
Effects of Physical Exercise on Executive Function in Schizophrenia: Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,  , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Sources of Information
2.3. Search Strategy
2.4. Selection Process
2.5. Data Extraction and Management
2.6. Risk of Bias Assessment and Certainty Assessment
2.7. Meta-Analysis
3. Results
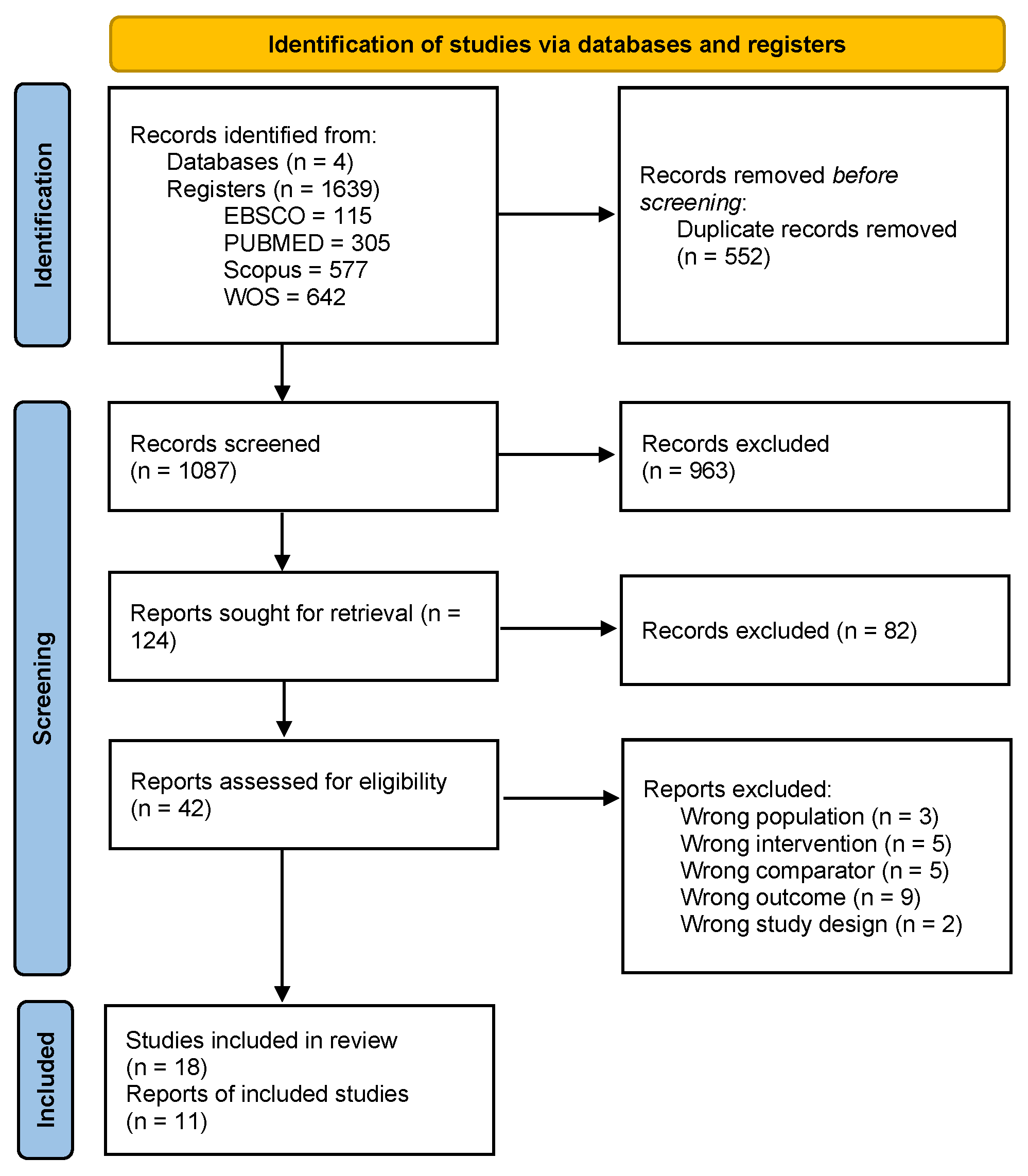
3.1. Study Selection
3.2. Characteristics of Studies
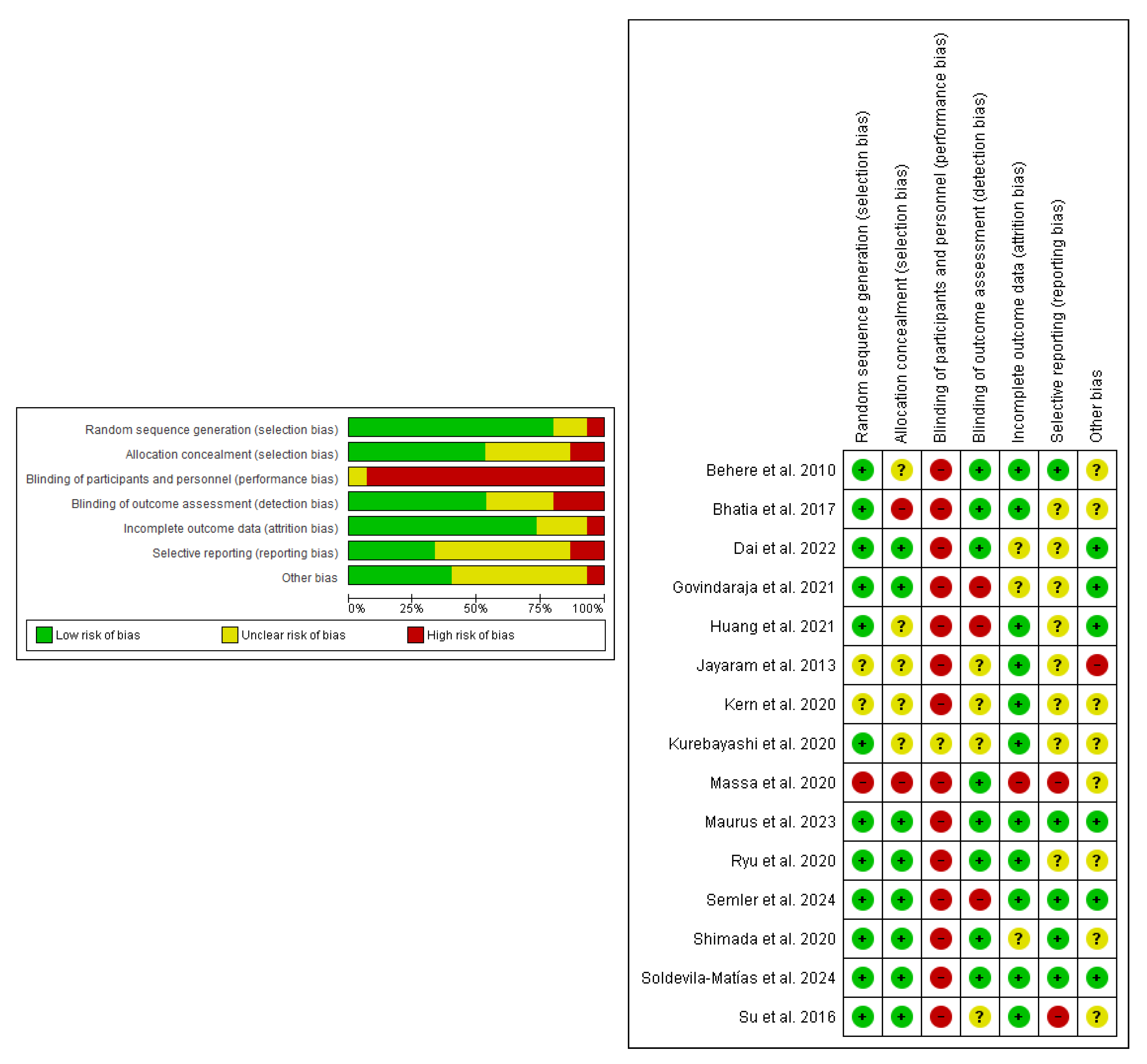
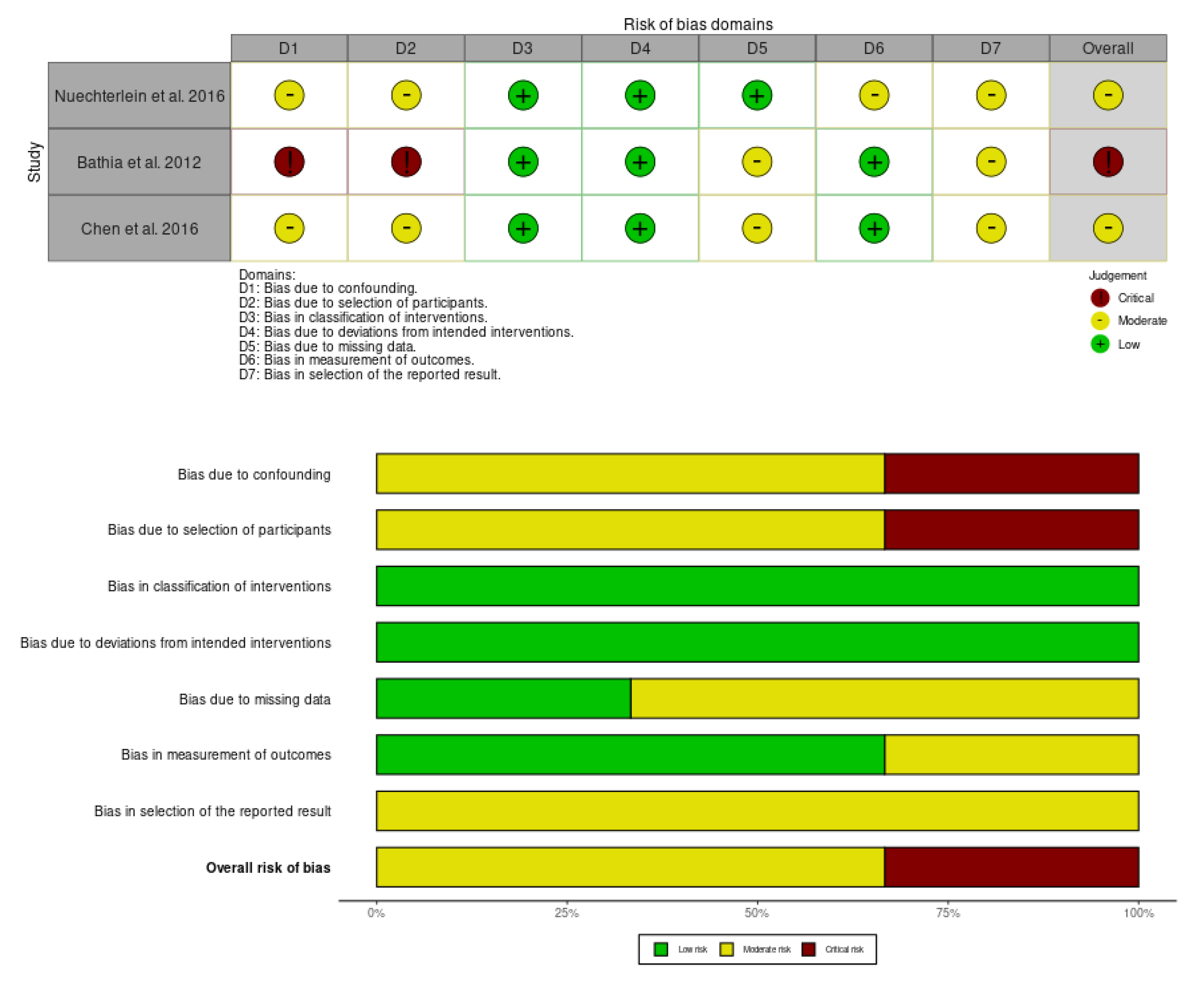
3.3. Risk of Bias
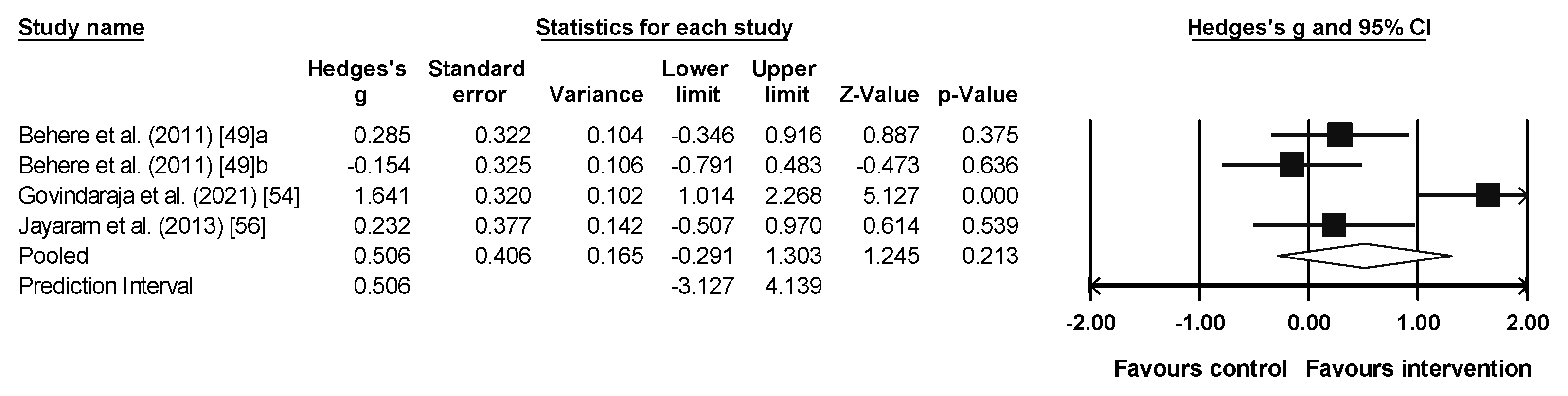
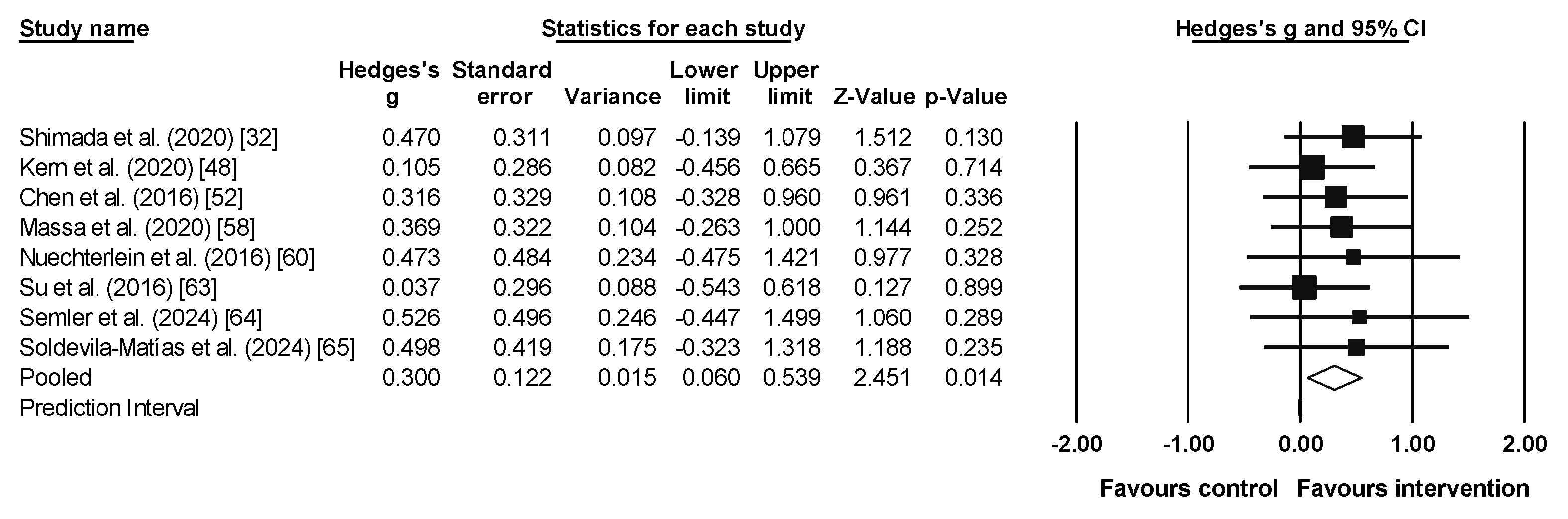
3.4. Meta-Analysis Results for Emotion Recognition
3.5. Meta-Analysis Results for Working Memory
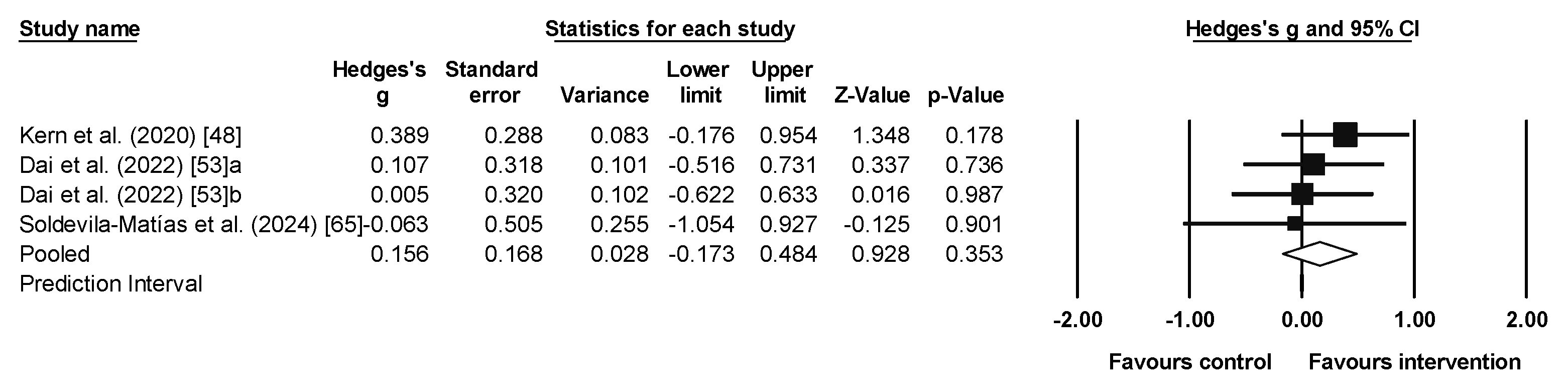
3.6. Meta-Analysis Results for Inhibition
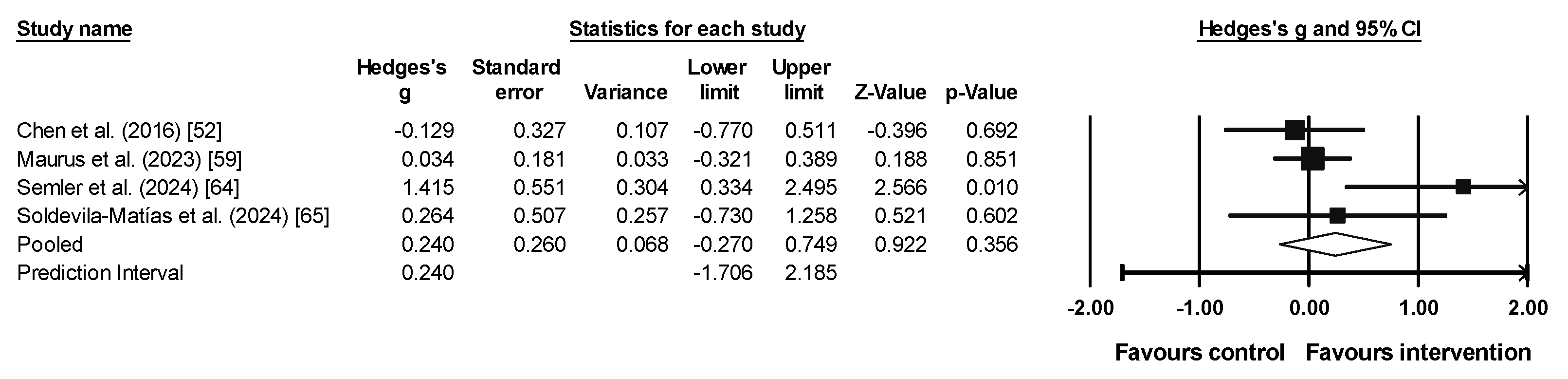
3.7. Meta-Analysis Results for Cognitive Flexibility
3.8. Certainty of the Evidence
4. Discussion
4.1. Non-Significant Results: Emotion Recognition, Inhibition, and Cognitive Flexibility
4.2. Significant Results: Working Memory
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Degnan, A.; Berry, K.; Sweet, D.; Abel, K.; Crossley, N.; Edge, D. Social Networks and Symptomatic and Functional Outcomes in Schizophrenia: A Systematic Review and Meta-Analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 873–888. [Google Scholar] [CrossRef] [PubMed]
- De Donatis, D.; Porcelli, S.; De Ronchi, D.; Merlo Pich, E.; Kas, M.J.; Bilderbeck, A.; Serretti, A. Social Withdrawal and Neurocognitive Correlates in Schizophrenia. Int. Clin. Psychopharmacol. 2022, 37, 102–109. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Manual Diagnóstico y Estadístico de Los Tras-Tornos Mentales (DSM-5®), 5th ed.; Arlington, V., Ed.; American Psychiatric Association: Washington, DC, USA, 2014. [Google Scholar]
- Khalil, M.; Hollander, P.; Raucher-Chéné, D.; Lepage, M.; Lavigne, K.M. Structural Brain Correlates of Cognitive Function in Schizophrenia: A Meta-Analysis. Neurosci. Biobehav. Rev. 2022, 132, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Lepage, M.; Bodnar, M.; Bowie, C.R. Neurocognition: Clinical and Functional Outcomes in Schizophrenia. Can. J. Psychiatry 2014, 59, 5–12. [Google Scholar] [CrossRef]
- Gebreegziabhere, Y.; Habatmu, K.; Mihretu, A.; Cella, M.; Alem, A. Cognitive Impairment in People with Schizophrenia: An Umbrella Review. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 272, 1139–1155. [Google Scholar] [CrossRef]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Salehinejad, M.A.; Ghanavati, E.; Rashid, M.H.A.; Nitsche, M.A. Hot and Cold Executive Functions in the Brain: A Prefrontal-Cingular Network. Brain Neurosci. Adv. 2021, 5, 23982128211007769. [Google Scholar] [CrossRef]
- Savla, G.N.; Vella, L.; Armstrong, C.C.; Penn, D.L.; Twamley, E.W. Deficits in Domains of Social Cognition in Schizophrenia: A Meta-Analysis of the Empirical Evidence. Schizophr. Bull. 2013, 39, 979–992. [Google Scholar] [CrossRef]
- Rüsch, N.; Tebartz van Elst, L.; Valerius, G.; Büchert, M.; Thiel, T.; Ebert, D.; Hennig, J.; Olbrich, H.-M. Neurochemical and Structural Correlates of Executive Dysfunction in Schizophrenia. Schizophr. Res. 2008, 99, 155–163. [Google Scholar] [CrossRef]
- Sánchez, P.; Ojeda, N.; Peña, J.; Elizagárate, E.; Yoller, A.B.; Gutiérrez, M.; Ezcurra, J. Predictors of Longitudinal Changes in Schizophrenia. J. Clin. Psychiatry 2009, 70, 888–896. [Google Scholar] [CrossRef]
- Sawada, K.; Kanehara, A.; Sakakibara, E.; Eguchi, S.; Tada, M.; Satomura, Y.; Suga, M.; Koike, S.; Kasai, K. Identifying Neurocognitive Markers for Outcome Prediction of Global Functioning in Individuals with First-Episode and Ultra-High-Risk for Psychosis. Psychiatry Clin. Neurosci. 2017, 71, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Firth, J.; Schuch, F.B.; Rosenbaum, S.; Mugisha, J.; Hallgren, M.; Probst, M.; Ward, P.B.; Gaughran, F.; De Hert, M.; et al. Sedentary Behavior and Physical Activity Levels in People with Schizophrenia, Bipolar Disorder and Major Depressive Disorder: A Global Systematic Review and Meta-Analysis. World Psychiatry 2017, 16, 308–315. [Google Scholar] [CrossRef]
- Stubbs, B.; Ku, P.-W.; Chung, M.-S.; Chen, L.-J. Relationship Between Objectively Measured Sedentary Behavior and Cognitive Performance in Patients With Schizophrenia Vs Controls. Schizophr. Bull. 2017, 3, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Stubbs, B.; Rosenbaum, S.; Vancampfort, D.; Malchow, B.; Schuch, F.; Elliott, R.; Nuechterlein, K.H.; Yung, A.R. Aerobic Exercise Improves Cognitive Functioning in People With Schizophrenia: A Systematic Review and Meta-Analysis. Schizophr. Bull. 2017, 3, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Girdler, S.J.; Confino, J.E.; Woesner, M.E. Exercise as a Treatment for Schizophrenia: A Review. Psychopharmacol. Bull. 2019, 49, 56–69. [Google Scholar]
- Maurus, I.; Hasan, A.; Röh, A.; Takahashi, S.; Rauchmann, B.; Keeser, D.; Malchow, B.; Schmitt, A.; Falkai, P. Neurobiological Effects of Aerobic Exercise, with a Focus on Patients with Schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 269, 499–515. [Google Scholar] [CrossRef]
- Roeh, A.; Hasan, A. Exercise for the Treatment of Schizophrenia: A Current Review and Recommendations. Dtsch. Z. Sportmed./Ger. J. Sports Med. 2021, 72, 288–292. [Google Scholar] [CrossRef]
- van der Stouwe, E.C.D.; van Busschbach, J.T.; de Vries, B.; Cahn, W.; Aleman, A.; Pijnenborg, G.H.M. Neural Correlates of Exercise Training in Individuals with Schizophrenia and in Healthy Individuals: A Systematic Review. Neuroimage Clin. 2018, 19, 287–301. [Google Scholar] [CrossRef]
- Pesce, C. Shifting the Focus From Quantitative to Qualitative Exercise Characteristics in Exercise and Cognition Research. J. Sport Exerc. Psychol. 2012, 34, 766–786. [Google Scholar] [CrossRef]
- Deste, G.; Corbo, D.; Nibbio, G.; Italia, M.; Dell’Ovo, D.; Calzavara-Pinton, I.; Lisoni, J.; Barlati, S.; Gasparotti, R.; Vita, A. Impact of Physical Exercise Alone or in Combination with Cognitive Remediation on Cognitive Functions in People with Schizophrenia: A Qualitative Critical Review. Brain Sci. 2023, 13, 320. [Google Scholar] [CrossRef]
- Falkai, P.; Malchow, B.; Schmitt, A. Aerobic Exercise and Its Effects on Cognition in Schizophrenia. Curr. Opin. Psychiatry 2017, 30, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Cramer, H.; Lauche, R.; Klose, P.; Langhorst, J.; Dobos, G. Yoga for Schizophrenia: A Systematic Review and Meta-Analysis. BMC Psychiatry 2013, 13, 32. [Google Scholar] [CrossRef]
- Vella, S.A.; Sutcliffe, J.T.; Fernandez, D.; Liddelow, C.; Aidman, E.; Teychenne, M.; Smith, J.J.; Swann, C.; Rosenbaum, S.; White, R.L.; et al. Context Matters: A Review of Reviews Examining the Effects of Contextual Factors in Physical Activity Interventions on Mental Health and Wellbeing. Ment. Health Phys. Act. 2023, 25, 100520. [Google Scholar] [CrossRef]
- Pesce, C.; Vazou, S.; Benzing, V.; Álvarez-Bueno, C.; Anzeneder, S.; Mavilidi, M.F.; Leone, L.; Schmidt, M. Effects of Chronic Physical Activity on Cognition across the Lifespan: A Systematic Meta-Review of Randomized Controlled Trials and Realist Synthesis of Contextualized Mechanisms. Int. Rev. Sport Exerc. Psychol. 2023, 16, 722–760. [Google Scholar] [CrossRef]
- Dauwan, M.; Begemann, M.J.H.; Slot, M.I.E.; Lee, E.H.M.; Scheltens, P.; Sommer, I.E.C. Physical Exercise Improves Quality of Life, Depressive Symptoms, and Cognition across Chronic Brain Disorders: A Transdiagnostic Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Neurol. 2021, 268, 1222–1246. [Google Scholar] [CrossRef]
- Firth, J.; Cotter, J.; Carney, R.; Yung, A.R. The Pro-Cognitive Mechanisms of Physical Exercise in People with Schizophrenia. Br. J. Pharmacol. 2017, 174, 3161–3172. [Google Scholar] [CrossRef]
- Malchow, B.; Reich-Erkelenz, D.; Oertel-Knöchel, V.; Keller, K.; Hasan, A.; Schmitt, A.; Scheewe, T.W.; Cahn, W.; Kahn, R.S.; Falkai, P. The Effects of Physical Exercise in Schizophrenia and Affective Disorders. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 451–467. [Google Scholar] [CrossRef]
- Mittal, V.A.; Vargas, T.; Juston Osborne, K.; Dean, D.; Gupta, T.; Ristanovic, I.; Hooker, C.I.; Shankman, S.A. Exercise Treatments for Psychosis: A Review. Curr. Treat. Options Psychiatry 2017, 4, 152–166. [Google Scholar] [CrossRef]
- Vancampfort, D.; Probst, M.; Helvik Skjaerven, L.; Catalán-Matamoros, D.; Lundvik-Gyllensten, A.; Gómez-Conesa, A.; Ijntema, R.; De Hert, M. Systematic Review of the Benefits of Physical Therapy Within a Multidisciplinary Care Approach for People With Schizophrenia. Phys. Ther. 2012, 92, 11–23. [Google Scholar] [CrossRef]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be Smart, Exercise Your Heart: Exercise Effects on Brain and Cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Shimada, T.; Ito, S.; Makabe, A.; Yamanushi, A.; Takenaka, A.; Kawano, K.; Kobayashi, M. Aerobic Exercise and Cognitive Functioning in Schizophrenia: An Updated Systematic Review and Meta-Analysis. Psychiatry Res. 2022, 314, 114656. [Google Scholar] [CrossRef]
- Xu, Y.; Cai, Z.; Fang, C.; Zheng, J.; Shan, J.; Yang, Y. Impact of Aerobic Exercise on Cognitive Function in Patients with Schizophrenia during Daily Care: A Meta-Analysis. Psychiatry Res. 2022, 312, 114560. [Google Scholar] [CrossRef]
- Pontifex, M.B.; McGowan, A.L.; Chandler, M.C.; Gwizdala, K.L.; Parks, A.C.; Fenn, K.; Kamijo, K. A Primer on Investigating the after Effects of Acute Bouts of Physical Activity on Cognition. Psychol. Sport Exerc. 2019, 40, 1–22. [Google Scholar] [CrossRef]
- Duijkers, J.C.L.M.; Vissers, C.T.W.M.; Egger, J.I.M. Unraveling Executive Functioning in Dual Diagnosis. Front. Psychol. 2016, 7, 979. [Google Scholar] [CrossRef]
- Mihaljević-Peleš, A.; Bajs Janović, M.; Šagud, M.; Živković, M.; Janović, Š.; Jevtović, S. Cognitive Deficit in Schizophrenia: An Overview. Psychiatr. Danub. 2019, 31, 139–142. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Pérez-Romero, N.; Campos-Jara, C.; Pesce, C.; Araya Sierralta, S.; Cerda-Vega, E.; Ramirez-Campillo, R.; Campos-Jara, R.; Martínez-Salazar, C.; Arellano-Roco, C.; Contreras-Osorio, F. Effects of Physical Exercise on Executive Functions of Individuals with Schizophrenia Spectrum Disorders: Protocol for a Systematic Review and Meta-Analysis. PLoS ONE 2024, 19, e0296273. [Google Scholar] [CrossRef]
- Centre for Reviews and Dissemination. CRD’s Guidance for Undertaking Reviews in Health Care; York Publishing Services Ltd.: York, UK, 2009. [Google Scholar]
- Arora, N.K.; Roehrken, G.; Crumbach, S.; Phatak, A.; Labott, B.K.; Nicklas, A.; Wicker, P.; Donath, L. Good Scientific Practice and Ethics in Sports and Exercise Science: A Brief and Comprehensive Hands-on Appraisal for Sports Research. Sports 2023, 11, 47. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S. GRADE Guidelines: 3. Rating the Quality of Evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; deBeer, H. GRADE Guidelines: 1. Introduction—GRADE Evidence Profiles and Summary of Findings Tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Moran, J.; Ramirez-Campillo, R.; Granacher, U. Effects of Jumping Exercise on Muscular Power in Older Adults: A Meta-Analysis. Sports Med. 2018, 48, 2843–2857. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefits in Children and Adolescents? A Systematic Review and Meta-Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef]
- Kern, R.S.; Reddy, L.F.; Cohen, A.N.; Young, A.S.; Green, M.F. Effects of Aerobic Exercise on Cardiorespiratory Fitness and Social Functioning in Veterans 40 to 65 Years Old with Schizophrenia. Psychiatry Res. 2020, 291, 113258. [Google Scholar] [CrossRef]
- Behere, R.V.; Arasappa, R.; Jagannathan, A.; Varambally, S.; Venkatasubramanian, G.; Thirthalli, J.; Subbakrishna, D.K.; Nagendra, H.R.; Gangadhar, B.N. Effect of Yoga Therapy on Facial Emotion Recognition Deficits, Symptoms and Functioning in Patients with Schizophrenia. Acta Psychiatr. Scand. 2011, 123, 147–153. [Google Scholar] [CrossRef]
- Bhatia, T.; Agarwal, A.; Shah, G.; Wood, J.; Richard, J.; Gur, R.E.; Gur, R.C.; Nimgaonkar, V.L.; Mazumdar, S.; Deshpande, S.N. Adjunctive Cognitive Remediation for Schizophrenia Using Yoga: An Open, Non-Randomised Trial. Acta Neuropsychiatr. 2012, 24, 91–100. [Google Scholar] [CrossRef]
- Bhatia, T.; Mazumdar, S.; Wood, J.; He, F.; Gur, R.E.; Gur, R.C.; Nimgaonkar, V.L.; Deshpande, S.N. A Randomised Controlled Trial of Adjunctive Yoga and Adjunctive Physical Exercise Training for Cognitive Dysfunction in Schizophrenia. Acta Neuropsychiatr. 2017, 29, 102–114. [Google Scholar] [CrossRef]
- Chen, M.; Kuo, Y.; Chang, Y.; Hsu, S.; Kuo, C.; Chang, J. Influences of Aerobic Dance on Cognitive Performance in Adults with Schizophrenia. Occup. Ther. Int. 2016, 23, 346–356. [Google Scholar] [CrossRef]
- Dai, Y.; Ding, H.; Lu, X.; Wu, X.; Xu, C.; Jiang, T.; Ming, L.; Xia, Z.; Song, C.; Shen, H.; et al. CCRT and Aerobic Exercise: A Randomised Controlled Study of Processing Speed, Cognitive Flexibility, and Serum BDNF Expression in Schizophrenia. Schizophrenia 2022, 8, 84. [Google Scholar] [CrossRef] [PubMed]
- Govindaraj, R.; Naik, S.S.; Mehta, U.M.; Sharma, M.; Varambally, S.; Gangadhar, B.N. Yoga Therapy for Social Cognition in Schizophrenia: An Experimental Medicine-Based Randomized Controlled Trial. Asian J. Psychiatr. 2021, 62, 102731. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-C.; Hung, C.-F.; Hsu, S.-T.; Lin, P.-Y.; Lee, Y.; Chong, M.-Y.; Chen, C.-C.; Kuo, Y.-H.; Wang, L.-J. Effects of Aerobic Walking on Cognitive Function in Patients with Schizophrenia: A Randomized Controlled Trial. J. Psychiatr. Res. 2021, 134, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, N.; Varambally, S.; Behere, R.; Venkatasubramanian, G.; Arasappa, R.; Christopher, R.; Gangadhar, B. Effect of Yoga Therapy on Plasma Oxytocin and Facial Emotion Recognition Deficits in Patients of Schizophrenia. Indian J. Psychiatry 2013, 55, 409. [Google Scholar] [CrossRef]
- Kurebayashi, Y.; Mori, K.; Otaki, J. Effects of Mild-intensity Physical Exercise on Neurocognition in Inpatients with Schizophrenia: A Pilot Randomized Controlled Trial. Perspect. Psychiatr. Care 2022, 58, 1037–1047. [Google Scholar] [CrossRef]
- Massa, N.; Alrohaibani, A.; Mammino, K.; Bello, M.; Taylor, N.; Cuthbert, B.; Fargotstein, M.; Coulter, M.M.; Boatright, J.H.; Nocera, J.; et al. The Effect of Aerobic Exercise on Physical and Cognitive Outcomes in a Small Cohort of Outpatients with Schizophrenia. Brain Plast. 2020, 5, 161–174. [Google Scholar] [CrossRef]
- Maurus, I.; Roell, L.; Lembeck, M.; Papazova, I.; Greska, D.; Muenz, S.; Wagner, E.; Campana, M.; Schwaiger, R.; Schneider-Axmann, T.; et al. Exercise as an Add-on Treatment in Individuals with Schizophrenia: Results from a Large Multicenter Randomized Controlled Trial. Psychiatry Res. 2023, 328, 115480. [Google Scholar] [CrossRef]
- Nuechterlein, K.H.; Ventura, J.; McEwen, S.C.; Gretchen-Doorly, D.; Vinogradov, S.; Subotnik, K.L. Enhancing Cognitive Training Through Aerobic Exercise After a First Schizophrenia Episode: Theoretical Conception and Pilot Study. Schizophr. Bull. 2016, 42, S44–S52. [Google Scholar] [CrossRef]
- Ryu, J.; Jung, J.H.; Kim, J.; Kim, C.-H.; Lee, H.-B.; Kim, D.-H.; Lee, S.-K.; Shin, J.-H.; Roh, D. Outdoor Cycling Improves Clinical Symptoms, Cognition and Objectively Measured Physical Activity in Patients with Schizophrenia: A Randomized Controlled Trial. J. Psychiatr. Res. 2020, 120, 144–153. [Google Scholar] [CrossRef]
- Shimada, T.; Ito, S.; Makabe, A.; Yamanushi, A.; Takenaka, A.; Kawano, K.; Kobayashi, M. Aerobic Exercise and Cognitive Functioning in Schizophrenia: Results of a 1-Year Follow-up from a Randomized Controlled Trial. Psychiatry Res. 2020, 286, 112854. [Google Scholar] [CrossRef]
- Su, C.-Y.; Wang, P.-W.; Lin, Y.-J.; Tang, T.-C.; Liu, M.-F.; Chen, M.-D. The Effects of Aerobic Exercise on Cognition in Schizophrenia: A 3-Month Follow-up Study. Psychiatry Res. 2016, 244, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Semler, E.; Herpich, F.; Zellner, L.; Zwick, S.; Zwanzger, P.; Brunnauer, A. The Impact of Aerobic Endurance Training on Cognitive Performance in Schizophrenic Inpatients in a Clinical Routine Setting. Eur. Arch. Psychiatry Clin. Neurosci. 2024, 275, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Soldevila-Matías, P.; Sánchez-Ortí, J.V.; Correa-Ghisays, P.; Balanzá-Martínez, V.; Selva-Vera, G.; Sanchis-Sanchis, R.; Iglesias-García, N.; Monfort-Pañego, M.; Tomás-Martínez, P.; Victor, V.M.; et al. Exercise as a Promoter of Neurocognitive Improvement in People with Psychiatric Disorders and Comorbid Obesity: A Randomized Controlled Trial. Psychiatry Res. 2024, 342, 116226. [Google Scholar] [CrossRef] [PubMed]
- Green, M.F.; Horan, W.P.; Lee, J. Nonsocial and Social Cognition in Schizophrenia: Current Evidence and Future Directions. World Psychiatry 2019, 18, 146–161. [Google Scholar] [CrossRef]
- Firth, J.; Cotter, J.; Elliott, R.; French, P.; Yung, A.R. A Systematic Review and Meta-Analysis of Exercise Interventions in Schizophrenia Patients. Psychol. Med. 2015, 45, 1343–1361. [Google Scholar] [CrossRef]
- Stubbs, B.; Vancampfort, D.; Hallgren, M.; Firth, J.; Veronese, N.; Solmi, M.; Brand, S.; Cordes, J.; Malchow, B.; Gerber, M.; et al. EPA Guidance on Physical Activity as a Treatment for Severe Mental Illness: A Meta-Review of the Evidence and Position Statement from the European Psychiatric Association (EPA), Supported by the International Organization of Physical Therapists in Mental Health (IOPTMH). Eur. Psychiatry 2018, 54, 124–144. [Google Scholar] [CrossRef]
- Tsukamoto, H.; Olesen, N.D.; Petersen, L.G.; Suga, T.; Sørensen, H.; Nielsen, H.B.; Ogoh, S.; Secher, N.H.; Hashimoto, T. Circulating Plasma Oxytocin Level Is Elevated by High-Intensity Interval Exercise in Men. Med. Sci. Sports Exerc. 2024, 56, 927–932. [Google Scholar] [CrossRef]
- Domes, G.; Heinrichs, M.; Michel, A.; Berger, C.; Herpertz, S.C. Oxytocin Improves “Mind-Reading” in Humans. Biol. Psychiatry 2007, 61, 731–733. [Google Scholar] [CrossRef]
- Marsh, A.A.; Yu, H.H.; Pine, D.S.; Blair, R.J.R. Oxytocin Improves Specific Recognition of Positive Facial Expressions. Psychopharmacology 2010, 209, 225–232. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Fogassi, L. The Mirror Mechanism: Recent Findings and Perspectives. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130420. [Google Scholar] [CrossRef]
- Festante, F.; Ferrari, P.F.; Thorpe, S.G.; Buchanan, R.W.; Fox, N.A. Intranasal Oxytocin Enhances EEG Mu Rhythm Desynchronization during Execution and Observation of Social Action: An Exploratory Study. Psychoneuroendocrinology 2020, 111, 104467. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, P.F.; Coudé, G. Mirror Neurons, Embodied Emotions, and Empathy. In Neuronal Correlates of Empathy; Elsevier: Amsterdam, The Netherlands, 2018; pp. 67–77. [Google Scholar]
- Contreras-Osorio, F.; Ramirez-Campillo, R.; Cerda-Vega, E.; Campos-Jara, R.; Martínez-Salazar, C.; Reigal, R.E.; Morales-Sanchez, V.; Araya Sierralta, S.; Campos-Jara, C. Effects of Physical Exercise on Executive Function in Adults with Depression: A Systematic Review and Meta-Analysis Protocol. Sustainability 2022, 14, 15158. [Google Scholar] [CrossRef]
- Zhidong, C.; Wang, X.; Yin, J.; Song, D.; Chen, Z. Effects of Physical Exercise on Working Memory in Older Adults: A Systematic and Meta-Analytic Review. Eur. Rev. Aging Phys. Act. 2021, 18, 18. [Google Scholar] [CrossRef] [PubMed]
- Cabral, D.F.; Rice, J.; Morris, T.P.; Rundek, T.; Pascual-Leone, A.; Gomes-Osman, J. Exercise for Brain Health: An Investigation into the Underlying Mechanisms Guided by Dose. Neurotherapeutics 2019, 16, 580–599. [Google Scholar] [CrossRef]
- Baek, S.-S. Role of Exercise on the Brain. J. Exerc. Rehabil. 2016, 12, 380–385. [Google Scholar] [CrossRef]
- Stillman, C.M.; Esteban-Cornejo, I.; Brown, B.; Bender, C.M.; Erickson, K.I. Effects of Exercise on Brain and Cognition Across Age Groups and Health States. Trends Neurosci. 2020, 43, 533–543. [Google Scholar] [CrossRef]
- Pajonk, F.-G.; Wobrock, T.; Gruber, O.; Scherk, H.; Berner, D.; Kaizl, I.; Kierer, A.; Müller, S.; Oest, M.; Meyer, T. Hippocampal Plasticity in Response to Exercise in Schizophrenia. Arch. Gen. Psychiatry 2010, 67, 133–143. [Google Scholar] [CrossRef]
- Lin, J.; Chan, S.K.W.; Lee, E.H.M.; Chang, W.C.; Tse, M.; Su, W.W.; Sham, P.; Hui, C.L.M.; Joe, G.; Chan, C.L.W. Aerobic Exercise and Yoga Improve Neurocognitive Function in Women with Early Psychosis. NPJ Schizophr. 2015, 1, 15047. [Google Scholar] [CrossRef]
- Kimhy, D.; Vakhrusheva, J.; Bartels, M.N.; Armstrong, H.F.; Ballon, J.S.; Khan, S.; Chang, R.W.; Hansen, M.C.; Ayanruoh, L.; Lister, A.; et al. The Impact of Aerobic Exercise on Brain-Derived Neurotrophic Factor and Neurocognition in Individuals With Schizophrenia: A Single-Blind, Randomized Clinical Trial. Schizophr. Bull. 2015, 41, 859–868. [Google Scholar] [CrossRef]
- World Health Organization. Esquizofrenia. Available online: https://www.who.int/es/news-room/fact-sheets/detail/schizophrenia (accessed on 4 May 2023).
- Li, J.; Shen, J.; Wu, G.; Tan, Y.; Sun, Y.; Keller, E.; Jiang, Y.; Wu, J. Mindful Exercise versus Non-Mindful Exercise for Schizophrenia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Complement. Ther. Clin. Pract. 2018, 32, 17–24. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion | Exclusion | |
|---|---|---|
| Population | Adult individuals (age, 18–60 years) diagnosed with schizophrenia spectrum according to the Diagnostic and Statistical Manual of Mental Disorders (DSM), the International Classification of Diseases (ICD), or its equivalents from any version. | Major psychiatric disorders (e.g., bipolar disorder, dementia) and intellectual disabilities as comorbid conditions. Medical conditions that restrict physical activity (e.g., cardiopulmonary disease). |
| Intervention | Interventions involving physical exercise without restrictions regarding the type of exercise (e.g., multicomponent, aerobics, sports programs, yoga) that may include (or not) cognitive exercises. | Interventions with a duration of less than four weeks. |
| Comparator | Active (e.g., relaxation techniques) or passive (e.g., waiting list) control groups not exposed to physical exercise intervention. | Comparator group(s) with meaningfully different characteristic(s) other than the physical exercise intervention (e.g., sex). |
| Outcomes | Pre- and post-intervention data from at least one instrument for the direct assessment of ‘cold’ (working memory, inhibition, cognitive flexibility) or ‘hot’ (emotion regulation, decision making, and dimensions of social cognition) executive functions evaluated with instruments that have been previously validated (e.g., Trail Making Test, Flanker task, N-back task, or Iowa Gambling Task). | Indirect evaluation measures of the executive function, self-report questionnaires. |
| Study design | Randomized and non-randomized controlled studies. | Single-group studies; Case study (e.g., n < 4). |
| Reference | N | Sex (M/F) | Age (Years) | Diagnosis (Diagnostic Tool) | Baseline Schizophrenia Symptom Severity | Baseline Cognitive Status | Psychosocial Variables | Comorbidity |
|---|---|---|---|---|---|---|---|---|
| [49] | 91, EG1: 34, EG2: 31, CG: 26 | EG1: 18/9 EG2: 14/3 CG: 15/7 | EG1: 31.3 ± 9.3 EG2: 30.2 ± 8.0 CG: 33.6 ± 9.9 | Sch. (DSM-IV) | Positive symptoms: EG1: 15.1 ± 11.7, EG2: 14.9 ± 4.3, CG: 14.7 ± 6.3 Negative symptoms: EG1: 17.8 ± 4.9, EG2: 14.8 ± 3.9, CG: 14.3 ± 3.7 | N. R. | N. R. | N. R. |
| [50] | 88, EG: 65, CG: 23 | EG: 43/22, CG: 11/12 | EG: 31.50 ± 9.82, CG: 31.38 ± 11.14 | Psychoses (DIGS and FIGS) | Global Assessment of Functioning (GAF): EG: 34.33 ± 12.78, CG: 27.22 ± 6.266 | N. R. | Education in years: EG: 33.27 ± 9.815; CG: 8.79 ± 5.150 Marital status (ever married/never married): EG: 51.8%/48.2%; CG: 55.3%/44.7% Occupation [Employed/ (Unemployed or Retired)/Housewife/Student]: EG: 20%/59%/15%/6%; CG: 25%/56%/13%/6% | N. R. |
| [51] | 286, EG1: 104, EG2: 90, CG: 92 | EG1: 62/42, EG2: 62/28, CG: 57/35 | EG1: 34.76 ± 9.56, EG2: 35.20 ± 9.49, CG: 35.72 ± 10.06 | Sch. (DSM-IV) | SAPS: EG1: 12.44 ± 11.50, EG2: 13.30 ± 12.93, EG2: 10.52 ± 12.55 SANS: EG1: 23.58, EG2: 24.02 ± 18.10, CG: 24.82 ± 18.69 | MMSE: EG1: 26.21 ± 6.01, EG2: 25.91 ± 7.24, CG: 25.05 ± 7.25 | Married/not married: EG1: 51/53; EG2: 51/39; CG: 55/37. Occupation (professional specialty/ technical, sales and administrative support/ service (household, protective)/ all other occupations: EG1: 2/3/9/90; EG2: 0/1/7/82; CG: 0/3/6/83. Education (years): EG1: 10.24 ± 4.05; EG2: 9.38 ± 4.07; CG: 8.76 ± 4.54 | N. R. |
| [52] | 41; EG: 21, CG: 20 | EG: 11/10, CG: 8/12 | EG: 37.0 ± 9.7, CG: 36.1 ± 8.1 | Sch. (DSM-IV) | Illness length (years): EG: 11.2 ± 6.3, CG: 14.7 ± 7.9 Not evaluated with severity instruments | MMSE: EG: 27.3 ± 1.8, CG: 27.4 ± 1.7 | Education: high school EG: 57.1%, CG: 60.0%; College or above EG: 42.9%; CG: 40.0% Residence: with families EG: 90.5%, CG: 100%; alone EG: 9.5%, CG: 0% Marital status: single EG: 85.7%, CG: 85%; Married EG: 0%, CG: 10%; Divorced EG: 14.3%, CG: 5% | N. R. |
| [53] | 82, EG1: 25, EG2: 26, CG: 31 | EG1: 20/5, EG2: 22/4, CG: 20/11 | EG1: 41.40 ± 7.86, EG2: 41.50 ± 8.72, CG: 44.06 ± 8.40 | Sch. (DSM-V) | PANSS general: EG1: 35.96 ± 5.30, EG2: 34.23 ± 6.26, CG: 33.87 ± 4.65 | MoCA: EG1: 20.44 ± 2.02, EG2: 20.08 ± 1.98, CG: 19.97 ± 1.54 | Years of education: CG: 9.16 ± 2.72; EG1: 10.00 ± 2.74; EG2: 9.00 ± 3.16 | N. R. |
| [54] | 51, EG: 26; CG: 25 | EG: 15/11; CG: 19/06 | EG: 33.62 ± 7.22; CG: 32.92 ± 6.40 | Sch. (DSM-V) | CGI: EG: 4.62 ± 0.85, CG: 4.76 ± 1.01 SANS: EG: 47.76 ± 14.32, CG: 43.56 ± 14.72 SAPS: EG: 29.00 ± 12.87, CG: 24.72 ± 14.52 | N. R. | Years of education: EG: 12.54 (3.14); CG: 11.20 ± 4.13 Married: Single = EG: 8:18; CG: 10:15 | N. R. |
| [55] | 77, EG: 33, CG: 34 | EG: 15/18, CG: 13/21 | EG: 41.0 ± 10.3, CG: 42.5 ± 8.7 | Sch. (DSM-V) | PANSS: EG: 80.8 ± 12.6, CG: 76.6 ± 12.9 | N. R. | Education, years: EG: 13.3 ± 2.2; CG: 13.3 ± 1.8 Married: EG: 11.8%; CG: 9.1 Employed: EG: 26.5%; CG: 24.2% | N. R. |
| [56] | 27, EG: 15, CG: 12 | EG: 12/3, CG: 7/5 | EG: 28.33 ± 4.7, CG: 29.5 ± 8.2 | Sch. (DSM-IV) | SAPS: EG: 7.8 ± 2.8, CG: 6.6 ± 2.3 SANS: EG: 13.8 ± 5.2, CG: 10 ± 4.6 | N. R. | Years of education: EG: 12.54 ± 3.14; CG: 11.20 ± 4.13 | N. R. |
| [48] | 53, EG: 35, CG: 18 | EG: 94% male, EC: 18/0 | EG: 56.3 ± 6.2, GC: 55.7 ± 7.1 | Sch. or schizoaffective disorder (DSM-V) | BPRS total: EG: 39.2 ± 11.3, CG: 45.7 ± 14.2 | N. R. | Education (years): EG: 12.8 ± 1.6; CG: 12.8 ± 1.2 | N. R. |
| [57] | 18, EG: 4, CG:14 | Not reported | EG: 59.7 ± 13.0, CG: 50.3 ± 14.0 | Sch. (DSM-V) | PANSS: EG: 75.5 ± 13.1, CG: 71.0 ± 18.3 | Neurocognitive index: EG: 54.6 ± 21.6, CG: 44.5 ± 37.7 | N. R. | N. R. |
| [58] | 38, EG: 21, CG: 17 | EG: 16/5, CG: 15/2 | EG: 52.52 ± 6.66, CG: 53.18 ± 10.27 | Sch. (Not reported) | PANSS: EG: 62.38 ± 12.79, CG: 59.94 ± 8.99 | MATRICS: EG: 26.10 ± 12.48, CG: 25.47 ± 9.87 | N. R. | N. R. |
| [59] | 180, EG: 89, CG: 91 | EG: 53/36, CG: 50/41 | EG: 36.84 ± 11.83, CG: 47.90 ± 12.15 | Sch. (DSM-IV) | PANSS: 50.26 ± SD 11.81 | N. R. | Education years: EG: 14.23 ± 3.54; CG: 14.34 ± 3.94 | N. R. |
| [60] | 16, EG: 7, CG: 9 | EG: 4/3, CG: 8/1 | EG: 21.8 ± 3.8, CG: 23.5 ± 5.4 | Schizophrenia, schizoaffective disorder, depressed type, or schizophreniform disorder (DSM-IV) | 24-item BPRS: EG: 37.0 ± 8.9, CG: 44.4 ± 11.1 | Not reported | Married: Single: EG: 8:18; CG: 10:15 | Not reported. |
| [61] | 60, EG: 30, CG: 30 | EG: 15/15, CG: 17/13 | EG: 38.65 ± 10.11, CG: 39.00 ± 8.62 | Schizophrenia or schizoaffective disorder (DSM-IV-TR) | BPRS: EG: 48.08 ± 15.64, CG: 43.75 ± 10.61 | WCST (CR): EG: 51.36 ± 17.56, CG: 56.77 ± 16.56 | Years of education: EG: 13.35 ± 3.38; CG: 14.63 ± 2.123 | BDI: EG: 22.12 ± 10.02, CG: 20.71 ± 8.14 STAI: EG: 47.23 ± 8.02, CG:45.29 ± 10.17 |
| [62] | 41, EG: 20, CG: 21 | EG: 9/11, CG: 9/12 | EG: 21.62 ± 3.63; CG: 18.75 ± 3.89 | Schizophrenia: EG: 16, CG: 4; schizoaffective disorder: EG: 18, CG: 3 (DSM-V) | PANSS: EG: 112.65 ± 19.43, CG: 105.75 ± 11.33 | Not reported | Education (year): EG: 12.57 ± 2.04; CG: 11.95 ± 1.61 Employment experience (% yes): EG: 76.19%; CG: 80.00% | Not reported |
| [63] | 44, EG: 22, CG: 22 | EG: 10/12, CG: 10/12 | EG: 37.64 ± 8.23, CG: 36.68 ± 8.33 | Schizophrenia or schizoaffective disorder (DSM-IV) | PANSS positive symptoms: EG: 16.05 ± 6.48, 18.18 ± 7.11, PANSS negative symptoms: EG: 22.36 ± 9.65, CG: 21.82 ± 8.72 | WAIS-III total IQ: EG: 87.83 ± 14.06, 82.11 ± 8.36 | Years of education: EG: 12.55 ± 2.86; CG: 11.50 ± 2.37 | Not reported |
| [64] | 15, EG: 8, CG: 7 | EG1: 5/3CG: 7/0 | EG: 35.00 ± 9.87 CG: 29.86 ± 9.14 | Paranoid schizophrenia (ICD-10) | PANSS: EG: 72.88 ± 22.78, CG: 82.14 ± 7.31 | N. R. | N. R. | N. R. |
| [65] | 17, EG: 12, CG: 5 | N. R. | N. R. | Schizophrenia (DSM-V) | N. R. | N. R. | N. R. | N. R. |
| Reference/Design | Exercise Program | Control Condition | Compliance with the Intervention Program | Intervention Length | Frequency | Session Length | Intensity | Other Treatments | EF Dimension and Instrument |
|---|---|---|---|---|---|---|---|---|---|
| [49] RCT | Yoga (EG1): SVYASA, a program combining loosening, breathing exercises, various postures (sitting, supine, prone), and relaxation techniques (excluding meditation). The first 2 months guided by instructors; for the next 2 months, the patient’s caregivers were instructed to monitor the yoga therapy at home. Exercise group (EG2): adapted National Fitness Corps program, focusing on brisk walking, jogging, and postures in various positions (standing, sitting) with relaxation. | Waitlist | Drop-outs: 7 in yoga group, 14 in exercise group, and 4 in waitlist group. Final sample: 27 in yoga group, 17 in exercise group, and 22 in waitlist group. | 4 months | Not reported | 60 min | Not reported. | Antipsychotic (CPZ equivalents in mg/day): EG1: 335.0 ± 205.3 [400], EG2: 297.9 ± 150.9 [300], CG: 340.0 ± 172.4 [675] | ER: TRENDS |
| [50] Non-RCT | Yoga: supervised by a professor, combined postures (Asanas) and breathing exercises (Pranayama). Sessions started with chanting and warm-up, followed by diverse poses (standing, lying, prone, and sitting) designed to synchronize movement with breath. Saturdays featured sinus-cleansing practices (Kriya/Jalneti) for added benefits. | TAU | 89 participants drop out in different moments of yoga intervention. | 21 days | 6/week (no Sundays) | 60 min | Not reported. | All participants received conventional pharmacological and non-pharmacological treatment from their psychiatrists and therapists throughout the study. | CF: CNB in a web base interface WM: CNB in a web base interface similar to N-back ER: CNB in a web base interface |
| [51] RCT | Yoga (EG1): comprised postures, breathing and weekly nasal cleansing, by qualified instructors to groups of participants (1–5). Physical exercise (EG2): brisk walks, followed by jogging and directed aerobic exercises. The participants were advised to continue TAU, YT, or PE past the training period. By qualified instructors to groups of participants (1–5). | TAU | Dropout (n = 48) in the YT and PE groups: transportation difficulties (YT 2; PE 3; TAU 3), staying far away (YT 3; PE 2); not able to arise early (YT 5); symptoms aggravated (YT 2; PE 2); being transferred out of Delhi (YT 3; PE 1; TAU 3) | 21 days | 6/week (no Sundays, no public holidays) | 60 min | Not reported. | Not reported. | CF: CNB in a web base interface WM: CNB in a web base interface ER: CNB in a web base interface |
| [52] Non-RCT | Aerobic dance intervention: 5 min warm-up, 40 min of aerobic dance with a 5 min break and 10 min cool down. Simple movements choreographed by an occupational therapist. Motivational strategies were implemented. | Coloring and handwriting activities (text copies of 300 words) and attentional control. | In EG (n = 1) and in CG (n = 3), participants withdrew from the program because of unstable psychiatric symptoms. Average attendance EG = 73% and CG = 71%. | 3 months (38 sessions) | 3/week | 50–60 min | 52.8% HRR | No changes in antipsychotic medications between the previous 3 months | CF: TMT-B WM: Semantic Association of Verbal Fluency Test |
| [53] RCT | Aerobic exercise training (EG1): aerobic exercise by qualified instructors, music warm-up exercise (10 min) and walking on a treadmill at a speed of 6–9 kminm/h (30 min) followed by cool-down stretching (5 min). CCRT training (EG2): by experienced therapists at a ratio of one therapist to five participants, 30 exercise sequences that dynamically adjust the difficulty as the accuracy reaches 80%. | TAU | 14 individuals withdrew for personal reasons (Control 1, CAE 6, AE 7). Reasons: discharge before the trial started (CAE 1, AE 2); worsened symptoms (Control 1, AE 1); unwillingness to rush to the training room within the agreed-upon time (CAE 1; AE 2); not being able to complete computer operations (CAE 3); without a specified reason (CAE 1; AE 2). | 8 weeks | EG1: 5/week, EG2: 2/week | EG1: 45 min, EG2: 45 min | EG1: 50–70% HRR | Antipsychotics (FGA/SGA): EG1: 3/22, EG2: 2/24, CG: 3/28. Equivalent dose of chlorpromazine: EG1: 328.00 ± 96.91, EG2: 357.69 ± 102.66, CG: 374.19 ± 97.36 | I: SCWT |
| [54] RCT | Yoga: Most of the yoga sessions were individual sessions (a maximum of three subjects were taught together in a few sessions). Most of the subjects finished 20 sessions in 6 weeks. Few subjects finished in 4 weeks. | Waitlist | Yoga group: One move to another place; one discontinued intervention. Waitlist group: One could not be contacted. | 6 weeks (20 sessions) | 4–5/week | 60 min | Not reported | Antipsychotic: EG: 518.0 ± 329.05, CG: 434.0 ± 191.33 | SC: SOCRATIS TofM: story-based tasks SP: social cue recognition test ER: TRENDS |
| [55] RCT | Treatment-as-usual plus aerobic walking (TAW): The target dosage of the structured walking program, based on the American College of Sports Medicine guideline. The participants walked for 30 min after a 5 min warm-up. The schedule was flexible, and the participants could decide the number of days they would attend to achieve a feasible goal of 150 min per week, for example, 50 min sessions three/week. | TAU | During the 12-week trial period, one participant in the TAU group dropped out due to personal issues; two in the TAW group lacked motivation and withdrew consent. Finally, 33 (97.1%) participants in the TAU group and 31 (93.9%) in the TAW group completed the 12-week trial and posttrial assessment. | 12 weeks | 5/weeks | 30 min | 30–40% HRR | Aripiprazole or Ziprasidone: EG: 18.20%, CG: 11.80%; Olanzapine or Clozapine: EG: 51.5%, CG: 50.00%; Other antipsychotics: EG: 30.30%, CG: 38.2% | WM: Digit Sequencing Task (BACS) |
| [56] RCT | Yoga: a specific yoga therapy module for schizophrenia, by a professional yoga therapist at the Advanced Center for Yoga in NIMHANS for a period of 1 month. It consisted of loosening exercises, breathing practices, Suryanamaskāra, sitting and supine and prone posture Āsanas, along with Prāṇāyāma and relaxation techniques. | Waitlist | In the yoga group, all 15 patients completed baseline and follow-up assessments. The 16 patients who dropped out in the waitlist group did so primarily due to logistic reasons. | 1 month | Not reported | Not reported | Not reported | Not reported | ER: TRENDS |
| [48] RCT | Each session includes a 5 min warm-up and cool-down period, as well as stretching exercises. The walking duration gradually increases over the 12-week period. During weeks 1–2, veterans walked for 20 min per session; during weeks 3–4, they walked for 30 min per session; and from weeks 5–12, they walked for 40 min per session (the desired maximum outcome). The walking exercises were led by two research personnel trained on the study procedures by the PI and monitored for fidelity on a weekly basis. | Stretching exercise: 5 min warm-up and cool-down period of slow walking | One participant dropped out of the study after randomization and before completion of baseline testing, leaving 53 subjects available for data analyses. | 12 weeks | 3/week | 40 min | 60–70% HRR | Antipsychotic medication: atypical (EG: 83%; CG: 72%), typical (EG: 9%; CG: 16%) | WM: WAIS-IV letter-number sequencing test I: AX-CPT ER: Facial Emotion Identification Test TofM: The Awareness of Social Inference Test (TASIT–Part 2) |
| [57] RCT | Exercise intervention: One session, three phases: warm-up (15 min), aerobic exercise (30–40 min), and cool down (5 min). In the warm-up phase, the participants stretched and could talk to one another. In the aerobic exercise phase, the participants could choose which one activity they preferred: an ergometer and/or aerobics and/or Tai-chi. | TAU | The dropout rates in the TAU and exercise groups were 17.6% and 20%, respectively. | 8 weeks | 2/week | 60 min | Mild intensity | FGA (mg): EG: 246.4 ± 358.4, CG: 87.5 ± 143.6 SGA (mg): EG: 802.3 ± 589.4, CG: 1000.00 ± 516.4 Antipsychotic (mg): EG: 1048.7 ± 846.4, CG: 1087.5 ± 632.9 | CF: Cognitrax Basic Version |
| [59] RCT | Bike ergometer AET: Participants cycled consistently at lactate threshold intensity (2 mmol/L, slightly strenuous, talking possible). 5 min warm-up/cool down at 80% intensity. Lactate tests every 4 weeks, adjusted training intensity. | Exercises focused on flexibility, stability, balance, and relaxation. 5 min warm-up and cool-down at 80% intensity, without using lactate threshold for intensity definition. | 59.55% of the AET group and 57.14% of the FSBT group dropped out of the study during the six-month active study phase | 6 months | 3/week | 40 min 1–6° weeks, 45 min 7–12° weeks, 50 min 13–26° weeks | Slightly strenuous but should have still been able to talk without being short of breath. | Not reported | WM: Digit Span Test ER: Pictures of Facial Affect Recognition Test CF: TMT global |
| [58] RCT | Aerobic exercise: stationary bicycle ergometer. 20 min per session to a maximum of 45 min by increasing 5 min each week | Stretching and balance training | The final cohort of subjects who completed 12 weeks of treatment included nine in the AE group and six in the CON group. | 12 weeks | 3/weeks | 20–45 min | 50% HRR | Atypical Antipsychotics: EG: 14.00 ± 66.67, CG: 13.00 ± 76.47; Typical Antipsychotics: EG: 1.00 ± 4.76, CG: 2.00 ± 11.76; Both (Atypical and Typical): EG: 2.00 ± 9.52, CG: 1.00 ± 5.88; Antidepressants: EG: 6.00 ± 28.57, CG: 4.00 ± 23.53 | WM: MCCB SC: MCCB |
| [60] Non-RCT | Cognitive training and aerobic exercise: exercise videos approved by a certified personal trainer. Calisthenics (e.g., lunges, squats, pushups) and simple movement sequences at several levels of intensity, without resistance training. | Neurocognitive training and social cognitive training. Bridging group: discussions about how computerized training exercise could help. | Attendance at the CT sessions, 90% of these in-clinic sessions. For the exercise groups at the clinic, 95% attendance. Adherence with the at-home exercise, 92%. | 10 weeks | CG: 2/week EG: 2/week + 2/week | CG: 60 min EG: 150 min/week + 2 session (45 min) + 30 min at clinic | 60–80% HRR | Second-generation antipsychotic medication: 11 oral risperidone, three long-acting injectable risperidone, two aripiprazole, two with supplemental quetiapine | WM: MCCB SC: MCCB |
| [61] RCT | Outdoor cycling: (1) 15 min for setting goals for the day and safety education, (2) 10 min to warm-up exercise, 40 min of bike training, 10 min of cool-down exercise, (3) 15 min for discussion on achievement of day. | Occupational therapy | OC and OT groups 13.3% and 20%, respectively. Dropout rates did not vary significantly across intervention groups [χ2(1) = 0.480, p = 0.488]. | 16 weeks | N. R. | 40 min | Not reported | Second-generation antipsychotic and regular visits with the treating psychiatrist: all participants. | CF: WCST |
| [62] RCT | Aerobic exercise: individual and group programs by occupational therapists. In the group AE program, exercise videos. Squats, repeated lateral movements, arm and leg movements, and deep breathing. | TAU | The TAU + AE patients completed an average of 85.75% (mean = 20.58 sessions, standard deviation = 2.63) of the AE sessions over 12 weeks. | 12 weeks | 2/week | 60 min | 60–80% HRR | Antipsychotic | WM: BACS |
| [64] RCT | Endurance training: outdoor walking, Nordic walking, or running. | Occupational therapy | 13 dropout = 10 patients because of early discharge from hospital and 3 patients because of various other reasons. | >4 weeks (22 sessions) | 3/week | 20–30 min | 85% MHR | N.R. | WM: digit span of the German adaption of the revised Wechsler Memory Scale. CF: a computer-assisted card-sorting procedure (CKV). |
| [65] RCT | Guided intervention in physical exercise: walking (aerobic resistance). | Typical daily physical activity (e.g., shopping at the supermarket), without guidance or incentives. | Retention rate: 100% | 12 weeks | 3/week | 60 min | 64–76% MHR | N. R. | Inhibition: Stroop Color and Word test (SCWT). CF: Wisconsin Card Sorting Test (WCST); TMT-B WM: Verbal Fluency; digit span backwards subtest (WAIS-III). |
| Certainty Assessment | № of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirect Evidence | Imprecision | Other Considerations | Exercise | Control | Relative (95% CI) | Absolute (95% CI) | ||
| Emotion Recognition | ||||||||||||
| 4 | RCT | Not serious | Serious a | Not serious | Not serious | none | 106 | 66 | - | ES 0.299 (0.062–0.535) | ⨁⨁⨁◯ Moderate a | IMPORTANT |
| Working Memory | ||||||||||||
| 8 | RCT | Not serious | Not serious | Not serious | Not serious | none | 122 | 106 | - | ES 0.132 (0.005–0.523) | ⨁⨁⨁⨁ High | IMPORTANT |
| Inhibition | ||||||||||||
| 3 | RCT | Not serious | Not serious | Not serious | Not serious | none | 98 | 54 | - | ES 0.156 (0.173–0.484) | ⨁⨁⨁⨁ High | IMPORTANT |
| Cognitive flexibility | ||||||||||||
| 4 | RCT | Not serious | Not serious | Not serious | Not serious | none | 130 | 123 | - | ES 0.171 (0.245–0.586) | ⨁⨁⨁⨁ High | IMPORTANT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Romero, N.; Campos-Jara, C.; Pesce, C.; Araya Sierralta, S.; Cerda-Vega, E.; Ramirez-Campillo, R.; Campos-Jara, R.; Martínez-Salazar, C.; Arellano-Roco, C.; Hernández-Cifuentes, V.; et al. Effects of Physical Exercise on Executive Function in Schizophrenia: Systematic Review and Meta-Analysis. Sports 2025, 13, 123. https://doi.org/10.3390/sports13040123
Pérez-Romero N, Campos-Jara C, Pesce C, Araya Sierralta S, Cerda-Vega E, Ramirez-Campillo R, Campos-Jara R, Martínez-Salazar C, Arellano-Roco C, Hernández-Cifuentes V, et al. Effects of Physical Exercise on Executive Function in Schizophrenia: Systematic Review and Meta-Analysis. Sports. 2025; 13(4):123. https://doi.org/10.3390/sports13040123
Chicago/Turabian StylePérez-Romero, Nuria, Christian Campos-Jara, Caterina Pesce, Sergio Araya Sierralta, Enrique Cerda-Vega, Rodrigo Ramirez-Campillo, Rodrigo Campos-Jara, Cristian Martínez-Salazar, Cristián Arellano-Roco, Victoria Hernández-Cifuentes, and et al. 2025. "Effects of Physical Exercise on Executive Function in Schizophrenia: Systematic Review and Meta-Analysis" Sports 13, no. 4: 123. https://doi.org/10.3390/sports13040123
APA StylePérez-Romero, N., Campos-Jara, C., Pesce, C., Araya Sierralta, S., Cerda-Vega, E., Ramirez-Campillo, R., Campos-Jara, R., Martínez-Salazar, C., Arellano-Roco, C., Hernández-Cifuentes, V., & Contreras-Osorio, F. (2025). Effects of Physical Exercise on Executive Function in Schizophrenia: Systematic Review and Meta-Analysis. Sports, 13(4), 123. https://doi.org/10.3390/sports13040123