
Building Water Quality Commissioning in Healthcare Settings: Reducing Legionella and Water Contaminants Utilizing a Construction Scheduling Method



Abstract
:1. Introduction
1.1. Healthcare Construction, Scheduling, and Commissioning
1.2. Current Construction Industry Practices
2. Materials and Methods
2.1. Construction Scheduling Method
2.2. BWQC Construction Schedule Tasks and Milestones
2.3. BWQC Roles and Responsibilities
3. Results
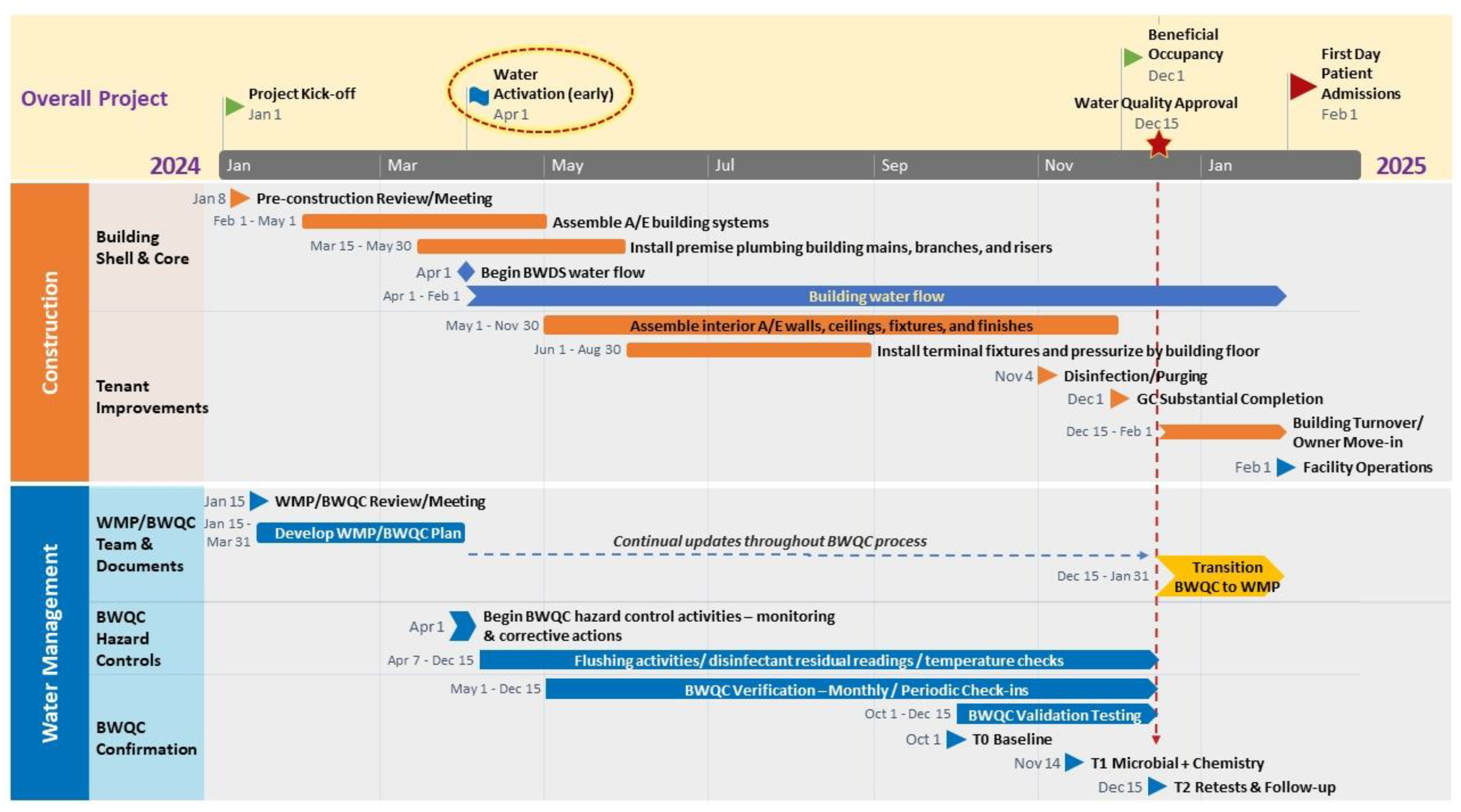
3.1. Gantt Chart Results
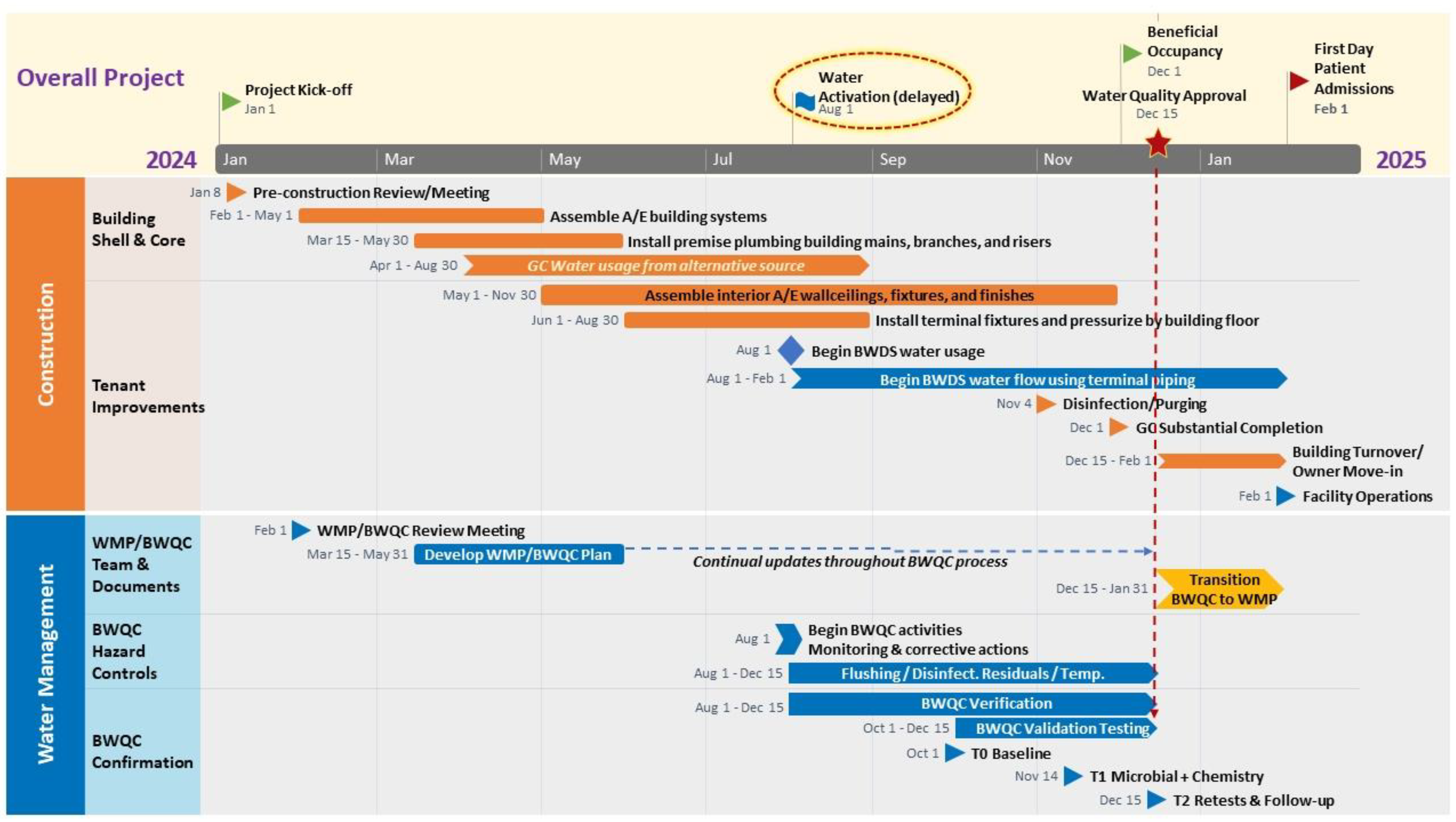
3.2. Adapting Gantt Chart for Project-Specific Results
4. Discussion
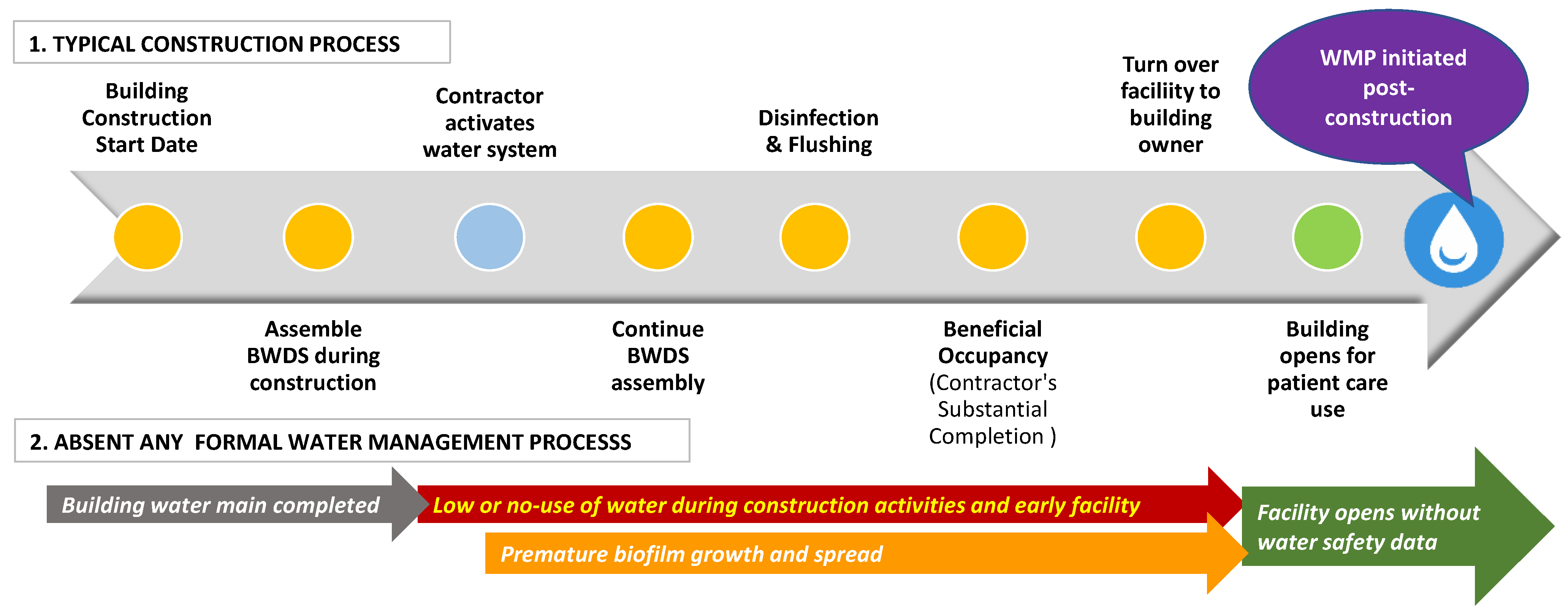
4.1. Construction Activities without Commissioning
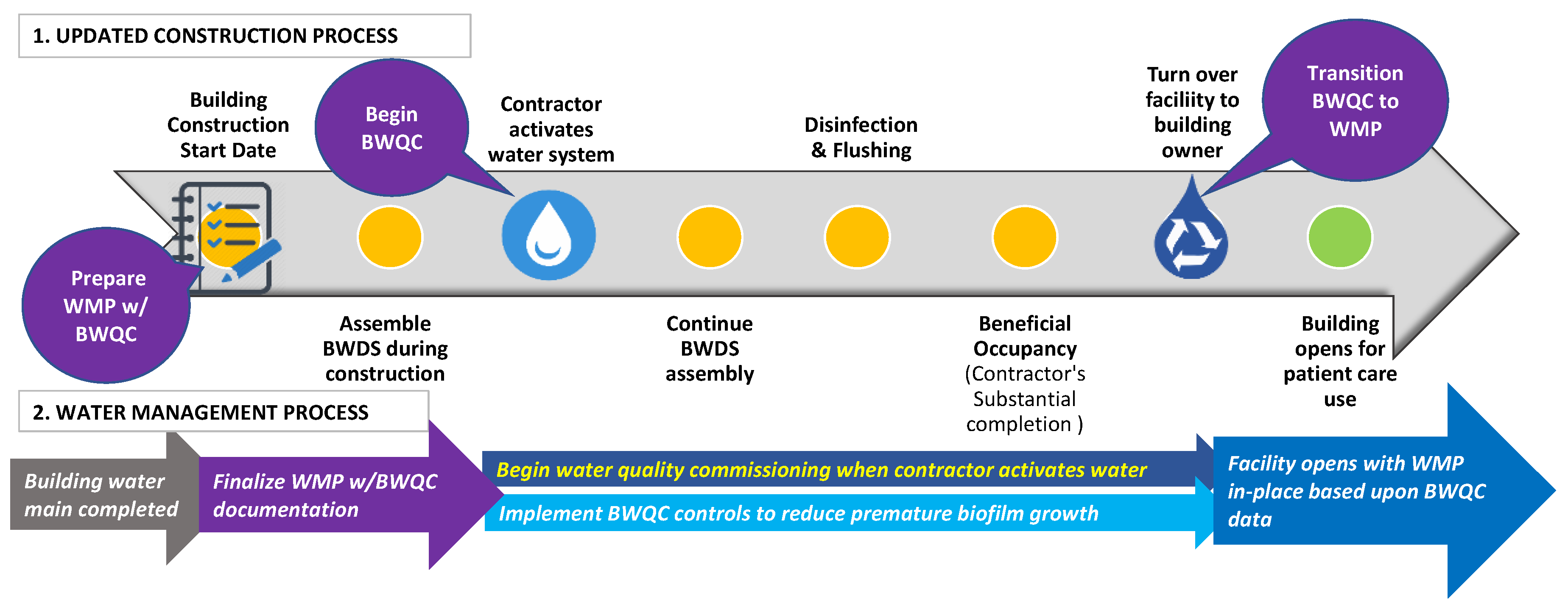
4.2. Construction Activities with Pseudo Commissioning Efforts
4.3. A/E/C and CxA Professional Liability
4.4. Future Smart Building Water Systems
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Walker, J.T.; Surman-Lee, S.; McDermott, P.J.; Weinbren, M. Safe Water in Healthcare: A Practical and Clinical Guide, 1st ed.; Elsevier Science & Technology: San Diego, CA, USA, 2023. [Google Scholar]
- Scanlon, M.M.; Gordon, J.L.; McCoy, W.F.; Cain, M.F. Water management for construction: Evidence for risk characterization in community and healthcare settings: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 2168. [Google Scholar] [CrossRef] [PubMed]
- Maynard, E. An overview of a seminar on patient infections and drinking water management within healthcare buildings in the UK. Perspect. Public Health 2020, 140, 79. [Google Scholar] [CrossRef] [PubMed]
- Hayward, C.; Ross, K.E.; Brown, M.H.; Whiley, H. Water as a source of antimicrobial resistance and healthcare-associated infections. Pathogens 2020, 9, 667. [Google Scholar] [CrossRef] [PubMed]
- Kanamori, H.; Weber, D.J.; Rutala, W.A. Healthcare outbreaks associated with a water reservoir and infection prevention strategies. Clin. Infect. Dis. 2016, 62, 1423–1435. [Google Scholar] [CrossRef]
- ASHRAE. ANSI/ASHRAE Standard 514 Risk Management for Building Water Systems: Physical, Chemical, and Microbial Hazards; American Society of Heating Refrigerating and Air Conditioning Engineers: Atlanta, GA, USA, 2023; pp. 1–88. [Google Scholar]
- ASHRAE. ANSI/ASHRAE Standard 188 Legionellosis: Risk Management for Building Water Systems; American Society of Heating Refrigerating and Air Conditioning Engineers: Atlanta, GA, USA, 2021; pp. 1–24. [Google Scholar]
- ASHRAE. ASHRAE Guideline 12-2020 Managing the Risk of Legionellosis Associated with Building Water Systems; American Society of Heating Refrigerating and Air Conditioning Engineers: Atlanta, GA, USA, 2020; pp. 1–54. [Google Scholar]
- Proctor, C.R.; Rhoads, W.J.; Keane, T.; Salehi, M.; Hamilton, K.; Pieper, K.J.; Cwiertny, D.M.; Prévost, M.; Whelton, A.J. Considerations for large building water quality after extended stagnation. AWWA Water Sci. 2020, 2, e1186. [Google Scholar] [CrossRef] [PubMed]
- CDC. Toolkit for Controlling Legionella in Common Sources of Exposure: Information on Controlling Legionella in Commonly Implicated Sources of Legionnaires’ Disease Outbreaks; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021; pp. 1–27. [Google Scholar]
- Leslie, E.; Hinds, J.; Hai, F.I. Causes, factors and control measures of opportunistic premise plumbing pathogens—A critical review. Appl. Sci. 2021, 11, 4474. [Google Scholar] [CrossRef]
- Centers for Medicare and Medicaid Services. Requirement to reduce legionella risk in healthcare facility water systems to prevent cases and outbreaks of Legionnaires’ disease. In Policy and Memos to States and Regions, Services; CMS.gov: Baltimore, MD, USA, 2018; pp. 1–3. [Google Scholar]
- CDC. Developing a Water Management Program to Reduce Legionella Growth and Spread in Buildings: A Practical Guide to Implementing Industry Standards; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021; pp. 1–36.
- Facility Guidelines Institute. FGI Guidelines for the Design and Construction of Hospitals; FGI with American Society of Healthcare Engineering: St. Louis, MO, USA, 2022. [Google Scholar]
- United States Department of Veteran Affairs. Prevention of Health Care-Associated Legionella Disease and Scald Injury from Water Systems VHA Directive 1061; United States Department of Veteran Affairs: Washington, DC, USA, 2021; p. 60.
- The Joint Commission. R3 Report Issue 32: New Standard for Water Management Program. Available online: https://www.jointcommission.org/standards/r3-report/r3-report-issue-32-new-standard-for-water-management-program/ (accessed on 15 August 2023).
- Van Kenhove, E.; Dinne, K.; Janssens, A.; Laverge, J. Overview and comparison of Legionella regulations worldwide. Am. J. Infect. Control 2019, 47, 968–978. [Google Scholar] [CrossRef]
- Fullerton, J.; Hota, S. Construction and Remodeling in the Healthcare Environment: The Critical Role of the Healthcare Epidemiologist. In Infection Prevention: New Perspectives and Controversies; Bearman, G., Morgan, D.J.K., Murthy, R., Hota, S., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 379–386. [Google Scholar]
- National Health Service England. Health Service England. Health Technical Memorandum 04-01: Safe water in healthcare premises. In Part A: Design, Installation and Commissioning; National Health Service England: London, UK, 2016. [Google Scholar]
- Sylvestre, E.; Julian, T. Legionella Control in Building Water Systems: A Guide for Building Managers and Operators; EAWAG Aquatic Research: Dubendorf, Switzerland, 2023; Volume 16, p. 60. [Google Scholar]
- Scanlon, M.M.; Gordon, J.L.; Tonozzi, A.A.; Griffin, S.C. Reducing the Risk of Healthcare Associated Infections from Legionella and Other Waterborne Pathogens Using a Water Management for Construction (WMC) Infection Control Risk Assessment (ICRA) Tool. Infect. Dis. Rep. 2022, 14, 341–359. [Google Scholar] [CrossRef]
- APIC. Infection Prevention Manual for Construction & Renovation, 1st ed.; Vogel, R., Ed.; Association for Professionals in Infection Control and Epidemiology: Arlington, VA, USA, 2015; p. 164. [Google Scholar]
- Gamage, S.D.; Ambrose, M.; Kralovic, S.M.; Roselle, G.A. Water Safety and Health Care: Preventing Infections Caused by Opportunistic Premise Plumbing Pathogens. Infect. Dis. Clin. N. Am. 2021, 35, 667–695. [Google Scholar] [CrossRef]
- Olmsted, R.N. Reimagining Construction and Renovation of Health Care Facilities During Emergence from a Pandemic. Infect. Dis. Clin. N. Am. 2021, 35, 697–716. [Google Scholar] [CrossRef]
- Ficheux, A.; Réthoret, J.; Laget, J.; Baux, C.; Gayrard, N.; Duranton, F.; Vetromile, F.; Szwarc, I.; Cazevieille, C.; Servel, M.-F.; et al. Successful Disinfection of a New Healthcare Facility Contaminated with Pseudomonas aeruginosa. Hygiene 2022, 2, 1–13. [Google Scholar] [CrossRef]
- Weinbren, M.J. Dissemination of antibiotic resistance and other healthcare waterborne pathogens. The price of poor design, construction, usage and maintenance of modern water/sanitation services. J. Hosp. Infect. 2020, 105, 406–411. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Management of Legionella in Water Systems; The National Academies Press: Washington, DC, USA, 2020; p. 290. [Google Scholar]
- Rhoads, W.J.; Pruden, A.; Edwards, M.A. Survey of green building water systems reveals elevated water age and water quality concerns. Environ. Sci. Water Res. Technol. 2016, 2, 164–173. [Google Scholar] [CrossRef]
- Griffin, S.C.; Scanlon, M.M.; Reynolds, K.A. Managing Building Water Disruptions in a Post-COVID World: Water Quality and Safety Risk Assessment Tool for Academic Institutions and School Settings. Buildings 2023, 13, 921. [Google Scholar] [CrossRef]
- Iskandar, K.A.; Hanna, A.S.; Lotfallah, W. Modeling the performance of healthcare construction projects. Eng. Constr. Archit. Manag. 2019, 26, 2023–2039. [Google Scholar] [CrossRef]
- Collins, W.; Holley, P.; Chavan, A.; Sattineni, A. general contractor knowledge of infection control requirements on hospital renovation construction projects. In Collaboration and Integration in Construction, Engineering, Management and Technology. Advances in Science, Technology & Innovation; Springer: Cham, Switzerland, 2021; pp. 63–67. [Google Scholar]
- Kaba, A.; Barnes, S. Commissioning simulations to test new healthcare facilities: A proactive and innovative approach to healthcare system safety. Adv. Simul. 2019, 4, 17. [Google Scholar] [CrossRef]
- Howie, G. Scheduling for project success. Health Facil. Manag. 2021, 34, 32–35. [Google Scholar]
- Guzman, K.; Agner, J.; Aguilera, L.; Stevenson, K. Simplifying the Complex: A Guide to Transition and Activation Planning for Healthcare Construction Projects; Emerald Publishing Limited: Bingley, UK, 2020; p. 101. [Google Scholar]
- Mubarak, S.A. Construction Project Scheduling and Control, 3rd ed.; Wiley: Somerset, UK, 2015. [Google Scholar]
- Howe, T.; Myers, M.; Pickett, J. Deliver smart buildings using CSI Division 25, commissioning: The use of CSI Division 25 and commissioning are critical to the successful design and operation of a smart building. Consult. Specif. Eng. 2021, 58, 36. [Google Scholar]
- Sidari, F.P. A water-safety approach to design and construction: Perform environmental testing for Legionella before and after building occupancy. PM Eng. 2019, 25, 28–31. [Google Scholar]
- Sidari, F.P. Are all waterborne pathogens created equally? Engineers and building professionals need to understand a little about the microbiology and epidemiology of these organisms. PM Eng. 2019, 25, 98. [Google Scholar]
- De Giglio, O.; Diella, G.; Lopuzzo, M.; Triggiano, F.; Calia, C.; Pousis, C.; Fasano, F.; Calabrese, G.; Rafaschieri, V.; Carpagnano, L.F.; et al. Management of Microbiological Contamination of the Water Network of a Newly Built Hospital Pavilion. Pathogens 2021, 10, 75. [Google Scholar] [CrossRef] [PubMed]
- Francois Watkins, L.K.; Toews, K.-A.E.; Harris, A.M.; Davidson, S.; Ayers-Millsap, S.; Lucas, C.E.; Hubbard, B.C.; Kozak-Muiznieks, N.A.; Khan, E.; Kutty, P.K. Lessons From an Outbreak of Legionnaires’ Disease on a Hematology-Oncology Unit. Infect. Control Hosp. Epidemiol. 2017, 38, 306–313. [Google Scholar] [CrossRef] [PubMed]
- van der Mee-Marquet, N.; Bloc, D.; Briand, L.; Besnier, J.M.; Quentin, R. Non-touch fittings in hospitals: A procedure to eradicate Pseudomonas aeruginosa contamination. J. Hosp. Infect. 2005, 60, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.W.; Lewis, S.S.; Alexander, B.D.; Chen, L.F.; Wallace, R.J.; Brown-Elliott, B.A.; Isaacs, P.J.; Pickett, L.C.; Patel, C.B.; Smith, P.K.; et al. Two-Phase Hospital-Associated Outbreak of Mycobacterium abscessus: Investigation and Mitigation. Clin. Infect. Dis. 2017, 64, 902. [Google Scholar] [CrossRef]
- Johnson, R.C.; Deming, C.; Conlan, S.; Zellmer, C.J.; Michelin, A.V.; Lee-Lin, S.; Thomas, P.J.; Park, M.; Weingarten, R.A.; Less, J.; et al. Investigation of a Cluster of Sphingomonas koreensis Infections. N. Engl. J. Med. 2018, 379, 2529–2539. [Google Scholar] [CrossRef]
- Dipping, J.; Scanlon, M.M. 5 Tips for reducing Legionella risk: Utilizing water management for construction and commissioning buildings. Plumb. Mech. Eng. 2022, 28, 1–5. [Google Scholar]
- Ellis, R. Plumbing Systems Commissioning. PM Eng. 2008, 14, 41–46. [Google Scholar]
- Office Timeline. Make Impressive Powerpoint Timelines with Just a Few Clicks. Available online: https://www.officetimeline.com/ (accessed on 30 June 2023).
- Simmons, S. ASHRAE to Continue Development of Building Water Management Standard; American Society of Heating, Refrigerating and Air-Conditioning Engineers: Atlanta, GA, USA, 2019. [Google Scholar]
- Krageschmidt, D.A.; Kubly, A.F.; Browning, M.S.; Wright, A.J.; Lonneman, J.D.; Detmer, M.J.; McCoy, W.F. A Comprehensive Water Management Program for Multicampus Healthcare Facilities. Infect. Control Hosp. Epidemiol. 2014, 35, 556–563. [Google Scholar] [CrossRef]
- Demirjian, A.; Lucas, C.E.; Garrison, L.E.; Kozak-Muiznieks, N.A.; States, S.; Brown, E.W.; Wortham, J.M.; Beaudoin, A.; Casey, M.L.; Marriott, C.; et al. The importance of clinical surveillance in detecting Legionnaires’ disease outbreaks: A large outbreak in a hospital with a Legionella disinfection system-Pennsylvania, 2011–2012. Clin. Infect. Dis. 2015, 60, 1596–1602. [Google Scholar] [CrossRef]
- New York State Department of Health. Environmental Health Information Related to Legionellosis in Healthcare Facilities; New York State Department of Health: New York, NY, USA, 2019; p. 17.
- Scanlon, M.M. Raising Awareness about Water Safety During Construction. Work. Press. 2018, 1, 11–16. [Google Scholar]
- Richardson, C. Facility-borne illness poses environmental risk in hospital construction. Healthc. Financ. Manag. 2013, 67, 126. [Google Scholar]
- Collier, S.A.; Deng, L.; Adam, E.A.; Benedict, K.M.; Beshearse, E.M.; Blackstock, A.J.; Bruce, B.B.; Derado, G.; Edens, C.; Fullerton, K.E.; et al. Estimate of burden and direct healthcare cost of infectious waterborne disease in the United States. Emerg. Infect. Dis. 2021, 27, 140–149. [Google Scholar] [CrossRef]
- Inkster, T.; Peters, C.; Wafer, T.; Holloway, D.; Makin, T. Investigation and control of an outbreak due to a contaminated hospital water system, identified following a rare case of Cupriavidus pauculus bacteraemia. J. Hosp. Infect. 2021, 111, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Lecointe, D.; Beauvais, R.; Breton, N.; Cailleret, R.; Pangon, B. Control of legionellae in a new healthcare facility following implementation of a thermal control strategy. Infect. Dis. 2019, 51, 102–112. [Google Scholar] [CrossRef]
- Nakamura, I.; Miura, Y.; Umeda, A.; Imura, R.; Watanabe, Y.; Watanabe, H. The Legionella contamination of tap water in a brand-new hospital in Japan before patients move in. Infect. Control Hosp. Epidemiol. 2020, 41, 998–999. [Google Scholar] [CrossRef] [PubMed]
- Cunliffe, D.; Bartram, J.; Briand, E.; Chartier, Y.; Colbourne, J.; Drury, D.; Lee, J.; Schaefer, B. Water Safety in Buildings; Surman-Lee, S., Ed.; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Boehlert, G.R.; Stout, J.E. New mandates for building water systems affect legal liability in Legionnaires’ disease cases. Probate Prop. 2012, 26, 62–64. [Google Scholar]
- Dipping, J. Plumbing engineering for 2022: A call for water intelligence in the age of smart buildings. PM Eng. 2022, 28, 18. [Google Scholar]
- Hegazy, T.; Elbeltagi, E.; Zhang, K. Keeping Better Site Records Using Intelligent Bar Charts. J. Constr. Eng. Manag. 2005, 131, 513–521. [Google Scholar] [CrossRef]
- Mehrbod, S.; Staub-French, S.; Tory, M. BIM-based building design coordination: Processes, bottlenecks, and considerations. Can. J. Civ. Eng. 2020, 47, 25–36. [Google Scholar] [CrossRef]
- Rolfsen, C.N.; Merschbrock, C. Corrigendum to Acceptance of Construction Scheduling Visualizations: Bar-charts, Flowline-charts, Or Perhaps BIM? Procedia Eng. 2016, 164, 558–565. [Google Scholar] [CrossRef]
- Bedard, E.; Prevost, M.; Deziel, E. Pseudomonas aeruginosa in premise plumbing of large buildings. Microbiol. Open 2016, 5, 937–956. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Discipline | Phase | Key Tasks/ Milestones | Key Team Leader(s) | Description |
|---|---|---|---|---|
| Overall Project | N/A | Project Kick-off | GC, BOR | The first day the GC is contractually engaged to perform work on the construction project [44]. |
| Water Activation | GC, CxA, BOR | The first date water is flowing in any section or component of BWDS beyond the building’s main point of entry [3,44]. | ||
| Beneficial Occupancy | GC, CxA, BOR, FM | The date GC has substantially completed the construction project and the building owner’s staff can legally and safely occupy the building. It is also referred to as the date of substantial completion for fire and life safety conditions [6,7]. | ||
| Water Quality Approval | BOR, CL, IPC, OES, WMS, CxA, AHJ | The building owner formally accepts the water quality results from the GC and deems the water quality appropriate for patient care operations [6]. | ||
| First Day of Patient Admissions | BOR, FM, IPC, CL, AHJ | A date on which the building owner plans to begin legal healthcare operations after approvals from local, state, or national AHJ and admit patients to the healthcare facility [44]. | ||
| Construction | Building Shell and Core | Pre- Construction Review Meeting | GC, SUB, A/E, BOR, FM, WMS | Similar to other core building systems, conduct a review of the BWDS design documents to ensure the system and its components meet the building owner’s WMP performance criteria (e.g., incoming water, hot and cold water distribution systems, hot water storage, and fixture types). Next, coordinate a specific meeting for the WMP/BWQC safety team to review project goals and objectives, using the overall construction project schedule as a document for discussion and agreement [44]. |
| Assemble A/E core building systems for plumbing | GC, SUB | Divide this task into levels, floors, or key departmental sections to install the premise plumbing core components of the BWDS main, branches, and risers [44]. | ||
| Building Water Flow | GC, SUB, CxA | The amount of water passing through a pipe at any given time is water flow. Water flow is affected by the width of a supply pipe. Fixture water flow can be altered by aerators, lamer flow screens, or auto-fixtures [9]. | ||
| Tenant Improvements | Assemble interior A/E systems for plumbing | GC, SUB | Divide this work effort into departments and rooms on each floor and install the premise plumbing interior finish components of the BWDS, including local branching, valves, plumbing fixtures, and fixture trim, as well as pressurizing the system [44]. | |
| Disinfection/ Purging | GC, SUB, CxA, BOR, FM, WMS | Disinfection: A form of hyperchlorination of the BWDS (chemical disinfection) toward the later stages of building construction. Chemical disinfection injects high quantities of chemicals into the BWDS above allowable drinking water limits. This water is purged eventually from the system [6,7,8]. Purging: A form of elimination of water from the BWDS in large quantities to turn water over rapidly after water disinfection activities. This is a distinct activity separate from periodic fixture flushing. | ||
| GC Substantial Completion | GC, SUB, CxA | The GC has completed a substantial portion of the project (e.g., 90% complete), and 100% of all building fire and life safety issues (e.g., fire exiting, stairs, fire alarms, smoke dampers, etc.) are complete for people to occupy the structure safely while other work (e.g., punch list items) can be completed. | ||
| Building Turnover/ Owner Move-in | BOR, FM, CxA, AHJ | The period of time in which the building owner’s facility engineering and maintenance staff take possession of the building to initiate preliminary facility operations, transition planning, and move-in/setup. The building owner is preparing for review with AHJs (national, state, or third-party agencies) for approval to admit patients into a licensed healthcare setting. | ||
| Facility Operations | BOR, FM | The building owner’s staff takes 100% control of the building and its engineering systems, including BWDS water quality and safety. The GC has completed the project contract. | ||
| Water Management | WMP/BWQC Team and Documents | WMP/BWQC Review Meeting | GC, CxA | Coordinate a meeting for the construction/commissioning water safety team to review WMP/BWQC project goals and objectives using the overall project construction schedule as a document for review, discussion, and agreement [44]. |
| WMP/BWQC Risk Assessment | BOR, CL, IPC, OES, FM, WMS | The water safety team should review the scope of the project and determine the risk of the project to building occupants (existing occupants and future occupants) [6,7,21]. | ||
| Developing WMP/BWQC Plan | BOR, FM, IPC, OES, WMS, GC | Create a WMP/BWQC document with the designated safety team for BWQC implementation during construction and commissioning activities per ANSI/ASHRAE 188 and 514 [6,7]. | ||
| Transition BWQC to WMP Documentation | GC, SUB, CxA, BOR, FM, WMS | At the conclusion of a construction project, the BWQC documentation is handed over to the building owner. The building owner transitions the BWQC from the safety team assigned during the construction/commissioning project phase toward a team focused on performing ongoing facility operations. Formal WMP team meetings are held to adjust the documentation accordingly with changes to hazard control options for ongoing facility operations [6]. | ||
| BWQC Hazard Controls | Flushing Activities | GC, SUB or BOR, FM, WMS | A hazard control to be implemented periodically to reduce the high water age and increase the movement of water through the BWDS. Establish a flushing protocol to occur on fixtures for day(s) per week and z minutes per fixture valve(s) (hot and cold) [8,9,10,48]. | |
| Disinfectant Residual Readings | GC, SUB or BOR, FM, WMS | Monitoring designated fixture locations for residual disinfectant measurements to ensure a minimum level of disinfectant residual resides within piping distribution and fixtures after the water is processed through the BWDS [10]. | ||
| Temperature Checks | GC, SUB or BOR, FM, WMS | Monitoring the temperature of water (hot and cold) at designated fixtures to ensure water temperature remains within range as defined by the water management program [10,19]. | ||
| BWQC Confirmation | BWQC Verification | BOR, WMS, CxA | The building owner and their designee(s) will verify that hazard controls are being implemented as designed for the WMP/BWQC plan on a routine basis (e.g., monthly meetings) by having periodic check-ins, including the GC [6,7]. | |
| BWQC Validation Testing | BOR, FM, CL, IPC, WMS, CxA | WMP/BWQC team to determine the type, quantity, location, and method of analytical testing for microbials (e.g., Legionella, Pseudomonas, NTM) and/or chemicals (e.g., lead, copper) [10] at each sampling date and time (T0, T1, and T2) [6,8,19,39]. | ||
| T0 Baseline | WMS, CxA, BOR, FM | Time Zero—baseline analytical testing; determine system performance after hazard controls (e.g., flushing, monitoring disinfectant residual, temperature) are implemented and prior to chemical disinfection [19,21]. | ||
| T1 Microbial + Chemistry | WMS, CxA, BOR, FM | Time One—analytical testing conducted after chemical disinfection and purging of BWDS; performed post disinfection after the system is at rest for at least 48 h [19], and suggest sampling is undertaken by an accredited laboratory independent of the GC [19] (lab processing times will vary based on analytical test types being performed). | ||
| T2 Retests and Follow-up | WMS, CxA, BOR, FM | Time Two—analytical testing after T1 is successfully completed. Perform T2 between the completion of T1 and the first day of patient care operations for any retests or additional testing to ensure the BWDS has maintained a low water age after the chemical disinfection was performed. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scanlon, M.M.; Gordon, J.L.; Reynolds, K.A. Building Water Quality Commissioning in Healthcare Settings: Reducing Legionella and Water Contaminants Utilizing a Construction Scheduling Method. Buildings 2023, 13, 2533. https://doi.org/10.3390/buildings13102533
Scanlon MM, Gordon JL, Reynolds KA. Building Water Quality Commissioning in Healthcare Settings: Reducing Legionella and Water Contaminants Utilizing a Construction Scheduling Method. Buildings. 2023; 13(10):2533. https://doi.org/10.3390/buildings13102533
Chicago/Turabian StyleScanlon, Molly M., James L. Gordon, and Kelly A. Reynolds. 2023. "Building Water Quality Commissioning in Healthcare Settings: Reducing Legionella and Water Contaminants Utilizing a Construction Scheduling Method" Buildings 13, no. 10: 2533. https://doi.org/10.3390/buildings13102533
APA StyleScanlon, M. M., Gordon, J. L., & Reynolds, K. A. (2023). Building Water Quality Commissioning in Healthcare Settings: Reducing Legionella and Water Contaminants Utilizing a Construction Scheduling Method. Buildings, 13(10), 2533. https://doi.org/10.3390/buildings13102533