Effects of a Single Ingestion of Trehalose during Prolonged Exercise

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design—Part 1 and Part 2
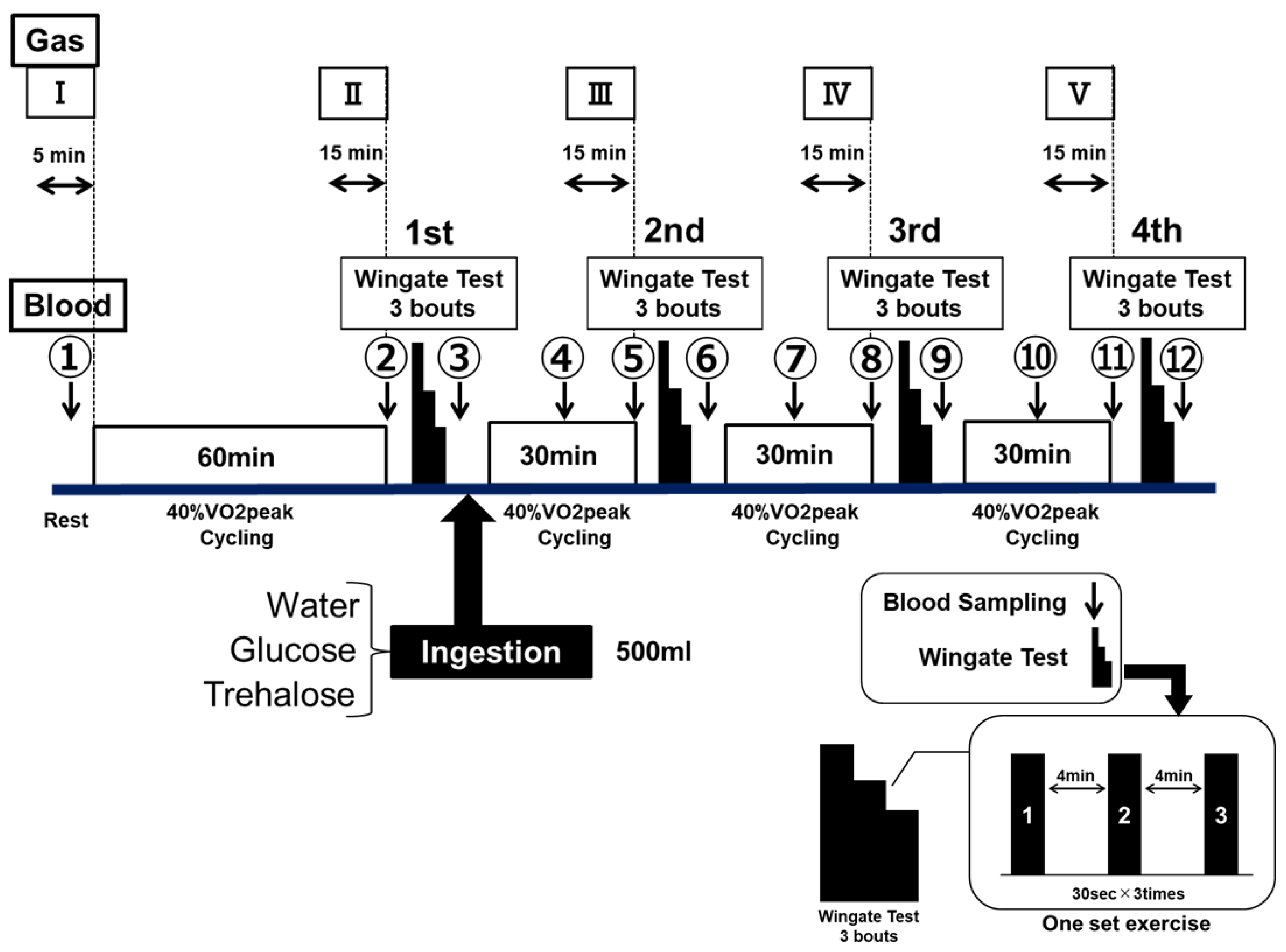
2.2.1. Part 1: Exercise Performance Protocol
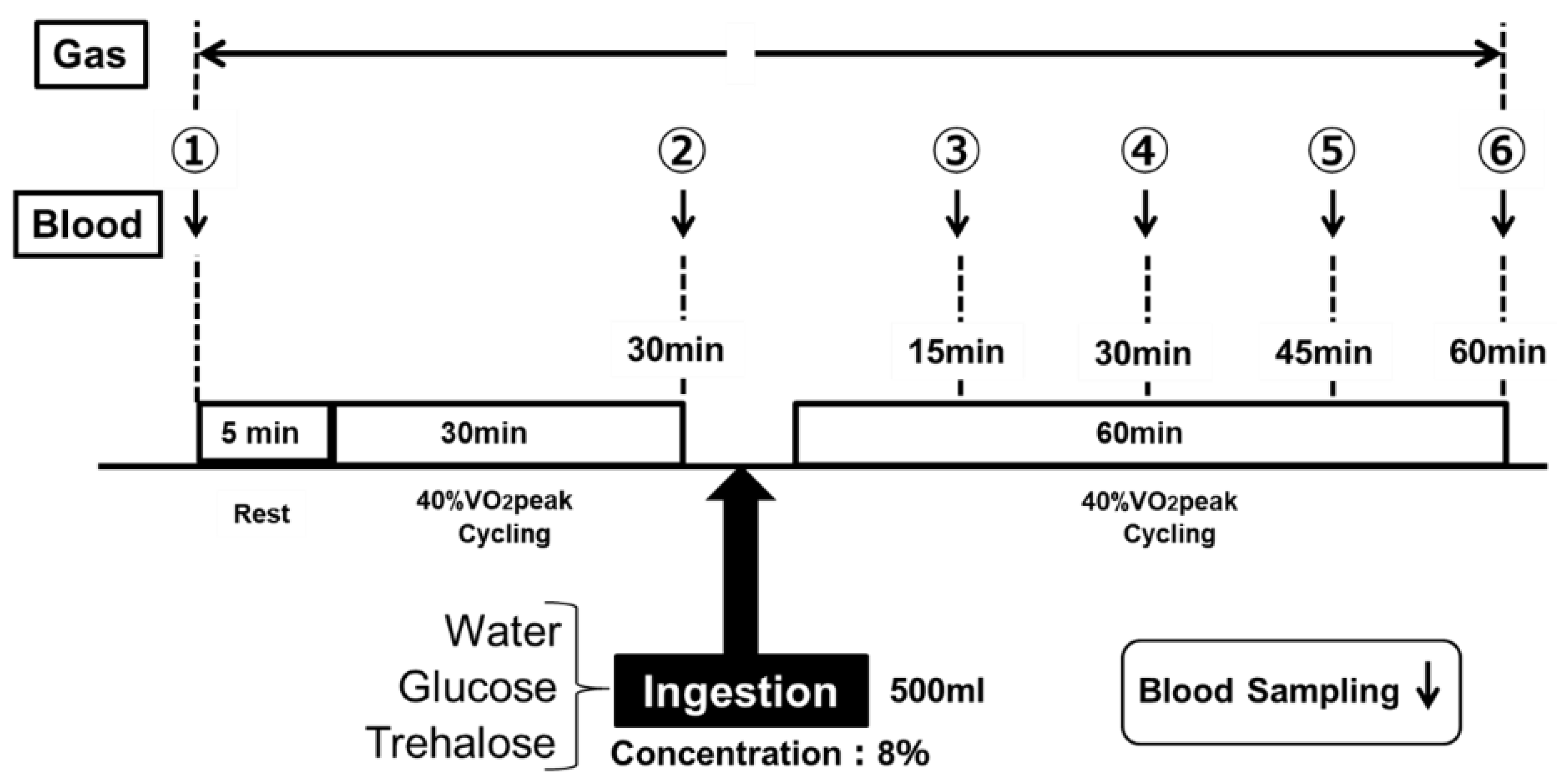
2.2.2. Part 2: Energy Metabolism Protocol
2.3. Assessments—Exercise Performance (Part 1) and Energy Metbolism (Part 2)
2.4. Statistical Analysis
3. Results
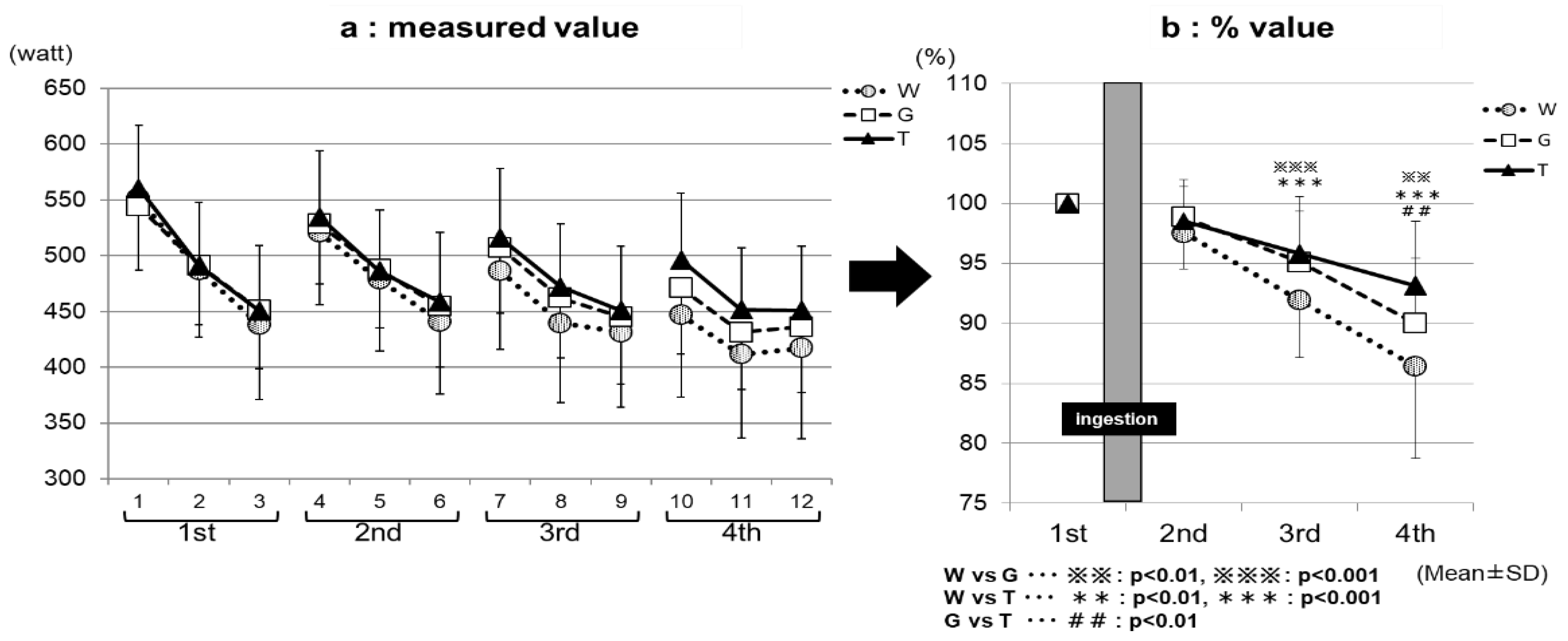
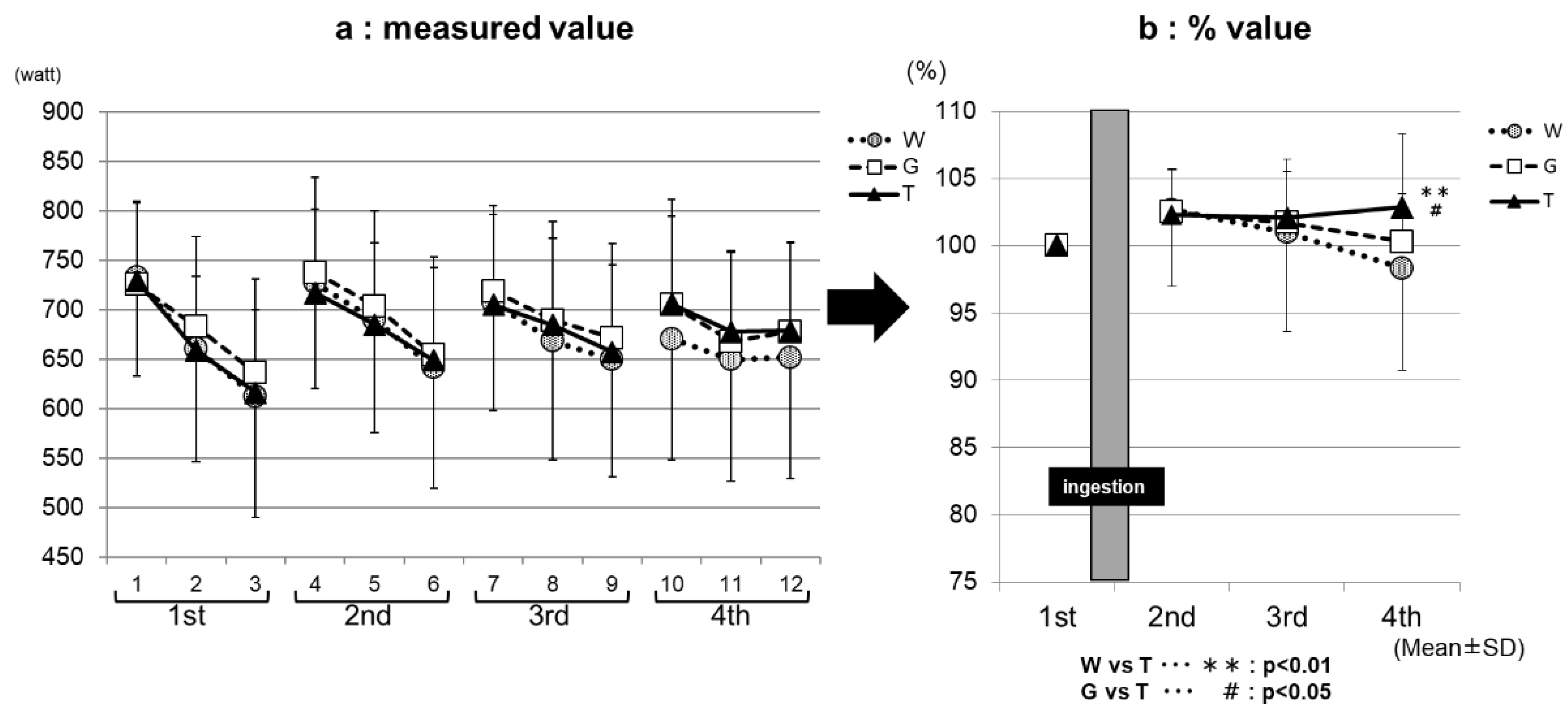
3.1. Assessment of Exercise Performance—Part 1
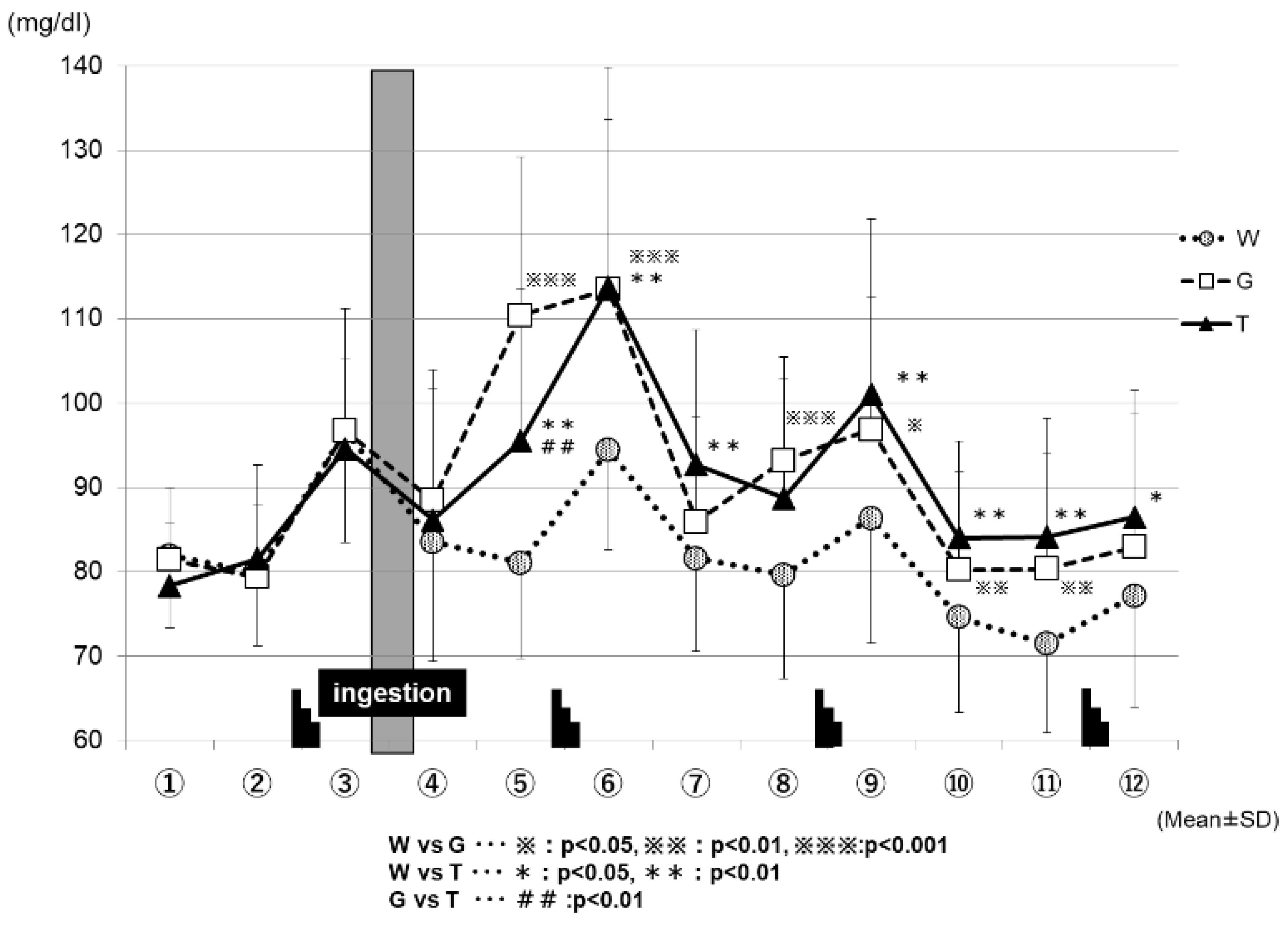
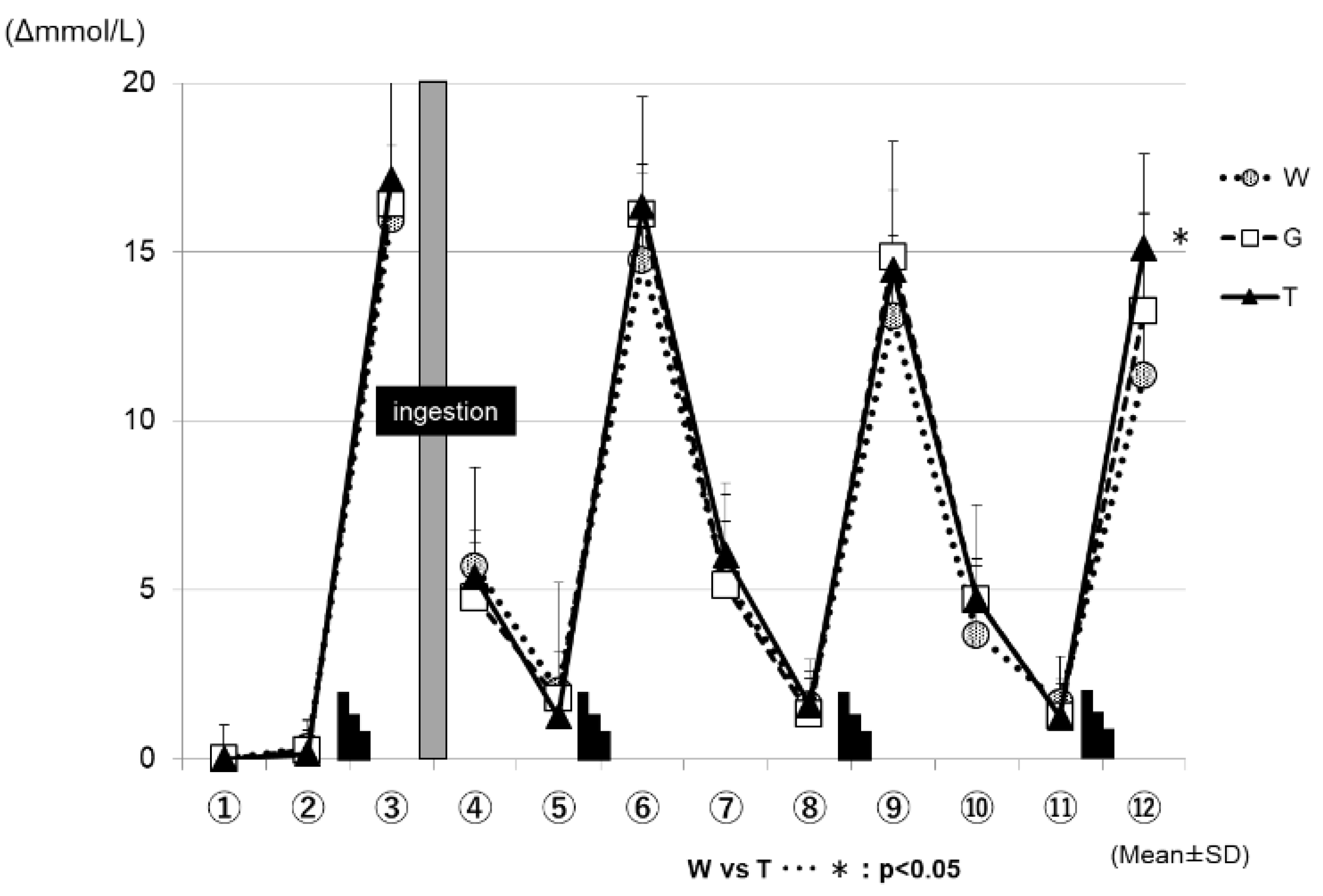
3.2. Changes in Blood Glucose and Lactate Levels—Part 1
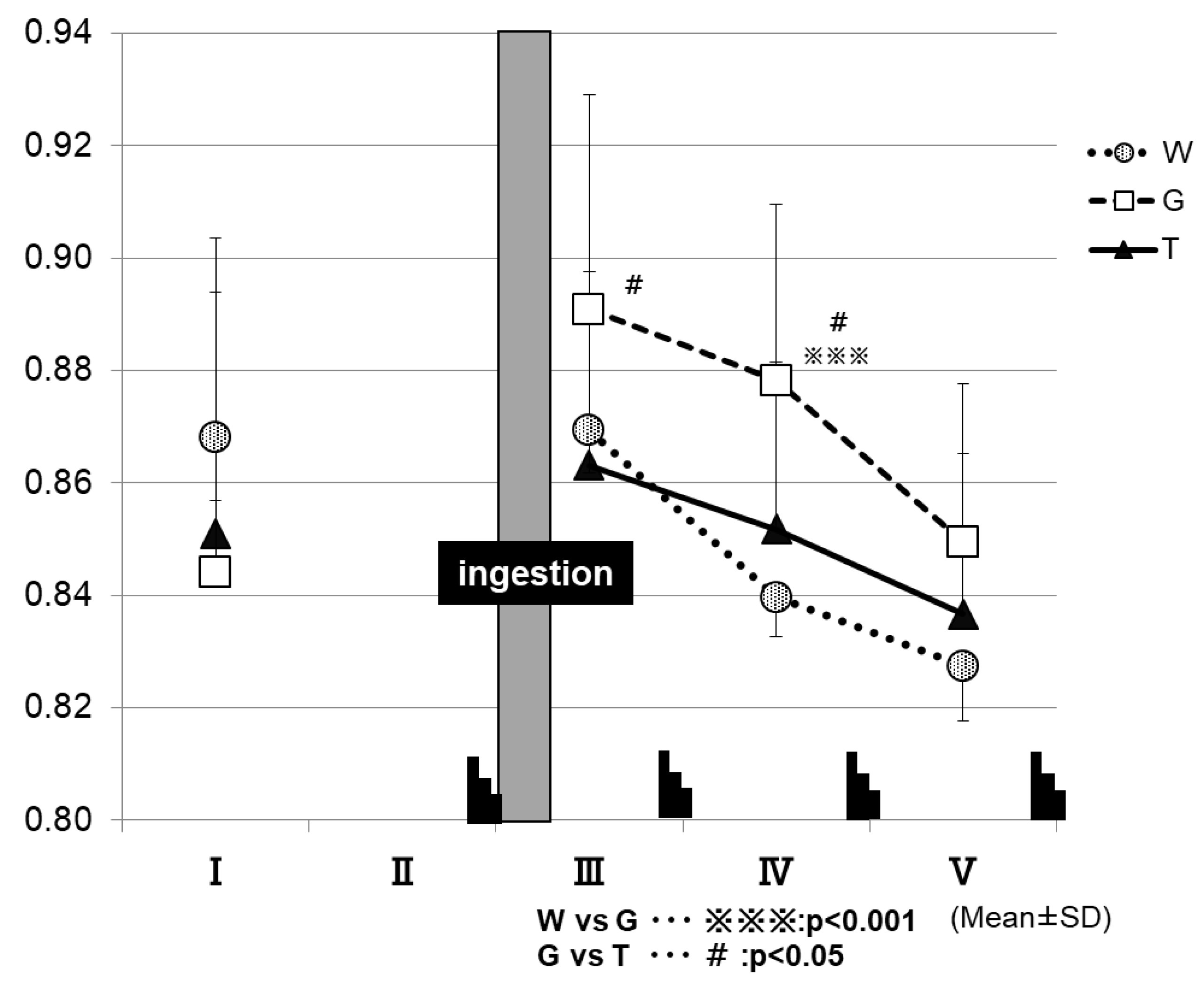
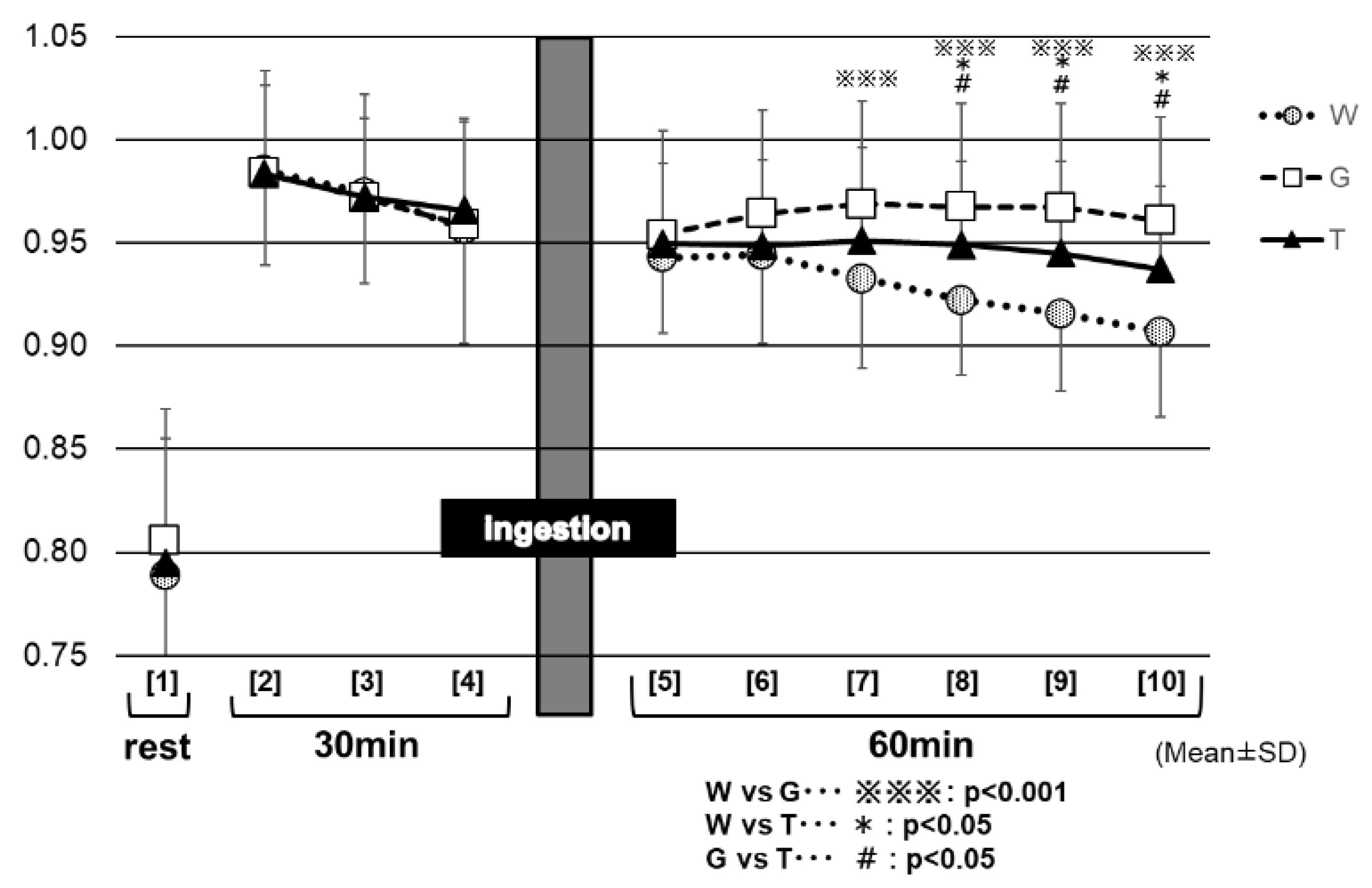
3.3. Changes in RER—Part 1
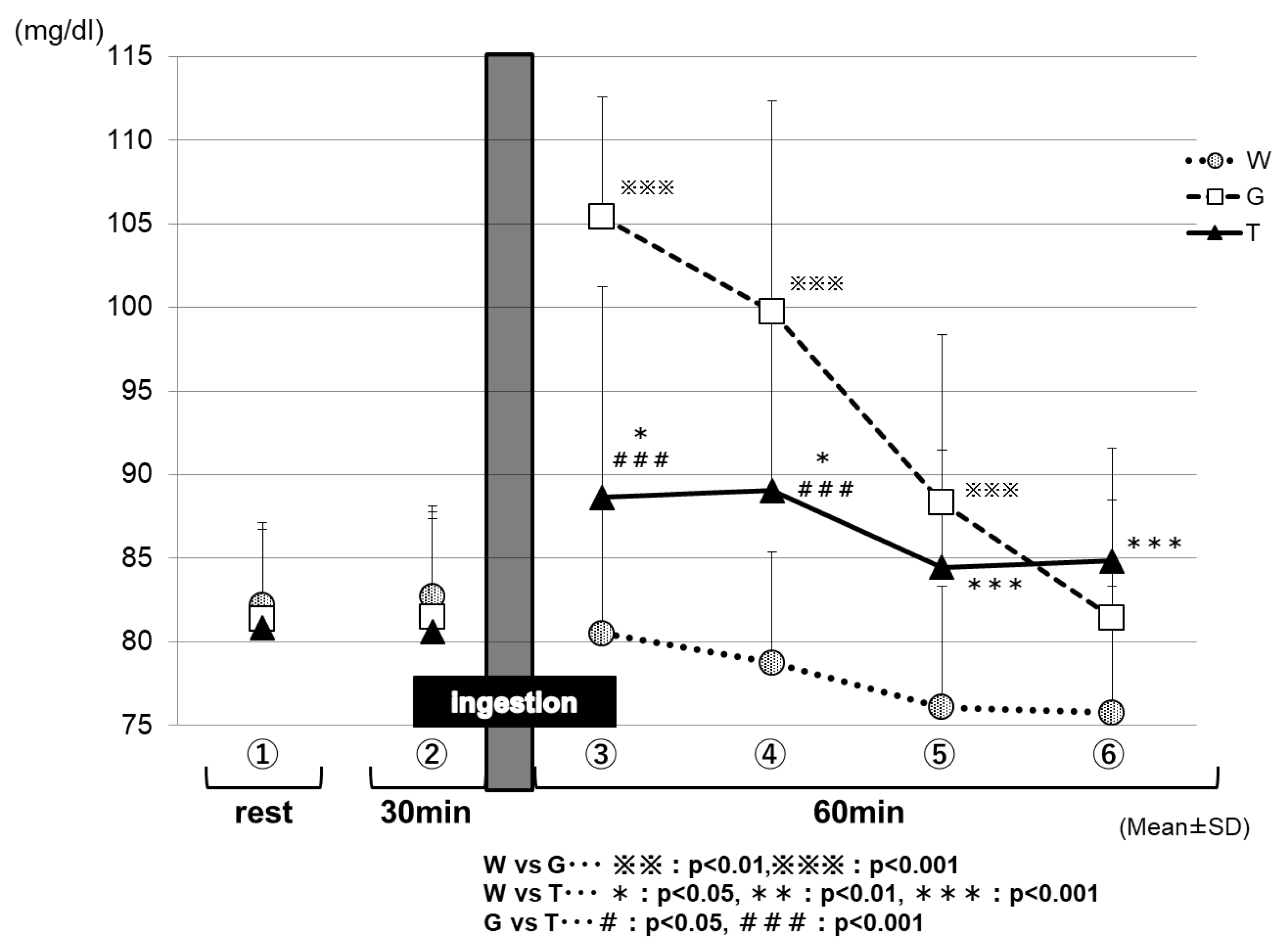
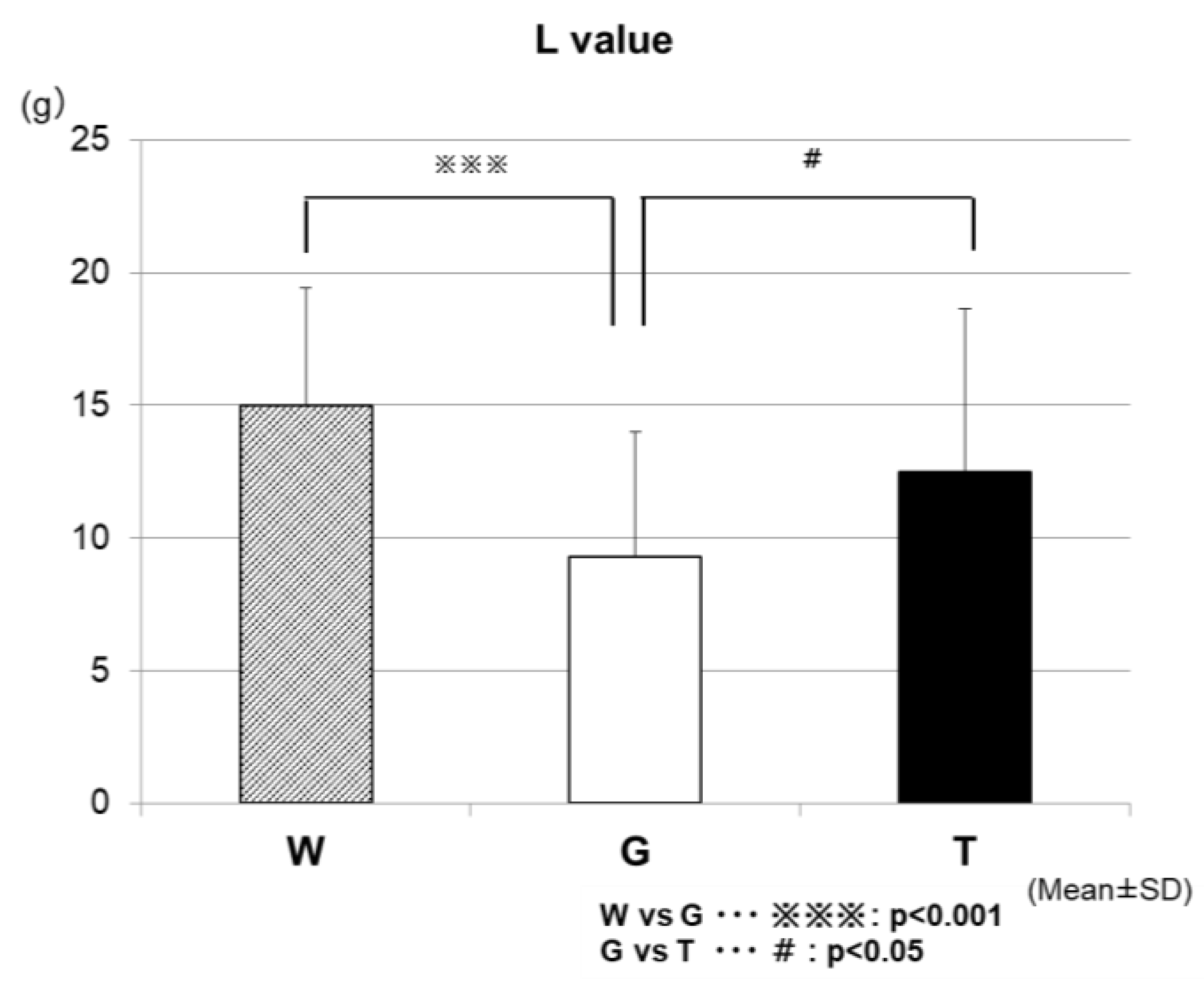
3.4. Assessment of Energy Metabolism in Low-Intensity Constant-Load Exercise—Part 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Parolin, M.L.; Chesley, A.; Matsos, M.P.; Spriet, L.L.; Jones, N.L.; Heigenhauser, G.J. Regulation of skeletal muscle glycogen phosphorylase and PDH during maximal intermittent exercise. Am. J. Physiol. 1999, 277, 890–900. [Google Scholar] [CrossRef]
- Calbet, J.A.; De Paz, J.A.; Garatachea, N.; Cabeza de Vaca, S.; Chavarren, J. Anaerobicenergy provision does not limit Wingate exercise performance in endurance-trained cyclists. J. Appl. Physiol. 2003, 94, 668–676. [Google Scholar] [CrossRef]
- Gibala, M.J.; McGee, S.L.; Garnham, A.P.; Howlett, K.F.; Snow, R.J.; Hargreaves, M. Brief intense interval exercise activates AMPK and p38 MAPK signaling and increases the expression of PGC-1 alpha in human skeletal muscle. J. Appl. Physiol. 2009, 106, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Farrell, P.A.; Joyner, M.; Caiozzo, V. ACSM’s Advanced Exercise Physiology, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; pp. 379–391. [Google Scholar]
- McConell, G.; Snow, R.J.; Proietto, J.; Hargreaves, M. Muscle metabolism during prolonged exercise in humans: Influence of carbohydrate availability. J. Appl. Physiol. 1999, 87, 1083–1086. [Google Scholar] [CrossRef] [PubMed]
- De Bock, K.; Derave, W.; Ramaekers, M.; Richter, E.A.; Hespel, P. Fiber type-specific muscle glycogen sparing due to carbohydrate intake before and during exercise. J. Appl. Physiol. 2007, 102, 183–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stellingwerff, T.; Boon, H.; Gijsen, A.P.; Stegen, J.H.; Kuipers, H.; van Loon, L.J. Carbohydrate supplementation during prolonged cycling exercise spares muscle glycogen but does not affect intramyocellular lipid use. Pflugers Arch. 2007, 454, 635–647. [Google Scholar] [CrossRef] [Green Version]
- Coyle, E.F. Carbohydrate supplementation during exercise. J. Nutr. 1992, 122, 788–795. [Google Scholar] [CrossRef]
- Coyle, E.F.; Hamilton, M.T.; Alonso, J.G.; Montain, S.J.; Ivy, J.L. Carbohydrate metabolism during intense exercise when hyperglycemic. J. Appl. Physiol. 1991, 70, 834–840. [Google Scholar] [CrossRef] [Green Version]
- Bergstrom, J.; Hultman, E. Muscle glycogen synthesis after exercise: An enhancing factor localized to the muscle cells in man. Nature 1966, 210, 309–310. [Google Scholar] [CrossRef]
- McConell, G.; Kloot, K.; Hargreaves, M. Effect of timing of carbohydrate ingestion on endurance exercise performance. Med. Sci. Sports Exerc. 1996, 28, 1300–1304. [Google Scholar] [CrossRef]
- Mitchell, J.B.; Costill, D.L.; Houmard, A.; Flynn, M.G.; Fink, W.J.; Beltz, J.D. Effect of carbohydrate ingestion on gastric emptying and exercise performance. Med. Sci. Sports Exerc. 1988, 20, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Murray, R.; Eddy, D.E.; Murray, T.W.; Seifert, J.G.; Paul, G.L.; Halaby, G.A. The effect of fluid and carbohydrate feedings during intermittent cycling exercise. Med. Sci. Sports Exerc. 1987, 19, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Murray, R.; Paul, G.; Seifert, J.G.; Eddy, D.E.; Halaby, G.A. The effects of glucose, fructose, and sucrose ingestion during exercise. Med. Sci. Sports Exerc. 1989, 21, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Murray, R.; Paul, G.L.; Seifert, J.G.; Eddy, D.E. Response to varying rates of carbohydrate ingestion during exercise. Med. Sci. Sports Exerc. 1991, 23, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Neufer, P.D.; Costill, D.L.; Flynn, M.G.; Kirwan, J.P.; Mitchell, J.B.; Houmard, J. Improvements in exercise performance: effects of carbohydrate feeding and diet. J. Appl. Physiol. 1987, 62, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Skein, M.; Duffield, R.; Kelly, B.T.; Marino, F.E. The effects of carbohydrate intake and muscle glycogen content on self-paced intermittent-sprint exercise despite no knowledge of carbohydrate manipulation. Eur. J. Appl. Physiol. 2012, 112, 2859–2870. [Google Scholar] [CrossRef]
- Jeukendrup, A.E.; Jentjens, R. Oxidation of carbohydrate feedings during prolonged exercise: Current thoughts, guidelines and directions for future research. Sports Med. 2000, 29, 407–424. [Google Scholar] [CrossRef]
- Massicotte, D.; Pëonnet, F.; Brisson, G.; Bakkouch, K.; Hillaire-Marce, C. Oxidation of a glucose polymer during exercise: Comparison with glucose and fructose. J. Appl. Physiol. 1989, 66, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.; Costill, D.L.; Fink, W.J. Effect of prexercise feedings on endurance performance. Med. Sci. Sports. 1979, 11, 1–5. [Google Scholar] [PubMed]
- McMurray, R.G.; Wilson, J.R.; Kitchell, B.S. The effect of fructose and glucose on high intensity endurance performance. Res. Quart. Exerc. Sports Exerc. 1983, 20, 110–115. [Google Scholar] [CrossRef]
- Oku, T.; Okazaki, M. Transitory laxative threshold of trehalose and lactulose in healthy women. J. Nutr. Sci. Vitaminol. 1998, 44, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Oku, T.; Nakamura, S. Estimation of intestinal trehalase activity from a laxative threshold of trehalose and lactulose on healthy female subjects. Eur. J. Clin. Nutr. 2000, 4, 783–788. [Google Scholar] [CrossRef]
- Yoshizane, C.; Mizote, A.; Yamada, M.; Arai, N.; Arai, S.; Maruta, K.; Mitsuzumi, H.; Ariyasu, T.; Ushio, S.; Fukuda, S. Glycemic, insulinemic and incretin responses after oral trehalose ingestion in healthy subjects. Nutr. J. 2017, 16, 9. [Google Scholar] [CrossRef]
- Ahlborg, G.; Felig, P. Substrate utilization during prolonged exercise preceded by ingestion of glucose. Am. J. Physiol. 1977, 233, 188–194. [Google Scholar] [CrossRef]
- Jentjens, R.L.; Jeukendrup, A.E. Effects of pre-exercise ingestion of trehalose, galactose and glucose on subsequent metabolism and cycling performance. Eur. J. Appl. Physiol. 2003, 88, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Inbar, O.; Bar-Or, O.; Skinner, J.S. The Wingate Anaerobic Test; Human Kinetics: Champaign, IL, USA, 1996; pp. 1–40. [Google Scholar]
- Simon, B.; Vladimir, K.; Michael, M.; Rothkopf, C.W. Energy Metabolism, Indirect Calorimetry, and Nutrition; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1989. [Google Scholar]
- Greer, F.; McLean, C.; Graham, T.E. Caffeine, performance, and metabolism during repeated Wingate exercise tests. J. Appl. Physiol. 1998, 85, 1502–1508. [Google Scholar] [CrossRef]
- Vincent, S.; Berthon, P.; Zouhal, H.; Moussa, E.; Catheline, M.; Bentué-Ferrer, D.; Gratas-Delamarche, A. Plasma glucose, insulin and catecholamine responses to a Wingate test in physically active women and men. Eur. J. Appl. Physiol. 2004, 91, 15–21. [Google Scholar] [PubMed]
- Gaibo, H.; Hoist, J.J.; Christensen, N.J. Glucagon and plasma catecholamine responses to graded and prolonged exercise in man. J. Appl. Physiol. 1975, 38, 70–76. [Google Scholar]
- Kjaer, M.; Farrell, P.A.; Christensen, N.J.; Galbo, H. Increased epinephrine response and inaccurate glucoregulation in exercising athletes. J. Appl. Physiol. 1986, 61, 1693–1700. [Google Scholar] [CrossRef]
- Koivisto, V.; Hendler, R.; Nadel, E.; Feling, P. Influence of physical traning on the fuel-hormon responeses to prolonged low intensity exercise. Metabolism 1982, 31, 192–197. [Google Scholar] [CrossRef]
- Lundborg, P.; Astrom, H.; Bengtsson, C.; Fellenius, E.; Schenck, H.V.; Svensson, L.; Smith, U. Effect of β-adrenoceptor blockadeon exercise performance and metabolism. Clin. Sci. 1981, 61, 299–305. [Google Scholar] [CrossRef]
- Wojtaszewski, J.F.; MacDonald, C.; Nielsen, J.N.; Hellsten, Y.; Hardie, D.G.; Kemp, B.E.; Kiens, B.; Richter, E.A. Regulation of 5′AMP-activated protein kinase activity and substrate utilization in exercising human skeletal muscle. Am. J. Physiol. 2003, 284, E813–E822. [Google Scholar] [CrossRef] [Green Version]
- Beneke, R.; Pollmann, C.; Bleif, I.; Leithäuser, R.M.; Hütler, M. How anaerobic is the Wingate Anaerobic Test for humans? Eur. J. Appl. Physiol. 2002, 87, 388–392. [Google Scholar] [PubMed]
- Katz, A.; Sahlin, K. Regulation of lactic acid production during exercise. J. Appl. Physiol. 1988, 65, 509–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemper, W.F.; Lindstedt, S.L.; Hartzler, L.K.; Hicks, J.W.; Conley, K.E. Shaking up glycolysis: Sustained, high lactate flux during aerobic rattling. Proc. Natl. Acad. Sci. USA 2001, 98, 723–728. [Google Scholar] [CrossRef] [Green Version]
- Germaine, M.; Collins, K.; Shortall, M. The Effect of caffeine ingestion and carbohydrate mouth rinse on high-intensity running performance. Sports 2019, 14, 7. [Google Scholar] [CrossRef]
- Kuipers, H.; Costill, D.L.; Porter, D.A.; Fink, W.J.; Morse, W.M. Glucose feeding and exercise in trained rats: Mechanisms for glycogen sparing. J. Appl. Physiol. 1986, 61, 859–863. [Google Scholar] [CrossRef]
- Kuipers, H.; Keizer, H.A.; Brouns, F.; Saris, W.H.; Saris, W.H. Carbohydrate feeding and glycogen synthesis during exercise in man. Pflugers Arch. 1987, 410, 652–656. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 25 | Age (year) | Height (cm) | Weight (kg) | % fat (%) | VO2 (peak) (mL/min) | Load (peak) (watt) | 40%VO2peak (mL/min) | Load 40%VO2peak (watt) |
|---|---|---|---|---|---|---|---|---|
| Mean | 21.3 | 172.7 | 66.4 | 19.2 | 2812.4 | 251.7 | 1125.0 | 97.7 |
| SD | 1.1 | 5.0 | 6.9 | 2.5 | 380.6 | 33.1 | 152.3 | 14.6 |
| n = 24 | Age (year) | Height (cm) | Weight (kg) | %fat (%) | VO2 (peak) (mL/min) | Load (peak) (watt) | 40%VO2peak (mL/min) | Load 40%VO2peak (watt) |
|---|---|---|---|---|---|---|---|---|
| Mean | 21.9 | 173.4 | 66.2 | 19.6 | 2988.5 | 253.7 | 1195.4 | 99.0 |
| SD | 1.2 | 5.6 | 5.8 | 2.8 | 368.1 | 32.7 | 147.2 | 15.7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wadazumi, T.; Watanabe, K.; Watanabe, H.; Yokoyama, H.; Hongu, N.; Arai, N. Effects of a Single Ingestion of Trehalose during Prolonged Exercise. Sports 2019, 7, 100. https://doi.org/10.3390/sports7050100
Wadazumi T, Watanabe K, Watanabe H, Yokoyama H, Hongu N, Arai N. Effects of a Single Ingestion of Trehalose during Prolonged Exercise. Sports. 2019; 7(5):100. https://doi.org/10.3390/sports7050100
Chicago/Turabian StyleWadazumi, Tsuyoshi, Kanji Watanabe, Hitoshi Watanabe, Hisayo Yokoyama, Nobuko Hongu, and Norie Arai. 2019. "Effects of a Single Ingestion of Trehalose during Prolonged Exercise" Sports 7, no. 5: 100. https://doi.org/10.3390/sports7050100
APA StyleWadazumi, T., Watanabe, K., Watanabe, H., Yokoyama, H., Hongu, N., & Arai, N. (2019). Effects of a Single Ingestion of Trehalose during Prolonged Exercise. Sports, 7(5), 100. https://doi.org/10.3390/sports7050100