Quality of Life and Breast Cancer: How Can Mind–Body Exercise Therapies Help? An Overview Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection and Inclusion Criteria
2.3. Data Extraction and Quality Assessment
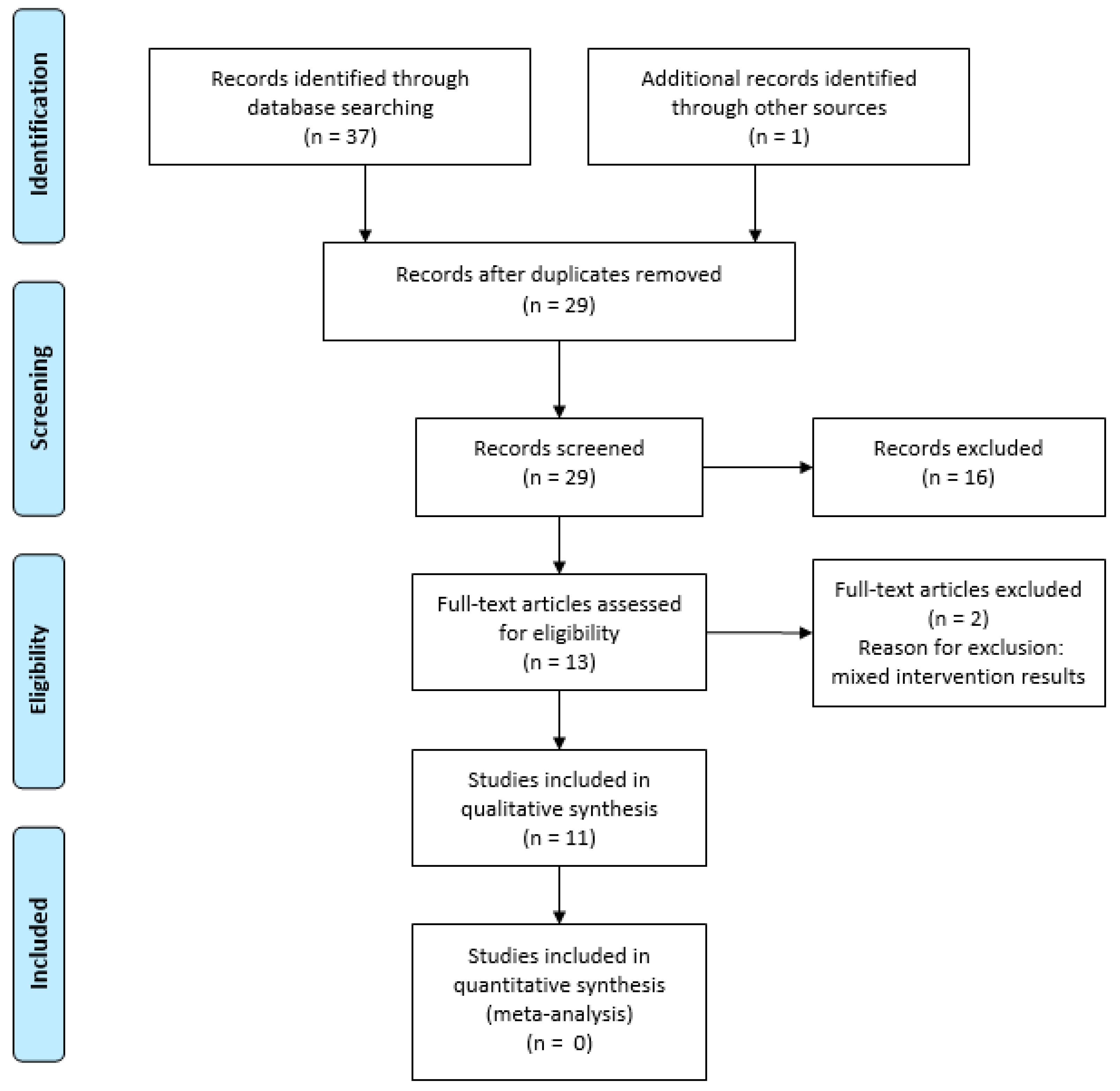
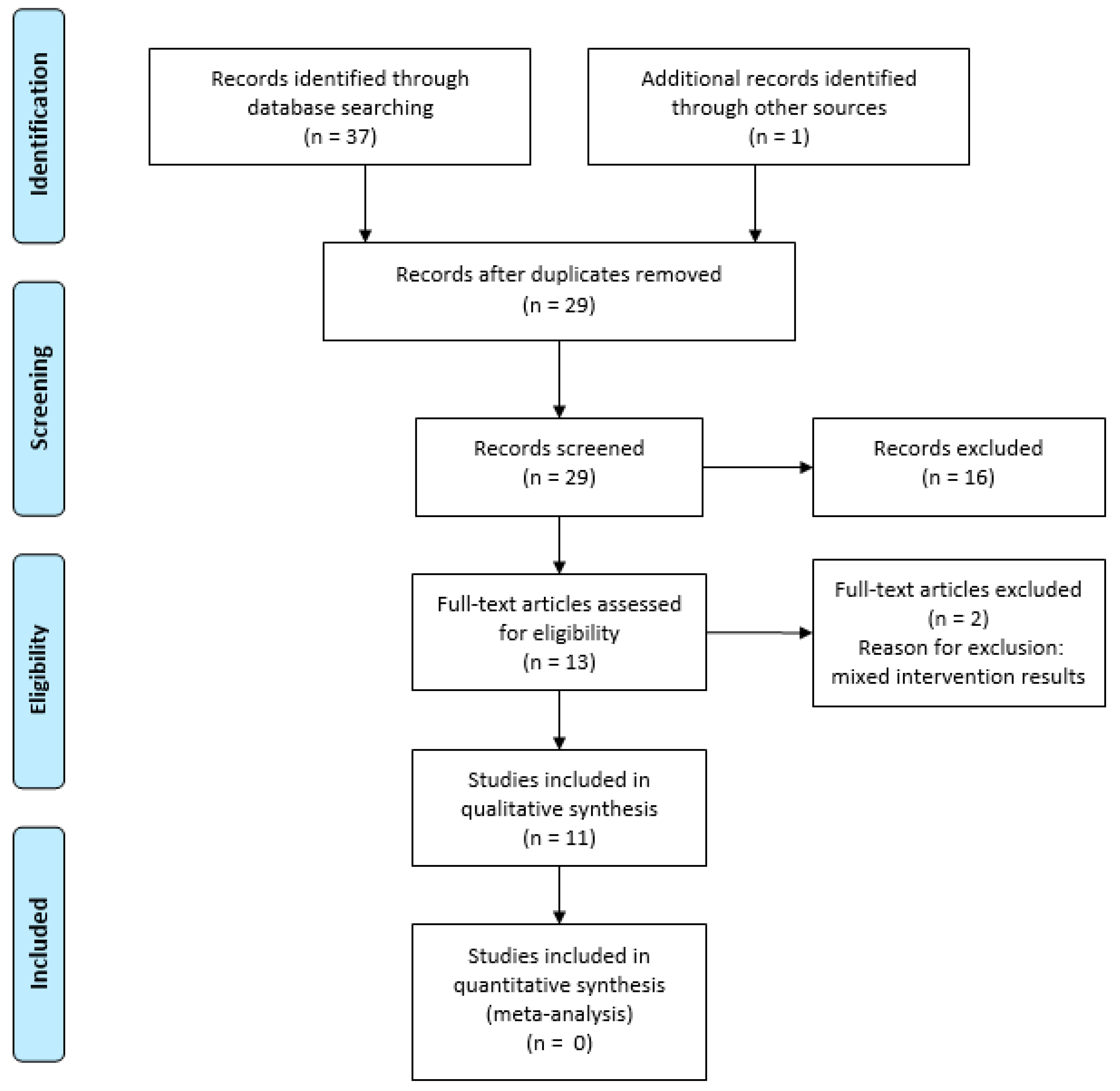
3. Results
3.1. Characteristics of Mind–Body Therapy Studies
3.2. Methodological Quality of Included Reviews
3.3. Program Features and Adherence
3.4. Effect of Mind–Body Therapies on Quality of Life
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dodd, M.J.; Cho, M.H.; Cooper, B.A.; Miaskowski, C. The effect of symptom clusters on functional status and quality of life in women with breast cancer. Eur. J. Oncol. Nurs. 2010, 14, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Paterson, C.L.; Lengacher, C.A.; Donovan, K.A.; Kip, K.E.; Tofthagen, C.S. Body image in younger breast cancer survivors: A systematic review. Cancer Nurs. 2016, 39, E39–E58. [Google Scholar] [CrossRef] [PubMed]
- Deng, G.; Cassileth, B. Complementary or alternative medicine in cancer care—Myths and realities. Nat. Rev. Clin. Oncol. 2013, 10, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Horneber, M.; Bueschel, G.; Dennert, G.; Less, D.; Ritter, E.; Zwahlen, M. How many cancer patients use complementary and alternative medicine: A systematic review and metaanalysis. Integr. Cancer Ther. 2012, 11, 187–203. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.M.; Bloom, B.; Nahin, R.L. Complementary and alternative medicine use among adults and children: United States, 2007. Natl. Health Stat. Rep. 2008, 12, 1–23. [Google Scholar]
- Pilkington, K. Yoga. 2015. Available online: http://www.cam-cancer.org/CAM-Summaries/Mind-body-interventions/Yoga (accessed on 10 August 2017).
- Lee, M.S.; Oh, B.; Ernst, E. Qigong for healthcare: An overview of systematic reviews. JRSM Short Rep. 2011, 2, 7. [Google Scholar] [CrossRef] [PubMed]
- McCall, M.C.; Ward, A.; Roberts, N.W.; Heneghan, C. Overview of systematic reviews: Yoga as a therapeutic intervention for adults with acute and chronic health conditions. J. Evid. Based Complement. Altern. Med. 2013, 2013, 945895. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S. Meditative movement therapies and health-related quality-of-life in adults: A systematic review of meta-analyses. PLoS ONE 2015, 10, e0129181. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011; Volume 4. [Google Scholar]
- Sarrami-Foroushani, P.; Travaglia, J.; Debono, D.; Clay-Williams, R.; Braithwaite, J. Scoping meta-review: Introducing a new methodology. Clin. Trans. Sci. 2015, 8, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Devane, D.; Begley, C.M.; Clarke, M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of amstar: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shneerson, C.; Taskila, T.; Gale, N.; Greenfield, S.; Chen, Y.F. The effect of complementary and alternative medicine on the quality of life of cancer survivors: A systematic review and meta-analyses. Complement. Ther. Med. 2013, 21, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Stan, D.L.; Collins, N.M.; Olsen, M.M.; Croghan, I.; Pruthi, S. The evolution of mindfulness-based physical interventions in breast cancer survivors. J. Evid. Based Complement. Altern. Med. 2012, 2012, 758641. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Pittler, M.H.; Ernst, E. Is tai chi an effective adjunct in cancer care? A systematic review of controlled clinical trials. Support. Care Cancer 2007, 15, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.Q.; Yang, K.H.; Wang, Y.L.; Zhang, L.P.; Liang, H.Q. Could yoga practice improve treatment-related side effects and quality of life for women with breast cancer? A systematic review and meta-analysis. Asia Pac. J. Clin. Oncol. 2017, 13, e79–e95. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Yang, K.; Shi, X.; Liang, H.; Zhang, F.; Lv, Q. Tai chi chuan exercise for patients with breast cancer: A systematic review and meta-analysis. J. Evid. Based Complement. Altern. Med. 2015, 2015, 535237. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Yang, K.H.; Tian, J.H.; Wang, C.M. Effects of yoga on psychologic function and quality of life in women with breast cancer: A meta-analysis of randomized controlled trials. J. Altern. Complement. Med. 2012, 18, 994–1002. [Google Scholar] [CrossRef] [PubMed]
- Bleakley, K.; Stinson, M. Complementary and alternative therapies: Do they improve quality of life for women with breast cancer? Phys. Ther. Rev. 2011, 16, 96–105. [Google Scholar] [CrossRef]
- Buffart, L.M.; van Uffelen, J.G.; Riphagen, I.I.; Brug, J.; van Mechelen, W.; Brown, W.J.; Chinapaw, M.J. Physical and psychosocial benefits of yoga in cancer patients and survivors, a systematic review and meta-analysis of randomized controlled trials. BMC Cancer 2012, 12, 559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, H.; Lange, S.; Klose, P.; Paul, A.; Dobos, G. Yoga for breast cancer patients and survivors: A systematic review and meta-analysis. BMC Cancer 2012, 12, 412. [Google Scholar] [CrossRef] [PubMed]
- Harder, H.; Parlour, L.; Jenkins, V. Randomised controlled trials of yoga interventions for women with breast cancer: A systematic literature review. Support. Care Cancer 2012, 20, 3055–3064. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.S.; Balk, J.L. Yoga and quality-of-life improvement in patients with breast cancer: A literature review. Int. J. Yoga Ther. 2012, 22, 95–99. [Google Scholar]
- Sawyer, A. Complementary exercise and quality of life in patients with breast cancer. Br. J. Nurs. 2014, 23, S18–S23. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.C.; Bauer, I.E. A systematic review of randomised control trials on the effects of yoga on stress measures and mood. J. Psychiatr. Res. 2015, 68, 270–282. [Google Scholar] [CrossRef] [PubMed]
- Daley, A. Exercise and depression: A review of reviews. J. Clin. Psychol. Med. Set. 2008, 15, 140. [Google Scholar] [CrossRef] [PubMed]
- Ray, U.S.; Pathak, A.; Tomer, O.S. Hatha yoga practices: Energy expenditure, respiratory changes and intensity of exercise. J. Evid. Based Complement. Altern. Med. 2011, 2011, 241294. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, D.B.; Saper, R.B.; Aronson, M.D.; Sullivan, D.J. Overview of Yoga. 2016. Available online: https://www.uptodate.com/contents/overview-of-yoga (accessed on 10 October 2017).
- Kneis, S.; Wehrle, A.; Freyler, K.; Lehmann, K.; Rudolphi, B.; Hildenbrand, B.; Bartsch, H.H.; Bertz, H.; Gollhofer, A.; Ritzmann, R. Balance impairments and neuromuscular changes in breast cancer patients with chemotherapy-induced peripheral neuropathy. Clin. Neurophysiol. 2016, 127, 1481–1490. [Google Scholar] [CrossRef] [PubMed]
- Vardar Yagli, N.; Sener, G.; Arikan, H.; Saglam, M.; Inal Ince, D.; Savci, S.; Calik Kutukcu, E.; Altundag, K.; Kaya, E.B.; Kutluk, T.; et al. Do yoga and aerobic exercise training have impact on functional capacity, fatigue, peripheral muscle strength, and quality of life in breast cancer survivors? Integr. Cancer Ther. 2015, 14, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J. The use of randomized control trials in complementary therapies: Exploring the issues. J. Adv. Nurs. 2000, 32, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Smithson, J.; Britten, N.; Paterson, C.; Lewith, G.; Evans, M. The experience of using complementary therapies after a diagnosis of cancer: A qualitative synthesis. Health 2012, 16, 19–39. [Google Scholar] [CrossRef] [PubMed]
- Littman, A.J.; Tang, M.T.; Rossing, M.A. Longitudinal study of recreational physical activity in breast cancer survivors. J. Cancer Surviv. 2010, 4, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Husebø, A.M.L.; Dyrstad, S.M.; Søreide, J.A.; Bru, E. Predicting exercise adherence in cancer patients and survivors: A systematic review and meta-analysis of motivational and behavioural factors. J. Clin. Nurs. 2013, 22, 4–21. [Google Scholar] [CrossRef] [PubMed]
- Lally, P.; van Jaarsveld, C.H.M.; Potts, H.W.W.; Wardle, J. How are habits formed: Modelling habit formation in the real world. Eur. J. Soc. Psychol. 2010, 40, 998–1009. [Google Scholar] [CrossRef]
- Raghavendra, R.M.; Kodaganur, S.G.; Srinath, B.S.; Patil, S.; Shashidhara, P.; Diwakar, R.B.; Rao, N.K.; Ajaikumar, B.S.; Prashanth, J.; Chidambaramurthy, K.N.; et al. Adherence to yoga practice improves symptom control and quality of life in breast cancer patients undergoing conventional treatment. J. Clin. Oncol. 2012, 30, e11511. [Google Scholar]
- Speed-Andrews, A.E.; Stevinson, C.; Belanger, L.J.; Mirus, J.J.; Courneya, K.S. Predictors of adherence to an iyengar yoga program in breast cancer survivors. Int. J. Yoga 2012, 5, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Galliford, M.; Robinson, S.; Bridge, P.; Carmichael, M. Salute to the sun: A new dawn in yoga therapy for breast cancer. J. Med. Radiat. Sci. 2017, 64, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Wanchai, A. Complementary and alternative medicine use among women with breast cancer: A systematic review. Clin. J. Oncol. Nurs. 2010, 14, E45–E55. [Google Scholar] [CrossRef] [PubMed]
- Pollock, M.; Fernandes, R.M.; Becker, L.A.; Featherstone, R.; Hartling, L. What guidance is available for researchers conducting overviews of reviews of healthcare interventions? A scoping review and qualitative metasummary. Syst. Rev. 2016, 5, 190. [Google Scholar] [CrossRef] [PubMed]
- Larkey, L.; Jahnke, R.; Etnier, J.; Gonzalez, J. Meditative movement as a category of exercise: Implications for research. J. Phys. Act. Health 2009, 6, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. Grade guidelines: 5. Rating the quality of evidence—Publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Search | Database | Search Terms | Limitations | Identified Titles |
|---|---|---|---|---|
| #1 | EBSCO * | Breast cancer | January 2007–March 2017 Abstract English language | 210,484 |
| #2 | EBSCO | Review | January 2007–March 2017 Abstract English language | 2,233,944 |
| #3 | EBSCO | Quality of life | January 2007–March 2017 Abstract English language | 414,926 |
| #4 | EBSCO | #1 AND #2 AND #3 | January 2007–March 2017 Abstract English language | 1319 |
| #5 | EBSCO | Yoga | January 2007–March 2017 Abstract English language | 16,772 |
| #6 | EBSCO | Tai chi | January 2007–March 2017 Abstract English language | 3269 |
| #7 | EBSCO | Qigong | January 2007–March 2017 Abstract English language | 1201 |
| #8 | EBSCO | #5 OR #6 OR #7 | January 2007–March 2017 Abstract English language | 20,514 |
| #9 | EBSCO | #4 AND #8 | January 2007–March 2017 Abstract English language | 37 |
| Author (Year) | Cancer Site Age Treatment Status | Mind–Body Intervention | Outcome | Study Designs Number of Studies (N) | Main Results |
|---|---|---|---|---|---|
| Bleakley & Stinson (2011) [21] | Breast 18–70 During and after treatment | Yoga Visualization Therapeutic massage Guided imagery Relaxation | Global QoL | RCT N = 4 Non-RCT N = 3 Cross-sectional N = 1 | Four out of eight studies concluded that body–mind therapies had a positive effect on patients’ QoL. |
| Buffart et al. (2012) ** [22] | Breast 44–63 During and after treatment | Yoga | Global QoL HRQoL | RCT N = 13 | Yoga had a large beneficial effect on anxiety and depression, a moderate but significant effect on HRQoL and fatigue and no significant effects on physical function. |
| Cramer et al. (2012) ** [23] | Breast 44–63 During and after treatment | Yoga | Global QoL | RCT N = 10 | Yoga had a short-term effect of moderate size on global QoL, and a short-term effect of small size on functional, social and spiritual quality of life. No evidence for longer-term effects of yoga in breast cancer patients and survivors were found. |
| Harder et al. (2012) * [24] | Breast 45-63 During and after treatment | Yoga | Global QoL | RCT N = 18 | Yoga had moderate-to-large effects on global and emotional QoL. The effect of yoga was greatest among patients with most yoga classes. |
| Lee et al. (2007) * [17] | Breast 30–78 During treatment | Tai Chi Chuan | HRQoL | RCT N = 3 Non-RCT N = 1 | Positive effect of tai chi chuan was detected in self-esteem. |
| Levine & Balk (2012) [25] | Breast n.r. During and after treatment | Yoga | Global QoL | RCT N = 8 Non-RCT N = 2 | Positive effects on global QoL, on symptoms of illness and treatment side-effects. Reduced fatigue and improved sleep quality, and positive results in physical, social and functional adaptation. |
| Pan et al. (2015) ** [19] | Breast 49–65 During treatment | Tai Chi Chuan | Global QoL HRQoL | RCT N = 9 | Tai chi chuan led to no substantial improvement in HRQoL, or global HRQoL. |
| Pan et al. (2017) ** [18] | Breast 30–70 During treatment | Yoga | HRQoL | RCT N = 16 | Yoga significantly improved overall HRQoL but had limited effect on physical well-being. Intervention duration >3 months showed better QoL. |
| Shneerson et al. (2013) ** [15] | Breast ≥18 After treatment | Yoga Qigong Meditation Mindfulness | Global QoL | RCT N = 13 | Yoga had significant effects on global and mental QoL, but not on physical QoL. One study found significant effect of qigong on all QoL domains. |
| Stan et al. (2012) [16] | Breast n.r. After treatment | Yoga Tai Chi Chuan Qigong | Global QoL | RCT N = 23 Non-RCT N = 2 One-arm pilot N = 10 | Yoga had statistically significant or trending toward significant effects. No strong evidence was found for effect from tai chi chuan and qigong. |
| Zhang et al. (2012) ** [20] | Breast ≥30 years old During treatment | Yoga | Global QoL | RCT N = 6 | Yoga resulted in a statistically significant effect. |
| Domain 1 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | AMSTAR Score 4 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | ||||||||||||
| Bleakley & Stinson (2011) [21] | Yes | No | Yes | No | No | Yes | Yes | Yes | No | No | No | 5 |
| Buffart et al. (2012) [22] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | No | Yes | 8 |
| Cramer et al. (2012) [23] | Yes | Yes | Yes | CA 2 | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
| Harder et al. (2012) [24] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 8 |
| Lee et al. (2007) [17] | Yes | Yes | Yes | Yes | No | Yes | Yes | No | No | No | No | 6 |
| Levine et al. (2012) [25] | Yes | CA | Yes | No | No | No | No | No | Yes | No | No | 3 |
| Pan et al. (2015) [19] | Yes | Yes | Yes | CA | No | Yes | Yes | Yes | Yes | No | Yes | 8 |
| Pan et al. (2017) [18] | Yes | Yes | Yes | CA | No | Yes | Yes | Yes | Yes | No | Yes | 8 |
| Shneerson et al. (2013) [15] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
| Stan et al. (2012) [16] | Yes | Yes | Yes | Yes | No | Yes | No | Yes | No | No | No | 6 |
| Zhang et al. (2012) [20] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | NA 3 | Yes | 8 |
| Domain total score across studies | 11 | 9 | 11 | 3 | 0 | 10 | 9 | 9 | 7 | 2 | 7 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Husebø, A.M.L.; Husebø, T.L. Quality of Life and Breast Cancer: How Can Mind–Body Exercise Therapies Help? An Overview Study. Sports 2017, 5, 79. https://doi.org/10.3390/sports5040079
Husebø AML, Husebø TL. Quality of Life and Breast Cancer: How Can Mind–Body Exercise Therapies Help? An Overview Study. Sports. 2017; 5(4):79. https://doi.org/10.3390/sports5040079
Chicago/Turabian StyleHusebø, Anne Marie Lunde, and Tormod Lunde Husebø. 2017. "Quality of Life and Breast Cancer: How Can Mind–Body Exercise Therapies Help? An Overview Study" Sports 5, no. 4: 79. https://doi.org/10.3390/sports5040079
APA StyleHusebø, A. M. L., & Husebø, T. L. (2017). Quality of Life and Breast Cancer: How Can Mind–Body Exercise Therapies Help? An Overview Study. Sports, 5(4), 79. https://doi.org/10.3390/sports5040079