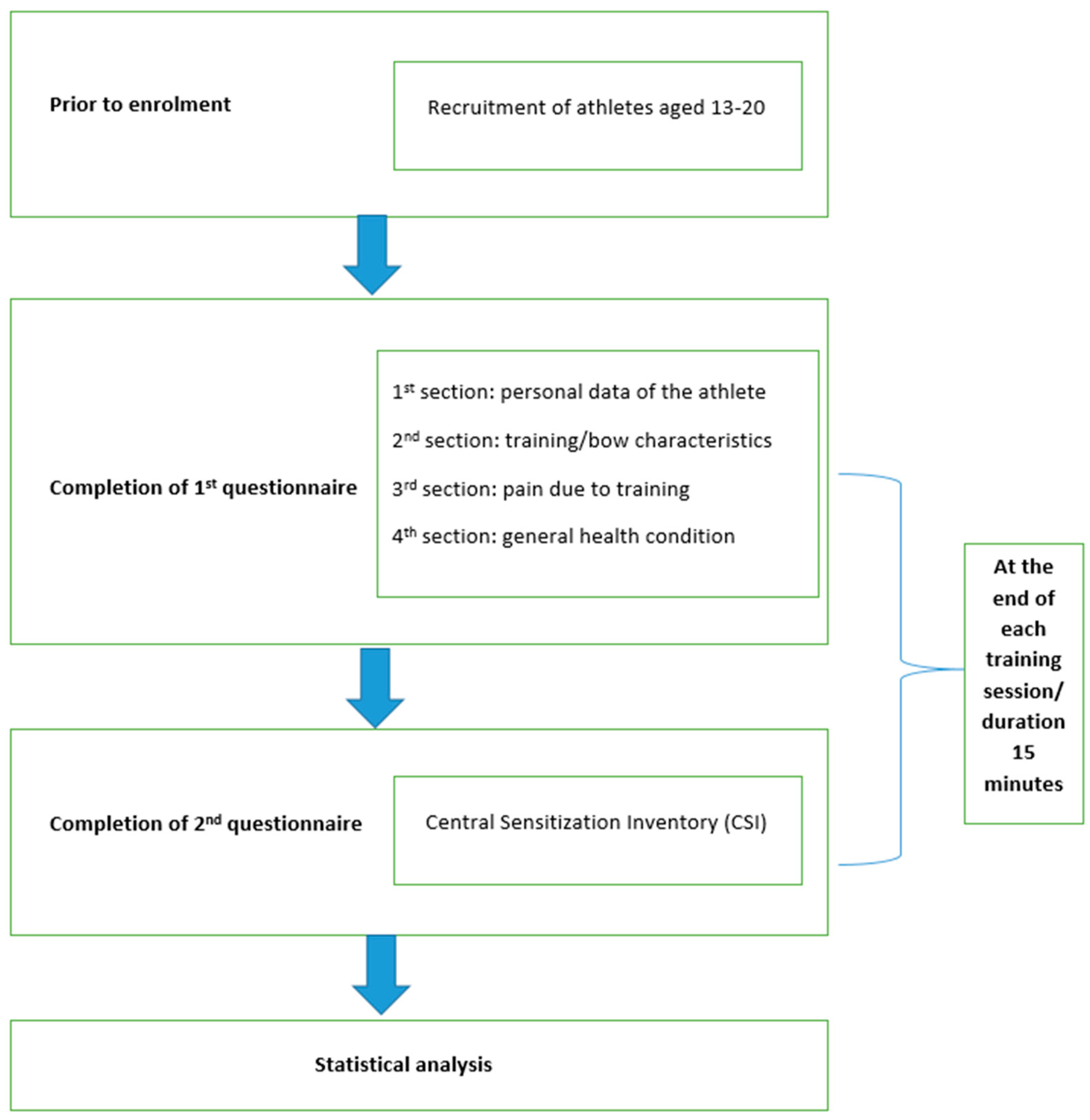
2.1. Instruments/Measurement
2.2. Statistical Analysis
3. Results
3.1. Training Characteristics
3.2. Competition Participation
3.3. Training Components and Practices
3.4. Pain and Injury Analysis
4. Discussion
4.1. Limitations
4.2. Recommendations for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Aspect | Archery [22,50] | Swimming [51,52] | Tennis [53,54] | Golf [55,56] |
|---|---|---|---|---|
| Physical Demands | Requires upper body strength and stability, with emphasis on shoulder and back muscles. | Emphasizes full-body aerobic endurance, along with upper body and core strength. | Demands agility, speed, and coordination, with rapid changes in direction and pace. | Focuses on precision and control, with minimal physical exertion. |
| Injury Risk | Risk of overuse injuries in the shoulder and back due to repetitive movements. | Low risk of overuse injuries, but potential for shoulder injuries from improper technique. | Moderate risk of overuse injuries due to repetitive movements and intense play. | Lower risk of overuse injuries, but potential for strain from swinging motion. |
| Mental Focus | Requires intense concentration and mental discipline to maintain consistent form and accuracy. | Demands focus on technique and pacing, with attention to breathing and stroke mechanics. | Requires mental agility, quick decision-making, and adaptability during matches. | Emphasizes mental toughness and concentration, especially during precision shots. |
| Training Intensity | Training involves regular practice to build muscle memory and refine technique, with occasional breaks | Involves structured workouts and interval training to build endurance and improve technique. | Includes drills, matches, and physical conditioning to improve endurance and skill. | Practice typically involves repetitive swinging motions and putting techniques. |
| Equipment | Requires specialized equipment including bows, arrows, and protective gear. | Requires minimal equipment, with focus on swimwear and goggles. | Requires specific gear like rackets, balls, and appropriate footwear for surface. | Requires clubs, balls, and tees, but less frequent equipment purchases. |
References
- Beets, M.W.; Pitetti, K.H. Contribution of physical education and sport to health-related fitness in high school students. J. Sch. Health 2005, 75, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Kawabe, H.; Murata, K.; Shibata, H.; Hirose, H.; Tsujioka, M.; Saito, I.; Saruta, T. Participation in school sports clubs and related effects on cardiovascular risk factors in young males. Hypertens. Res. 2000, 23, 227–232. [Google Scholar] [CrossRef]
- National Council of Youth Sports. Report on Trends and Participation in Organized Youth Sports. Available online: https://www.ncys.org (accessed on 15 January 2021).
- Brenner, J.S.; Council on Sports Medicine and Fitness; LaBella, C.R.; Brookes, M.A.; Diamond, A.; Hennrikus, W.; Kelly, A.K.W.; LaBotz, M.; Logan, K.; Loud, K.J.; et al. Sports Specialization and Intensive Training in Young Athletes. Pediatrics 2016, 138, e20162148. [Google Scholar] [CrossRef] [PubMed]
- DiFiori, J.P.; Benjamin, H.J.; Brenner, J.S.; Gregory, A.; Jayanthi, N.; Landry, G.L.; Luke, A. Overuse injuries and burnout in youth sports: A position statement from the American Medical Society for Sports Medicine. Br. J. Sports Med. 2014, 48, 287–288. [Google Scholar] [CrossRef] [PubMed]
- Jayanthi, N.A.; Labella, C.R.; Fischer, D.; Pasulka, J.; Dugas, L.R. Sports-specialized intensive training and the risk of injury in young athletes: A clinical case-control study. Am. J. Sports Med. 2015, 43, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Grimmer, K.A.; Jones, D.; Williams, J. Prevalence of adolescent injury from recreational exercise: An australian perspective. J. Adolesc. Health 2000, 27, 266–272. [Google Scholar] [CrossRef]
- Haraldsdottir, K.; Watson, A.M. Psychosocial Impacts of Sports-Related Injuries in Adolescent Athletes. Optom. Vis. Sci. 2021, 20, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Kinney, C.-D. Archery: An Olympic History, 1900–2004; Easton, P., Ed.; World Sport Research & Publication Inc.: Palo Alto, CA, USA, 2005; p. 177. [Google Scholar]
- Subhash, C. Benefit of archery game to improve health and fitness. Int. J. Yoga Physiother. Phys. Educ. 2018, 3, 184–185. [Google Scholar]
- Shinohara, H.; Urabe, Y. Analysis of muscular activity in archery: A comparison of skill level. J. Sports Med. Phys. Fit. 2018, 58, 1752–1758. [Google Scholar] [CrossRef] [PubMed]
- Zulkifli, A.; Zahari, T.; Hasnun, A.-H.; Mohd, A.-H.; Nasrul, H.-J.; Kumaran, K. Biomechanics measurements in archery. Int. Conf. Mech. Eng. Res. 2013, 2, 1–9. [Google Scholar]
- Brachman, A.; Kamieniarz, A.; Michalska, J.; Pawłowski, M.; Słomka, K.J.; Juras, G. Balance Training Programs in Athletes—A Systematic Review. J. Hum. Kinet. 2017, 58, 45–64. [Google Scholar] [CrossRef] [PubMed]
- Sandeep, S.; Sukhpreet, K. Study of motor nerve conduction velocities of upper extremity in the female archers. Int. J. Phys. Educ. Sports Health 2015, 1, 31–33. [Google Scholar]
- Saroja, G.; Aseer, P.A.L.; Venkata Sai, P.M. Diagnostic accuracy of provocative tests in lateral epicondylitis. Int. J. Physiother. Res. 2014, 2, 815–823. [Google Scholar] [CrossRef]
- Adkitte, R.G.; Shah, S.; Jain, S.; Walia, S.; Chopra, N.; Kumar, H. Common injuries amongst Indian elite archers: A prospective study. Saudi J. Sports Med. 2016, 16, 210. [Google Scholar] [CrossRef]
- Iii, C.A.R.; Briner, W.W. Corticosteroid injection for treatment of de Quervain’s tenosynovitis: A pooled quantitative literature evaluation. J. Am. Board Fam. Med. 2003, 16, 102–106. [Google Scholar] [CrossRef]
- Ilyas, A.M.; Ast, M.; Schaffer, A.A.; Thoder, J. De quervain tenosynovitis of the wrist. J. Am. Acad. Orthop. Surg. 2007, 15, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Niestroj, C.K.; Schöffl, V.; Küpper, T. Acute and overuse injuries in elite archers. J. Sports Med. Phys. Fit. 2018, 58, 1063–1070. [Google Scholar] [CrossRef]
- Grover, J.-K.; Akhoury, G.-K.-S. Prevalence of shoulder pain in competitive archery. Asian J. Sports Med. 2016, 8, 6. [Google Scholar] [CrossRef]
- Ertan, H. Injury patterns among Turkish archers. Shield-Res. J. Phys. Educ. Sports Sci. 2006, 19–29. [Google Scholar]
- Konda, M.; Mangal, R.; Daniel, A.; Stead, T.S.; Ganti, L. Archery-Related Musculoskeletal Injuries: An Epidemiological Study Revealing Injury Sites, Risk Factors, and Implications for Prevention. Orthop. Rev. 2023, 15, 88933. [Google Scholar] [CrossRef]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The development and psychometric validation of the central sensitization inventory. Pain Pr. 2012, 12, 276–285. [Google Scholar] [CrossRef]
- Neblett, R.M.; Hartzell, M.M.; Cohen, H.; Mayer, T.G.; Williams, M.; Choi, Y.M.; Gatchel, R.J.P. Ability of the central sensitization inventory to identify central sensitivity syndromes in an outpatient chronic pain sample. Clin. J. Pain 2015, 31, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Bilika, P.; Neblett, R.; Georgoudis, G.; Dimitriadis, Z.; Fandridis, E.; Strimpakos, N.; Kapreli, E. Cross-cultural Adaptation and Psychometric Properties of the Greek Version of the Central Sensitization Inventory. Pain Pr. 2020, 20, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Campbell, I. Chi-squared and Fisher–Irwin tests of two-by-two tables with small sample recommendations. Stat. Med. 2007, 26, 3661–3675. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.T.E. The analysis of 2 × 2 contingency tables—Yet again. Stat. Med. 2011, 30, 890. [Google Scholar] [CrossRef] [PubMed]
- Palsbo, S.E. Epidemiology of recreational archery injuries: Implications for archery ranges and injury prevention. J. Sports Med. Phys. Fit. 2012, 52, 293–299. [Google Scholar]
- Mann, D.L.; Littke, N. Shoulder injuries in archery. Can J. Sport Sci. 1989, 14, 85–92. [Google Scholar] [PubMed]
- FITA. Becomes World Archery Federation. Available online: https://worldarchery.org/committees (accessed on 17 January 2024).
- Côté, J.; Gilbert, W. An integrative definition of coaching effectiveness and expertise. Int. J. Sports Sci. Coach. 2009, 4, 307–323. [Google Scholar] [CrossRef]
- Ertan, H.; Kentel, B.; Tümer, S.T.; Korkusuz, F. Activation patterns in forearm muscles during archery shooting. Hum. Mov. Sci. 2003, 22, 37–45. [Google Scholar] [CrossRef]
- Martin, P.E.; Siler, W.L.; Hoffman, D. Electromyographic analysis of bow string release in highly skilled archers. J. Sports Sci. 1990, 8, 215–221. [Google Scholar] [CrossRef]
- Zemková, E.; Zapletalová, L. The Role of Neuromuscular Control of Postural and Core Stability in Functional Movement and Athlete Performance. Front. Physiol. 2022, 13, 796097. [Google Scholar] [CrossRef]
- Kuch, A.; Tisserand, R.; Durand, F.; Monnet, T.; Debril, J.-F. Postural adjustments preceding string release in trained archers. J. Sports Sci. 2023, 41, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Cevdet, T. Shooting dynamics in archery: A multidimensional analysis for drawing to releasing in male archers. Procedia Eng. 2011, 13, 290–296. [Google Scholar] [CrossRef]
- Singh, A.K.; Lhee, S.-H. Injuries in archers. Saudi J. Sports Med. 2016, 16, 168. [Google Scholar] [CrossRef]
- Gundersen, A.; Borgstrom, H.; McInnis, K.C. Trunk Injuries in Athletes. Optom. Vis. Sci. 2021, 20, 150–156. [Google Scholar] [CrossRef]
- Covey, C.J.; Knobloch, A.C.; Kim, A.R. Hip Pain in an Athlete. Optom. Vis. Sci. 2023, 22, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Fishbain, D.A.; Cutler, R.; Rosomoff, H.L.; Rosomoff, R.S. Chronic pain-associated depression: Antecedent or consequence of chronic pain? A Review. Clin. J. Pain 1997, 13, 116–137. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Longo, U.G.; Gougoulias, N.; Loppini, M.; Denaro, V. Long-term health outcomes of youth sports injuries. Br. J. Sports Med. 2010, 44, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Paraskevopoulos, E.; Gioftsos, G.; Georgoudis, G.; Papandreou, M. Perceived Barriers and Facilitators of Sports Rehabilitation Adherence in Injured Volleyball Athletes: A Qualitative Study from Greece. J. Clin. Sport Psychol. 2023, 17, 86–105. [Google Scholar] [CrossRef]
- Paraskevopoulos, E.; Simeonidis, T.; Tsolakis, C.; Koulouvaris, P.; Papandreou, M. Mirror Cross-Exercise on a Kinetic Chain Approach Improves Throwing Performance in Professional Volleyball Athletes with Scapular Dyskinesis. J. Sport Rehabil. 2021, 31, 131–139. [Google Scholar] [CrossRef]
- Paraskevopoulos, E.; Pamboris, G.M.; Papandreou, M. The Changing Landscape in Upper Limb Sports Rehabilitation and Injury Prevention. Sports 2023, 11, 80. [Google Scholar] [CrossRef] [PubMed]
- Paraskevopoulos, E.; Kottaridis, F.-M.; Moutzouri, M.; Koumantakis, G.A.; Antonakis-Karamintzas, D.; Tsolakis, C.; Koulouvaris, P.; Christakou, A.; Papandreou, M. Preliminary Insights into the Diagnostic Accuracy of the Modified Arm Care Screen Test for Overhead Athletes: An On-Field Tool for Injury Prevention. Healthcare 2023, 11, 3046. [Google Scholar] [CrossRef] [PubMed]
- Matsel, K.A.; Butler, R.J.; Malone, T.R.; Hoch, M.C.; Westgate, P.M.; Uhl, T.L. Current concepts in arm care exercise programs and injury risk reduction in adolescent baseball players: A clinical review. Sports Health A Multidiscip. Approach 2021, 13, 245–250. [Google Scholar] [CrossRef] [PubMed]
- McElheny, K.; Sgroi, T.; Carr, J.B. Efficacy of Arm Care Programs for Injury Prevention. Curr. Rev. Musculoskelet. Med. 2021, 14, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Liaghat, B.; Pedersen, J.R.; Husted, R.S.; Pedersen, L.L.; Thorborg, K.; Juhl, C.B. Diagnosis, prevention and treatment of common shoulder injuries in sport: Grading the evidence—A statement paper commissioned by the Danish Society of Sports Physical Therapy (DSSF). Br. J. Sports Med. 2023, 57, 408–416. [Google Scholar] [CrossRef]
- Alberola-Zorrilla, P.; Castaño-Ortiz, C.; Sánchez-Zuriaga, D. Where do archers hurt? Epidemiology of injuries during archery practice. Physiother. Theory Pract. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wanivenhaus, F.; Fox, A.J.S.; Chaudhury, S.; Rodeo, S.A. Epidemiology of injuries and prevention strategies in competitive swimmers. Sports Health A Multidiscip. Approach 2012, 4, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.; Collins, M.; Posthumus, M. Risk factors for shoulder pain and injury in swimmers: A critical systematic review. Phys. Sportsmed. 2015, 43, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Vasenina, E.; Stout, J.R.; Fukuda, D.H. Tennis Specialization and Consequence of Injury/Illness Following Retirement. Sports 2023, 11, 106. [Google Scholar] [CrossRef]
- Abrams, G.D.; Renstrom, P.A.; Safran, M.R. Epidemiology of musculoskeletal injury in the tennis player. Br. J. Sports Med. 2012, 46, 492–498. [Google Scholar] [CrossRef]
- Meira, E.P.; Brumitt, J. Minimizing injuries and enhancing performance in golf through training programs. Sports Heal. A Multidiscip. Approach 2010, 2, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.I.; Khan, N.H.M.; Saeed, H.; Yawar, B.; Malik, M.; Saghir, M.; Khan, A.H. Injuries associated with golf: A qualitative study. Ann. Med. Surg. 2022, 78, 103899. [Google Scholar] [CrossRef] [PubMed]


| Variables | Female Athletes n = 96 | Male Athletes n = 104 | Total N = 200 | p-Value |
|---|---|---|---|---|
| Age (years) | 16.78 (±1.67) | 16.99 (±1.57) | 16.89 (±0.11) | p = 0.36 |
| Height (m) | 1.67 (±0.07) | 1.78 (±0.08) | 1.73 (±0.01) | p < 0.01 |
| Weight (Kg) | 60.11 (±8.51) | 75.60 (±13.6) | 68.17 (±0.97) | p < 0.01 |
| BMI | 21.52 (±2.73) | 23.80 (±4.81) | 22.71 (±4.10) | p < 0.01 |
| Training characteristics of the archery athletes (N = 200) | ||||
| Practice (years) | 6.42 (±2.59) | 6.64 (±3.07) | 6.53 (±0.20) | p = 0.57 |
| Upper arm dominance | ||||
| Right | 88 (91.7%) | 90 (86.5%) | 178 (89%) | p = 0.27 |
| Left | 8 (8.3%) | 14 (13.5%) | 22 (11%) | p = 0.72 |
| Cord pulling preference side | ||||
| Right | 85 (88.5%) | 92 (88.5%) | 177 (88.5%) | p = 0.99 |
| Left | 11 (11.5%) | 12 (11.5%) | 23 (11.5%) | p = 0.99 |
| Bow weight (lb) | 15.44 (±8.01) | 16.99 (±1.57) | 16.89 (±1.6) | p = 0.33 |
| Bow type | ||||
| Recurve | 69 (71.9%) | 76 (73.1%) | 145 (72.5%) | p = 0.87 |
| Compound | 27 (28.1%) | 28 (26.9%) | 55 (27.5%) | p = 0.92 |
| Training hours per week (h) | 15.44 (±8.501) | 14.38 (±7.52) | 14.89 (±7.76) | p = 0.33 |
| Arrows per training session | 160.36 (±63.81) | 165.10 (±65.07) | 162.84 (±64.35) | p = 0.60 |
| Number of matches | 11.94 (±10.78) | 10.26 (±6.92) | 11.07 (±9) | p = 0.19 |
| Duration of matches (min) | 86.54 (±108.54) | 118.72 (±127.45) | 103 (±12.55) | p = 0.36 |
| Training components | ||||
| Upper body strengthening | 79 (82.3%) | 90 (86.5%) | 169 (84.5%) | p = 0.45 |
| Lower body strengthening | 49 (51%) | 49 (47.1%) | 98 (49%) | p = 0.70 |
| Dominant arm strengthening | 69 (71.9%) | 76 (73.1%) | 145 (72.5%) | p = 0.87 |
| Non dominant arm strengthening | 60 (62.5%) | 66 (63.5%) | 126 (63%) | p = 0.91 |
| Aerobic conditioning | 50 (52.1%) | 49 (47.1%) | 99 (49.5%) | p = 0.62 |
| Stretching before training | 73 (76%) | 73 (70.2%) | 146 (73%) | p = 0.43 |
| Stretching after training | 60 (62.5%) | 56 (53.8%) | 116 (58%) | p = 0.34 |
| Relaxation techniques | 53 (55.2%) | 56 (53.8%) | 109 (54.5%) | p = 0.87 |
| Concentration techniques | 54 (56.3%) | 67 (64.4%) | 121 (60.5%) | p = 0.37 |
| Breathing exercises | 52 (54.2%) | 62 (59.6%) | 114 (57%) | p = 0.56 |
| Warm up | 86 (92.7%) | 87 (83.7%) | 176 (88%) | |
| Duration (min) | 15.01 (±8.45) | 13.27 (±14.29) | 14.18 (±11.595) | p = 0.35 |
| Cooldown | 42 (43.8%) | 46 (44.2%) | 88 (44%) | |
| Duration (min) | 14.46 (±8.13) | 16.12 (±18.23) | 15.34 (±14.35) | p = 0.59 |
| Annual physical assessment | 54 (56.3%) | 55 (52.9%) | 109 (54.5%) | p = 0.72 |
| Prescribed diet | 31 (32.3%) | 35 (33.7%) | 66 (33%) | p = 0.90 |
| Variables | Subclinical (CSI = 0–29) n = 157 78.5% | Mild (SCI = 30–39) n = 27 13.5% | Moderate (SCI = 40–49) n = 11 5.5% | Severe (SCI = 50–59) n = 3 1.5% | Extreme (SCI = 60–100) n = 2 1% | CSI Score > 40 n = 16 8% |
|---|---|---|---|---|---|---|
| CSI Score (mean ± SD) | 15.37 ± 7.264 | 34.70 ± 2.686 | 42.73 ± 2.760 | 52.67 ± 2.887 | 64 ± 0 | 47.25 ± 8.029 |
| Variables | Weekly Training Frequency | Training Duration Per Session | Number of Competitions Per Year | Competition Duration Per Match |
|---|---|---|---|---|
| CSI Score | r = 0.20, p = 0.775 | r = 0.69, p = 0.335 | r = 0.33, p = 0.643 | r = 0.08, p = 0.224 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasilis, N.; Kyriakides, A.; Vasilopoulos, G.; Chatzitimotheou, M.; Gonidakis, G.; Kotsakis, A.; Paraskevopoulos, E.; Kapreli, E. Injuries and Persistent Pain in Elite Adolescent Archery Athletes: A Cross-Sectional Epidemiological Study. Sports 2024, 12, 101. https://doi.org/10.3390/sports12040101
Vasilis N, Kyriakides A, Vasilopoulos G, Chatzitimotheou M, Gonidakis G, Kotsakis A, Paraskevopoulos E, Kapreli E. Injuries and Persistent Pain in Elite Adolescent Archery Athletes: A Cross-Sectional Epidemiological Study. Sports. 2024; 12(4):101. https://doi.org/10.3390/sports12040101
Chicago/Turabian StyleVasilis, Nikolaos, Athanasios Kyriakides, George Vasilopoulos, Maria Chatzitimotheou, Grigorios Gonidakis, Athanasios Kotsakis, Eleftherios Paraskevopoulos, and Eleni Kapreli. 2024. "Injuries and Persistent Pain in Elite Adolescent Archery Athletes: A Cross-Sectional Epidemiological Study" Sports 12, no. 4: 101. https://doi.org/10.3390/sports12040101
APA StyleVasilis, N., Kyriakides, A., Vasilopoulos, G., Chatzitimotheou, M., Gonidakis, G., Kotsakis, A., Paraskevopoulos, E., & Kapreli, E. (2024). Injuries and Persistent Pain in Elite Adolescent Archery Athletes: A Cross-Sectional Epidemiological Study. Sports, 12(4), 101. https://doi.org/10.3390/sports12040101