

The Impact of a 12-Week Aqua Fitness Program on the Physical Fitness of Women over 60 Years of Age
 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
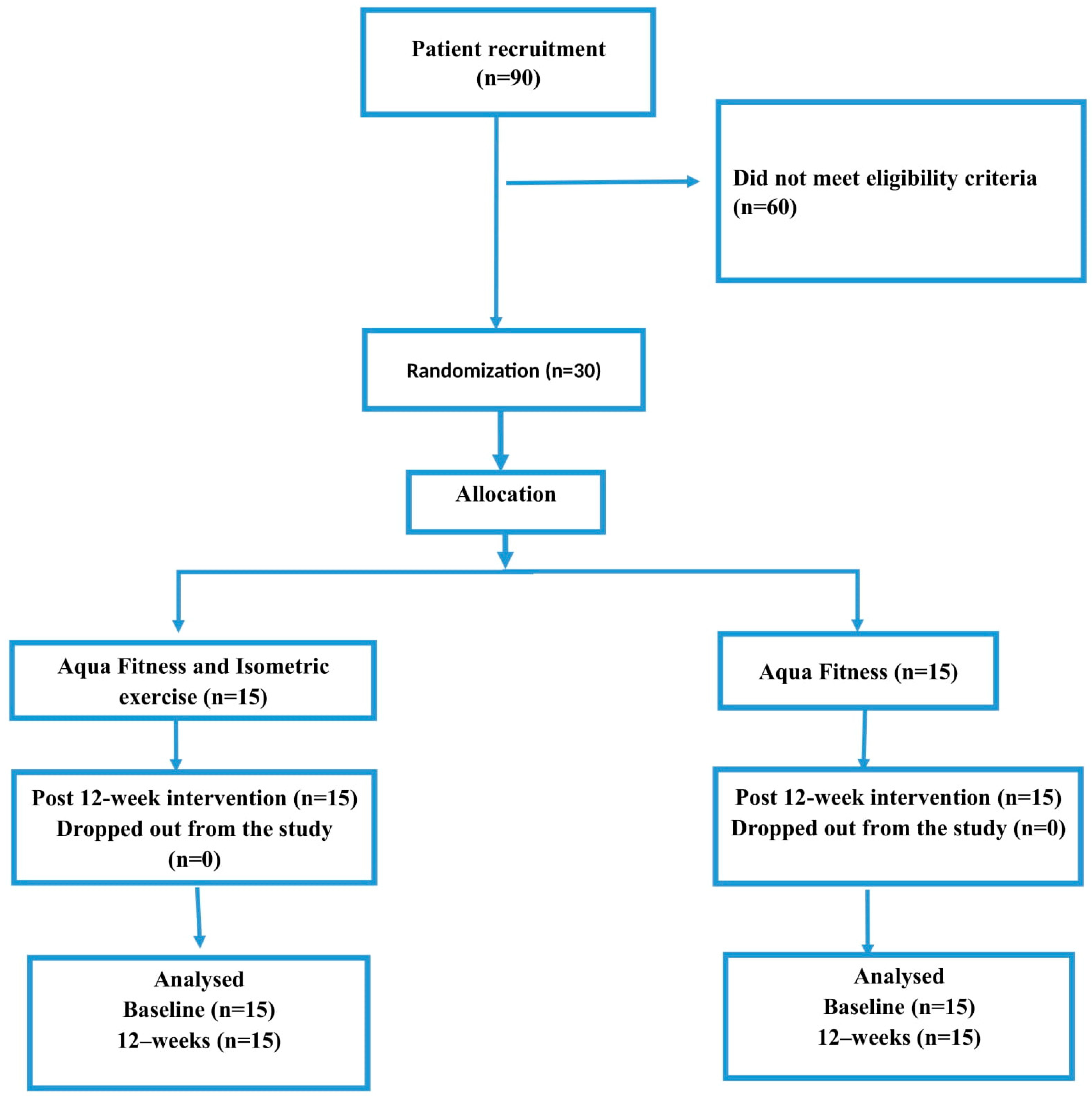
2.1. Study Design
2.1.1. Participants
2.1.2. Inclusion and Exclusion Criteria
2.2. Sample Size Estimate
2.3. Isometric Exercise Protocol
- Basic stance; one leg raised forward; “noodle (a foam float with a longitudinal shape)” held under the knee; bending and extending the leg at the hip joint.
- Basic stance; one leg raised forward; “noodle” held under the knee; abduction and adduction of the leg at the hip joint.
- Basic stance; right leg raised forward; “noodle” held under the knee; circling the leg at the hip joint.
- Straddle stance; arms bent forward; a gymnastic ball squeezed between the hands. Twists of the torso in the transverse plane.
- Straddle stance; arms bent forward; a gymnastic ball squeezed between the hands. Arm extensions and bends.
- Straddle stance; arms bent forward; a gymnastic ball squeezed between the hands. Circular movements of the arms down, forward, and bringing the arms back to the starting position.
- “Balance”; “betomic (a multifunctional tool for Aqua Fitness or rehabilitation)” squeezed between the knees. Hip twists to the right and left with alternating arm movements.
- “Balance”; “betomic” squeezed between the knees. Torso extension to lying on the back and return to the starting position.
- “Balance”; “betomic” squeezed between the knees. Torso extension to lying on the side and return to the starting position.
2.4. Procedure
- ➢
- The 30 s Chair Stand (30′CS) (standing up from a chair)—lower limb muscle strength; the patient repeats full stands from the sitting position. Repetitions are performed within 30 s with the arms crossed over the chest. The score is the number of completed chair stands in 30 s.
- ➢
- The Arm Curl Test (ACT) (forearm flexion)—upper limb muscle strength; the patient flexes the forearm in 30 s. The test is conducted on the dominant arm side (or stronger side). Curl the arm up through a full range of motion, gradually turning the palm up (flexion with supination). The score is the total number of controlled arm curls performed in 30 s.
- ➢
- Chair Sit and Reach (CS&R) (seated reach)—lower body flexibility; from a sitting position on a chair, the patient tries to reach the toes with the leg straight in the knee joint. The result in centimeters shows the distance between the fingers and the toes. The value can be negative when the patient is out of range of motion. The best score was recorded in centimeters.
- ➢
- Back Scratch (BS) (back scratch in standing)—upper body flexibility; the patient tries to join the hands behind the back, leading one hand from the top, and the other from the bottom. The result given in centimeters indicates the distance between the middle fingers. The value may be negative when the patient reaches further than the fingertips. The best score was recorded in centimeters. The higher the score the better the result.
- ➢
- Foot Up and Go (FU&G) (stand up and go)—dynamic balance and agility; the patient circles the cone in the shortest possible time at a distance of 2.44 m from the sitting starting position and returns to the starting position. The best time was recorded during two trials.
- ➢
- The 2 min Step in Place (2-SinP) (marching in place) test—endurance; the participant stands up straight next to the wall while a mark is placed on the wall at the level corresponding to midway between the patella (knee cap) and iliac crest (top of the hip bone). The participant then walks in place for two minutes, lifting the knees to the height of the mark on the wall. Resting is allowed, and holding onto the wall or a stable chair is allowed. Stop after two minutes of stepping. The total number of times the right knee reached the level of the bar in two minutes was recorded.
2.5. Statistical Analysis
3. Results
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rikli, R.E.; Edwards, D.J. Effects of a three-year exercise program on motor function and cognitive processing speed in older women. Res. Q. Exerc. Sport 1991, 62, 61–67. [Google Scholar] [CrossRef]
- King, A.C.; King, D.K. Physical activity for an aging population. Public Health Rev. 2010, 32, 401–426. [Google Scholar] [CrossRef]
- Figueira, H.A.; Figueira, O.A.; Corradi-Perini, C.; Martínez-Rodríguez, A.; Figueira, A.A.; da Silva, C.R.L.; Dantas, E.H.M. A descriptive analytical study on physical activity and quality of life in sustainable aging. Sustainability 2021, 13, 5968. [Google Scholar] [CrossRef]
- Peterson, M.J.; Giuliani, C.; Morey, M.C.; Pieper, C.F.; Evenson, K.R.; Mercer, V.; Cohen, H.J.; Visser, M.; Brach, J.S.; Kritchevsky, S.B. Physical activity as a preventative factor for frailty: The health, aging, and body composition study. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2009, 64, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Archer, E.; Paluch, A.E.; Shook, R.P.; Blair, S.N. Physical activity and the science of successful aging. Kinesiol. Rev. 2013, 2, 29–38. [Google Scholar] [CrossRef]
- Castelo-Branco, C.; Soveral, I. The immune system and aging: A review. Gynecol. Endocrinol. 2014, 30, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, P.; El-Jawhari, J.J.; Giannoudis, P.V.; Burska, A.N.; Ponchel, F.; Jones, E.A. Age-related changes in bone marrow mesenchymal stromal cells: A potential impact on osteoporosis and osteoarthritis development. Cell Transplant. 2017, 26, 1520–1529. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef]
- Dargatz, T.; Röwekamp, A. Aqua-Fitness: Aqua-Aerobic, Aqua-Power, Aqua-Jogging, Wassergymnastik; Stiebner Verlag GmbH: Munich, Germany, 2017. [Google Scholar]
- Holland, G.J.; Tanaka, K.; Shigematsu, R.; Nakagaichi, M. Flexibility and physical functions of older adults: A review. J. Aging Phys. Act. 2002, 10, 169–206. [Google Scholar] [CrossRef]
- Stathokostas, L.; Little, R.; Vandervoort, A.; Paterson, D.H. Flexibility training and functional ability in older adults: A systematic review. J. Aging Res. 2012, 2012, 306818. [Google Scholar] [CrossRef]
- Brach, J.S.; Perera, S.; Shuman, V.; Gil, A.B.; Kriska, A.; Nadkarni, N.K.; Rockette-Wagner, B.; Cham, R.; VanSwearingen, J.M. Effect of Timing and Coordination Training on Mobility and Physical Activity Among Community-Dwelling Older Adults: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2212921. [Google Scholar] [CrossRef]
- Van Abbema, R.; De Greef, M.; Crajé, C.; Krijnen, W.; Hobbelen, H.; Van Der Schans, C. What type, or combination of exercise can improve preferred gait speed in older adults? A meta-analysis. BMC Geriatr. 2015, 15, 72. [Google Scholar] [CrossRef]
- Cheng, S.-J.; Yang, Y.-R.; Cheng, F.-Y.; Chen, I.-H.; Wang, R.-Y. The changes of muscle strength and functional activities during aging in male and female populations. Int. J. Gerontol. 2014, 8, 197–202. [Google Scholar] [CrossRef]
- Dugan, S.A.; Gabriel, K.P.; Lange-Maia, B.S.; Karvonen-Gutierrez, C. Physical activity and physical function: Moving and aging. Obstet. Gynecol. Clin. 2018, 45, 723–736. [Google Scholar] [CrossRef]
- Jerome, G.J.; Glass, T.A.; Mielke, M.; Xue, Q.-L.; Andersen, R.E.; Fried, L.P. Physical activity participation by presence and type of functional deficits in older women: The Women’s Health and Aging Studies. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 1171–1176. [Google Scholar] [CrossRef]
- DiPietro, L. Physical activity in aging: Changes in patterns and their relationship to health and function. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.; Bellew, B.; Vita, P.; Brown, W.; Owen, N. Getting Australia Active: Towards Better Practice for the Promotion of Physical Activity; National Public Health Partnership: Melbourne, Australia, 2002.
- Andersen, L.B.; Schnohr, P.; Schroll, M.; Hein, H.O. All-cause mortality associated with physical activity during leisure time, work, sports, and cycling to work. Arch. Intern. Med. 2000, 160, 1621–1628. [Google Scholar] [CrossRef]
- Crespo, C.J.; Palmieri, M.R.G.; Perdomo, R.P.; Mcgee, D.L.; Smit, E.; Sempos, C.T.; Sorlie, P.D. The relationship of physical activity and body weight with all-cause mortality: Results from the Puerto Rico Heart Health Program. Ann. Epidemiol. 2002, 12, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.-M.; Skerrett, P.J. Physical activity and all-cause mortality: What is the dose-response relation? Med. Sci. Sports Exerc. 2001, 33, S459–S471. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Shaper, A.G.; Walker, M. Physical activity and mortality in older men with diagnosed coronary heart disease. Circulation 2000, 102, 1358–1363. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.M.; Stewart, A.L.; McLellan, B.Y.; Verboncoeur, C.J.; King, A.C.; Brown, B.W. Evaluation of enrollment bias in a physical-activity-promotion program for seniors. J. Aging Phys. Act. 2001, 9, 398–413. [Google Scholar] [CrossRef]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Leirós-Rodríguez, R.; Romo-Pérez, V.; Pérez-Ribao, I.; García-Soidán, J.L. A comparison of three physical activity programs for health and fitness tested with older women: Benefits of aerobic activity, aqua fitness, and strength training. J. Women Aging 2019, 31, 419–431. [Google Scholar] [CrossRef] [PubMed]
- Boguszewski, D.; Ogonowska, K.; Adamczyk, J.; Ochal, A.; Dudziak, D.; Białoszewski, D. Impact of aquafitness and gymnastics health exercises on the mental well-being of women after the age 60. J. Health Sci. 2013, 3, 193–200. [Google Scholar]
- Kovách, M.V.; Plachy, J.K.; Bognár, J.; Balogh, Z.O.; Barthalos, I. Effects of Pilates and aqua fitness training on older adults’ physical functioning and quality of life. Biomed. Hum. Kinet. 2013, 5, 22–27. [Google Scholar] [CrossRef]
- Waller, B.; Ogonowska-Słodownik, A.; Vitor, M.; Rodionova, K.; Lambeck, J.; Heinonen, A.; Daly, D. The effect of aquatic exercise on physical functioning in the older adult: A systematic review with meta-analysis. Age Ageing 2016, 45, 593–601. [Google Scholar] [CrossRef]
- Földesi, G.S. Life-styles and aging: The Hungarian case. Women Sport Phys. Act. J. 1998, 7, 171–190. [Google Scholar] [CrossRef]
- Achour, E.C.; Barthelemy, J.C.; Lionard, K.C.; Trombert, B.; Lacour, J.R.; Thomas-Anterion, C.; Gonthier, R.; Garet, M.; Roche, F. Level of physical activity at the age of 65 predicts successful aging seven years later: The PROOF study. Rejuvenation Res. 2011, 14, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Vieira, E.R.; Palmer, R.C.; Chaves, P.H. Prevention of falls in older people living in the community. BMJ 2016, 353, i1419. [Google Scholar] [CrossRef]
- Tomás, M.T.; Galán-Mercant, A.; Carnero, E.A.; Fernandes, B. Functional capacity and levels of physical activity in aging: A 3-year follow-up. Front. Med. 2018, 4, 244. [Google Scholar] [CrossRef]
- Chou, C.-H.; Hwang, C.-L.; Wu, Y.-T. Effect of exercise on physical function, daily living activities, and quality of life in the frail older adults: A meta-analysis. Arch. Phys. Med. Rehabil. 2012, 93, 237–244. [Google Scholar] [CrossRef]
- Naylor, L.H.; Maslen, B.A.; Cox, K.L.; Spence, A.L.; Robey, E.; Haynes, A.; Carter, H.H.; Lautenschlager, N.T.; Ridgers, N.D.; Pestell, C. Land-versus water-walking interventions in older adults: Effects on body composition. J. Sci. Med. Sport 2020, 23, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Prado, A.K.; Reichert, T.; Conceição, M.O.; Delevatti, R.S.; Kanitz, A.C.; Kruel, L.F. Effects of aquatic exercise on muscle strength in young and elderly adults: A systematic review and meta-analysis of randomized trials. J. Strength Cond. Res. 2022, 36, 1468–1483. [Google Scholar] [CrossRef]
- Clarke, L.H.; Bennett, E.V. Constructing the moral body: Self-care among older adults with multiple chronic conditions. Health 2013, 17, 211–228. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Status Report on Physical Activity 2022; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M.; American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Cole, A.J.; Becker, B.E. Comprehensive Aquatic Therapy; Butterworth-Heinemann: Oxford, UK, 2004. [Google Scholar]
- Smart, N.A.; Gow, J.; Bleile, B.; Van der Touw, T.; Pearson, M.J. An evidence-based analysis of managing hypertension with isometric resistance exercise—Are the guidelines current? Hypertens. Res. 2020, 43, 249–254. [Google Scholar] [CrossRef]
- Ogbutor, G.; Nwangwa, E.; Uyagu, D. Isometric handgrip exercise training attenuates blood pressure in prehypertensive subjects at 30% maximum voluntary contraction. Niger. J. Clin. Pract. 2019, 22, 1765–1771. [Google Scholar]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Jones, C.J.; Rikli, R.E. Measuring functional. J. Act. Aging 2002, 1, 24–30. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.M.; Goodpaster, B.H.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubin, S.M.; Harris, T.B. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Takeshima, N.; Rogers, M.E.; Watanabe, E.; Brechue, W.F.; Okada, A.; Yamada, T.; Islam, M.M.; Hayano, J. Water-based exercise improves health-related aspects of fitness in older women. Med. Sci. Sports Exerc. 2002, 34, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Association, A.E. Aquatic Fitness Professional Manual; Human Kinetics: Champaign, IL, USA, 2017. [Google Scholar]
- De Vries, N.; Van Ravensberg, C.; Hobbelen, J.; Rikkert, M.O.; Staal, J.; Nijhuis-Van der Sanden, M. Effects of physical exercise therapy on mobility, physical functioning, physical activity and quality of life in community-dwelling older adults with impaired mobility, physical disability and/or multi-morbidity: A meta-analysis. Ageing Res. Rev. 2012, 11, 136–149. [Google Scholar] [CrossRef]
- Guizelini, P.C.; de Aguiar, R.A.; Denadai, B.S.; Caputo, F.; Greco, C.C. Effect of resistance training on muscle strength and rate of force development in healthy older adults: A systematic review and meta-analysis. Exp. Gerontol. 2018, 102, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Moreland, J.D.; Richardson, J.A.; Goldsmith, C.H.; Clase, C.M. Muscle weakness and falls in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2004, 52, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Papalia, G.F.; Papalia, R.; Diaz Balzani, L.A.; Torre, G.; Zampogna, B.; Vasta, S.; Fossati, C.; Alifano, A.M.; Denaro, V. The effects of physical exercise on balance and prevention of falls in older people: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 2595. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Part of Classes | Contents | Duration |
|---|---|---|
| Introductory part | Greeting, checking attendance, and giving lesson assignments. Warming-up in the water. Choreography based on walking steps performed in different directions at a gradually increasing pace with gradually introduced arm work. | 10 min |
| Main part | Strengthening exercises: Strengthening exercises were based on basic Aqua Aerobic steps, such as the following:
| 40 min |
| Final part | Calming, stretching, and relaxing exercises at the edge of the pool. | 10 min |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Female gender | Previous surgeries in the last year |
| Age 60 years or older | Neurological deficits |
| Residence in or near Krakow | Cardiovascular diseases and pacemaker |
| No health contraindications to participate in aqua fitness classes, confirmed by a doctor | Cancers |
| Provided informed consent to undergo diagnostic tests and participate in the project | Trip to a sanatorium during the project |
| No injuries to the lower and upper limbs, or the last injury occurred more than 3 years before the start of the project | Scheduled surgery or hospitalization during the project |
| Regular participation in planned classes: 2 times a week for 12 weeks | Missing more than 20% of classes |
| Variables | Group | Pre-Test Evaluation a | Post-Test Evaluation a | Within-Group Differences (Paired t-Test) | Between-Group Differences at Baseline (Independent t-Test) | |
|---|---|---|---|---|---|---|
| ES | (p-Value) | p | ||||
| 30CS [lp] | exp | 15.26 ± 2.15 | 16.46 ± 1.76 | 0.61 | (0.001) * | 0.45 |
| con | 13.73 ± 2.57 | 14.41 ± 3.86 | 0.29 | (0.19) | ||
| ACT [lp] | exp | 17.33 ± 3.41 | 20.20 ± 3.44 | 0.84 | (0.002) * | 0.61 |
| con | 16.26 ± 3.08 | 18.60 ± 2.69 | 0.81 | (0.004) * | ||
| CS&R Right [cm] | exp | 8.23 ± 10.21 | 12.66 ± 8.51 | 0.47 | (0.03) * | 0.17 |
| con | −0.30 ± 16.62 | 6.43 ± 12.51 | 0.46 | (0.016) * | ||
| CS&R Right [cm] | exp | 7.63 ± 10.43 | 13.90 ± 9.43 | 0.63 | (0.010) * | 0.078 |
| con | −1.66 ± 16.0 | 10.55 ± 11.23 | 0.88 | (0.004) * | ||
| BC Right [cm] | exp | 0.66 ± 7.78 | 1.00 ± 7.55 | 0.75 | (0.043) * | 0.088 |
| con | 5.28 ± 11.69 | −3.03 ± 9.71 | 0.21 | (0.094) | ||
| BC Left [cm] | exp | −3.63 ± 5.50 | −3.20 ± 6.43 | 0.88 | (0.54) | 0.10 |
| con | −10.30 ± 10.42 | −8.66 ± 10.42 | 0.27 | (0.15) | ||
| FU&G [s] | exp | 4.89 ± 0.66 | 4.59 ± 0.71 | 0.44 | (0.002) * | 0.58 |
| con | 5.11 ± 0.72 | 5.44 ± 0.74 | 0.45 | (0.10) | ||
| 2-sinP [lp] | exp | 108.40 ± 10.22 | 118.86 ± 6.22 | 1.27 | (0.008) * | 0.43 |
| con | 101.46 ± 16.40 | 113.80 ± 13.32 | 0.83 | (0.001) * | ||
| Variables | Between-Group Differences (Repeated-Measures ANOVA) | |||||||
|---|---|---|---|---|---|---|---|---|
| Time | Time * Group | Group | ||||||
| p | ES | Mean Difference (%0.95 CI) | p | ES | p | ES | Mean Difference (%0.95 CI) | |
| 30′CS [lp] | 0.009 * | 0.22 | −1.06 (−1.83 to −0.29) | 0.72 | 0.004 | 0.079 | 0.10 | 1.66 (−0.20 to 3.54) |
| ACT [lp] | 0.001 * | 0.46 | −2.60 (−3.67 to −1.52) | 0.61 | 0.009 | 0.20 | 0.056 | 1.33 (−0.78 to 3.44) |
| CS&R Right [cm] | 0.001 * | 0.32 | −5.58 (−8.72 to −2.44) | 0.45 | 0.020 | 0.093 | 0.098 | 7.38 (−1.30 to 16.07) |
| CS&R Right [cm] | 0.001 * | 0.44 | −7.56 (−10.81 to −4.31) | 0.41 | 0.23 | 0.067 | 0.11 | 8.00 (−0.58 to 16.58) |
| BC Right [cm] | 0.12 | 0.083 | −1.29 (−2.94 to 0.36) | 0.24 | 0.048 | 0.14 | 0.075 | 4.99 (−1.79 to 11.77) |
| BC Left [cm] | 0.20 | 0.05 | −1.03 (−2.68 to 0.61) | 0.56 | 0.46 | 0.059 | 0.12 | 6.07 (−0.26 to 12.40) |
| FU&G [s] | 0.86 | 0.001 | 0.005 * | 0.25 | 0.032 * | 0.15 | −0.53 (−1.02 to −0.05) | |
| 2-sinP [lp] | 0.001 * | 0.61 | −11.40 (−14.92 to −7.87) | 0.59 | 0.010 | 0.15 | 0.071 | 6 (−2.37 to 14.37) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kucia, K.; Koteja, A.; Rydzik, Ł.; Javdaneh, N.; Shams, A.; Ambroży, T. The Impact of a 12-Week Aqua Fitness Program on the Physical Fitness of Women over 60 Years of Age. Sports 2024, 12, 105. https://doi.org/10.3390/sports12040105
Kucia K, Koteja A, Rydzik Ł, Javdaneh N, Shams A, Ambroży T. The Impact of a 12-Week Aqua Fitness Program on the Physical Fitness of Women over 60 Years of Age. Sports. 2024; 12(4):105. https://doi.org/10.3390/sports12040105
Chicago/Turabian StyleKucia, Katarzyna, Agnieszka Koteja, Łukasz Rydzik, Norollah Javdaneh, Arash Shams, and Tadeusz Ambroży. 2024. "The Impact of a 12-Week Aqua Fitness Program on the Physical Fitness of Women over 60 Years of Age" Sports 12, no. 4: 105. https://doi.org/10.3390/sports12040105