Injuries in Novice Participants during an Eight-Week Start up CrossFit Program—A Prospective Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Data Sources
2.5. Outcome Variables
2.5.1. Exposure
2.5.2. Registration of Injuries
2.5.3. Injury Rate
2.5.4. Risk Factors
2.5.5. Rhabdomyolysis
2.6. Bias
2.7. Study Size
2.8. Ethics
2.9. Statistical Methods
3. Results
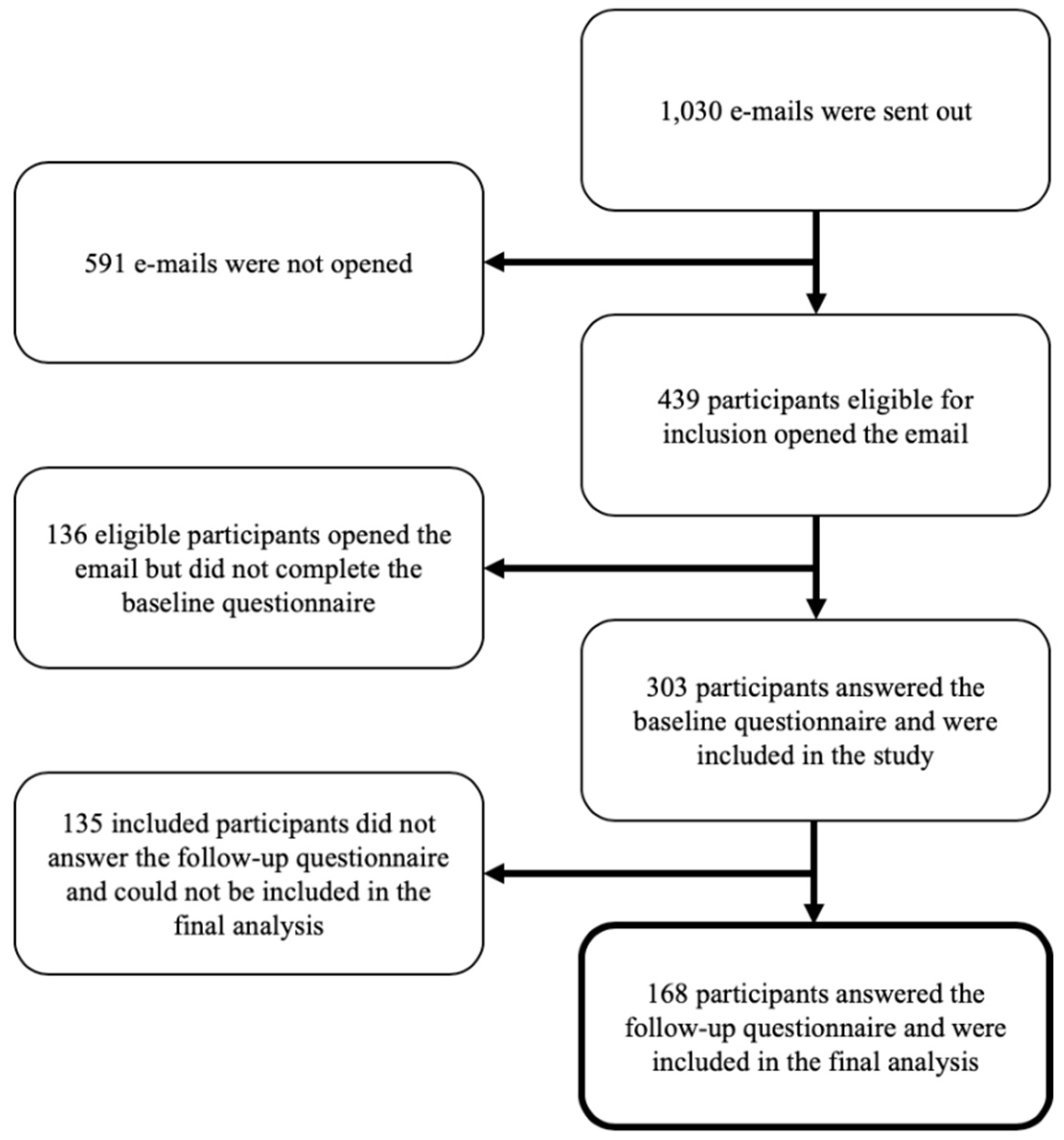
3.1. Participants
3.2. Exposure
3.3. Injury Incidence
3.4. Injury Rate
3.5. Risk Factors
3.6. Rhabdomyolysis
3.7. Explorative Associations
3.8. Explorative Sensitivity Analysis
4. Discussion
4.1. Results
4.1.1. Incidence and Injury Rate
4.1.2. Injury Location
4.1.3. Risk Factors
4.1.4. Exertional Rhabdomyolysis
5. Methodological Considerations
5.1. Definition of Injury
5.2. Inclusion and Response Rate
5.3. General Limitations and Recommendations for Future Research
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ritter, E. By The Numbers: The Growth of Crossfit. Available online: https://channelsignal.com/blog/by-the-numbers-the-growth-of-crossfit/ (accessed on 26 November 2018).
- Wang, C. How CrossFit Rode a Single Issue to World Fitness Domination. Available online: https://www.cnbc.com/2016/04/05/how-crossfit-rode-a-single-issue-to-world-fitness-domination.html (accessed on 26 November 2018).
- Glassman, G. Understanding CrossFit. Available online: https://channelsignal.com/blog/by-the-numbers-the-growth-of-crossfit/ (accessed on 26 November 2018).
- Hak, P.T.; Hodzovic, E.; Hickey, B. The nature and prevalence of injury during Crossfit training. J. Strength Cond. Res. 2013. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, M.F.; Nindl, B.C.; Deuster, P.A.; Baumgartner, N.; Kane, S.F.; Kraemer, W.J.; Sexauer, L.R.; Thompson, W.R.; O’Connor, F.G. Consortium for Health and Military Performance and American College of Sports Medicine consensus paper on extreme conditioning programs in military personnel. Curr. Sports Med. Rep. 2011, 10, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Aune, K.T.; Powers, J.M. Injuries in an Extreme Conditioning Program. Sports Health 2017, 9, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Chachula, L.A.; Cameron, K.L.; Svoboda, S.J. Association of Prior Injury with the Report of New Injuries Sustained During CrossFit Training. Athl. Train. Sports Health Care 2016, 8, 28–34. [Google Scholar] [CrossRef]
- Escalante, G.A.; Gentry, C.; Kern, B.; Waryasz, G. Injury patterns and rates of Costa Rican CrossFit® participants—A retrospective study—No.48. Sport Med. J. 2017, 13, 2927–2934. [Google Scholar]
- Grier, T.; Canham-Chervak, M.; McNulty, V.; Jones, B.H. Extreme conditioning programs and injury risk in a US Army Brigade Combat Team. US Army Med. Dep. J. 2013, 36–47. Available online: https://www.ncbi.nlm.nih.gov/pubmed/24146241 (accessed on 26 November 2018).
- Hopkins, B.S.; Cloney, M.B.; Kesavabhotla, K.; Yamaguchi, J.; Smith, Z.A.; Koski, T.R.; Hsu, W.K.; Dahdaleh, N.S. Impact of CrossFit-Related Spinal Injuries. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2017, 29, 482–485. [Google Scholar] [CrossRef] [Green Version]
- Mehrab, M.; de Vos, R.-J.; Kraan, G.A.; Mathijssen, N.M.C. Injury Incidence and Patterns Among Dutch CrossFit Athletes. Orthop. J. Sports Med. 2017, 5. [Google Scholar] [CrossRef] [Green Version]
- Moran, S.; Booker, H.; Staines, J.; Williams, S. Rates and risk factors of injury in CrossFitTM: A prospective cohort study. J. Sports Med. Phys. Fitness 2017, 57, 1147–1153. [Google Scholar]
- Sprey, J.W.C.; Ferreira, T.; de Lima, M.V.; Duarte, A.; Jorge, P.B.; Santili, C. An Epidemiological Profile of CrossFit Athletes in Brazil. Orthop. J. Sports Med. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Summitt, R.J.; Cotton, R.A.; Kays, A.C.; Slaven, E.J. Shoulder Injuries in Individuals Who Participate in CrossFit Training. Sports Health 2016, 8, 541–546. [Google Scholar] [CrossRef] [Green Version]
- Weisenthal, B.M.; Beck, C.A.; Maloney, M.D.; DeHaven, K.E.; Giordano, B.D. Injury Rate and Patterns Among CrossFit Athletes. Orthop. J. Sports Med. 2014, 2. [Google Scholar] [CrossRef]
- Montalvo, A.M.; Shaefer, H.; Rodriguez, B.; Li, T.; Epnere, K.; Myer, G.D. Retrospective Injury Epidemiology and Risk Factors for Injury in CrossFit. J. Sports Sci. Med. 2017, 16, 53–59. [Google Scholar] [PubMed]
- Feito, Y.; Burrows, E.K.; Tabb, L.P. A 4-Year Analysis of the Incidence of Injuries Among CrossFit-Trained Participants. Orthop. J. Sports Med. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- Tolstrup Larsen, R. Letter to the Editor. Sports Health Multidiscip. Approach 2018, 10, 468. [Google Scholar] [CrossRef]
- Minghelli, B.; Vicente, P. Musculoskeletal injuries in Portuguese CrossFit practitioners. J. Sports Med. Phys. Fitness 2019, 59, 1213–1220. [Google Scholar] [CrossRef]
- Van Mechelen, W.; Hlobil, H.; Kemper, H.C. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med. Auckl. N. Z. 1992, 14, 82–99. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Clarsen, B.; Myklebust, G.; Bahr, R. Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: The Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire. Br. J. Sports Med. 2013, 47, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Tafuri, S.; Salatino, G.; Napoletano, P.; Monno, A.; Notarnicola, A. The risk of injuries among CrossFit athletes: An Italian observational retrospective survey. J. Sports Med. Phys. Fitness 2018. [Google Scholar] [CrossRef]
- Huynh, A.; Leong, K.; Jones, N.; Crump, N.; Russell, D.; Anderson, M.; Steinfort, D.; Johnson, D.F. Outcomes of exertional rhabdomyolysis following high-intensity resistance training. Intern. Med. J. 2016, 46, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Phillips, L.H. Sports injury incidence. Br. J. Sports Med. 2000, 34, 133–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice, 4th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2009; ISBN 978-0-13-234470-8. [Google Scholar]
- Elkin, J.L.; Kammerman, J.S.; Kunselman, A.R.; Gallo, R.A. Likelihood of Injury and Medical Care Between CrossFit and Traditional Weightlifting Participants. Orthop. J. Sports Med. 2019, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Lost to Follow up, n = 135 | Included in Final Analysis, n = 168 | p | |
|---|---|---|---|
| Age, mean ± SD (95%CI) | 26.8 ± 6.6 (25.7 to 28.0) | 29.2 ± 7.9 (28.0 to 30.4) | p = 0.006 |
| Sex, male, n (%) | 42 (31.1%) | 51 (30.7%) | p = 0.888 |
| BMI, mean ± SD (95%CI) | 24.5 ± 5.4 (23.5 to 25.4) | 24.3 ± 2.9 (23.9 to 24.7) | p = 0.799 |
| Educational level, n (%) | 9 (6.7%) | 7 (4.2%) | p = 0.045 |
| Primary education | 76 (56.3%) | 71 (42.6%) | |
| Secondary education | 36 (26.7%) | 57 (33.4%) | |
| Tertiary | 14 (10.4%) | 32 (19.1%) | |
| Master’s, Doctoral or equivalent education | 0 (0%) | 1 (0.6%) | |
| “Do not know” | |||
| Currently studying, n (%) | 68 (50.4%) | 86 (51.2%) | p = 0.887 |
| Employed, n (%) | 93 (68.9%) | 120 (71.4%) | p = 0.631 |
| Currently smoking, n (%) | 12 (8.9%) | 12 (7.2%) | p = 0.576 |
| Units of alcohol per week, median (IQR) | 2 (0.2 to 5) | 2.5 (1 to 5) | p = 0.307 |
| Previous primary sport, n (%) | p = 0.052 | ||
| CrossFit or functional training | 1 (0.7%) | 2 (1.2%) | |
| Cycling | 4 (2.9%) | 12 (7.1%) | |
| Dance | 2 (1.5%) | 2 (1.2%) | |
| Fitness | 43 (31.9%) | 34 (20.2%) | |
| Team sports (handball, soccer etc.) | 10 (7.4%) | 25 (14.9%) | |
| Gymnastics | 6 (4.4%) | 2 (1.2%) | |
| Running | 19 (14.1%) | 40 (23.8%) | |
| Strength training | 14 (10.4%) | 12 (7.1%) | |
| Swimming | 2 (1.5%) | 5 (3.0%) | |
| Yoga or Pilates | 3 (2.2%) | 5 (3.0%) | |
| Other sports | 11 (8.2%) | 12 (6.6%) | |
| I did not exercise previously | 14 (10.4%) | 15 (8.9%) | |
| Unanswered | 6 (4.4%) | 2 (1.8%) | |
| Eating habits prior to participation, n (%) | p = 0.331 | ||
| Did not think about eating habits | 13 (9.6%) | 16 (9.5%) | |
| Thought a little bit about eating habits | 79 (58.5%) | 107 (63.7%) | |
| Thought a lot about eating habits | 37 (27.4%) | 43 (25.6%) | |
| Unanswered | 6 (4.4%) | 2 (1.2%) | |
| Physically active at least 30 min daily with moderate to high intensity, n (%) | 68 (50.4%) | 83 (49.4%) | p = 0.096 |
| Unanswered | 10 (7.4%) | 4 (2.4%) | |
| Physically active with high intensity twice a week of at least 20 min duration, n (%) | 75 (55.6%) | 99 (58.9%) | p = 0.117 |
| Unanswered | 10 (7.4%) | 4 (2.4%) | |
| Having pain, soreness, stiffness or swelling within the last two weeks in at least one body region prior to CrossFit, n (%) | 70 (54.26%) | 87 (52.4%) | p = 0.752 |
| Risk Factor | Number of Participants | IRR (95%CI) | P |
|---|---|---|---|
| Male | n = 51 | 0.57 (0.22 to 1.53) | p = 0.266 |
| Reference: female | n = 117 | ||
| Higher age | n = 168 | 0.97 (0.92 to 1.02) | p = 0.247 |
| Higher BMI | n = 168 | 1.02 (0.89 to 1.16) | p = 0.818 |
| Higher number of weekly units of alcohol | n = 168 | 1.05 (0.95 to 1.15) | p = 0.366 |
| Having pain, soreness, stiffness or swelling within the last two weeks prior to CrossFit | n = 88 | 0.87 (0.40 to 1.97) | p = 0.768 |
| Reference: no problems | n = 78 | ||
| Higher number of system-registered CrossFit class attendance | n = 164 | 0.96 (0.92 to 1.01) | p = 0.144 |
| Higher number of reported minutes of weekly Open Gym training | n = 168 | 1.00 (1.00 to 1.00) | p = 0.811 |
| Higher number of minutes reported for participation in other sports | n = 168 | 1.00 (1.00 to 1.00) | p = 0.509 |
| Participated in one or two introduction classes | n = 47 | 3.04 (0.88 to 10.60) | p = 0.080 |
| Participated in all introduction classes | n = 72 | 2.56 (0.68 to 9.64) | p = 0.165 |
| Reference: did not participate in introduction classes | n = 47 | ||
| Reported to participate in sports or exercise prior to CrossFit | n = 152 | 1.09 (0.26 to 4.62) | p = 0.912 |
| Reference: did not report to participate in sports or exercise | n = 15 | ||
| Reported to meet one of the physical activity recommendations | n = 60 | 1.72 (0.60 to 4.96) | p = 0.313 |
| Reported to meet both of the physical activity recommendations | n = 61 | 1.39 (0.46 to 4.14) | p = 0.558 |
| Reference: did not meet any of the physical activity recommendations | n = 47 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larsen, R.T.; Hessner, A.L.; Ishøi, L.; Langberg, H.; Christensen, J. Injuries in Novice Participants during an Eight-Week Start up CrossFit Program—A Prospective Cohort Study. Sports 2020, 8, 21. https://doi.org/10.3390/sports8020021
Larsen RT, Hessner AL, Ishøi L, Langberg H, Christensen J. Injuries in Novice Participants during an Eight-Week Start up CrossFit Program—A Prospective Cohort Study. Sports. 2020; 8(2):21. https://doi.org/10.3390/sports8020021
Chicago/Turabian StyleLarsen, Rasmus Tolstrup, Andreas Lund Hessner, Lasse Ishøi, Henning Langberg, and Jan Christensen. 2020. "Injuries in Novice Participants during an Eight-Week Start up CrossFit Program—A Prospective Cohort Study" Sports 8, no. 2: 21. https://doi.org/10.3390/sports8020021