
Analysis of Injuries in the Swiss U20 Elite Ice Hockey Season 2019/2020—A Retrospective Survey



Abstract
:1. Introduction
Aim
2. Materials and Methods
2.1. Design
2.2. Recruitment of the Participants
2.3. In- and Exclusion Criteria
2.4. Definitions
2.5. Data Extraction
2.6. Statistics
3. Results
3.1. Participants’ Characteristics
3.2. Injury Data
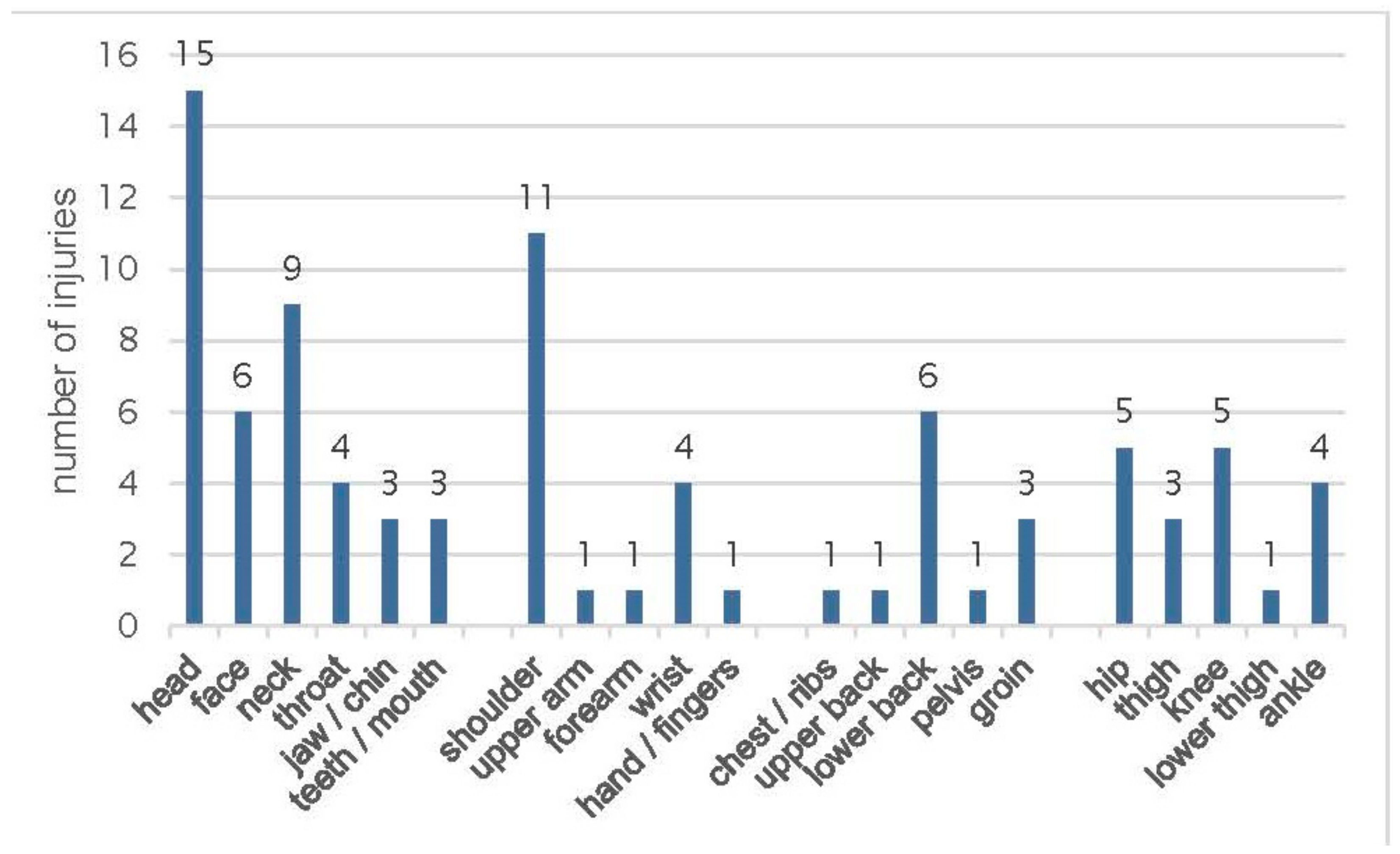
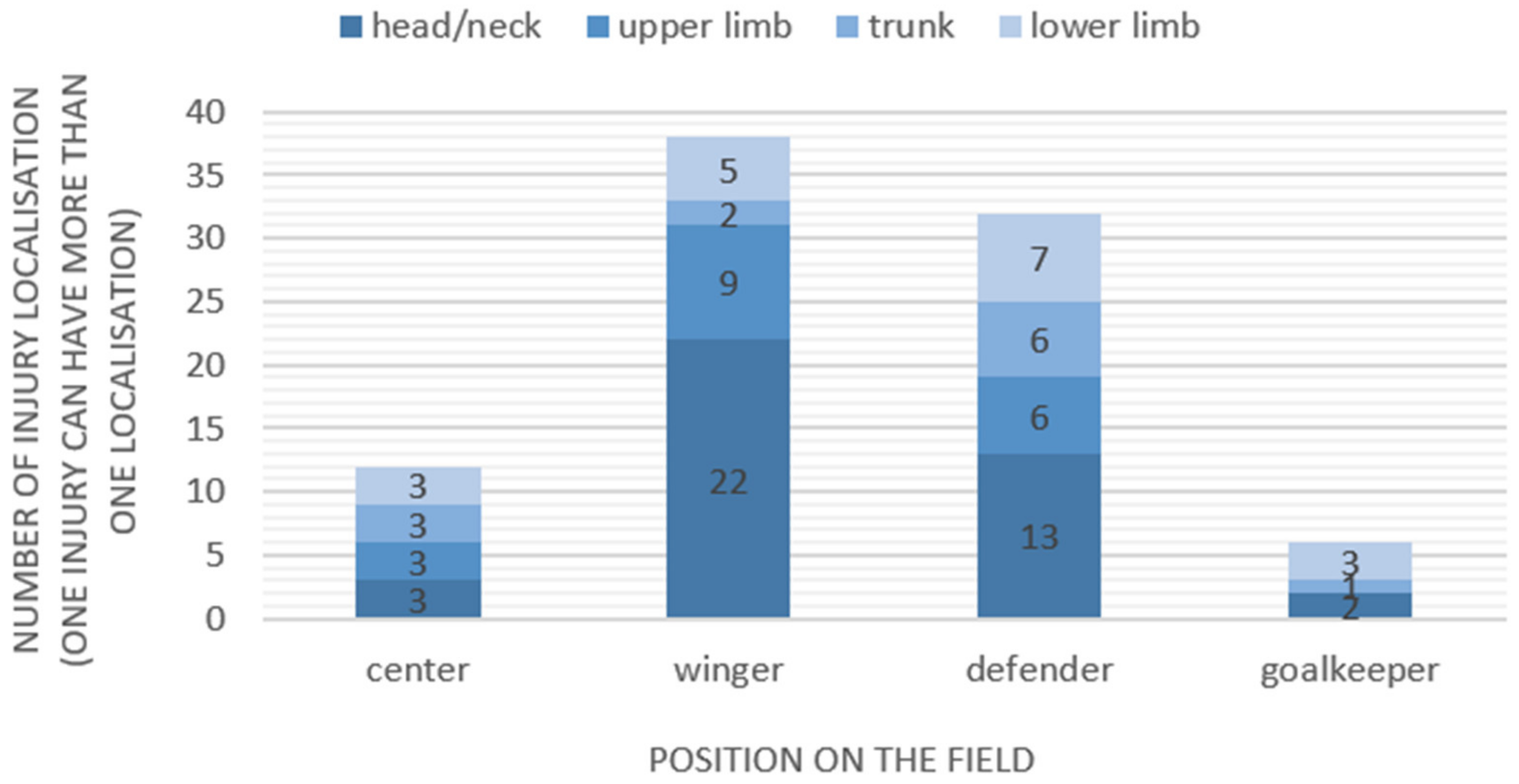
3.3. Injury Locations, Types, and Severity
3.4. Injury Mechanism
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rogan, S.; Blasimann, A.; Steiger, M.; Torre, A.; Radlinger, L. Acute effects of fast dynamic stretching on rate of force development in ice hockey players: A pilot study. Sportverletz. Sportschaden 2012, 26, 207–211. [Google Scholar] [PubMed]
- Taeymans, J.; Blaser, V.; Kneubuehl, M.; Rogan, S. Injuries in ice hockey: A questionnaire survey in second league amateur ice hockey players in the canton of bern (switzerland). Sportverletz. Sportschaden 2019, 33, 216–223. [Google Scholar]
- Morrissey, P.J.; Maier, S.P.; Zhou, J.J.; Sedaghatpour, D.; Shah, N.V.; Torre, B.B.; Beaufort, A.; Chatterjee, D.; Doran, J.P.; Urban, W.P. Epidemiology and trends of adult ice hockey injuries presenting to united states emergency departments: A ten-year analysis from 2007–2016. J. Orthop. 2020, 22, 231–236. [Google Scholar] [CrossRef]
- Jin, H.; Lee, H. Risk factors based on analysis of injury mechanism and protective equipment for ice hockey amateur players. Int. J. Environ. Res. Public Health 2022, 19, 4232. [Google Scholar] [CrossRef]
- Emery, C.A.; Kang, J.; Shrier, I.; Goulet, C.; Hagel, B.E.; Benson, B.W.; Nettel-Aguirre, A.; McAllister, J.R.; Hamilton, G.M.; Meeuwisse, W.H. Risk of injury associated with body checking among youth ice hockey players. JAMA 2010, 303, 2265–2272. [Google Scholar] [CrossRef]
- Gröger, A. Ten years of ice hockey-related-injuries in the german ice hockey federation. Sportverletz. Sportschaden 2001, 15, 82–86. [Google Scholar] [CrossRef]
- Hostetler, S.G.; Xiang, H.; Smith, G.A. Characteristics of ice hockey–related injuries treated in us emergency departments, 2001–2002. Pediatrics 2004, 114, e661–e666. [Google Scholar] [CrossRef]
- Sim, F.H.; Simonet, W.T.; Melton, L.J.; Lehn, T.A. Ice hockey injuries. Am. J. Sports Med. 1987, 15, 30–40. [Google Scholar] [CrossRef]
- Weisskopf, L. Verletzungen des bewegungsapparates im eishockey. Schweiz. Z. Sportmed. Sport. 2010, 58, 52–55. [Google Scholar]
- Hämel, D. Eishockey. In Praxiswissen Halte- und Bewegungsorgane. Sportverletzungen-Sportschaden; Griffka, J., Engelhardt, M., Krüger-Franke, M., Pieper, H.-G., Siebert, C.H., Eds.; Thieme Verlag: Stuttgart, Germany, 2005; pp. 164–170. [Google Scholar]
- Åman, M.; Forssblad, M.; Larsén, K. National injury prevention measures in team sports should focus on knee, head, and severe upper limb injuries. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1000–1008. [Google Scholar] [CrossRef]
- Brügger, O.; Bianchi, G.; Hofer, F.; Walter, M.; Michel, F.I.; Müller, C. Unfallforschung Sport; BfU-Beratungsstelle für Unfallverhütung: Bern, Switzerland, 2012. [Google Scholar]
- Lamprecht, M.; Stamm, H. Observatorium Sport und Bewegung Schweiz; Bundesamt für Sport BASPO: Magglingen, Switzerland, 2014. [Google Scholar]
- Knowles, S.B.; Marshall, S.W.; Guskiewicz, K.M. Issues in estimating risks and rates in sports injury research. J. Athl. Train. 2006, 41, 207–215. [Google Scholar]
- Theisen, D.; Malisoux, L.; Seil, R.; Urhausen, A. Injuries in youth sports: Epidemiology, risk factors and prevention. Dtsch. Z. Sportmed. 2014, 65, 248–252. [Google Scholar] [CrossRef]
- Engel, J.; Kaelin, M.; Rogan, S. Verletzungen im Unihockey–eine Fragebogenerhebung bei Schweizer-Nationalliga-A-Unihockey-Spielern. Sportverletz. Sportschaden 2018, 33, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Olsen, O.-E.; Myklebust, G.; Engebretsen, L.; Holme, I.; Bahr, R. Exercises to prevent lower limb injuries in youth sports: Cluster randomised controlled trial. BMJ 2005, 330, 449. [Google Scholar] [CrossRef] [PubMed]
- Agel, J.; Dompier, T.P.; Dick, R.; Marshall, S.W. Descriptive epidemiology of collegiate men’s ice hockey injuries: National collegiate athletic association injury surveillance system, 1988–1989 through 2003–2004. J. Athl. Train. 2007, 42, 241–248. [Google Scholar] [PubMed]
- Tuominen, M.; Stuart, M.J.; Aubry, M.; Kannus, P.; Parkkari, J. Injuries in world junior ice hockey championships between 2006 and 2015. Br. J. Sports Med. 2016, 51, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Donskov, A.S.; Humphreys, D.; Dickey, J.P. What is injury in ice hockey: An integrative literature review on injury rates, injury definition, and athlete exposure in men’s elite ice hockey. Sports 2019, 7, 227. [Google Scholar] [CrossRef]
- Dick, R.; Agel, J.; Marshall, S.W. National collegiate athletic association injury surveillance system commentaries: Introduction and methods. J. Athl. Train. 2007, 42, 173–182. [Google Scholar]
- Patel, D.R.; Yamasaki, A.; Brown, K. Epidemiology of sports-related musculoskeletal injuries in young athletes in united states. Transl. Pediatr. 2017, 6, 160–166. [Google Scholar] [CrossRef]
- R Foundation for Statistical Computing. The R Project for Statistical Computing R: A Language and Environment for Statistical Computing, Version 4.1.3; R Core Team, R: Vienna, Austria, 2020. [Google Scholar]
- Perkhofer, S.; Gebhart, V.; Tucek, G.; Wertz, F.J.; Weigl, R.; Ritschl, V.; Ritschl, H.; Höhsl, B.; Prinz-Buchberger, B.; Stamm, T. Qualitative forschung. In Wissenschaftliches Arbeiten und Schreiben; Springer: Berlin/Heidelberg, Germany, 2016; pp. 67–135. [Google Scholar]
- Brunner, R.; Bizzini, M.; Niedermann, K.; Maffiuletti, N.A. Epidemiology of traumatic and overuse injuries in swiss professional male ice hockey players. Orthop. J. Sports Med. 2020, 8, 2325967120964720. [Google Scholar] [CrossRef]
- Anderson, G.R.; Melugin, H.P.; Stuart, M.J. Epidemiology of injuries in ice hockey. Sports Health 2019, 11, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Szukics, P.F.; Otlans, P.T.; Arevalo, A.; Meade, M.; DeLuca, P.; Salvo, J.P. A scoping review of injuries in amateur and professional men’s ice hockey. Orthop. J. Sports Med. 2022, 10, 23259671221085968. [Google Scholar] [PubMed]
- Verschueren, J.; Tassignon, B.; De Pauw, K.; Proost, M.; Teugels, A.; Van Cutsem, J.; Roelands, B.; Verhagen, E.; Meeusen, R. Does acute fatigue negatively affect intrinsic risk factors of the lower extremity injury risk profile? A systematic and critical review. Sports Med. 2020, 50, 767–784. [Google Scholar] [CrossRef]
- Smith, A.M.; Stuart, M.J.; Wiese-Bjornstal, D.M.; Gunnon, C. Predictors of injury in ice hockey players: A multivariate, multidisciplinary approach. Am. J. Sports Med. 1997, 25, 500–507. [Google Scholar] [CrossRef]
- Mölsä, J.; Kujala, U.; Näsman, O.; Lehtipuu, T.-P.; Airaksinen, O. Injury profile in ice hockey from the 1970s through the 1990s in finland. Am. J. Sports Med. 2000, 28, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Azuelos, Y.H.; Pearsall, D.J.; Turcotte, R.A.; Montgomery, D.L. A review of ice hockey injuries: Location, diagnosis, and mechanism. In Safety in Ice Hockey; Pearsall, D.J., Ashare, A.B., Eds.; ASTM International: West Conshohocken, PA, USA, 2004; Volume 4, pp. 59–69. [Google Scholar]
- Flik, K.; Lyman, S.; Marx, R.G. American collegiate men’s ice hockey: An analysis of injuries. Am. J. Sports Med. 2005, 33, 183–187. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Player’s Position | Weight (kg) | Height (cm) | BMI (kg/m2) |
|---|---|---|---|
| Center (n = 11) | 72.6 (±4.2) | 179.0 (±3.7) | 22.7 (±1.5) |
| Winger (n = 28) | 78.4 (±6.5) | 179.0 (±5.7) | 24.4 (±1.8) |
| Defender (n = 26) | 76.7 (±7.4) | 178.0 (±5.3) | 24.1 (±1.8) |
| Goalkeeper (n = 8) | 75.3 (±6.4) | 181.0 (±4,4) | 23.2 (±2.4) |
| Exposure | Off-Season [h] (April 2019–August 2019) | Peak Season [h] (September 2019–March 2020) | Total [h] |
|---|---|---|---|
| Practice | 223.0 ± 52.1 | 376.0 ± 105.0 | 599.0 ± 140 |
| Game | 16.5 ± 16.5 | 121.0 ± 33.8 | 138.0 ± 37.4 |
| Practice and game | 240.0 ± 55.3 | 497.0 ± 112 | 737.0 ± 144.0 |
| Part of the Body | <1 Week | 1–4 Weeks | >4 Weeks |
|---|---|---|---|
| Contusion/sprain | 5 | 5 | 4 |
| Ligament lesion | 0 | 2 | 3 |
| Muscle-tendon injury | 3 | 6 | 6 |
| Skin injury | 4 | 1 | 0 |
| Joint injury | 0 | 0 | 5 |
| Fracture | 0 | 1 | 7 |
| Concussion | 0 | 10 | 4 |
| Inflammation | 3 | 4 | 2 |
| Other | 0 | 0 | 1 |
| Total | 15 | 29 | 32 |
| Injury Mechanism | % of Injuries |
|---|---|
| Contact with an opponent (unintended) | 56% |
| Body check | 38% and partly localized to the head (n = 8) |
| Contact with stick or puck | 12% |
| Boarding | 30% |
| Without external impact | 12% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruff, J.; Taeymans, J.; Blasimann, A.; Rogan, S. Analysis of Injuries in the Swiss U20 Elite Ice Hockey Season 2019/2020—A Retrospective Survey. Sports 2024, 12, 88. https://doi.org/10.3390/sports12040088
Ruff J, Taeymans J, Blasimann A, Rogan S. Analysis of Injuries in the Swiss U20 Elite Ice Hockey Season 2019/2020—A Retrospective Survey. Sports. 2024; 12(4):88. https://doi.org/10.3390/sports12040088
Chicago/Turabian StyleRuff, Jonas, Jan Taeymans, Angela Blasimann, and Slavko Rogan. 2024. "Analysis of Injuries in the Swiss U20 Elite Ice Hockey Season 2019/2020—A Retrospective Survey" Sports 12, no. 4: 88. https://doi.org/10.3390/sports12040088