Exertional Rhabdomyolysis after an Extreme Conditioning Competition: A Case Report

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Case Report
3. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Bergeron, M.F.; Nindl, B.C.; Deuster, P.A.; Baumgartner, N.; Kane, S.F.; Kraemer, W.J.; Sexauer, L.R.; Thompson, W.R.; O’Connor, F.G. Consortium for Health and Military Performance and American College of Sports Medicine consensus paper on extreme conditioning programs in military personnel. Curr. Sports Med. Rep. 2011, 10, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Tibana, R.A.; de Almeida, L.M.; Frade de Sousa, N.M.; Nascimento Dda, C.; Neto, I.V.; de Almeida, J.A.; de Souza, V.C.; Lopes Mde, F.; Nobrega Ode, T.; Vieira, D.C.; et al. Two Consecutive Days of Crossfit Training Affects Pro and Anti-inflammatory Cytokines and Osteoprotegerin without Impairments in Muscle Power. Front. Physiol. 2016, 7, 260. [Google Scholar] [CrossRef] [PubMed]
- Tibana, R.A.; Farias, D.L.; Nascimento, D.C.; Da Silva-Grigoletto, M.E.; Prestes, J. Relação da força muscular com o desempenho no levantamento olímpico em praticantes de CrossFit®. Rev. Andal. Med. Deporte 2016, 11, 84–88. [Google Scholar] [CrossRef]
- Tibana, R.A.; Almeida, L.A.; Prestes, J. Crossfit® riscos ou benefícios? O que sabemos até o momento? Rev. Bras. Cienc. Mov. 2015, 23, 182–185. [Google Scholar] [CrossRef]
- Rawson, E.S.; Clarkson, P.M.; Tarnopolsky, M.A. Perspectives on Exertional Rhabdomyolysis. Sports Med. 2017, 47 (Suppl. 1), 33–49. [Google Scholar] [CrossRef] [PubMed]
- Chavez, L.O.; Leon, M.; Einav, S.; Varon, J. Beyond muscle destruction: A systematic review of rhabdomyolysis for clinical practice. Crit. Care 2016, 20, 135. [Google Scholar] [CrossRef] [PubMed]
- Pearcey, G.E.; Bradbury-Squires, D.J.; Power, K.E.; Behm, D.G.; Button, D.C. Exertionalrhabdomyolysis in an acutely detrained athlete/exercise physiology professor. Clin. J. Sport Med. 2013, 23, 496–498. [Google Scholar] [CrossRef] [PubMed]
- Lozowska, D.; Liewluck, T.; Quan, D.; Ringel, S.P. Exertional rhabdomyolysis associated with high intensity exercise. Muscle Nerve 2015, 52, 1134–1135. [Google Scholar] [CrossRef] [PubMed]
- Aynardi, M.C.; Jones, C.M. Bilateral upper arm compartment syndrome after a vigorous cross-training workout. J. Shoulder Elbow Surg. 2016, 25, e65–e67. [Google Scholar] [CrossRef] [PubMed]
- Hummel, K.; Gregory, A.; Desai, N.; Diamond, A. Rhabdomyolysis in adolescent athletes: Review of cases. Phys. Sportsmed. 2016, 44, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Meyer, M.; Sundaram, S.; Schafhalter-Zoppoth, I. Exertional and CrossFit-Induced Rhabdomyolysis. Clin. J. Sport Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Honda, S.; Kawasaki, T.; Kamitani, T.; Kiyota, K. Rhabdomyolysis after High Intensity Resistance Training. Intern. Med. 2017, 56, 1175–1178. [Google Scholar] [CrossRef] [PubMed]
- Hadeed, M.J.; Kuehl, K.S.; Elliot, D.L.; Sleigh, A. Exertional Rhabdomyolysis after Crossfit Exercise Program. Med. Sci. Sports Exerc. 2011, 45, 224–225. [Google Scholar] [CrossRef]
- Wagner, M.; LeNorman, D.; Dooley, A.; Rollins, L. Recurrent Rhabdomyolysis and Extreme Exercise—A Case Study. J. Sports Med. Allied Health Sci. 2015, 2, 3. [Google Scholar] [CrossRef]
- Torres, P.A.; Helmstetter, J.A.; Kaye, A.M.; Kaye, A.D. Rhabdomyolysis: Pathogenesis, diagnosis, and treatment. Ochsner J. 2015, 15, 58–69. [Google Scholar] [PubMed]
- Cervellin, G.; Comelli, I.; Lippi, G. Rhabdomyolysis: Historical background, clinical, diagnostic and therapeutic features. Clin. Chem. Lab. Med. 2010, 48, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.Y. Rhabdomyolysis: A review of the literature. Neth. J. Med. 2009, 67, 272–283. [Google Scholar] [PubMed]
- Elsayed, E.F.; Reilly, R.F. Rhabdomyolysis: A review, with emphasis on the pediatric population. Pediatr. Nephrol. 2010, 25, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Schwaber, M.J.; Liss, H.P.; Steiner, I.; Brezis, M. Hazard of sauna use after strenuous exercise. Ann. Intern. Med. 1994, 120, 441–442. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, J.; Kim, S.; Ryu, H.Y.; Cha, K.S.; Sung, D.J. Exercise-induced rhabdomyolysis mechanisms and prevention: A literature review. J. Sport Health Sci. 2016, 5, 324–333. [Google Scholar] [CrossRef]
- Peake, J.M.; Neubauer, O.; Della Gatta, P.A.; Nosaka, K. Muscle damage and inflammation during recovery from exercise. J. Appl. Physiol. (1985) 2017, 22, 559–570. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors | Subject | Physical Status | Protocol of ECP |
|---|---|---|---|
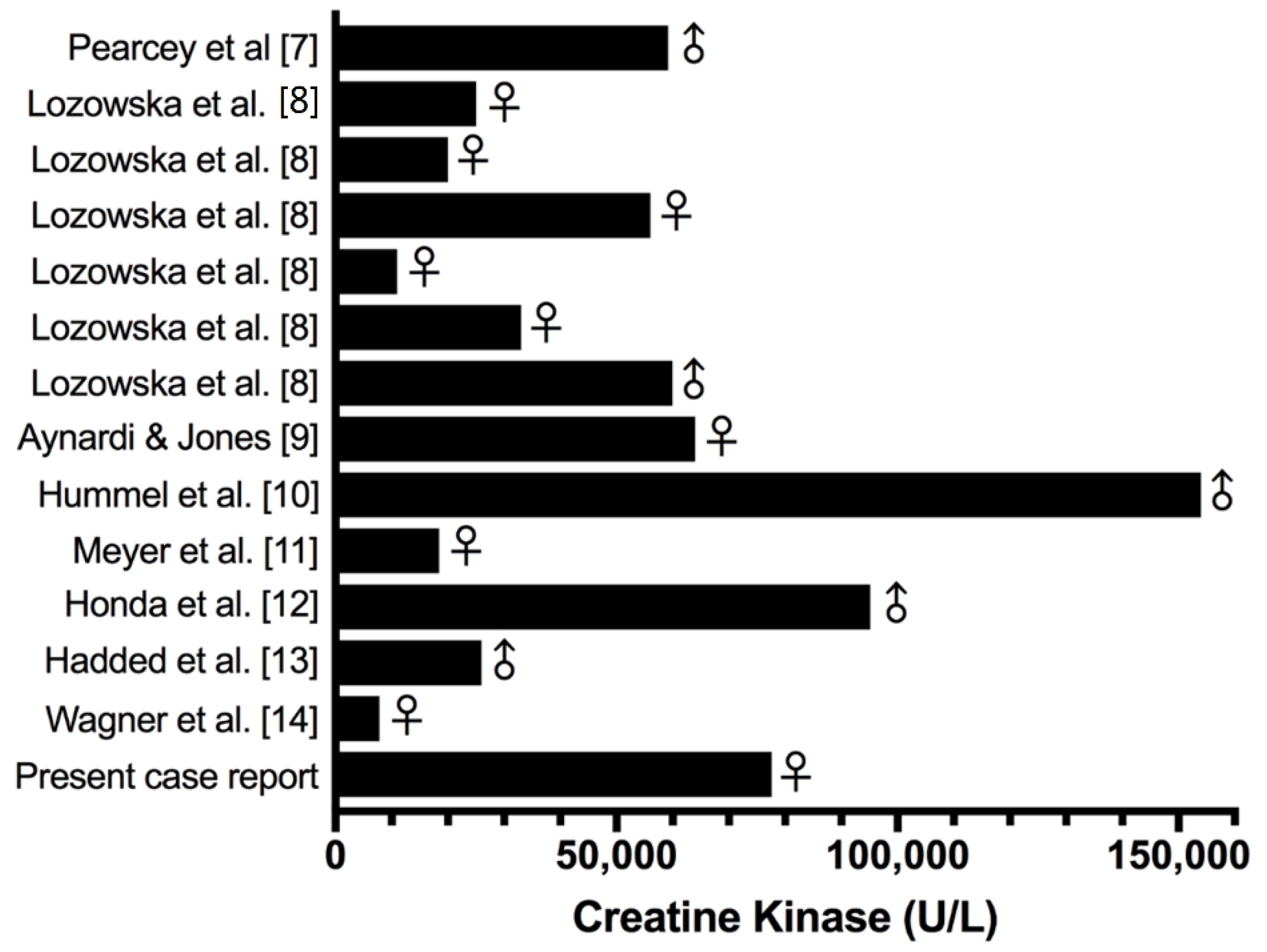
| Pearcey et al. [7] | Man | Athlete who was acutely trained (approximately 3 months). | 48 alternating sets (60 s duration) of push-up and pull-up variations. The subject performed the maximum number of repetitions possible of push-ups or pull-ups in each set. The total exercise duration was 48 min. The subject performed approximately 400 push-ups and approximately 200 pull-ups in 48 min. |
| Lozowska et al. [8] | Five of 6 patients were women | Three of the 6 patients were very physically fit before experiencing rhabdomyolysis, having participated in CrossFit for months to years. The remaining 3 patients were less fit and sustained rhabdomyolysis after their first encounter with CrossFit. | Non-informed. |
| Aynardi & Jones [9] | A 43-year old, African American female | She was healthy overall and had been active in multiple gym-related exercise programs over the past 10 years. | The ECP consisted of a standard warm-up followed by 3 sets of chin-ups that were performed until “failure” lasting approximately 20 min. |
| Hummel et al. [10] | A 15-year-old previously healthy male | Non-informed. | Intense CrossFit® workout. |
| Meyer et al. [11] | A previously healthy 31-year-old woman | She was exercising regularly 4 times per week, performing pushups, running, and other physical workouts. | The subject denied recent trauma or illness, but reported performing a variety of high intensity exercises such as pushups, plyometrics, and weightlifting at CrossFit. |
| Honda et al. [12] | A previously healthy 37-year-old man | He had exercised regularly but had never performed such intense training before. | Intense exercise training that included 100 pushups, 100 exercises using a 20-kg dumbbell, 50 lifts using a 10-kg weight. |
| Hadded et al. [13] | Man | He reports having had 5 previous days of exercise but did not involve CrossFit type training. | Non-informed. |
| Wagner et al. [14] | Woman | A healthy 21-year-old Caucasian female was participating in an organized, extreme exercise workout session conducted at a fitness center. | The exercise session consisting of performing a designated number of pushups in one minute. The protocol dictated 5 pushups in the first minute, 10 in the second, and adding 5 pushups each minute until participants can no longer continue. She recalls completing 6 rounds of increasing repetitions in each minute, thereby performing 105 pushups in 6 min. |
| Schedule | Day 1 | Day 2 |
|---|---|---|
| Workout 1 2:00 p.m. | 21 chest-to-bar pull-ups 21 thrusters (40 kg) 9 chest-to-bar pull-ups 9 thrusters (40 kg) | - |
| Workout 2 05:00 p.m. | 60 GHD sit ups (unaccustomed exercise) 15 toes-to-bar | - |
| Workout 3 1:00 p.m. | - | 1 RM of squat snatch + overhead squat |
| Workout 4 04:00 p.m. | - | AMRAP during 5 min of strict handstand push-ups |
| Workout 5 5:30 p.m. | - | 40 deadlifts (45 kg) 20 kettlebells clean and jerks (24 kg) 5 bar muscle-ups |
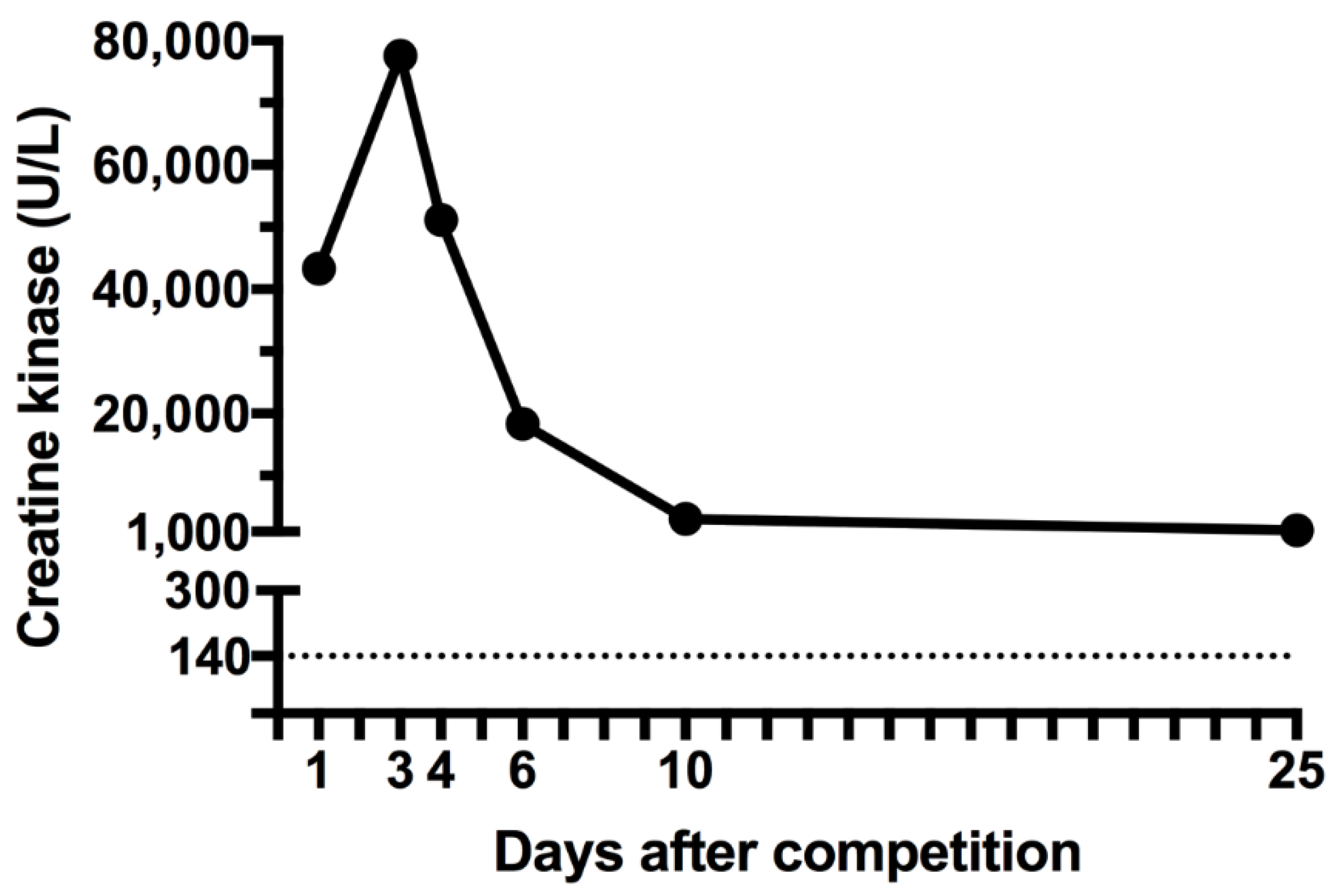
| Biomarkers | Reference Values | 1st Day Post-ECC | 3rd Day Post-ECC | 4th Day Post-ECC | 6th Day Post-ECC | 6th Day Post-ECC | 10th Day Post-ECC | 25th Day Post-ECC |
|---|---|---|---|---|---|---|---|---|
| Creatine kinase (CK) (U/L) | 26–140 | 43.322 | 77590 | 51.195 | 18.347 | 18.287 | 3034 | 1257 |
| Lactic dehydrogenase (LDH) (U/L) | 240–248 | - | - | 1.835 | 555 | 607 | - | - |
| Myoglobin (ng/mL) | 10–46 | - | 1350 | - | - | - | 24 | 58 |
| C-reactive protein (CRP) (mg/dL) | - | 0.46 | 1.18 | 0.84 | 0.53 | 0.55 | - | - |
| Erythrocyte sedimentation rate (ESR) (mm/h) | <10 | 27 | 14 | 22 | 9 | 8 | - | - |
| Urea (mg/dl) | 10–50 | 26 | 17 | 14 | 13 | 13 | - | - |
| Creatinine (mg/dL) | 0.60–1.10 | 1.22 | 0.99 | 0.90 | 1.02 | 1.01 | - | - |
| Potassium (mEq/L) | 3.5–4.5 | 4.3 | 4.6 | 3.9 | 4.2 | 4.3 | - | - |
| Sodium (mEq/L) | 136–145 | 139 | 142 | 139 | 139 | 139 | - | - |
| Calcium (mg/dL) | 8.6–10.3 | 9.7 | 9.3 | - | 8.2 | 8.4 | - | - |
| Chlorine (mEq/L) | 98–107 | 105 | - | 108 | - | 109 | - | - |
| Phosphorus (mg/dL) | 2.5–4.5 | 4.9 | - | 2.7 | - | 3.8 | - | - |
| Magnesium (mg/dL) | 1.6–2.6 | 2.1 | - | 1.9 | - | 1.7 | - | - |
| Aspartate transaminase (AST) (U/L) | <32 | 17 | 477 | 969 | 682 | 322 | 108 | 37 |
| Alanine transaminase (ALT) (U/L) | <33 | 12 | 74 | 208 | 159 | 100 | 78 | 20 |
| Gamma-glutamyl transferase (GGT) (U/L) | 8–41 | - | 9 | 7 | 5 | 9 | - | - |
| Alkaline phosphatase (FA) (U/L) | 35–104 | - | 55 | 54 | 49 | 44 | - | - |
| Lactate (mg/dL) | 5.7–22 | - | 16.3 | 14.3 | 23.7 | 10.5 | - | - |
| Leukocytes (cells/mm3) | 3.500–10.500 | 10.860 | 8.240 | 6.960 | 7.220 | 6.820 | 11220 | 8480 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tibana, R.A.; Sousa, N.M.F.d.; Cunha, G.V.; Prestes, J.; Navalta, J.W.; Voltarelli, F.A. Exertional Rhabdomyolysis after an Extreme Conditioning Competition: A Case Report. Sports 2018, 6, 40. https://doi.org/10.3390/sports6020040
Tibana RA, Sousa NMFd, Cunha GV, Prestes J, Navalta JW, Voltarelli FA. Exertional Rhabdomyolysis after an Extreme Conditioning Competition: A Case Report. Sports. 2018; 6(2):40. https://doi.org/10.3390/sports6020040
Chicago/Turabian StyleTibana, Ramires Alsamir, Nuno Manuel Frade de Sousa, Gabriel Veloso Cunha, Jonato Prestes, James W. Navalta, and Fabricio Azevedo Voltarelli. 2018. "Exertional Rhabdomyolysis after an Extreme Conditioning Competition: A Case Report" Sports 6, no. 2: 40. https://doi.org/10.3390/sports6020040
APA StyleTibana, R. A., Sousa, N. M. F. d., Cunha, G. V., Prestes, J., Navalta, J. W., & Voltarelli, F. A. (2018). Exertional Rhabdomyolysis after an Extreme Conditioning Competition: A Case Report. Sports, 6(2), 40. https://doi.org/10.3390/sports6020040