
A Multilevel Analysis of Risk and Protective Factors for Adolescent Childbearing in Malawi



Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Outcome Variable
2.3. Explanatory Variables
2.4. Multilevel Modelling
Model Specification
3. Results
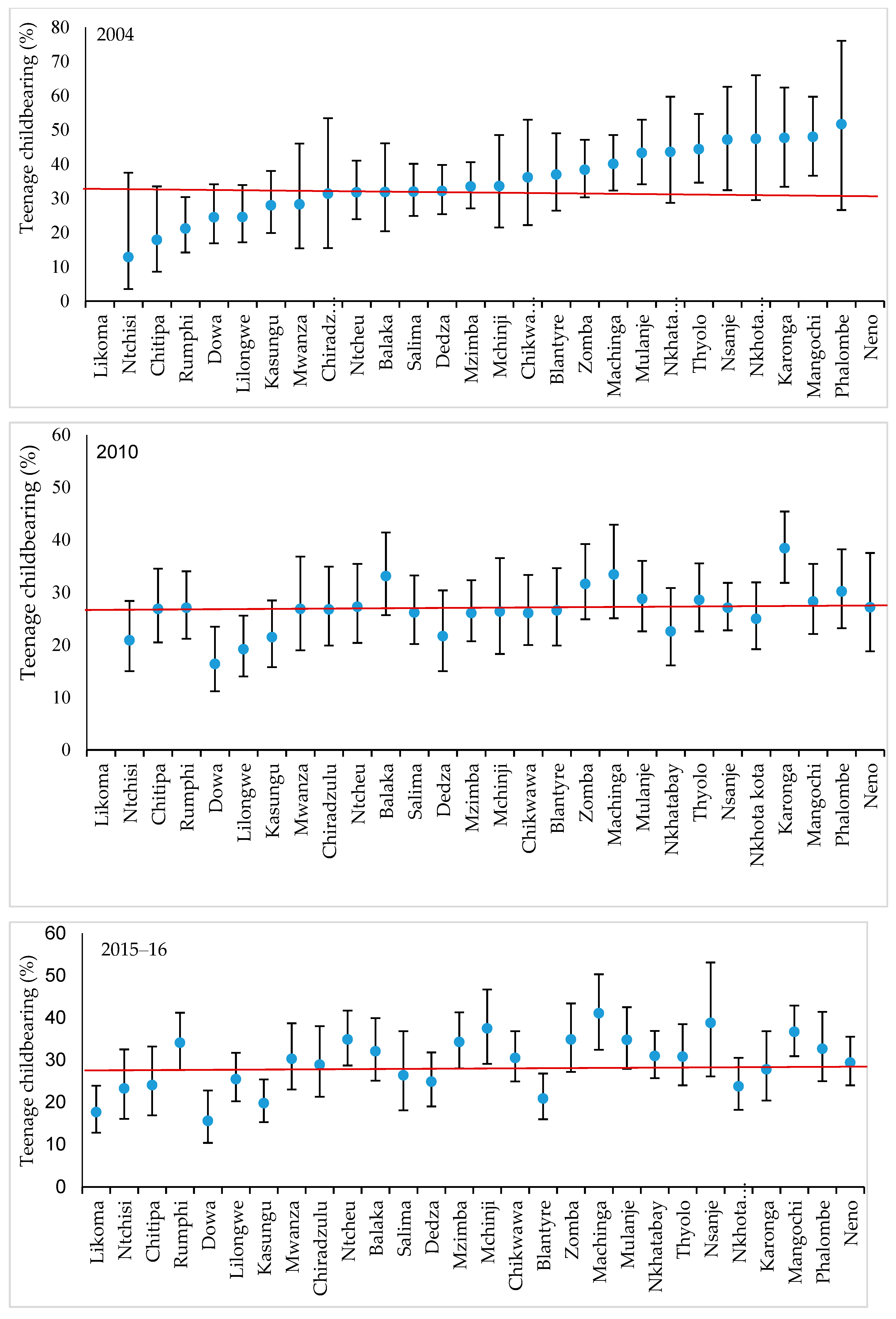
3.1. Descriptive Results
3.2. Multilevel Results
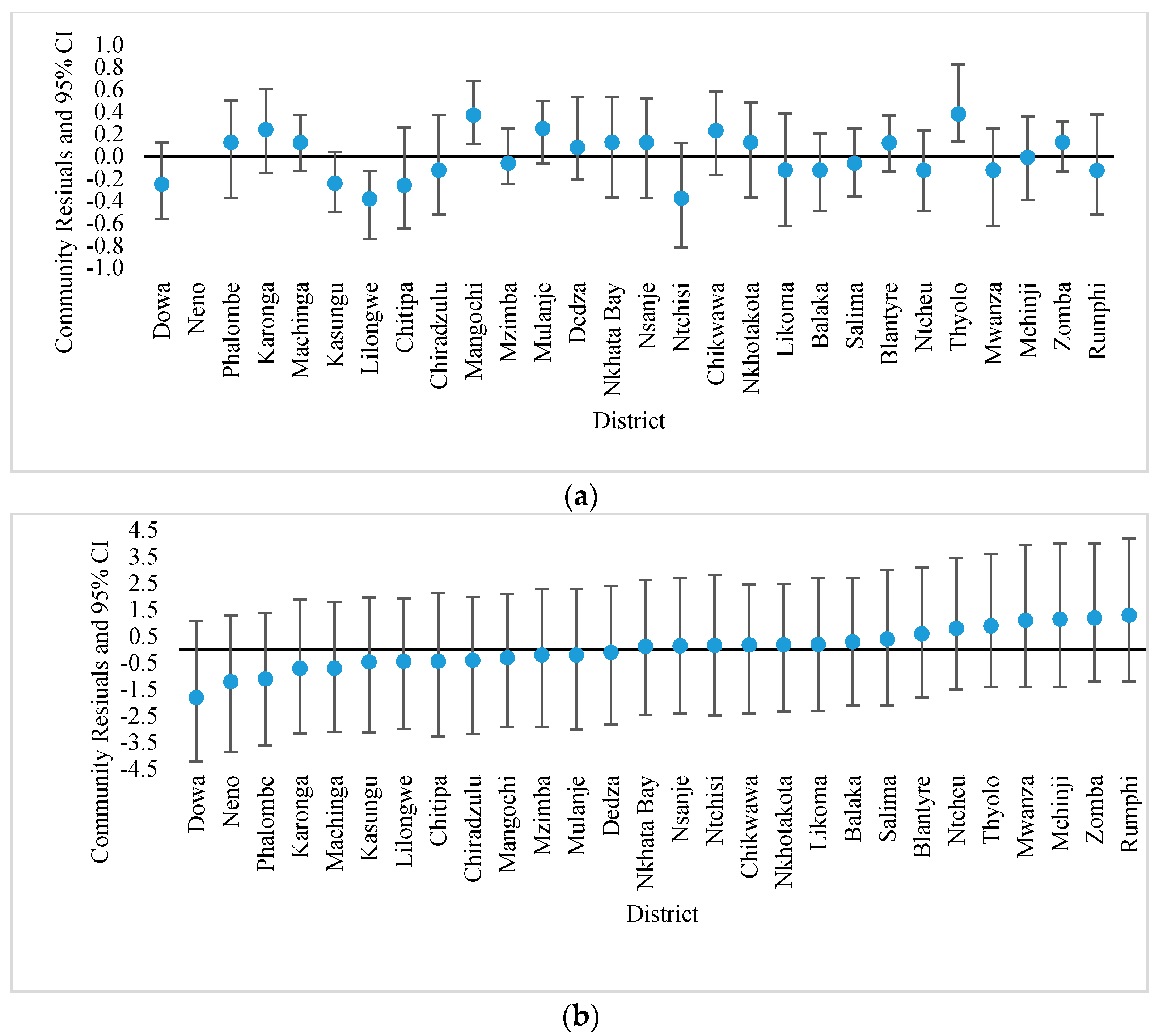
3.3. District Level Residuals
4. Discussion
4.1. Effect of Socioeconomic Factors (Education, Wealth and Residence) on Teenage Childbearing
4.2. Influence of Sociocultural Factors on Teenage Fertility
5. Conclusions
Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Acharya, Dev R., Rabi Bhattarai, Amudha Poobalan, Edwin R. van Teijlingen, and Glyn Chapman. 2010. Factors associated with teenage pregnancy in South Asia: A systematic review. European International Journal of Science and Technology 2: 3–14. [Google Scholar]
- Akella, Devi, and Melissa Jordan. 2015. Impact of social and cultural factors on teenage pregnancy. Journal of Health Disparities Research and Practice 8: 41–62. [Google Scholar]
- Arceo-Gómez, Eva O., and Raymundo M. Campos-Vazque. 2014. Teenage pregnancy in Mexico: Evolution and consequences. Latin American Journal of Economics 51: 109–46. [Google Scholar] [CrossRef] [Green Version]
- Ayele, Brhane G. K., Tesfay Gebrehiwot Gebregzabher, Tesfay Tekle Hailu, and Belete Abera Assefa. 2018. Determinants of teenage pregnancy in Degua Tembien District, Tigray, Northern Ethiopia: A community-based case-control study. PLoS ONE 13: e0200898. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, Joao P., Marta Favara, Sarah E. Haddock, Luis F. López-Calva, Miriam Muller, and Elizaveta Perova. 2012. Teenage Pregnancy and Opportunities in Latin America and the Caribbean: On Teenage Fertility Decisions, Poverty and Economic Achievement. Available online: http://documents.worldbank.org/curated/en/983641468238477531/Embarazoadolescente-resumen-2013 (accessed on 27 May 2020).
- Birhanu, B. E., D. L. Kebede, A. B. Kahsay, and A. B. Belachew. 2019. Predictors of teenage pregnancy in Ethiopia: A multilevel analysis. BMC Public Health 19: 601. [Google Scholar] [CrossRef] [Green Version]
- Bongaarts, John, and Robert G. Potter. 2013. Fertility, Biology, and Behavior: An Analysis of the Proximate Determinants. New York: Academic Press. [Google Scholar]
- Brown, Bradford B., Reed W. Larson, and Tharakad Subramanium Saraswathi. 2002. Experiences of the World’s Youth at the beginning of the 21st Century. In The World’s Youth: Adolescence in Eight Regions of the Globe. Edited by Bradford B. Brown and Reed W. Larson. Cambridge: Cambridge University Press, pp. 1–21. [Google Scholar]
- Chalasani, Satvika, Christine A. Kelly, Barbara S. Mensch, and Erica Soler-Hampejsek. 2012. Adolescent Pregnancy and Education Trajectories in Malawi. Pregnancy and Education. Available online: https://paa2013.princeton.edu/papers/132776 (accessed on 27 April 2020).
- Chandra-Mouli, Venkatraman, Catherine Lane, and Sylvia Wong. 2015. What does not work in adolescent sexual and reproductive health: A review of evidence on interventions commonly accepted as best practices. Global Health: Science and Practice 3: 333–40. [Google Scholar] [CrossRef] [Green Version]
- Chiavegatto Filho, Alexandre D. P., and Ichiro Kawachi. 2015. Income inequality is associated with adolescent fertility in Brazil: A longitudinal multilevel analysis of 5565 municipalities. BMC Public Health 15: 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chilinda, Chilinda, Idesi, Georgina Hourahane, Mercy Pindani, Caroline Chitsulo, and Alfred Maluwa. 2014. Attitude of health care providers towards adolescent sexual and reproductive health services in developing countries: A systematic review. Scientific Research 14: 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chirwa, Gowokani C., Jacob Mazalale, Gloria Likupe, Dominic Nkhoma, Levison Chiwaula, and Jesman Chintsanya. 2019. An evolution of socioeconomic related inequality in teenage pregnancy and childbearing in Malawi. PLoS ONE 14: e0225374. [Google Scholar] [CrossRef] [PubMed]
- Eloundou-Enyegue, Parfait M., and C. Shannon Stokes. 2004. Teen fertility and gender inequality in education: A contextual hypothesis. Demographic Research 11: 305–34. [Google Scholar] [CrossRef]
- Erulkar, Annabel S., Tekle-Ab Mekbib, Negussie Simie, and Tsehai Gulema. 2006. Differential use of adolescent reproductive health programs in Addis Ababa, Ethiopia. Journal of Adolescent Health 38: 253–60. [Google Scholar] [CrossRef]
- Family Planning 2020. 2019. Malawi Commitment Self-Reporting Questionnaire 2019. Available online: http://www.familyplanning2020.org/sites/default/files/Malawi_Questionnaire_Self-Report_2019_FINAL.pdf (accessed on 24 February 2021).
- Girma, S., and D. Paton. 2015. Is education the best contraception: The case of teenage pregnancy in England? Social Science and Medicine 131: 1–9. [Google Scholar] [CrossRef]
- Gunawardena, Nathali, Arone W. Fantaye, and Sanni Yaya. 2019. Predictors of pregnancy among young people in sub-Saharan Africa: A systematic review and narrative synthesis. BMJ Global Health 4: e001499. [Google Scholar] [CrossRef] [Green Version]
- Heaton, Tim. B. 2011. Does religion influence fertility in developing countries. Population Research and Policy Review 3: 449–65. [Google Scholar] [CrossRef]
- Hox, Joop J., Mirjam Moerbeek, and Rens Van de Schoot. 2018. Multilevel Analysis: Techniques and Applications, 3rd ed. New York: Routledge. [Google Scholar]
- Kassa, Getachew M., A. O. Arowojolu, A. A. Odukogbe, and Alemayehu W. Yalew. 2018. Prevalence and determinants of adolescent pregnancy in Africa: A systematic review and meta-analysis. Reproductive Health 15: 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, Elissa C., Siula Bulu, Jennifer Harris, David Humphreys, Jayline Malverus, and Natalie J. Gray. 2013. Be kind to young people so they feel at home: A qualitative study of adolescents and service providers’ perceptions of youth-friendly sexual and reproductive health services in Vanuatu. BMC Health Services Research 13: 455. [Google Scholar] [CrossRef] [Green Version]
- Likupe, Gloria, Jesman Chintsanya, Monica Magadi, Alister Munthali, and Medson Makwemba. 2020. Barriers to sexual and reproductive education among in-school adolescents in Zomba and Mangochi districts, Malawi. Sex Education 21: 450–62. [Google Scholar] [CrossRef]
- Magadi, Monica A. 2017. Multilevel determinants of teenage childbearing in sub-Saharan Africa in the context of HIV/AIDS. Health and Place 46: 37–48. [Google Scholar] [CrossRef] [PubMed]
- Magadi, Monica. 2006. Poor pregnancy outcomes among adolescents in South Nyanza Region of Kenya. African Journal of Reproductive Health 10: 26–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQueston, Kate, Rachel Silverman, and Amanda Glassman. 2012. Adolescent Fertility in Low- and Middle-Income Countries: Effects and Solutions. Washington, DC: Center for Global Development, p. 295. [Google Scholar]
- Meekers, Dominique, Ghyasuddin Ahmed, and M. T. Molatlhegi. 2001. Understanding constraints to adolescent condom procurement: The case of urban Botswana. Aids Care 13: 297–302. [Google Scholar] [CrossRef] [PubMed]
- Mensch, Barbara S., Susheela Singh, and John B. Casterline. 2005. Trends in the timing of first marriage among men and women in the developing world. In The Changing Transitions to Adulthood in Developing Countries: Selected Studies. Edited by Cynthia B. Lloyd, Jere R. Behrman, Nelly P. Stromquist and Barney Cohen. Washington, DC: The National Academies Press, pp. 118–71. [Google Scholar]
- Ministry of Education, Science and Technology (MoEST), and United Nations Children’s Emergency Fund (UNICEF). 2017. Girls’ Primary and Secondary Education in Malawi: Sector Review. Lilongwe: Malawi Government, Ministry of Education Science and Technology, Available online: https://research.acer.edu.au/cgi/viewcontent.cgi?article=1031&context=monitoring_learning (accessed on 24 April 2020).
- Morris, Jessica L., and Hamid Rushwan. 2015. Adolescent sexual and reproductive health: The global challenges. International Journal of Gynecology and Obstetrics 131: S40–S42. [Google Scholar] [CrossRef] [Green Version]
- Munthali, Alister, Eliya M. Zulu, Nyovani Madise, Ann M. Moore, Sidon Konyani, James Kaphuka, and Dixie Maluwa-Banda. 2006. Adolescent Sexual and Reproductive Health in Malawi: Results from the 2004 National Survey of Adolescents. New York: Alan Guttmacher Institute, Available online: https://www.guttmacher.org/sites/default/files/pdfs/pubs/2006/07/25/or24.pdf (accessed on 20 March 2020).
- National Statistical Office (NSO) [Malawi], and ICF. 2017. Malawi Demographic and Health Survey 2015–16. Zomba and Rockville: NSO and ICF. [Google Scholar]
- Neal, Sarah, Zoë Matthews, Melanie Frost, Helga Fogstad, Alma V. Camacho, and Laura Lask. 2012. Childbearing in adolescents aged 12–15 years in low resource countries: A neglected issue. New estimates from demographic and household surveys in 42 countries. Acta Obstetricia et Gynecologica Scandinavica 91: 1114–18. [Google Scholar] [CrossRef] [PubMed]
- Ngome, Enock, and Clifford Odimegwu. 2014. The social context of adolescent women’s use of modern contraceptives in Zimbabwe: A multilevel analysis. Reproductive Health 11: 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obasohan, Phillips E. 2015. Religion, Ethnicity and Contraceptive Use among Reproductive age Women in Nigeria. International Journal of MCH and AIDS 3: 63–73. [Google Scholar] [CrossRef] [PubMed]
- Palamuleni, Martin. E. 2017. Determinants of adolescent fertility in Malawi. Gender and Behaviour 15: 10126–41. Available online: https://hdl.handle.net/10520/EJC-c1e75d3b4 (accessed on 28 December 2020).
- Pot, Hanneke. 2019. INGO Behavior Change Projects: Culturalism and Teenage Pregnancies in Malawi. Medical Anthropology 38: 327–41. [Google Scholar] [CrossRef] [Green Version]
- Poudel, Samikshya, Nawaraj Upadhaya, Resham Bahadur Khatri, and Pramesh Raj Ghimire. 2018. Trends and factors associated with pregnancies among adolescent women in Nepal: Pooled analysis of Nepal Demographic and Health Surveys (2006, 2011 and 2016). PLoS ONE 13: e0202107. [Google Scholar] [CrossRef] [Green Version]
- Rabe-Hesketh, S., and A. Skrondal. 2012. Multilevel and Longitudinal Modelling Using Stata, 3rd ed. College Station: STATA Press, vol. 2. [Google Scholar]
- Rosenberg, Nora E., Nivedita L. Bhushan, Dhrutika Vansia, Twambilile Phanga, Bertha Maseko, Tiyamike Nthani, Colleta Libale, Catherine Bamuya, Linda Kamtsendero, Annie Kachigamba, and et al. 2018. Comparing Youth Friendly Health Services to the Standard of Care through “Girl Power-Malawi”: A Quasi-Experimental Cohort Study. Journal of Acquired Immune Deficiency Syndromes 79: 458–66. [Google Scholar] [CrossRef]
- Rutstein, Shea, and Guillermo Rojas. 2006. Guide to Demographic and Health Survey (DHS). Calverton: ORC Macro, Available online: https://dhsprogram.com/pubs/pdf/DHSG1/Guide_to_DHS_Statistics_DHS-7.pdf (accessed on 14 July 2020).
- Self, Andrew, Samuel Chipokosa, Amos Misomali, Tricia Aung, Steven A. Harvey, Mercy Chimchere, James Chilembwe Fannie Kachale, Jameson Ndawala, and Melissa A. Marx. 2018. Youth accessing reproductive health services in Malawi: Drivers, barriers, and suggestions from the perspectives of youth and parents. Reproductive Health 15: 108. [Google Scholar] [CrossRef]
- Strayhorn, Joseph M., and Jillian C. Strayhorn. 2009. Religiosity and teen birth rate in the United States. Reproductive Health 6: 1–7. [Google Scholar] [CrossRef] [Green Version]
- Sully, Elizabeth, Ann Biddlecom, Jacqueline E. Darroch, Taylor Riley, Lori S. Ashford, Naomi Lince-Deroche, Lauren Firestein, and Rachel Murro. 2019. Adding It Up: Investing in Sexual and Reproductive Health 2019; New York: Guttmacher Institute. Available online: https://www.guttmacher.org/report/adding-it-upinvesting-in-sexual-reproductive-health-2019 (accessed on 20 February 2021).
- Sustainable Development Goals (SDGs) Indicators, Global Database. n.d. Available online: https://unstats.un.org/sdgs/indicators/database/ (accessed on 24 April 2020).
- Temmerman, Marleen. 2017. Adolescent mothers: Too young to be neglected. The Lancet Child and Adolescent Health 1: 164–66. [Google Scholar] [CrossRef]
- Twisk, Jos W. 2006. Applied Multilevel Analysis: A Practical Guide for Medical Researchers. Cambridge: Cambridge University Press. [Google Scholar]
- United Nations Department of Economic and Social Affairs (UNDESA) Population Division. 2017. World Population Prospects: The 2017 Revision, DVD ed. New York: UNDESA, Population Division, Available online: https://www.un.org/development/desa/publications/world-population-prospects-the-2017-revision.html (accessed on 28 May 2020).
- United Nations Population Fund (UNFPA). 2013. Motherhood in Childhood: Facing the Challenge of Adolescent Pregnancy. New York: UNFPA, Available online: https://www.unfpa.org/sites/default/files/pub-pdf/EN-SWOP2013.pdf (accessed on 20 March 2020).
- Wado, Yohannes D., Elizabeth A. Sully, and Joyce N. Mumah. 2019. Pregnancy and early motherhood among adolescents in five East African countries: A multi-level analysis of risk and protective factors. BMC Pregnancy and Childbirth 19: 59. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO). 2016. Global Health Estimates 2015: Deaths by Cause, Age, Sex, by Country and by Region, 2000–15. Geneva: WHO, Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates (accessed on 14 January 2020).
- World Health Organisation (WHO). 2020. Adolescent Pregnancy. Geneva: World Health Organization, Available online: https://www.who.int/en/news-room/fact-sheets/detail/adolescent-pregnancy (accessed on 12 January 2021).
- Yeatman, Sara E., and Jenny Trinitapoli. 2008. Beyond Denomination: The Relationship between Religion and Family Planning in Rural Malawi. Demographic Research 19: 1851–82. [Google Scholar] [CrossRef] [PubMed]
- Youth Friendly Health Service (YFHS) Evaluation Study. 2014. Evaluation of Youth—Friendly Health Services in Malawi. Available online: https://www.e2aproject.org/wp-content/uploads/evaluation-yfhs-malawi.pdf (accessed on 27 October 2019).



{kind=link}
{kind=link}
| Explanatory Variable | Description and Coding of the Variable |
|---|---|
| Demographic | |
| Age of a respondent | Categorised into (1) 15, (2) 16, (3) 17, (4) 18 and (5) 19. |
| Early sexual debut a | Coded as 1 if adolescent engaged in sexual intercourse before the age of 15 completed years, 0 if otherwise |
| Marital status b | Coded (1) never married and (2) ever married. |
| Sociocultural and economic variables | |
| Education | The highest educational level attained by an individual: (0) no education, (1) primary—1–4, (2) primary—5–8, (3) secondary and higher. |
| Ever used modern contraceptives | Adolescents were categorised into (1) if they ever used modern contraceptives or (0) if otherwise. |
| Religion | Religion was grouped into (1) Catholic, (2) Presbyterians, (3) Pentecost, (4) Muslim and (5) other. |
| Ethnicity | Ethnicity in Malawi has five major stratifications grouped as (1) Chewa, (2) Ngoni, (3) Yao, (4) Lomwe and (5) other |
| Wealth Index c | Obtained using principal component analysis (PCA) following the standard methodology and divided into five equal groups of 20% of household quintiles (poorest, poorer, medium, richer and richest) at the national level |
| Source of family planning message | Coded from whether or not an individual had heard family planning messages on the radio, on television or read family planning messages in the newspaper or watched. A “yes” response was coded (1) and (0), if otherwise. |
| Occupation | Recoded as (1) currently employed or (0) not currently working |
| Contextual factors | |
| Place of residence | Place of residence was categorised into (1) urban and (2) rural. |
| District | (1) Chitipa, (2) Karonga, (3) Nkhatabay, (4) Rumphi (5) Mzimba, (6) Likoma, (7) Kasungu (8) Nkhotakota, (9) Ntchisi, (10) Dowa, (11) Salima, (12) Lilongwe, (13) Mchinji (14) Dedza (15) Ntcheu, (16) Mangochi, (17) Machinga, (18). Zomba (19) Chiradzulu, (20) Blantyre, (21) Mwanza (22) Thyolo, (23) Mulanje, (24) Phalombe, (25) Chikwawa, (26) Nsanje, (27) Balaka and (28) Neno |
| Background Characteristics | Malawi Demographic and Health Surveys (MDHS) | |||||
|---|---|---|---|---|---|---|
| 2004 MDHS | 2010 MDHS | 2015–16 MDHS | ||||
| Percent | n | Percent | n | Percent | n | |
| Age (years) | ||||||
| 15 | 18.6 | 451 | 24.7 | 1246 | 23.8 | 1258 |
| 16 | 19.5 | 474 | 23.0 | 1171 | 17.9 | 971 |
| 17 | 17.8 | 420 | 18.5 | 944 | 18.4 | 941 |
| 18 | 23.2 | 578 | 18.1 | 883 | 20.4 | 1085 |
| 19 | 20.9 | 484 | 15.7 | 796 | 19.6 | 1018 |
| Sexual debut | ||||||
| Median (years) a | 16.6 | 16.4 | 16.4 | |||
| Early sex debut | 28.4 | 684 | 23.0 | 1159 | 22.7 | 1197 |
| Marital status | ||||||
| Proportion ever married | 36.3 | 903 | 26.2 | 1318 | 26.8 | 1364 |
| Highest education | ||||||
| No education | 5.5 | 134 | 3.3 | 140 | 2.7 | 126 |
| Primary 1–4 | 24.2 | 611 | 21.2 | 998 | 17.3 | 816 |
| Primary 5–8 | 52.1 | 1244 | 53.9 | 2843 | 58.2 | 3101 |
| Secondary and higher | 18.2 | 418 | 21.6 | 1059 | 21.7 | 1230 |
| Ever employment | 37.1 | 930 | 36.6 | 1932 | 40.0 | 1291 |
| Wealth index | ||||||
| Poorest | 16.5 | 423 | 17.8 | 957 | 18.3 | 863 |
| Poorer | 17.2 | 411 | 17.8 | 918 | 19.1 | 950 |
| Middle | 18.6 | 457 | 19.7 | 1004 | 19.9 | 979 |
| Richer | 21.4 | 537 | 19.7 | 1079 | 19.3 | 1071 |
| Richest | 26.3 | 579 | 25.1 | 1082 | 23.4 | 1410 |
| None | 39.5 | 920 | 47.6 | 2321 | 64.25 | 3300 |
| Radio | 42.3 | 1050 | 31.3 | 1685 | 21.22 | 1163 |
| Television | 2.7 | 64 | 4.2 | 196 | 5.33 | 290 |
| Newspaper | 15.5 | 373 | 16.9 | 838 | 9.2 | 520 |
| Modern contraceptives use | 7.6 | 185 | 9.0 | 461 | 15.2 | 802 |
| Ethnicity | ||||||
| Chewa | 34.2 | 757 | 34.8 | 1502 | 36.0 | 1646 |
| Tumbuka | 15.6 | 385 | 12.8 | 838 | 12.4 | 841 |
| Ngoni | 26.2 | 645 | 28.9 | 1490 | 30.8 | 1624 |
| Yao | 12.7 | 368 | 12.6 | 503 | 12.9 | 588 |
| Other | 11.3 | 252 | 10.8 | 707 | 7.9 | 574 |
| Religion | ||||||
| Catholic | 28.6 | 662 | 25.6 | 1323 | 23.1 | 1321 |
| Presbyterian | 20.8 | 484 | 20.3 | 965 | 18.2 | 859 |
| Pentecost | 39.8 | 924 | 42.0 | 2245 | 46.6 | 2522 |
| Muslim | 10.7 | 337 | 12.1 | 507 | 12.1 | 571 |
| Living in rural | 81.0 | 2028 | 81.1 | 4358 | 82.6 | 4151 |
| Background Characteristics | 2004 MDHS | 2010 MDHS | 2015–16 MDHS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Percent (C.I.) | n | X2 | Percent (C.I.) | n | X2 | Percent (C.I.) | n | X2 | |
| Age (years) | 617 | 1175 | 1097 | ||||||
| 15 | 3.20 (1.80–5.60) | 451 | 3.50 (2.60–4.90) | 1246 | 4.50 (3.30–6.20) | 1258 | |||
| 16 | 11.5 (8.80–15.0) | 474 | 12.6 (10.5–15.0) | 1171 | 12.2 (9.90–14.9) | 971 | |||
| 17 | 30.7 (26.0–36.0) | 420 | 21.7 (18.4–25.4) | 944 | 26.6 (23.2–30.2) | 941 | |||
| 18 | 49.9 (44.8–55.0) | 578 | 43.4 (39.0–47.9) | 883 | 45.6 (42.0–49.2) | 1085 | |||
| 19 | 67.9 (62.7–72.8) | 484 | 63.5 (59.0–67.7) | 796 | 59.2 (55.5–62.7) | 1018 | |||
| Sexual debut | 647 | 1246 | 740 | ||||||
| Under 15 | 72.1 (68.0–75.9) | 706 | 65.3 (61.7–68.8) | 1168 | 58.0 (54.7–61.2) | 1303 | |||
| 15 and over | 18.2 (15.8–20.8) | 1701 | 13.7 (12.4–15.2) | 3872 | 19.0 (17.5–20.6) | 3970 | |||
| Marital status | 1444 | 3077 | 2863 | ||||||
| Never married | 6.40 (5.00–8.20) | 1504 | 5.30 (4.50–6.30) | 3722 | 9.00 (7.80–10.3) | 3909 | |||
| Ever married | 82.7 (79.7–85.4) | 903 | 82.8 (80.0–85.3) | 1318 | 83.8 (81.1–86.1) | 1364 | |||
| Highest education | 111 | 122 | 2809 | ||||||
| No education | 63.1 (53.7–71.7) | 134 | 44.1 (34.8–53.9) | 140 | 53.0 (43.3–62.4) | 126 | |||
| Primary 1–4 | 41.8 (37.1–46.8) | 611 | 33.5 (29.7–37.4) | 998 | 35.3 (31.7–39.0) | 816 | |||
| Primary 5–8 | 32.6 (29.2–36.2) | 1244 | 25.4 (23.4–27.4) | 2843 | 29.8 (27.7–32.1) | 3101 | |||
| Secondary and higher | 19.0 (14.8–24.2) | 418 | 15.6 (12.4–19.6) | 1059 | 18.9 (16.0–22.3) | 1230 | |||
| Employment status | 88 | 22 | 115 | ||||||
| Unemployed | 27.1 (24.2–30.3) | 1475 | 23.4 (21.4–25.5) | 3097 | 23.5 (21.8–25.4) | 3352 | |||
| Employed | 45.9 (41.9–50.0) | 930 | 29.4 (26.9–32.1) | 1932 | 37.3 (34.4–40.2) | 1921 | |||
| Wealth index | 100 | 107 | 116 | ||||||
| Poorest | 43.2 (37.8–48.8) | 423 | 31.1 (27.2–35.2) | 957 | 43.6 (39.5–47.8) | 863 | |||
| Poorer | 46.9 (41.0–52.8) | 411 | 31.1 (27.3–35.2) | 918 | 34.8 (30.9–38.8) | 950 | |||
| Middle | 35.8 (30.7–41.3) | 457 | 30.2 (26.7–33.9) | 1004 | 30.5 (27.0–34.2) | 979 | |||
| Richer | 32.0 (27.2–37.2) | 537 | 23.8 (20.4–27.5) | 1079 | 24.7 (21.6–28.1) | 1071 | |||
| Richest | 20.4 (16.1–25.3) | 579 | 15.6 (12.7–19.1) | 1082 | 15.3 (12.8–18.3) | 1410 | |||
| Source of family planning message | 41 | 64 | 239 | ||||||
| None | 33.2 (29.2–37.4) | 920 | 23.6 (21.5–26.0) | 2321 | 30.0 (28.1–32.0) | 3300 | |||
| Radio | 39.9 (36.3–43.5) | 1050 | 32.4 (29.6–35.4) | 1685 | 32.2 (28.6–35.9) | 1163 | |||
| Television | 21.0 (11.4–35.4) | 64 | 23.9 (16.6–33.2) | 196 | 17.8 (12.4–25.0) | 290 | |||
| Newspaper | 22.9 (17.8–28.9) | 373 | 18.9 (15.6–22.7) | 838 | 21.5 (17.1–26.7) | 520 | |||
| Ever used modern contraceptives | 190 | 747 | 37 | ||||||
| No | 30.2 (27.8–32.8) | 2222 | 20.3 (18.8–21.9) | 4579 | 20.7 (19.2–22.3) | 4471 | |||
| Yes | 80.4 (73.3–86.0) | 185 | 79.0 (73.5–83.5) | 461 | 75.6 (71.2–79.5) | 802 | |||
| Ethnicity | 23 | 33.6 | 993 | ||||||
| Chewa | 29.7 (25.6–34.1) | 757 | 21.2 (18.6–24.1) | 1502 | 25.4 (22.5–28.5) | 1646 | |||
| Tumbuka | 33.5 (28.2–39.2) | 385 | 25.7 (22.4–29.2) | 838 | 27.5 (23.7–31.7) | 841 | |||
| Ngoni | 35.0 (31.0–39.3) | 645 | 27.4 (24.7–30.2) | 1490 | 30.9 (28.1–33.9) | 1624 | |||
| Yao | 44.7 (38.5–51.0) | 368 | 31.4 (27.0–36.1) | 503 | 34.7 (30.8–38.9) | 588 | |||
| Other | 33.9 (26.8–41.8) | 252 | 28.3 (23.8–33.4) | 707 | 31.0 (26.9–35.5) | 574 | |||
| Religion | 73 | 63 | 27 | ||||||
| Catholic | 31.6 (27.1–36.4) | 662 | 22.4 (19.5–25.5) | 1323 | 25.5 (22.6–28.6) | 1321 | |||
| Presbyterian | 21.6 (17.5–26.2) | 484 | 18.3 (15.5–21.4) | 965 | 23.5 (19.7–27.8) | 859 | |||
| Pentecost | 27.1 (19.1–36.8) | 924 | 21.4 (16.5–27.2) | 2245 | 22.7 (17.7–28.7) | 2522 | |||
| Muslim | 42.3 (38.6–46.0) | 337 | 31.1 (28.8–33.6) | 507 | 33.5 (31.3–35.7) | 571 | |||
| Residence | 22 | 16 | 51 | ||||||
| Urban | 24.8 (18.7–32.1) | 379 | 20.5 (16.0–25.9) | 682 | 21.3 (17.7–25.3) | 1122 | |||
| Rural | 36.2 (33.6–39.0) | 2028 | 26.8 (25.2–28.5) | 4358 | 30.7 (28.9–32.5) | 4151 | |||
| Total | 36.1 (31.5–36.7) | 2407 | 25.6 (24.0–27.3) | 5040 | 29.0 (27.4–30.7) | 5273 | |||
| 2004 MDHS | 2010 MDHS | 2015–16 MDHS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Model 2 | Model 3 | Model 4 | Model 2 | Model 3 | Model 4 | Model 2 | Model 3 | Model 4 | |
| Age (Ref: 15) | |||||||||
| 16 | 2.28 * | 2.38 * | 2.44 *** | 2.41 *** | 1.90 ** | 2.00 *** | |||
| (1.17–4.43) | (1.20–4.70) | (1.62–3.69) | (1.60–3.65) | (1.29–2.80) | (1.35–2.98) | ||||
| 17 | 3.97 *** | 4.14 *** | 2.89 *** | 3.01 *** | 4.20 *** | 4.36 *** | |||
| (2.08–7.57) | (2.13–8.07) | (1.90–4.39) | (1.97–4.59) | (2.92–6.03) | (2.98–6.37) | ||||
| 18 | 5.63 *** | 6.00 *** | 5.08 *** | 5.38 *** | 5.21 *** | 5.56 *** | |||
| (2.99–10.6) | (3.12–11.5) | (3.37–7.65) | (3.53–8.19) | (3.63–7.47) | (3.81–8.13) | ||||
| 19 | 11.6 *** | 12.33 *** | 9.02 *** | 9.43 *** | 6.97 *** | 7.56 *** | |||
| (6.11–22.1) | (6.31–24.1) | (5.9–13.7) | (6.08–14.63) | (4.82–10.1) | (5.09–11.2) | ||||
| Early sex debut (Ref: under 15) | |||||||||
| 15 and over | 0.51 *** | 0.49 *** | 0.57 *** | 0.58 *** | 0.81 | 0.79 * | |||
| (0.37–0.68) | (0.36–0.67) | (0.44–0.72) | (0.45–0.75) | (0.66–1.00) | (0.63–0.98) | ||||
| Marital status (Ref: Never married) | |||||||||
| Ever married | 35.2 *** | 28.9 *** | 52.6 *** | 39.2 *** | 37.5 *** | 26.3 *** | |||
| (26.2–47.3) | (20.9–40.1) | (41.6–66.5) | (30.3–50.7) | (30.6–45.9) | (21.0–32.9) | ||||
| Education (Ref: No education) | |||||||||
| Primary 1–4 | 0.56 ** | 1.07 | 0.84 | 1.68 | 0.47 *** | 0.99 | |||
| (0.37–0.84) | (0.59–1.93) | (0.56–1.26) | (0.91–3.11) | (0.31–0.72) | (0.54–1.83) | ||||
| Primary 5–8 | 0.42 *** | 1.18 | 0.50 *** | 1.30 | 0.40 *** | 0.84 | |||
| (0.28–0.63) | (0.65–2.12) | (0.34–0.74) | (0.72–2.37) | (0.27–0.60) | (0.47–1.51) | ||||
| Secondary and higher | 0.31 *** | 0.75 | 0.30 *** | 0.72 | 0.27 *** | 0.44 * | |||
| (0.19–0.51) | (0.37–1.53) | (0.19–0.47) | (0.37–1.42) | (0.17–0.43) | (0.23–0.83) | ||||
| Employment status (Ref: Not employed) | |||||||||
| Employed | 1.88 *** | 1.15 | 1.19 * | 0.87 | 1.56 *** | 0.99 | |||
| (1.54–2.29) | (0.85–1.56) | (1.03–1.39) | (0.69–1.09) | (1.35–1.81) | (0.81–1.22) | ||||
| Wealth index (Ref: Poorest) | |||||||||
| Poorer | 1.37 * | 1.07 | 0.91 | 0.69 * | 0.70 ** | 0.64 ** | |||
| (1.02–1.84) | (0.68–1.70) | (0.73–1.14) | (0.49–0.98) | (0.56–0.87) | (0.47–0.89) | ||||
| Middle | 0.89 | 1.00 | 0.92 | 0.79 | 0.53 *** | 0.79 | |||
| (0.66–1.20) | (0.63–1.59) | (0.74–1.14) | (0.56–1.12) | (0.42–0.66) | (0.57–1.08) | ||||
| Richer | 0.69 * | 0.75 | 0.67 *** | 0.56 ** | 0.45 *** | 0.78 | |||
| (0.51–0.93) | (0.48–1.19) | (0.54–0.84) | (0.39–0.80) | (0.36–0.57) | (0.56–1.08) | ||||
| Richest | 0.44 *** | 0.89 | 0.44 *** | 0.62 * | 0.24 *** | 0.40 *** | |||
| (0.30–0.63) | (0.50–1.58) | (0.33–0.58) | (0.41–0.95) | (0.18–0.32) | (0.28–0.60) | ||||
| Source of family planning message (Ref: none) | |||||||||
| Radio | 1.59 *** | 1.04 | 1.79 *** | 1.36 * | 1.46 *** | 1.06 | |||
| (1.29–1.97) | (0.75–1.43) | (1.52–2.10) | (1.06–1.75) | (1.23–1.74) | (0.83–1.34) | ||||
| Television | 1.39 | 1.00 | 1.30 | 1.00 | 0.92 | 0.95 | |||
| (0.71–2.69) | (0.39–2.53) | (0.86–1.95) | (0.55–1.82) | (0.63–1.34) | (0.58–1.54) | ||||
| Newspaper | 1.00 | 0.95 | 1.14 | 0.94 | 0.85 | 0.84 | |||
| (0.73–1.38) | (0.60–1.52) | (0.90–1.44) | (0.66–1.34) | (0.64–1.11) | (0.59–1.19) | ||||
| Modern contraceptives | |||||||||
| Yes | 11.12 *** | 5.51 *** | 19.01 *** | 7.08 *** | 13.53 *** | 6.35 *** | |||
| (7.41–16.7) | (3.19–9.51) | (14.6–24.69) | (4.83–10.4) | (11.2–16.4) | (4.92–8.20) | ||||
| Ethnicity (Ref Chewa) | |||||||||
| Tumbuka | 1.18 | 1.29 | 1.91 *** | 1.34 | 1.56 ** | 1.32 | |||
| (0.82–1.71) | (0.74–2.23) | (1.47–2.49) | (0.87–2.07) | (1.17–2.07) | (0.94–1.86) | ||||
| Ngoni | 1.10 | 1.02 | 1.61 *** | 1.74 ** | 1.36 ** | 1.87 *** | |||
| (0.81–1.51) | (0.64–1.64) | (1.31–1.98) | (1.22–2.47) | (1.11–1.67) | (1.43–2.46) | ||||
| Yao | 0.88 | 1.16 | 1.13 | 0.78 | 1.08 | 1.37 | |||
| (0.57–1.35) | (0.61–2.20) | (0.78–1.64) | (0.44–1.41) | (0.77–1.50) | (0.90–2.10) | ||||
| other | 0.99 | 1.09 | 1.35 * | 1.19 | 1.70 *** | 1.97 *** | |||
| (0.67–1.46) | (0.62–1.94) | (1.04–1.77) | (0.76–1.86) | (1.29–2.25) | (1.37–2.83) | ||||
| Religion (Ref: Catholic) | |||||||||
| Presbyterian | 0.73 * | 1.02 | 0.87 | 0.87 | 1.12 | 1.12 | |||
| (0.55–0.99) | (0.66–1.58) | (0.69–1.10) | (0.61–1.24) | (0.88–1.43) | (0.81–1.53) | ||||
| Pentecost | 1.19 | 1.16 | 1.19 | 1.03 | 1.18 | 0.94 | |||
| (0.94–1.50) | (0.81–1.67) | (1.00–1.43) | (0.78–1.36) | (0.99–1.42) | (0.74–1.21) | ||||
| Muslim | 1.66 * | 1.18 | 1.56 * | 1.35 | 1.98 *** | 1.70 * | |||
| (1.07–2.56) | (0.61–2.26) | (1.09–2.24) | (0.77–2.37) | (1.41–2.79) | (1.09–2.65) | ||||
| Residence (Ref: Urban) | |||||||||
| Rural | 0.75 | 1.17 | 0.94 | 0.90 | 0.72 ** | 0.63 ** | |||
| (0.53–1.06) | (0.71–1.92) | (0.72–1.23) | (0.61–1.33) | (0.57–0.91) | (0.46–0.85) | ||||
| N | 2407 | 2405 | 2405 | 5040 | 5029 | 5029 | 5273 | 5273 | 5273 |
| Model 1 (Null) | Model 2 | Model 3 | Model 4 | |
|---|---|---|---|---|
| Estimate (S.E.) | Estimate (S.E.) | Estimate (S.E.) | Estimate (S.E.) | |
| Constant (OR) | ||||
| 2004 | 0.52 *** (0.04) | 0.03 *** (0.01) | 0.83 (0.25) | 0.02 *** (0.01) |
| 2010 | 0.35 *** (0.02) | 0.31 *** (0.01) | 0.32 *** (0.08) | 0.08 (0.04) |
| 2015 | 0.39 *** (0.02) | 0.19 (0.03) | 0.81 (0.21) | 0.05 *** (0.02) |
| District Level Variance | ||||
| 2004 | 0.08 (0.04) | 0.16 (0.09) | 0.08 (0.05) | 0.16 (0.10) |
| 2010 | 0.04 (0.02) | 0.14 (0.06) | 0.02 (0.02) | 0.08 (0.05) |
| 2015 | 0.06 (0.02) | 0.02 (0.03) | 0.03 (0.02) | 0.02 (0.03) |
| Inter Cluster Correlation (ICC%) | ||||
| 2004 | 2.42 | 4.71 | 2.34 | 4.63 |
| 2010 | 1.13 | 4.13 | 4.82 | 2.36 |
| 2015 | 1.76 | 0.70 | 0.8 | 0.66 |
| Median Odds Ratio (MOR) | ||||
| 2004 | 1.31 | 1.47 | 1.31 | 1.47 |
| 2010 | 1.20 | 1.43 | 1.12 | 1.31 |
| 2015 | 1.26 | 1.16 | 1.16 | 1.15 |
| DIC (−2Log Likelihood) | ||||
| 2004 | −1550.6 | −718.4 | −1345.2 | −688.6 |
| 2010 | −2888.0 | −1261.9 | −2391.1 | −948.0 |
| 2015 | −3128.8 | −1270.7 | −2464.0 | −1456.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chintsanya, J.; Magadi, M.; Likupe, G. A Multilevel Analysis of Risk and Protective Factors for Adolescent Childbearing in Malawi. Soc. Sci. 2021, 10, 303. https://doi.org/10.3390/socsci10080303
Chintsanya J, Magadi M, Likupe G. A Multilevel Analysis of Risk and Protective Factors for Adolescent Childbearing in Malawi. Social Sciences. 2021; 10(8):303. https://doi.org/10.3390/socsci10080303
Chicago/Turabian StyleChintsanya, Jesman, Monica Magadi, and Gloria Likupe. 2021. "A Multilevel Analysis of Risk and Protective Factors for Adolescent Childbearing in Malawi" Social Sciences 10, no. 8: 303. https://doi.org/10.3390/socsci10080303
APA StyleChintsanya, J., Magadi, M., & Likupe, G. (2021). A Multilevel Analysis of Risk and Protective Factors for Adolescent Childbearing in Malawi. Social Sciences, 10(8), 303. https://doi.org/10.3390/socsci10080303