Influence of Training Load on Mood Disturbance at Sea Level and 3900 m Altitude: A Case Study of a Wheelchair Athlete


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant
2.2. Procedures
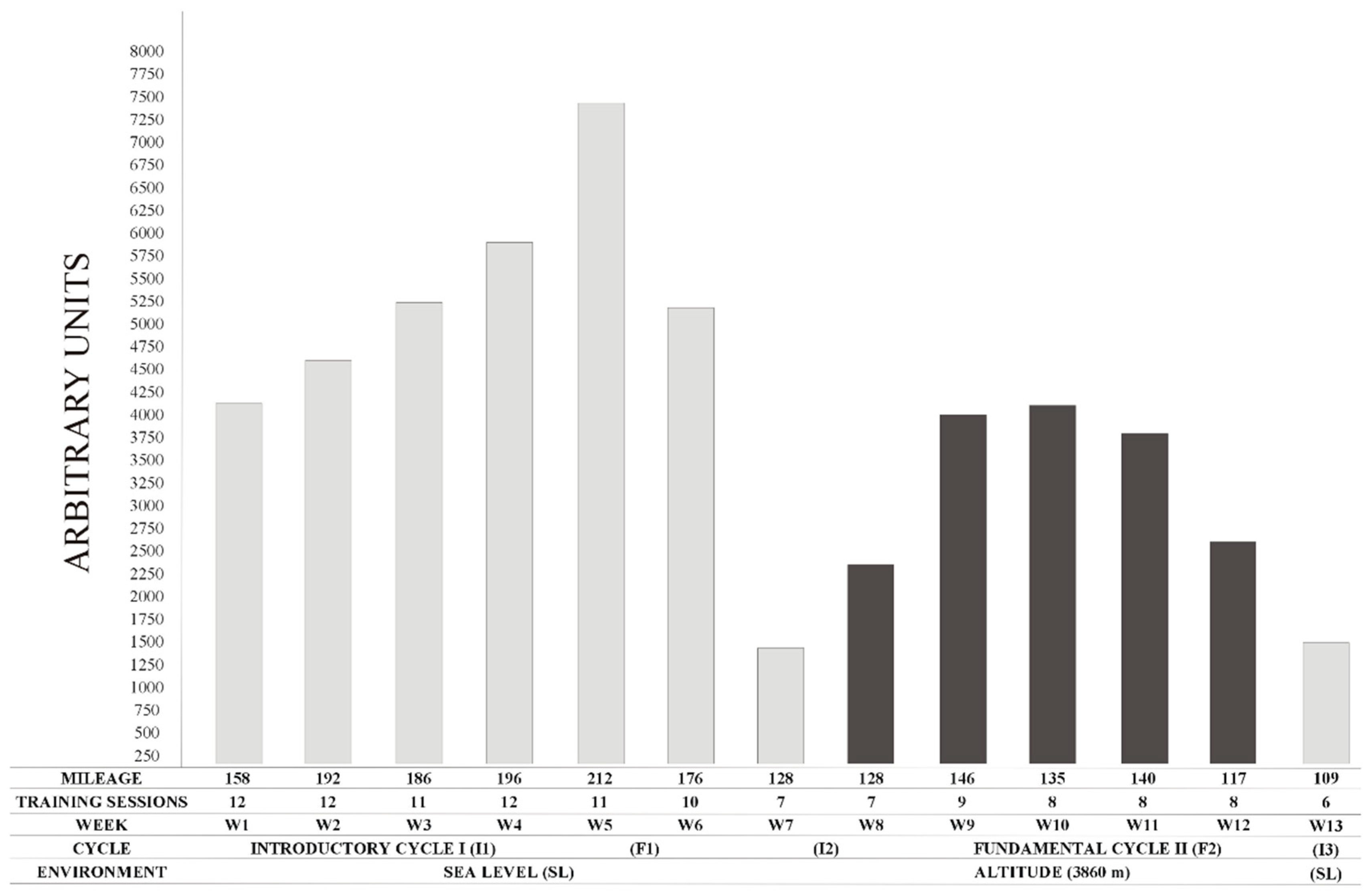
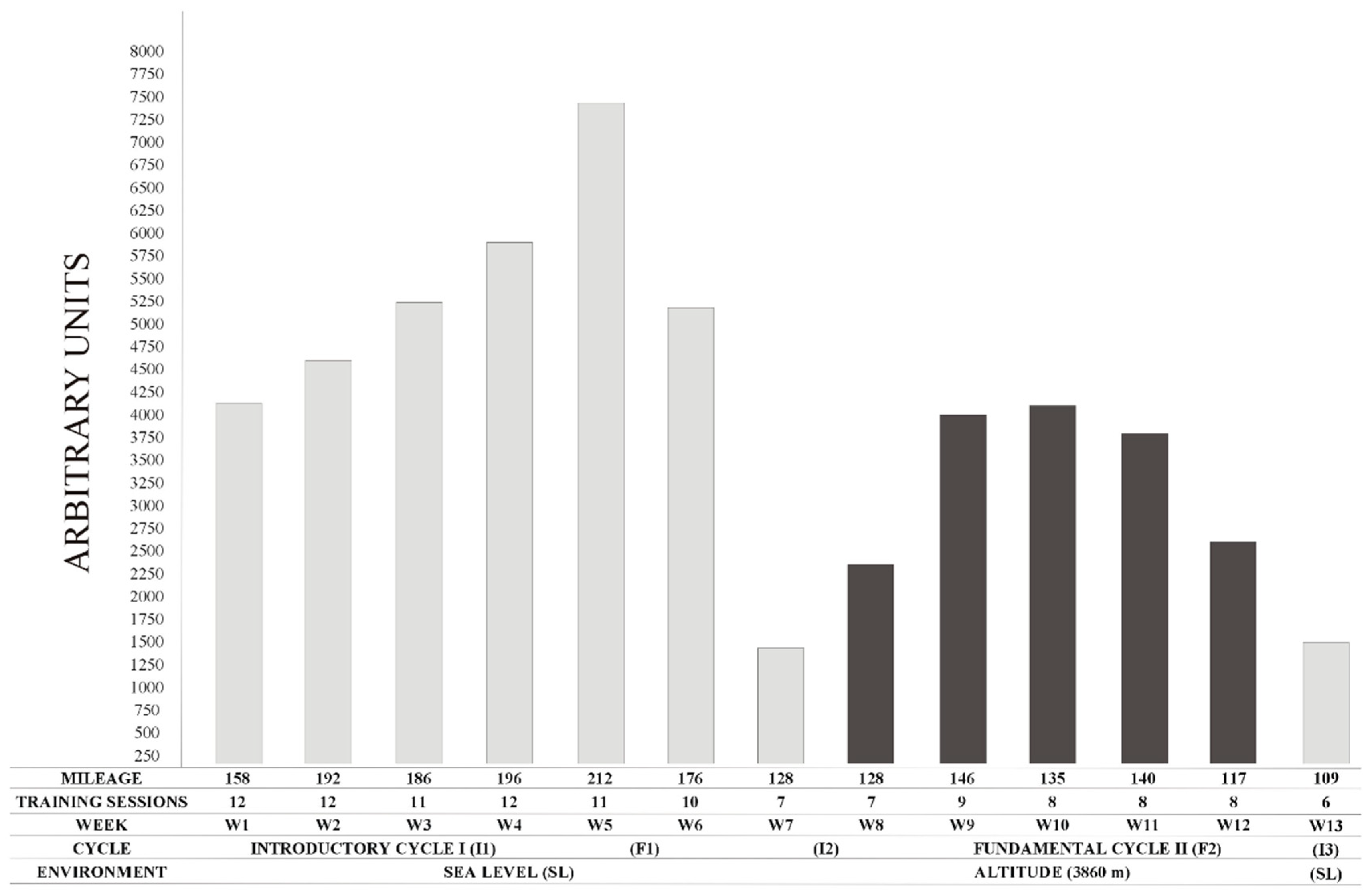
2.2.1. Training Features at Sea Level and Altitude
2.2.2. Mood States Assessment and Training Load Calculation
2.2.3. Oxygen Saturation and Brachial Blood Pressure Assessment
2.3. Statistical Analysis
3. Results
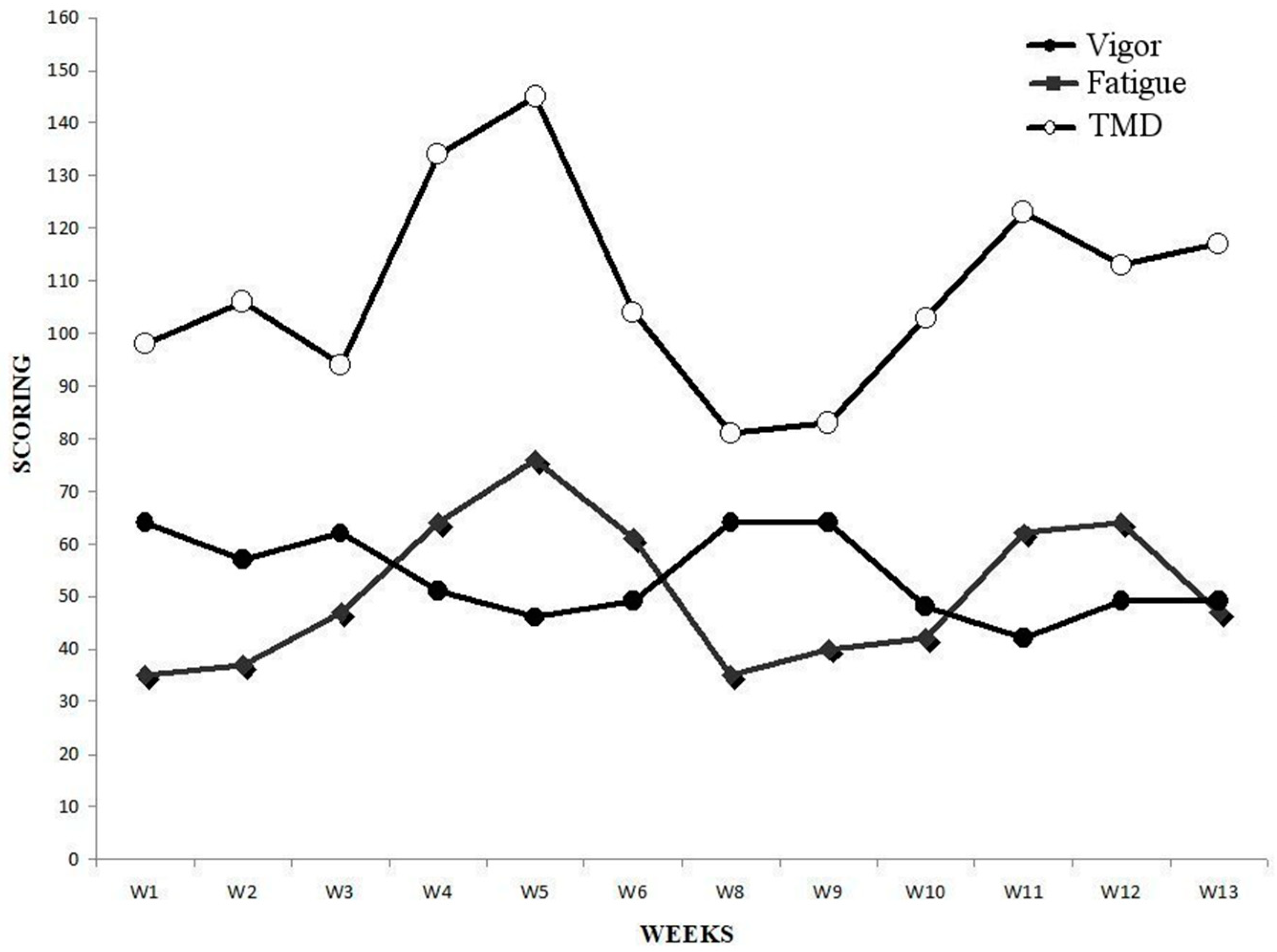
3.1. POMS
3.2. Oxygen Saturation
3.3. Brachial Blood Pressure
3.4. Total Mood Disturbance
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mcnair, D.; Loor, M.; Droppleman, L. EITS Manual for the Profile of Mood States, 1st ed.; Educational and Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- Odagiri, Y.; Shimomitsu, T.; Iwane, H.; Katsumura, T. Relationships between exhaustive mood state and changes in stress hormones following an ultraendurance race. Int. J. Sports Med. 1996, 17, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Purvis, D.; Gonsalves, S.; Deuster, P.A. Physiological and psychological fatigue in extreme conditions: Overtraining and elite athletes. PM&R 2010, 2, 442–450. [Google Scholar] [CrossRef]
- Morgan, W.P.; Brown, D.R.; Raglin, J.S.; O’Connor, P.J.; Ellickson, K.A. Psychological monitoring of overtraining and staleness. Br. J. Sports Med. 1987, 21, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Morgan, W.P. The trait psychology controversy. Res. Q. Exerc. Sport 1980, 51, 50–76. [Google Scholar] [CrossRef] [PubMed]
- Berglund, B.; Säfström, H. Psychological monitoring and modulation of training load of world-class canoeists. Med. Sci. Sports Exerc. 1994, 26, 1036–1040. [Google Scholar] [CrossRef] [PubMed]
- Shukitt-Hale, B.; Rauch, T.M.; Foutch, R. Altitude symptomatology and mood states during a climb to 3630 meters. Aviat. Space Environ. Med. 1990, 61, 225–228. [Google Scholar] [PubMed]
- Karinen, H.M.; Tuomisto, M.T. Performance, mood, and anxiety during a climb of Mount Everest. High Alt. Med. Biol. 2017, 18, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Shukitt, B.E.; Banderet, L.E. Mood states at 1600 and 4300 meters terrestrial altitude. Aviat. Space Environ. Med. 1988, 59, 530–532. [Google Scholar] [PubMed]
- Hassmén, P.; Blomstrand, E. Mood change and marathon running: A pilot study using a Swedish version of the POMS test. Scand. J. Psychol. 1991, 32, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Horvat, M.; French, R.; Henschen, K. A comparison of the psychological characteristics of male and female able-bodied and wheelchair athletes. Paraplegia 1986, 24, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz-Quinto, S.; López-Grueso, R.; Brizuela, G.; Flatt, A.A.; Moya-Ramón, M. Influence of training models at 3900m altitude on the physiological response and performance of a profesional wheelchair athlete: A case study. J. Strength Cond. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.D.; Stray-Gundersen, J. “Living high-training low”: Effect of moderate-altitude acclimatization with low-altitude training on performance. J. Appl. Physiol. 1997, 83, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Foster, C. Monitoring training in athletes with reference to overtraining syndrome. Med. Sci. Sports Exerc. 1998, 30, 1164–1168. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J.; Morgan, W.P.; Raglin, J.S. Psychobiologic effects of 3D of increased training in female and male swimmers. Med. Sci. Sports Exerc. 1991, 23, 1055–1061. [Google Scholar] [PubMed]
- Buskirk, E.R.; Kollias, J.; Akers, R.F.; Prokop, E.K.; Reategui, E.P. Maximal performance at altitude and on return from altitude in conditioned runners. J. Appl. Physiol. 1967, 23, 259–266. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Tension | Fatigue | Confusion | Depression | Anger | Vigor | TMD | BORG | |
|---|---|---|---|---|---|---|---|---|
| W1 | 55 | 35 | 31 | 39 | 39 | 64 | 98 | 4 |
| W2 | 57 | 37 | 31 | 39 | 42 | 57 | 106 | 4 |
| W3 | 37 | 47 | 31 | 39 | 39 | 62 | 94 | 5 |
| W4 | 55 | 64 | 33 | 41 | 51 | 51 | 134 | 5 |
| W5 | 54 | 76 | 33 | 39 | 56 | 46 | 145 | 6 |
| W6 | 29 | 61 | 31 | 40 | 38 | 49 | 104 | 5 |
| W7 | 72 | 64 | 60 | 44 | 76 | 48 | 182 | 4 |
| W8 | 29 | 35 | 31 | 39 | 39 | 64 | 81 | 4 |
| W9 | 28 | 40 | 31 | 39 | 39 | 64 | 83 | 5 |
| W10 | 28 | 42 | 33 | 43 | 46 | 48 | 103 | 6 |
| W11 | 35 | 62 | 33 | 41 | 48 | 42 | 123 | 5 |
| W12 | 34 | 64 | 31 | 39 | 44 | 49 | 113 | 5 |
| W13 | 40 | 47 | 43 | 42 | 46 | 49 | 117 | 4 |
| SO2 (%) | SP (mmHg) | DP (mmHg) | |
|---|---|---|---|
| W1 | 98.33 ± 0.25 †‡§¶** | 113.8 ± 4.3 †‡§¶** | 72.6 ± 3.1 *†‡§¶ |
| W2 | 98.77 ± 0.14 †‡§¶** | 117.9 ± 3.6 †‡§¶** | 77.4 ± 3.9 *†‡§¶ |
| W3 | 98.11 ± 0.42 †‡§¶** | 115.4 ± 6.1 †‡§¶** | 75.1 ± 4.5 *†‡§¶ |
| W4 | 98.56 ± 0.24 †‡§¶** | 112.7 ± 9.1 †‡§¶** | 71.4 ± 3.9 *†‡§¶ |
| W5 | 98.74 ± 0.17 †‡§¶** | 112.3 ± 6.8 †‡§¶** | 70.9 ± 5.8 *†‡§¶ |
| W6 | 98.52 ± 0.11 †‡§¶** | 107.6 ± 4.4 †‡§¶** | 68.6 ± 3.8 *†‡§¶ |
| W7 | 98.64 ± 0.14 †‡§¶** | 111.0 ± 3.3 | 68.4 ± 3.3 |
| W8 | 88.31 ± 2.46 * | 126.0 ± 5.1 | 80.4 ± 5.2 * |
| W9 | 91.19 ± 0.76 † | 127.1 ± 4.8 * | 81.1 ± 3.9 * |
| W10 | 91.92 ± 0.82 † | 132.4 ± 3.4 * | 83.4 ± 4.1 * |
| W11 | 92.35 ± 1.14 †‡ | 125.7 ± 6.9 * | 80.0 ± 2.1 * |
| W12 | 92.64 ± 1.12 † | 124.9 ± 3.5 *§ | 77.7 ± 2.1 *§ |
| W13 | 98.08 ± 0.26 †‡§¶** | 111.3 ± 7.6 †‡§¶** | 73.7 ± 4.7 *†‡§¶ |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanz-Quinto, S.; Brizuela, G.; López-Grueso, R.; Rice, I.; Moya-Ramón, M. Influence of Training Load on Mood Disturbance at Sea Level and 3900 m Altitude: A Case Study of a Wheelchair Athlete. Sports 2018, 6, 122. https://doi.org/10.3390/sports6040122
Sanz-Quinto S, Brizuela G, López-Grueso R, Rice I, Moya-Ramón M. Influence of Training Load on Mood Disturbance at Sea Level and 3900 m Altitude: A Case Study of a Wheelchair Athlete. Sports. 2018; 6(4):122. https://doi.org/10.3390/sports6040122
Chicago/Turabian StyleSanz-Quinto, Santiago, Gabriel Brizuela, Raúl López-Grueso, Ian Rice, and Manuel Moya-Ramón. 2018. "Influence of Training Load on Mood Disturbance at Sea Level and 3900 m Altitude: A Case Study of a Wheelchair Athlete" Sports 6, no. 4: 122. https://doi.org/10.3390/sports6040122