
Assessment of the Physical Activity of Children with Asthma Bronchiale


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Data Analysis
3. Results
3.1. Socio-Economic Factors Influencing Sports Behavior
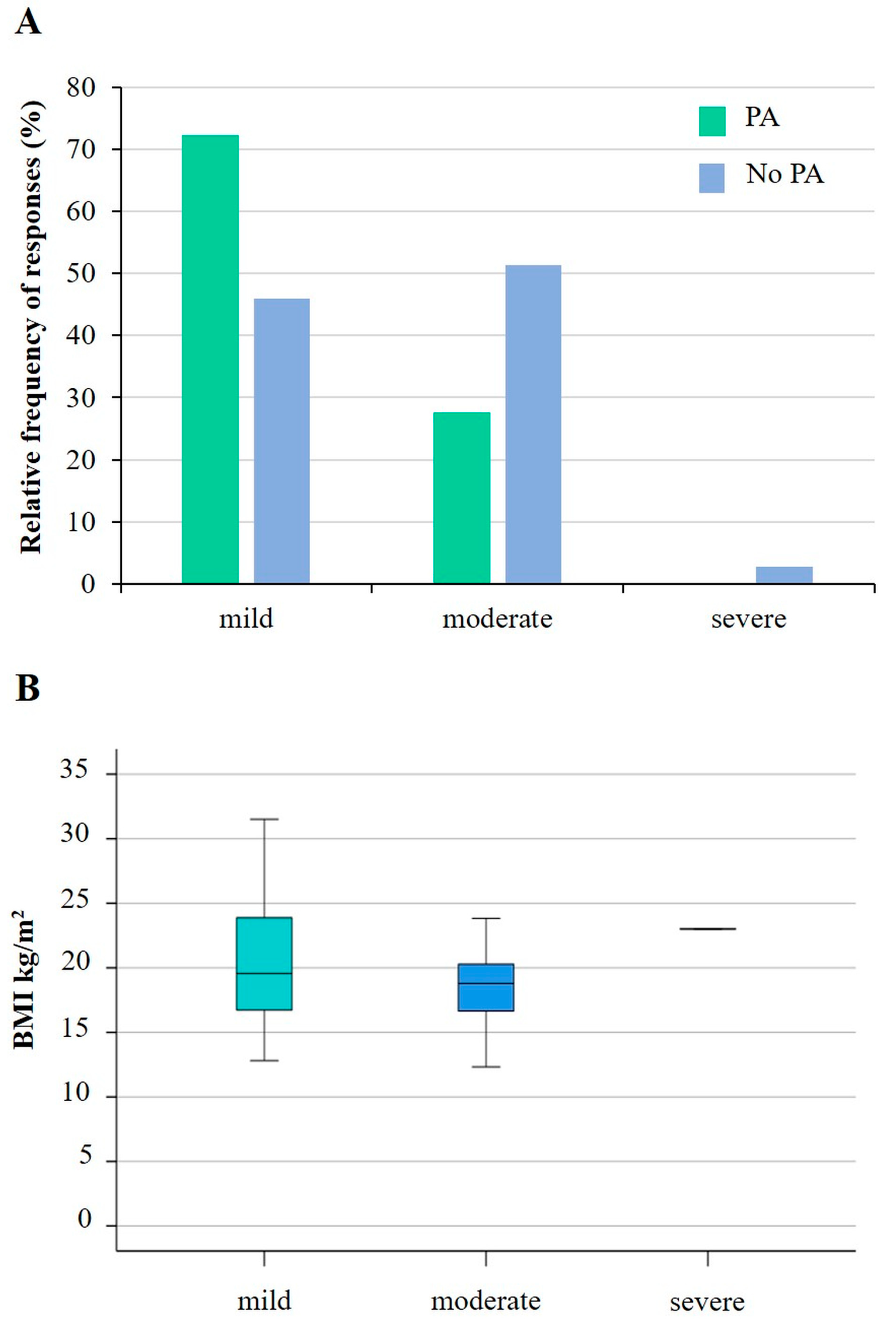
3.2. Physical and Health Status of Participating Children
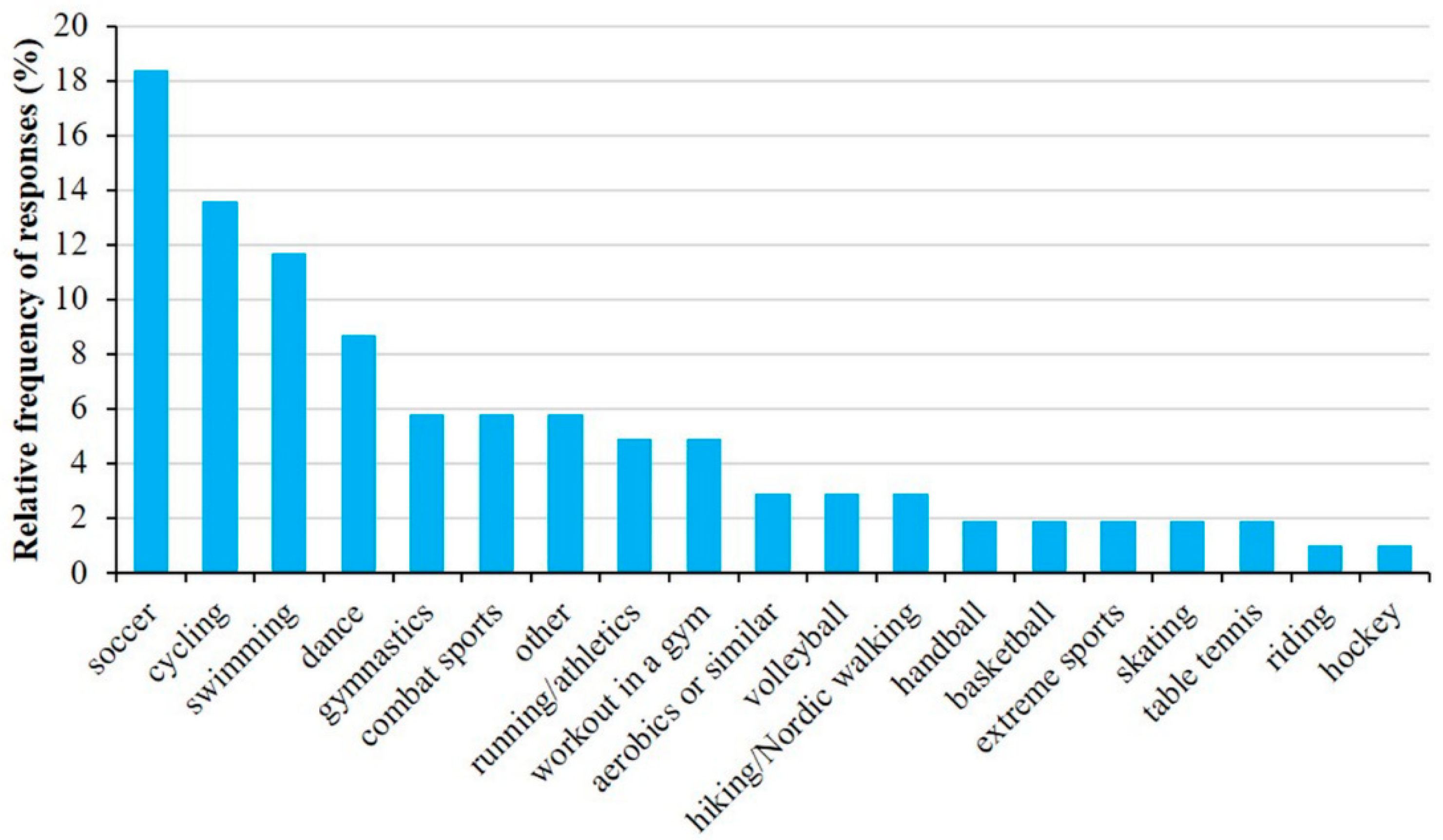
3.3. Sporting Habits of Children with Asthma
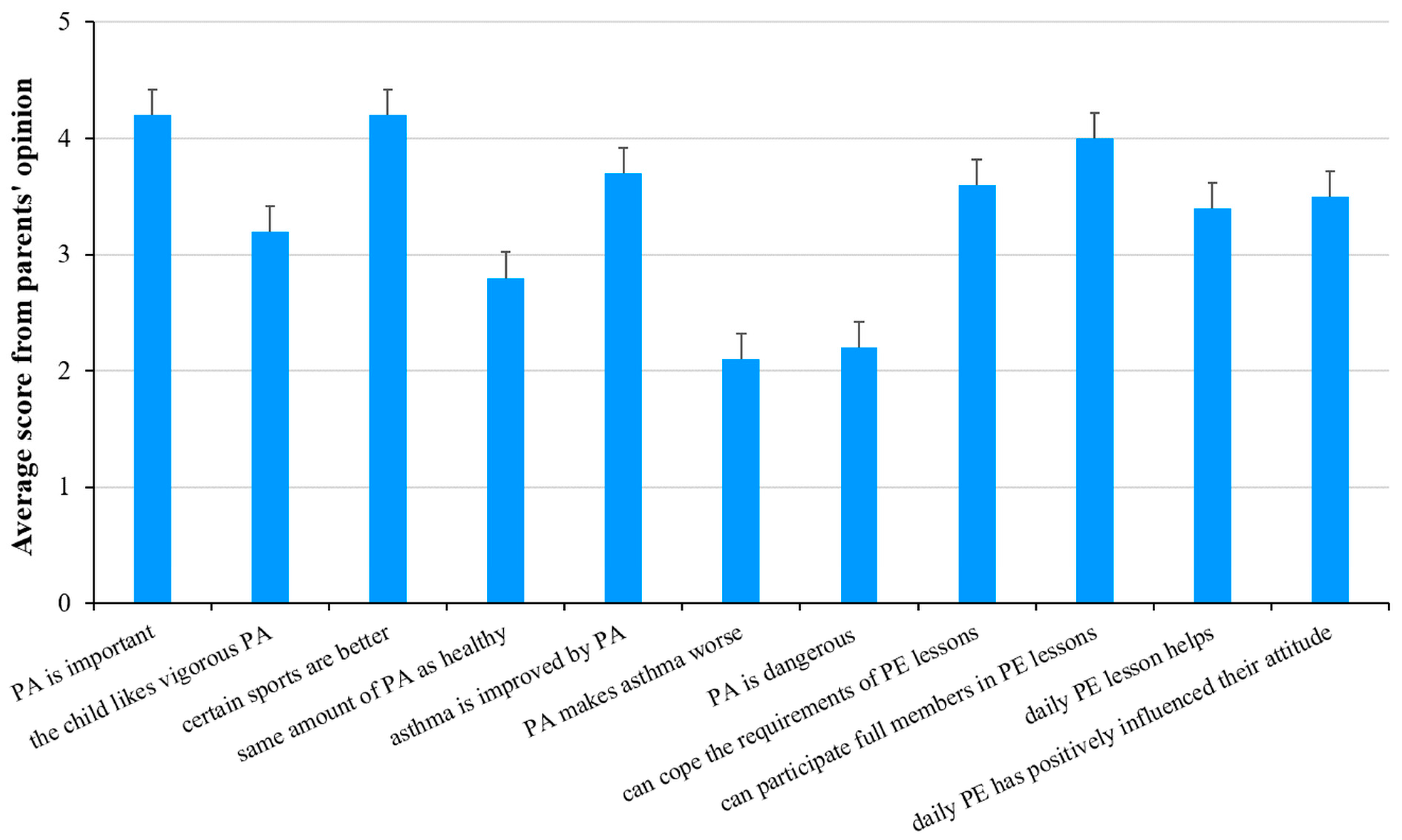
3.4. Parents’ Opinion on the Physical Activity of Their Children
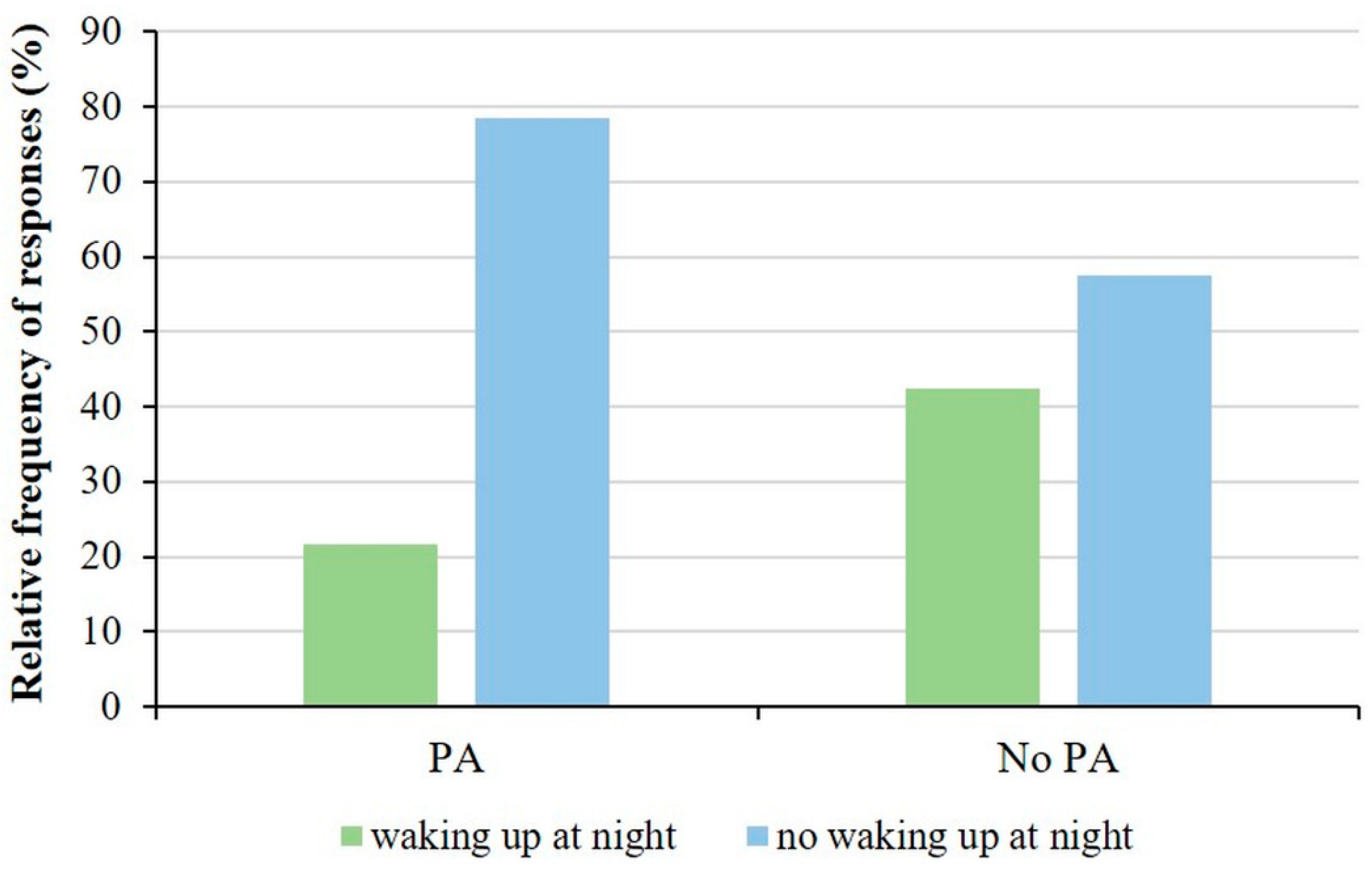
3.5. Impact of Illness on Children’s Quality of Life
3.6. Sex-Based Analysis of Physical Activity of Children with Asthma
3.7. Results of Follow-Up Examinations
4. Discussion
4.1. General Findings
4.2. Physical Activity
4.3. Parental Attitudes
4.4. Quality of Life and Physical Activity
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diseases, G.B.D.; Injuries, C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Molnar, D.; Galffy, G.; Horvath, A.; Tomisa, G.; Katona, G.; Hirschberg, A.; Mezei, G.; Sultesz, M. Prevalence of Asthma and Its Associating Environmental Factors among 6-12-Year-Old Schoolchildren in a Metropolitan Environment-A Cross-Sectional, Questionnaire-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 13403. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A. Subjective measures of well-being. Am. Psychol. 1976, 31, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Andrews, F.M.; Inglehart, R. The structure of subjective well-being in nine western societies. Social Indic. Res. 1979, 6, 73–90. [Google Scholar] [CrossRef]
- Mészáros, Á. Life Quality Measurement in Asthma Bronchial [Életminőség-mérés asthma bronchialéban]. LAM 2006, 16, 353–359. [Google Scholar]
- Müller, A.; Balatoni, I.; Csernoch, L.; Bacs, Z.; Biro, M.; Bendikova, E.; Pesti, A.; Bacsne Baba, E. Quality of life of asthmatic patients after complex rehabilitation treatment. Orv. Hetil. 2018, 159, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- le Coq, E.M.; Colland, V.T.; Boeke, A.J.; Boeke, P.; Bezemer, D.P.; van Eijk, J.T. Reproducibility, construct validity, and responsiveness of the “How Are You?” (HAY), a self-report quality of life questionnaire for children with asthma. J. Asthma 2000, 37, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Bousema, S.; Bohnen, A.M.; Bindels, P.J.E.; Elshout, G. A systematic review of questionnaires measuring asthma control in children in a primary care population. NPJ Prim. Care Respir. Med. 2023, 33, 25. [Google Scholar] [CrossRef] [PubMed]
- Juniper, E.F.; Gruffydd-Jones, K.; Ward, S.; Svensson, K. Asthma Control Questionnaire in children: Validation, measurement properties, interpretation. Eur. Respir. J. 2010, 36, 1410–1416. [Google Scholar] [CrossRef]
- Szabó, A. Asztmás Gyermekek és Szüleik Életminősége és Pszichés Állapota; Semmelweis Egyetem: Budapest, Hungary, 2009. [Google Scholar]
- Wanrooij, V.H.; Willeboordse, M.; Dompeling, E.; van de Kant, K.D. Exercise training in children with asthma: A systematic review. Br. J. Sports Med. 2014, 48, 1024–1031. [Google Scholar] [CrossRef]
- Kitsantas, A.; Zimmerman, B.J. Self-efficacy, activity participation, and physical fitness of asthmatic and nonasthmatic adolescent girls. J. Asthma 2000, 37, 163–174. [Google Scholar] [CrossRef] [PubMed]
- van Veldhoven, N.H.; Vermeer, A.; Bogaard, J.M.; Hessels, M.G.; Wijnroks, L.; Colland, V.T.; van Essen-Zandvliet, E.E. Children with asthma and physical exercise: Effects of an exercise programme. Clin. Rehabil. 2001, 15, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Lucas, S.R.; Platts-Mills, T.A. Physical activity and exercise in asthma: Relevance to etiology and treatment. J. Allergy Clin. Immunol. 2005, 115, 928–934. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.E.; Merkle, S.L.; Fulton, J.E.; Wheeler, L.S.; Mannino, D.M. Relationship between asthma, overweight, and physical activity among U.S. high school students. J. Community Health 2006, 31, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Welsh, L.; Roberts, R.G.; Kemp, J.G. Fitness and physical activity in children with asthma. Sports Med. 2004, 34, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Powell, A.; Hoskins, G.; Neville, R. Exploring and explaining low participation in physical activity among children and young people with asthma: A review. BMC Fam. Pract. 2008, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, F.; Lambrechtsen, J.; Siersted, H.C.; Hansen, H.S.; Hansen, N.C. Low physical fitness in childhood is associated with the development of asthma in young adulthood: The Odense schoolchild study. Eur. Respir. J. 2000, 16, 866–870. [Google Scholar] [CrossRef] [PubMed]
- Hind, K.; Burrows, M. Weight-bearing exercise and bone mineral accrual in children and adolescents: A review of controlled trials. Bone 2007, 40, 14–27. [Google Scholar] [CrossRef]
- Eijkemans, M.; Mommers, M.; Draaisma, J.M.; Thijs, C.; Prins, M.H. Physical activity and asthma: A systematic review and meta-analysis. PLoS ONE 2012, 7, e50775. [Google Scholar] [CrossRef]
- Malmberg, M.; Malmberg, L.P.; Pelkonen, A.S.; Makela, M.J.; Kotaniemi-Syrjanen, A. Overweight and exercise-induced bronchoconstriction—Is there a link? Pediatr. Allergy Immunol. 2021, 32, 992–998. [Google Scholar] [CrossRef]
- Groth, S.W.; Rhee, H.; Kitzman, H. Relationships among obesity, physical activity and sedentary behavior in young adolescents with and without lifetime asthma. J. Asthma 2016, 53, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Magnus, M.C.; Stigum, H.; Haberg, S.E.; Nafstad, P.; London, S.J.; Nystad, W. Peak weight and height velocity to age 36 months and asthma development: The Norwegian Mother and Child Cohort Study. PLoS ONE 2015, 10, e0116362. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Heath, G.; Nagakumar, P.; Pattison, H.; Farrow, C. Parental Feeding, Child Eating and Physical Activity: Differences in Children Living with and without Asthma. Int. J. Environ. Res. Public Health 2021, 18, 3452. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.; Jia, Y.; Zhao, B.; Chen, O. The Barriers to Shared Decision-making in Exercise Prescription for Children with Asthma: A Qualitative Study from Parents’ Perspective. J. Pediatr. Health Care 2024. [Google Scholar] [CrossRef]
- Cao, C.; Wang, Y.; Peng, L.; Wu, W.; Yang, H.; Li, Z. Asthma and Other Respiratory Diseases of Children in Relation to Personal Behavior, Household, Parental and Environmental Factors in West China. Toxics 2023, 11, 964. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; Wen, D.; Li, S.; Duan, X.; Zhang, Y.; Gong, J.; Guo, Q.; Xu, X.; Qin, N.; Meng, X.; et al. Changes in children’s asthma prevalence over two decades in Lanzhou: Effects of socioeconomic, parental and household factors. J. Thorac. Dis. 2020, 12, 6365–6378. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Heath, G.; Nagakumar, P.; Farrow, C. Influence of parental anxiety and beliefs about medicines on feeding and exercise in children living with asthma. J. Child. Health Care 2023. [Google Scholar] [CrossRef]
- Mitchell, D.K.; Kopel, S.J.; Esteban, C.A.; Seifer, R.; Vehse, N.W.; Chau, S.; Jelalian, E. Asthma Status and Physical Activity in Urban Children. Am. J. Resp. Crit. Care 2017, 195, A2993. [Google Scholar]
- Hungarian Central Statistical Office. 2023. Available online: https://www.ksh.hu/docs/hun/xftp/megy/233/index.html (accessed on 8 March 2024).
- Acs, P.; Betlehem, J.; Olah, A.; Bergier, J.; Melczer, C.; Premusz, V.; Makai, A. Measurement of public health benefits of physical activity: Validity and reliability study of the international physical activity questionnaire in Hungary. BMC Public Health 2020, 20, 1198. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Balatoni, I.; Szépné Varga, H.; Müller, A.; Kovács, S.; Kosztin, N. Sporting habits of university students in Hungary. Balt. J. Health Phys. Act. 2019, 11, 27–37. [Google Scholar] [CrossRef]
- Szépné Varga, H.; Csernoch, L.; Balatoni, I. E-sports versus physical activity among adolescents. Balt. J. Health Phys. Act. 2019, 11, 38–47. [Google Scholar] [CrossRef]
- Juniper, E.F.; Guyatt, G.H.; Feeny, D.H.; Ferrie, P.J.; Griffith, L.E.; Townsend, M. Measuring quality of life in children with asthma. Qual. Life Res. 1996, 5, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Miadich, S.A.; Everhart, R.S.; Borschuk, A.P.; Winter, M.A.; Fiese, B.H. Quality of Life in Children with Asthma: A Developmental Perspective. J. Pediatr. Psychol. 2015, 40, 672–679. [Google Scholar] [CrossRef]
- Schatz, M.; Sorkness, C.A.; Li, J.T.; Marcus, P.; Murray, J.J.; Nathan, R.A.; Kosinski, M.; Pendergraft, T.B.; Jhingran, P. Asthma Control Test: Reliability, validity, and responsiveness in patients not previously followed by asthma specialists. J. Allergy Clin. Immunol. 2006, 117, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.D.; Theurer, W.M. A stepwise approach to the interpretation of pulmonary function tests. Am. Fam. Physician 2014, 89, 359–366. [Google Scholar] [PubMed]
- Szépné Varga, H.; Balatoni, I. Exploring the background conditions for playing sports of pre-school children. Tér—Gazdaság—Ember 2018, 6, 119–135. [Google Scholar]
- Balatoni, I.; Szépné Varga, H.; Csernoch, L. Free Time Activities of High School Students: Sports or Video Games? Athens J. Sports 2020, 7, 141–154. [Google Scholar] [CrossRef]
- Aggarwal, B.; Mulgirigama, A.; Berend, N. Exercise-induced bronchoconstriction: Prevalence, pathophysiology, patient impact, diagnosis and management. NPJ Prim. Care Respir. Med. 2018, 28, 31. [Google Scholar] [CrossRef]
- Endre, L. Physical exercise and bronchial asthma. Orv. Hetil. 2016, 157, 1019–1027. [Google Scholar] [CrossRef]
- Hollmann, W. Exercise, training and sports in children with asthma from the sports medicine viewpoint. Monatsschr Kinderheilkd. 1985, 133, 863–867. [Google Scholar] [PubMed]
- Kemper, P. Asthma and sport—risk and chance. Pneumologie 2008, 62, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Pianosi, P.T.; Davis, H.S. Determinants of physical fitness in children with asthma. Pediatrics 2004, 113, e225–e229. [Google Scholar] [CrossRef] [PubMed]
- Todaro, A. Physical activities and sports in asthmatic patients. Minerva Med. 1983, 74, 1349–1356. [Google Scholar] [PubMed]
- van Gent, R.; van der Ent, C.K.; van Essen-Zandvliet, L.E.; Rovers, M.M.; Kimpen, J.L.; de Meer, G.; Klijn, P.H. No differences in physical activity in (un)diagnosed asthma and healthy controls. Pediatr. Pulmonol. 2007, 42, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.D.; Forno, E. Exercise and lifestyle changes in pediatric asthma. Curr. Opin. Pulm. Med. 2020, 26, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Nyenhuis, S.M.; Kahwash, B.; Cooke, A.; Gregory, K.L.; Greiwe, J.; Nanda, A. Recommendations for Physical Activity in Asthma: A Work Group Report of the AAAAI Sports, Exercise, and Fitness Committee. J. Allergy Clin. Immunol. Pract. 2022, 10, 433–443. [Google Scholar] [CrossRef] [PubMed]
- West, S.L.; Banks, L.; Schneiderman, J.E.; Caterini, J.E.; Stephens, S.; White, G.; Dogra, S.; Wells, G.D. Physical activity for children with chronic disease; a narrative review and practical applications. BMC Pediatr. 2019, 19, 12. [Google Scholar] [CrossRef]
- Milanese, M.; Miraglia Del Giudice, E.; Peroni, D.G. Asthma, exercise and metabolic dysregulation in paediatrics. Allergol. Immunopathol. 2019, 47, 289–294. [Google Scholar] [CrossRef]
- Papamichael, M.M.; Katsardis, C.; Tsoukalas, D.; Erbas, B.; Itsiopoulos, C. Weight Status and Respiratory Health in Asthmatic Children. Lung 2019, 197, 777–782. [Google Scholar] [CrossRef]
- Story, R.E. Asthma and obesity in children. Curr. Opin. Pediatr. 2007, 19, 680–684. [Google Scholar] [CrossRef] [PubMed]
- Peroni, D.G.; Pietrobelli, A.; Boner, A.L. Asthma and obesity in childhood: On the road ahead. Int. J. Obes. 2010, 34, 599–605. [Google Scholar] [CrossRef]
- Winn, C.O.N.; Mackintosh, K.A.; Eddolls, W.T.B.; Stratton, G.; Wilson, A.M.; Davies, G.A.; McNarry, M.A. Asthma, body mass and aerobic fitness, the relationship in adolescents: The exercise for asthma with commando Joe’s(R) (X4ACJ) trial. J. Sports Sci. 2020, 38, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, K.A.; McNarry, M.A.; Berntsen, S.; Steele, J.; Sejersted, E.; Westergren, T. Physical activity and sedentary time in children and adolescents with asthma: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2021, 31, 1183–1195. [Google Scholar] [CrossRef]
- Winn, C.O.N.; Mackintosh, K.A.; Eddolls, W.T.B.; Stratton, G.; Wilson, A.M.; Rance, J.Y.; Doull, I.J.M.; McNarry, M.A.; Davies, G.A. Perceptions of asthma and exercise in adolescents with and without asthma. J. Asthma 2018, 55, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Pike, K.C.; Griffiths, L.J.; Dezateux, C.; Pearce, A. Physical activity among children with asthma: Cross-sectional analysis in the UK millennium cohort. Pediatr. Pulmonol. 2019, 54, 962–969. [Google Scholar] [CrossRef]
- Lam, K.M.; Yang, Y.H.; Wang, L.C.; Chen, S.Y.; Gau, B.S.; Chiang, B.L. Physical Activity in School-Aged Children with Asthma in an Urban City of Taiwan. Pediatr. Neonatol. 2016, 57, 333–337. [Google Scholar] [CrossRef]
- Beets, M.W.; Cardinal, B.J.; Alderman, B.L. Parental social support and the physical activity-related behaviors of youth: A review. Health Educ. Behav. 2010, 37, 621–644. [Google Scholar] [CrossRef]
- de Moraes, A.C.; Guerra, P.H.; Menezes, P.R. The worldwide prevalence of insufficient physical activity in adolescents; a systematic review. Nutr. Hosp. 2013, 28, 575–584. [Google Scholar] [CrossRef]
- Rogulj, M.V.K.; Lusic Kalcina, L. A Closer Look at Parental Anxiety in Asthma Outpacing Children’s Concerns: Fear of Physical Activity over the Fear of Drug Side Effects. Children 2024, 11, 289. [Google Scholar] [CrossRef]
- Meltzer, L.J.; Beebe, D.W.; Jump, S.; Flewelling, K.; Sundstrom, D.; White, M.; Zeitlin, P.L.; Strand, M.J. Impact of sleep opportunity on asthma outcomes in adolescents. Sleep Med. 2020, 65, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Nnodum, B.N.; McCormack, M.C.; Putcha, N.; Hwang, S.; Paulin, L.M.; Brigham, E.P.; Fawzy, A.; Romero, K.; Diette, G.B.; Hansel, N.N. Impact of Physical Activity on Reporting of Childhood Asthma Symptoms. Lung 2017, 195, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Peftoulidou, P.; Gioulvanidou, M.; Chrysochoou, E.A.; Hatziagorou, E. Physical activity and quality of life in children with well-controlled asthma. J. Asthma 2023, 60, 1031–1037. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statement | Mean (SD) | p-Value a | |
|---|---|---|---|
| Physically Active Children | Physically Inactive Children | ||
| Physical activity is important for asthmatic children. | 4.44 (0.80) | 3.87 (1.08) | 0.006 |
| The child likes vigorous physical activity. | 3.63 (1.28) | 2.56 (1.05) | <0.001 |
| Certain sports are better for children with asthma. | 4.33 (0.84) | 4.00 (0.92) | 0.062 |
| Children with asthma can do the same amount of physical activity as their non-asthmatic peers. | 2.98 (1.38) | 2.44 (1.17) | 0.071 |
| Asthma is improved by physical activity. | 3.87 (1.07) | 3.33 (1.20) | 0.033 |
| Physical activity makes asthma worse. | 1.98 (1.09) | 2.35 (1.19) | 0.139 |
| Physical activity is dangerous for children with asthma. | 2.06 (1.02) | 2.46 (1.27) | 0.160 |
| My child feels that he/she can cope the requirements of PE lessons. | 3.98 (1.53) | 3.08 (1.42) | 0.002 |
| My child feels that he/she can participate fully in group sports activities in PE lessons. | 4.45 (1.10) | 3.49 (1.30) | <0.001 |
| My child’s health has been improved by the introduction of daily physical education. | 3.63 (1.25) | 2.95 (1.26) | 0.010 |
| My child’s attitude to physical activity has been positively influenced by the introduction of daily PE. | 3.87 (1.30) | 3.05 (1.30) | 0.002 |
| Type | Girls (%) | Boys (%) | p-Value a |
|---|---|---|---|
| Dance | 25 | 3.1 | 0.001 |
| Gymnastics | 10.7 | 4.6 | 0.272 |
| Swimming | 10.7 | 13.8 | 0.679 |
| Aerobics or similar | 7.1 | 1.5 | 0.161 |
| Soccer | 7.1 | 26.2 | 0.037 |
| Handball | 7.1 | 0 | 0.029 |
| Volleyball | 7.1 | 1.5 | 0.161 |
| Running/Athletics | 3.6 | 6.2 | 0.613 |
| Cycling | 3.6 | 20 | 0.042 |
| Riding | 3.6 | 0 | 0.126 |
| Skating | 3.6 | 1.5 | 0.535 |
| Other | 3.6 | 7.7 | 0.458 |
| Workout in a gym | 0 | 7.7 | 0.131 |
| Basketball | 0 | 3.1 | 0.348 |
| Hiking/Nordic walking | 0 | 4.6 | 0.248 |
| Combat sports | 0 | 9.2 | 0.096 |
| Extreme sports | 0 | 3.1 | 0.348 |
| Hockey | 0 | 1.5 | 0.509 |
| Table tennis | 0 | 3.1 | 0.348 |
| Statement | Mean (SD) | p-Value a | |
|---|---|---|---|
| Girls | Boys | ||
| Physical activity is important for asthmatic children. | 4.22 (0.97) | 4.18 (0.97) | 0.864 |
| The child likes vigorous physical activity. | 2.81 (1.33) | 3.34 (1.25) | 0.091 |
| Certain sports are better for children with asthma. | 4.11 (0.89) | 4.20 (0.89) | 0.592 |
| Children with asthma can do the same amount of physical activity as their non-asthmatic peers. | 2.33 (1.39) | 2.94 (1.25) | 0.023 |
| Asthma is improved by physical activity. | 3.32 (1.16) | 3.80 (1.13) | 0.053 |
| Physical activity makes asthma worse. | 2.32 (1.09) | 2.05 (1.17) | 0.250 |
| Physical activity is dangerous for children with asthma. | 2.68 (1.25) | 2.05 (1.05) | 0.020 |
| My child feels can cope the requirements of PE lessons. | 3.36 (1.55) | 3.70 (1.54) | 0.225 |
| My child feels that he/she can participate fully in group sports activities in PE lessons. | 3.74 (1.46) | 4.17 (1.18) | 0.177 |
| My child’s health has been improved by the introduction of daily physical education. | 2.93 (1.30) | 3.54 (1.26) | 0.042 |
| My child’s attitude to physical activity has been positively influenced by the introduction of daily PE. | 3.29 (1.41) | 3.63 (1.33) | 0.257 |
| Variables | Mean (SD) | t-Value | p-Value a | ||
|---|---|---|---|---|---|
| 2019 | 2023 | ||||
| BMI | (kg/m2) | 18.46 (3.95) | 21.94 (4.14) | −3.752 | 0.002 |
| VC | (L) | 2.81 (1.16) | 3.21 (1.18) | −2.268 | 0.039 |
| (%) | 88.66 (16.43) | 93.91 (20.29) | −1.117 | 0.282 | |
| FEV1 | (L) | 2.39 (0.99) | 2.72 (0.99) | −2.246 | 0.040 |
| (%) | 87.69 (13.20) | 88.59 (19.84) | −0.208 | 0.838 | |
| FEF25-75 | (L/s) | 3.21 (1.12) | 3.55 (1.19) | −2.400 | 0.030 |
| (%) | 76.82 (18.82) | 74.56 (22.18) | 0.549 | 0.591 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balatoni, I.; Kiss, T.; Balla, G.; Papp, Á.; Csernoch, L. Assessment of the Physical Activity of Children with Asthma Bronchiale. Sports 2024, 12, 114. https://doi.org/10.3390/sports12040114
Balatoni I, Kiss T, Balla G, Papp Á, Csernoch L. Assessment of the Physical Activity of Children with Asthma Bronchiale. Sports. 2024; 12(4):114. https://doi.org/10.3390/sports12040114
Chicago/Turabian StyleBalatoni, Ildikó, Tímea Kiss, György Balla, Ágnes Papp, and László Csernoch. 2024. "Assessment of the Physical Activity of Children with Asthma Bronchiale" Sports 12, no. 4: 114. https://doi.org/10.3390/sports12040114
APA StyleBalatoni, I., Kiss, T., Balla, G., Papp, Á., & Csernoch, L. (2024). Assessment of the Physical Activity of Children with Asthma Bronchiale. Sports, 12(4), 114. https://doi.org/10.3390/sports12040114