
Disparities Between Older Adults’ Potential and Realized Access to Community-Based Care: A Multilevel Analysis of Geo-Referenced Check-In Data from Senior Centers in Nanjing, China


Abstract
:1. Introduction
2. Literature Review
3. Research Context, Materials and Methods
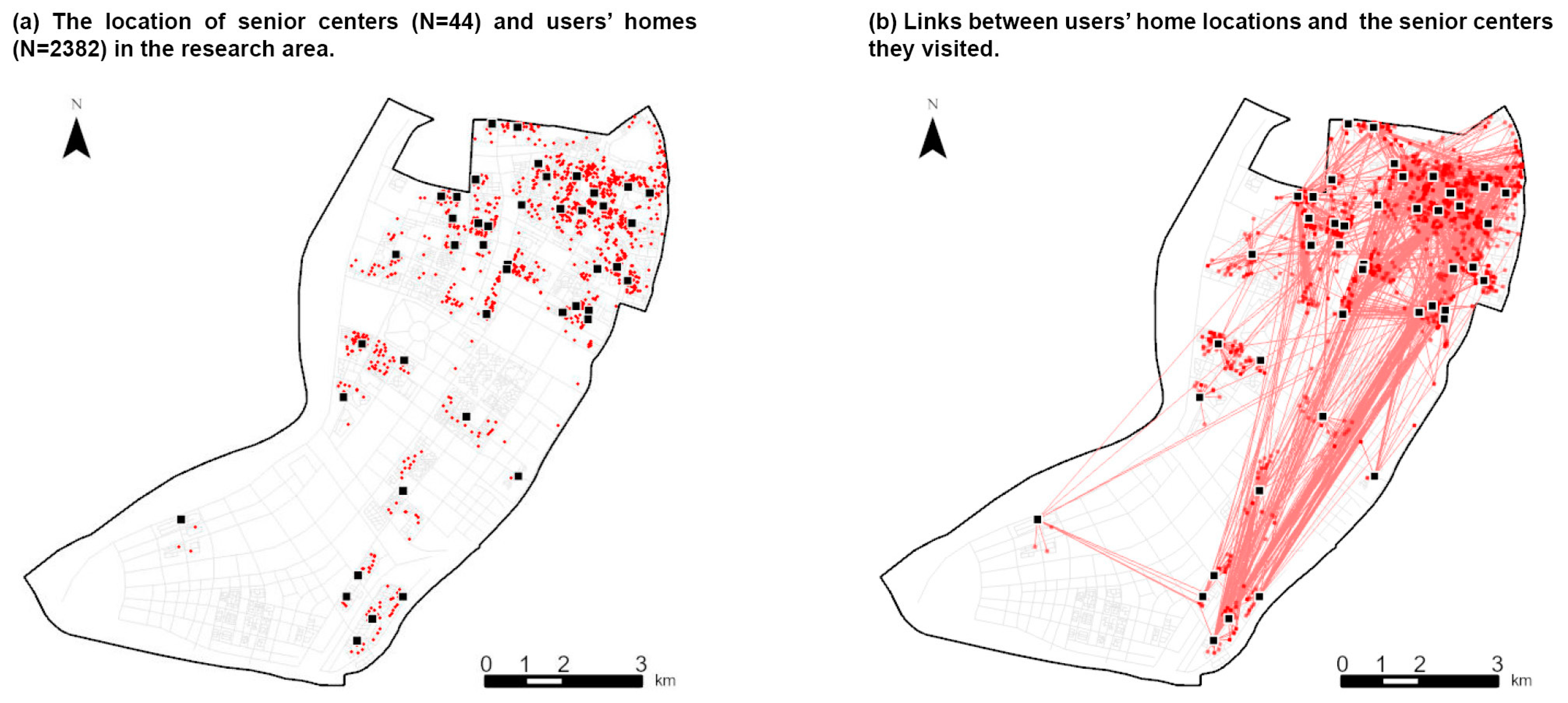
3.1. Research Context and Data
3.2. The Multilevel Analytic Framework
3.3. Models, Methods, and Variables
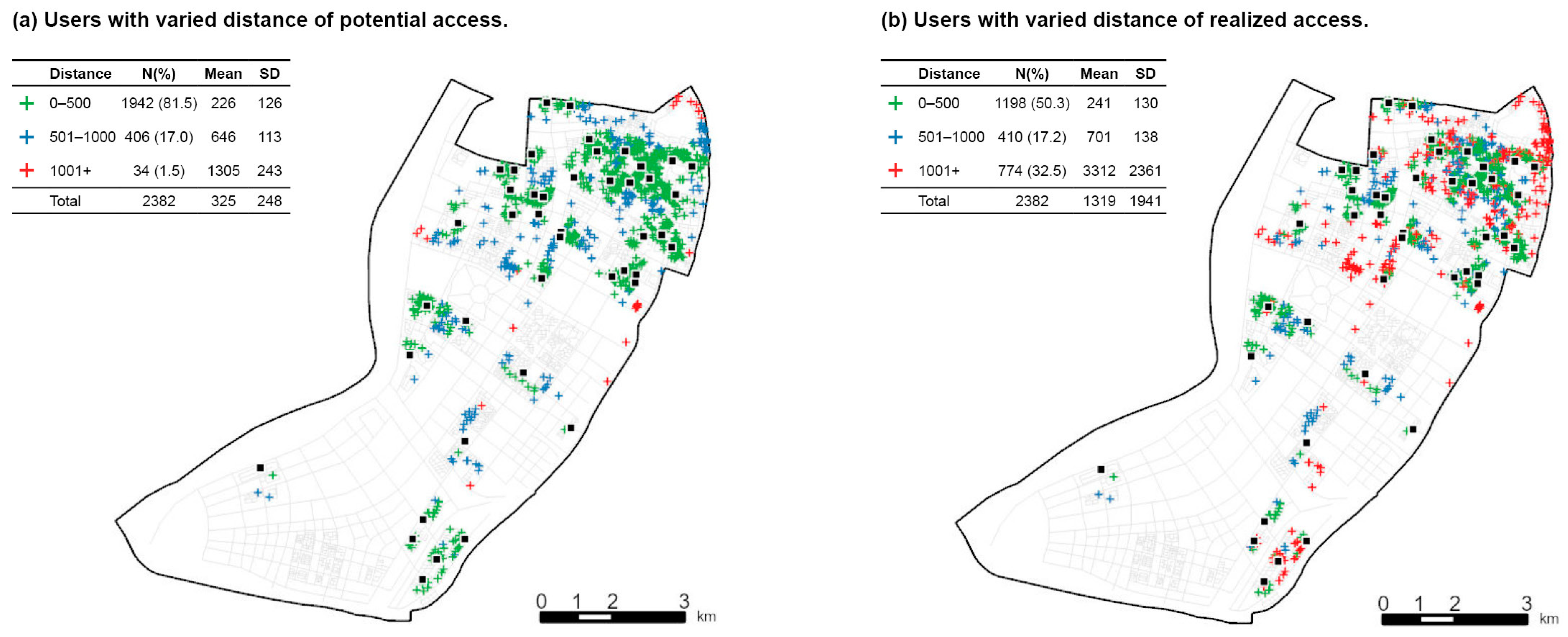
3.3.1. Defining and Characterizing the Disparity Between Potential and Realized Access
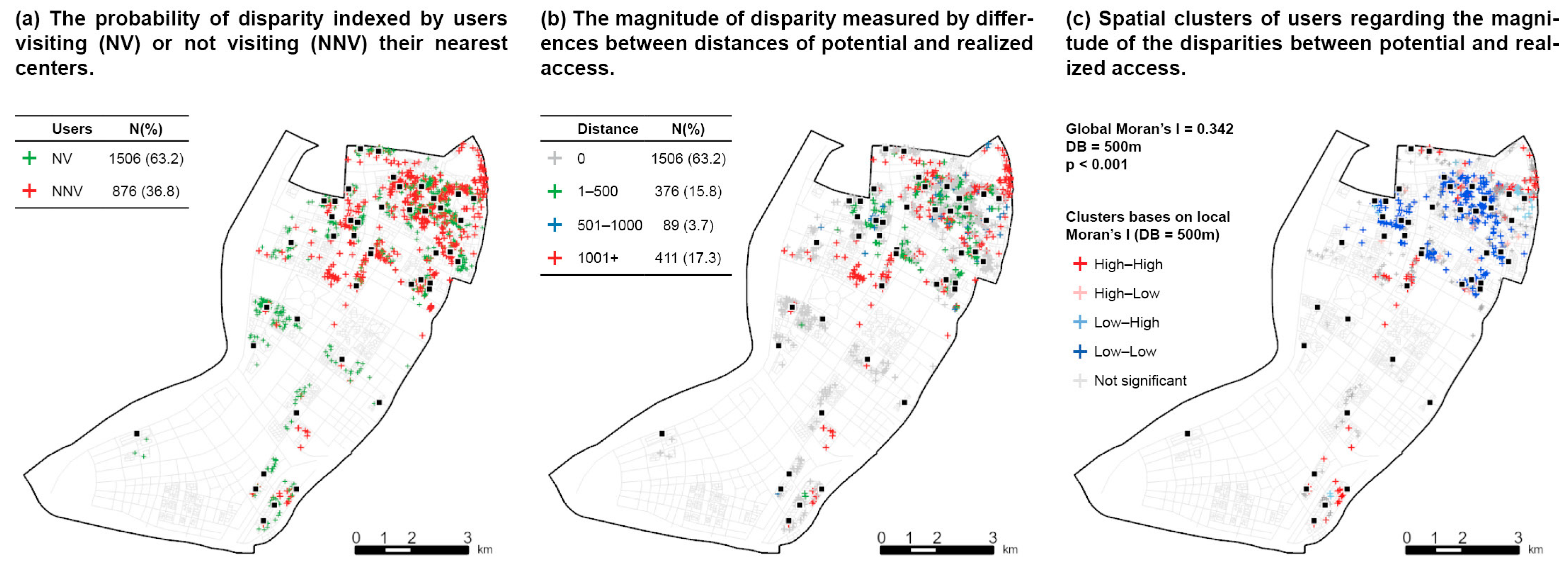
3.3.2. Spatial Patterns of the Disparity
3.3.3. Multilevel Social–Spatial Determinants of the Disparity
3.3.4. Statistic Models
4. Results
4.1. User-Level Analysis
4.1.1. A General Description of Potential and Realized Access
4.1.2. The Probability and Magnitude of Disparity
4.1.3. Spatial and Social Determinants of the Disparity
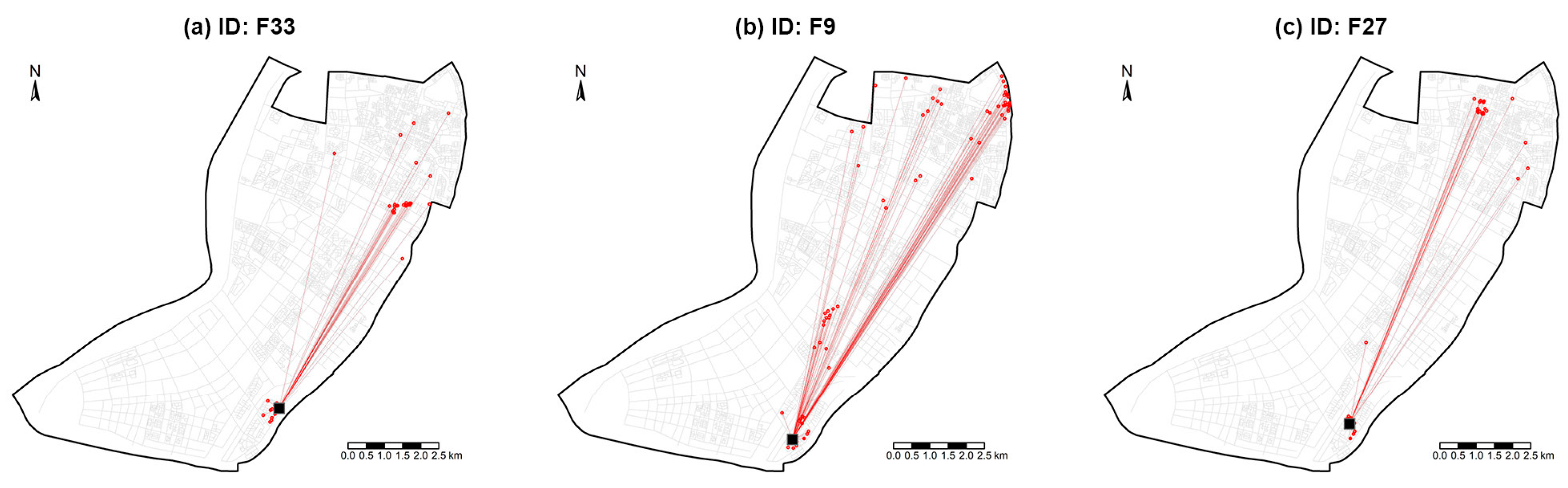
4.2. Facility-Level Analysis
4.2.1. A General Description of Potential and Realized Access to Senior Centers
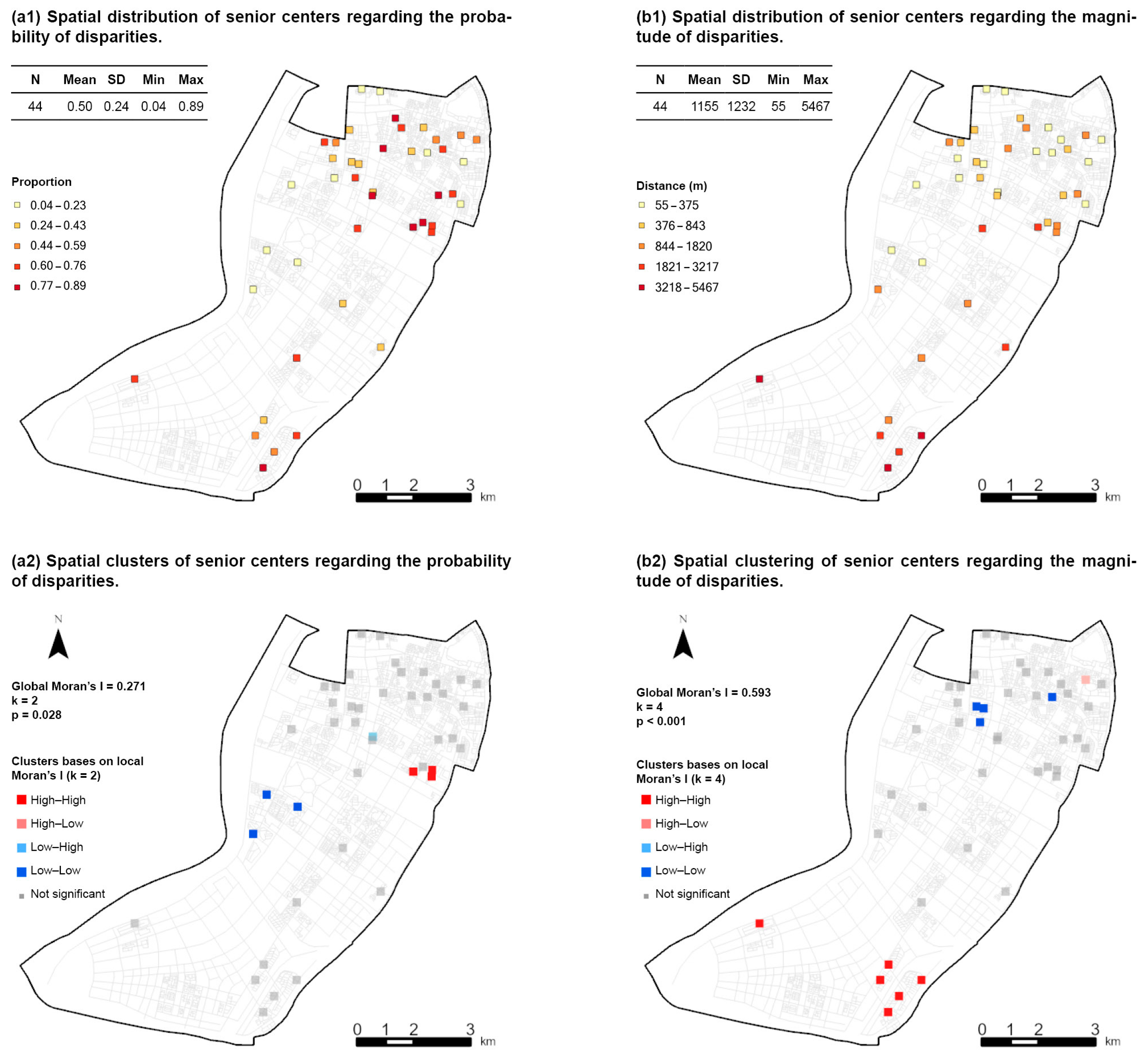
4.2.2. The Probability and Magnitude of the Disparity Among Senior Centers
4.2.3. Spatial and Social Determinants of Disparity
4.3. Summary of Main Findings
5. Discussion
5.1. The Biased Estimation of Potential Access
5.2. The Spatial Heterogeneity of the Disparities
5.3. The Role of Spatial Proximity and Other Underlying Factors
5.4. Implications for Research and Practice
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

References
- World Health Organization. Global Age-Friendly Cities: A Guide; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Tanner, D. Older People and Access to Care. Br. J. Soc. Work 2003, 33, 499–515. [Google Scholar] [CrossRef]
- Teo, P. Space to Grow Old In: The Availability of Public Spaces for Elderly Persons in Singapore. Urban Stud. 1997, 34, 419–439. [Google Scholar] [CrossRef]
- Weil, J. The New Neighborhood Senior Center: Redefining Social and Service Roles for the Baby Boom Generation; Rutgers University Press: New Brunswick, NJ, USA, 2014. [Google Scholar]
- Farone, D.W.; Fitzpatrick, T.R.; Tran, T.V. Use of Senior Centers as a Moderator of Stress-Related Distress Among Latino Elders. J. Gerontol. Soc. Work 2005, 46, 65–83. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.G.; McDougall, G.J. Comparison of Depressive Symptoms Between Homebound Older Adults and Ambulatory Older Adults. Aging Ment. Health 2007, 11, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zhang, Z. Smart Elderly Care Is an Inevitable Choice for China’s Elderly Care Services. Available online: https://news.sciencenet.cn/sbhtmlnews/2023/10/376759.shtm (accessed on 24 October 2023).
- Social Construction Committee of Nanjing. Report on Community-Based Elderly Care Service in Nanjing. Available online: http://rd.nanjing.gov.cn/rmtzx/rddy/202010/t20201020_2453967.html (accessed on 19 May 2020).
- Nanjing Municipal Government. Standard of Public Facility Planning and Provision. Available online: https://www.nanjing.gov.cn/zdgk/201502/t20150212_1056577.html (accessed on 26 January 2015).
- The State Council. The 14th Five-Year Planning on the Development of Elderly Care System. Available online: http://www.gov.cn/zhengce/content/2022-02/21/content_5674844.htm (accessed on 30 December 2021).
- Wang, N.; Ma, W. Evaluation Study on the Layout of Community Senior Living Facilities in the Main Area of Shanghai from the Perspective of Senior Life Circle. Sustainability 2023, 15, 10362. [Google Scholar] [CrossRef]
- Zhao, X.; Park, E.-S.; Kim, J.; Lee, S.-Y.; Lee, H. Basic Analysis of Physical Determinants Affecting the Distribution Density of Senior Citizen Centers around Small Apartment Complexes, Focusing on Administrative Districts in Busan. Buildings 2024, 14, 929. [Google Scholar] [CrossRef]
- Johnson, M.P.; Gorr, W.L.; Roehrig, S. Location of Service Facilities for the Elderly. Ann. Oper. Res. 2005, 136, 329–349. [Google Scholar] [CrossRef]
- Han, F.; Luo, R. A Study on the Matching of Supply and Demand for Community-based Elderly Care Services in Urban Communities Based on Accessibility Measures: A Case Study of Nanjing. Econ. Geogr. 2020, 40, 91–101. [Google Scholar]
- Borana, S.L.; Yadav, S.K. Spatial Disparity Analysis of Public Amenities in Jodhpur City. Int. Res. J. Eng. Technol. 2017, 4, 171–173. [Google Scholar]
- Ding, Q.; Zhu, L.; Luo, J. Analysing Spatial Accessibility to Residential Care Facilities in Wuhan. Hum. Geogr. 2016, 31, 36–42. [Google Scholar]
- Zhao, D.; Han, Z.; Zhao, B. A Study of Urban Pension Service Facilities Distribution Assessment Based on GIS: A Case Study of Jinzhou New District Dalian. Popul. Dev. 2017, 23, 74–81. [Google Scholar]
- Zhao, L.; He, D.; Zhao, J. Spatial Distribution and Factors Influencing Elderly Care Service Facilities based on Accessibility Evaluation—Taking Wuxi City as an Example. J. Resour. Ecol. 2024, 15, 130–139. [Google Scholar] [CrossRef]
- Guo, S.; Song, C.; Pei, T.; Liu, Y.; Ma, T.; Du, Y.; Chen, J.; Fan, Z.; Tang, X.; Peng, Y.; et al. Accessibility to urban parks for elderly residents: Perspectives from mobile phone data. Landsc. Urban Plan. 2019, 191, 103642. [Google Scholar] [CrossRef]
- Joseph, A.E.; Phillips, D.R. Accessibility and Utilization: Geographical Perspectives on Health Care Delivery; Sage: Newcastle upon Tyne, UK, 1984. [Google Scholar]
- Andersen, R.; Aday, L.A. Access to Medical Care in the US: Realized and Potential. Med. Care 1978, 16, 533–546. [Google Scholar] [CrossRef]
- Aday, L.A.; Andersen, R. A Framework for the Study of Access to Medical Care. Health Serv. Res. 1974, 9, 208. [Google Scholar]
- Shao, L.; Zhang, J.; Xu, B.; Tan, S. An Analysis of the Spatial Distribution and Demand-Supply Relation of Care Facilities for the Elderly in the Central Urban Area of Beijing. Archit. J. 2017, 10, 4–8. [Google Scholar]
- He, J.; Zhou, D.; Xu, Y.; Dai, J. The Study of Spatial Accessibility Measurement of Pension Facilities in Urban Community. Archit. J. 2018, 18, 18–22. [Google Scholar]
- Tao, Z.; Cheng, Y.; Dai, T.; Li, X. Sensitivity Analysis of Parameters in Measuring Spatial Accessibility to Public Service Facilities. Mordern Urban Res. 2017, 3, 30–35. [Google Scholar]
- Lin, S.-J.; Crawford, S.Y.; Warren Salmon, J. Potential Access and Revealed Access to Pain Management Medications. Soc. Sci. Med. 2005, 60, 1881–1891. [Google Scholar] [CrossRef]
- Luo, X.; Yue, B.; Lin, A. The Research of Accessibility and Fairness of Pension Service Facilities Based on Multiple Modes of Transportation—A Case Study of Wuhan. J. Cent. China Norm. Univ. 2018, 52, 883–893. [Google Scholar]
- Robitaille, E.; Durette, G.; Dubé, M.; Arbour, O.; Paquette, M.-C. Measuring the Potential and Realized (or Revealed) Spatial Access from Places of Residence and Work to Food Outlets in Rural Communities of Québec, Canada. ISPRS Int. J. Geo-Inf. 2024, 13, 43. [Google Scholar] [CrossRef]
- Gomez, D.; Haas, B.; Doumouras, A.G.; Zagorski, B.; Ray, J.; Rubenfeld, G.; McLellan, B.A.; Boyes, D.M.; Nathens, A.B. A Population-Based Analysis of the Discrepancy Between Potential and Realized Access to Trauma Center Care. Ann. Surg. 2013, 257, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M. What research in motivation suggests for public health. Am. J. Public Health Nations Health 1960, 50, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Suchman, E.A. Health orientation and medical care. Am. J. Public Health Nations Health 1966, 56, 97–105. [Google Scholar] [CrossRef]
- Andersen, R. A Behavioral Model of Families’ Use of Health Services; Center for Health Administration Studies, University of Chicago: Chicago, IL, USA, 1968. [Google Scholar]
- Cheng, Y.; Rosenberg, M.W.; Wang, W.Y.; Yang, L.S.; Li, H.R. Access to Residential Care in Beijing, China: Making the Decision to Relocate to a Residential Care Facility. Ageing Soc. 2012, 32, 1277–1299. [Google Scholar] [CrossRef]
- Nanjing Municipal Government. The Seventh National Population Census of Nanjing City. Available online: https://www.nanjing.gov.cn/zdgk/202105/t20210524_2946168.html (accessed on 24 May 2021).
- Joseph, A.E.; Poyner, A. Interpreting Patterns of Public Service Utilization in Rural Areas. Econ. Geogr. 1982, 58, 262–273. [Google Scholar] [CrossRef]
- Anselin, L. Spatial Econometrics: Methods and Models; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2013; Volume 4. [Google Scholar]
- Sauer, J.; Oshan, T.; Rey, S.; Wolf, L.J. The importance of null hypotheses: Understanding differences in local Moran’s under heteroskedasticity. Geogr. Anal. 2022, 54, 752–768. [Google Scholar] [CrossRef]
- Davidoff, T. Labor Income, Housing Prices, and Homeownership. J. Urban Econ. 2006, 59, 209–235. [Google Scholar] [CrossRef]
- Yang, Z.; Shen, Y. The Affordability of Owner Occupied Housing in Beijing. J. Hous. Built Environ. 2008, 23, 317–335. [Google Scholar] [CrossRef]
- Peng, C.-Y.J.; Lee, K.L.; Ingersoll, G.M. An Introduction to Logistic Regression Analysis and Reporting. J. Educ. Res. 2002, 96, 3–14. [Google Scholar] [CrossRef]
- Krout, J.A.; Cutler, S.J.; Coward, R.T. Correlates of Senior Center Participation: A National Analysis. Gerontol. 1990, 30, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Strain, L.A. Senior Centres: Who Participates? Can. J. Aging La Rev. Can. Du Vieil. 2001, 20, 471–492. [Google Scholar] [CrossRef]
- Dunn, P.K.; Smyth, G.K. Generalized Linear Models with Examples in R; Springer: Berlin/Heidelberg, Germany, 2018; Volume 53. [Google Scholar]
- Moran, J.L.; Solomon, P.J.; Peisach, A.R.; Martin, J. New Models for Old Questions: Generalized Linear Models for Cost Prediction. J. Eval. Clin. Pract. 2007, 13, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Salem, A.B.Z.; Mount, T.D. A Convenient Descriptive Model of Income Distribution: The Gamma Density. Econom. J. Econom. Soc. 1974, 42, 1115–1127. [Google Scholar] [CrossRef]
- Diehr, P.; Yanez, D.; Ash, A.; Hornbrook, M.; Lin, D.Y. Methods for Analyzing Health Care Utilization and Costs. Annu. Rev. Public Health 1999, 20, 125–144. [Google Scholar] [CrossRef]
- Thatcher, E.; Johnson, C.; Zenk, S.N.; Kulbok, P. Retail Food Store Access in Rural Appalachia: A Mixed Methods Study. Public Health Nurs. 2017, 34, 245–255. [Google Scholar] [CrossRef]
- Rui, Y.; Yang, Z.; Qian, T.; Khalid, S.; Xia, N.; Wang, J. Network-Constrained and Category-Based Point Pattern Analysis for Suguo Retail Stores in Nanjing, China. Int. J. Geogr. Inf. Sci. 2016, 30, 186–199. [Google Scholar] [CrossRef]
- Lin, S.; Deng, H.; Wang, Y.; Chen, S. Potential and Realized Access to Healthcare Services in Wuhan Metropolitan Area, China. Trans. Plan. Urban Res. 2023, 3, 97–120. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N (%)/Mean (SD) |
|---|---|
| User’s probability of disparity (PRBU) | |
| NV (0) | 1506 (63.2%) |
| NNV (1) | 876 (36.8%) |
| User’s magnitude of disparity (MAGU) | 1635 (2165) |
| Center’s probability of disparity (PRBC) | 0.50 (0.24) |
| Center’s magnitude of disparity (MAGC) | 1155 (1232) |
| Variables | N (%)/Mean (SD) |
|---|---|
| Age | |
| 70–75 | 1036 (43.5%) |
| 76–80 | 506 (21.2%) |
| 81–85 | 510 (21.4%) |
| 86+ | 330 (13.9%) |
| Gender | |
| Male | 1066 (44.8%) |
| Female | 1316 (55.2%) |
| Household composition | |
| Alone | 218 (9.2%) |
| With only spouse | 314 (13.2%) |
| With others | 1799 (75.6%) |
| Physical Capacity | |
| Independent | 2323 (97.5%) |
| Semi-independent | 50 (2.1%) |
| Dependent | 9 (0.4%) |
| House price (RMB/m2) | 41,471 (8396) |
| Community age (year) | 21 (7) |
| Distance to the city center (meter) | 5437 (2188) |
| Variables | Mean (SD) |
|---|---|
| Density of older population (N/km2) | 2649 (2485) |
| Distance to the city center (meter) | 6629 (2820) |
| Closeness to commercial amenities | 0.31 (0.35) |
| Closeness to public transport | 0.21 (0.01) |
| Closeness to medical centers | 0.02 (0.06) |
| Closeness to parks | 0.02 (0.06) |
| Service rank | 3.13 (0.67) |
| Facility size (m2) | 340 (225) |
| Variables | Probability (PRBU) | Magnitude (MAGU) | ||||
|---|---|---|---|---|---|---|
| Odd Ratios | CI | Z | Odds Ratios | CI | Z | |
| Intercept | 7.23 *** | 1.07–1.62 | 6.99 | 7.37 * | 1.21–41.69 | 2.26 |
| Age | ||||||
| 70–75 (ref) | ||||||
| 76–80 | 1.08 | 0.85–1.38 | 0.64 | 0.90 | 0.71–1.15 | −0.85 |
| 81–85 | 1.19 | 0.93–1.51 | 1.40 | 1.14 | 0.90–1.46 | 1.12 |
| 86+ | 1.13 | 0.84–1.50 | 0.82 | 1.28 | 0.97–1.71 | 1.68 |
| Gender | ||||||
| Male (ref) | ||||||
| Female | 0.89 | 0.74–1.07 | −1.27 | 1.10 | 0.91–1.31 | 0.99 |
| Household | ||||||
| Alone | 0.69 * | 0.50–0.96 | −2.21 | 0.83 | 0.61–1.17 | −1.11 |
| With spouse | 0.81 | 0.62–1.06 | −1.52 | 1.28 | 0.98–1.70 | 1.79 |
| With others (ref) | ||||||
| House price | 0.55 *** | 0.46–0.65 | −6.78 | 0.86 | 0.73–1.04 | −1.42 |
| Community age | 0.40 *** | 0.29–0.53 | −6.19 | 1.35 | 0.94–1.96 | 1.75 |
| Distance to city center | 0.63 *** | 0.58–0.69 | −10.91 | 1.06 | 0.97–1.15 | 1.23 |
| Distance of potential access | 1.34 *** | 1.28–1.40 | 12.96 | 1.08 *** | 1.04–1.12 | 4.44 |
| Log-likelihood | −1383.04 | −3226.77 | ||||
| AIC | 2788.08 | 6477.55 | ||||
| Pseudo R2 | 0.148 | 0.093 | ||||
| Variables | The Probability (PRBC) | The Magnitude (MAGC) | ||||
|---|---|---|---|---|---|---|
| Odd Ratios | CI | Z | Odds Ratios | CI | Z | |
| (Intercept) | 1.04 | 0.60–1.83 | 0.15 | 4.05 | 0.73–22.22 | 1.60 |
| Older population density | 0.96 | 0.91–1.00 | −1.82 | 0.82 * | 0.90–1.00 | −2.01 |
| Distance to city center | 0.96 * | 0.91–1.00 | −1.99 | 1.21 *** | 1.09–1.35 | 3.39 |
| Commercial amenities | 3.26 *** | 2.04–5.28 | 4.85 | 1.92 | 0.59–8.06 | 1.10 |
| Public transportation | 1.49 * | 1.08–2.05 | 2.41 | 0.69 | 0.30–1.66 | −0.78 |
| Medical centers | 0.84 | 0.39–1.78 | −0.46 | 1.79 | 0.46–16.08 | 0.74 |
| Parks | 1.71 ** | 0.55–0.92 | 2.64 | 0.86 | 0.31–2.99 | −0.26 |
| Service quality | 1.21 * | 1.03–1.41 | 2.32 | 0.95 | 0.83–1.10 | −0.66 |
| Facility size | 1.90 *** | 0.86–0.95 | 4.16 | 0.89 | 0.53–1.50 | −0.45 |
| Log-likelihood | −478.11 | −137.75 | ||||
| AIC | 974.22 | 295.51 | ||||
| Pseudo R2 | 0.140 | 0.564 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Xu, Z. Disparities Between Older Adults’ Potential and Realized Access to Community-Based Care: A Multilevel Analysis of Geo-Referenced Check-In Data from Senior Centers in Nanjing, China. Buildings 2024, 14, 3900. https://doi.org/10.3390/buildings14123900
Li X, Xu Z. Disparities Between Older Adults’ Potential and Realized Access to Community-Based Care: A Multilevel Analysis of Geo-Referenced Check-In Data from Senior Centers in Nanjing, China. Buildings. 2024; 14(12):3900. https://doi.org/10.3390/buildings14123900
Chicago/Turabian StyleLi, Xiaoming, and Zhixin Xu. 2024. "Disparities Between Older Adults’ Potential and Realized Access to Community-Based Care: A Multilevel Analysis of Geo-Referenced Check-In Data from Senior Centers in Nanjing, China" Buildings 14, no. 12: 3900. https://doi.org/10.3390/buildings14123900
APA StyleLi, X., & Xu, Z. (2024). Disparities Between Older Adults’ Potential and Realized Access to Community-Based Care: A Multilevel Analysis of Geo-Referenced Check-In Data from Senior Centers in Nanjing, China. Buildings, 14(12), 3900. https://doi.org/10.3390/buildings14123900