
Social Determinants of Health and Vascular Diseases: A Systematic Review and Call for Action

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
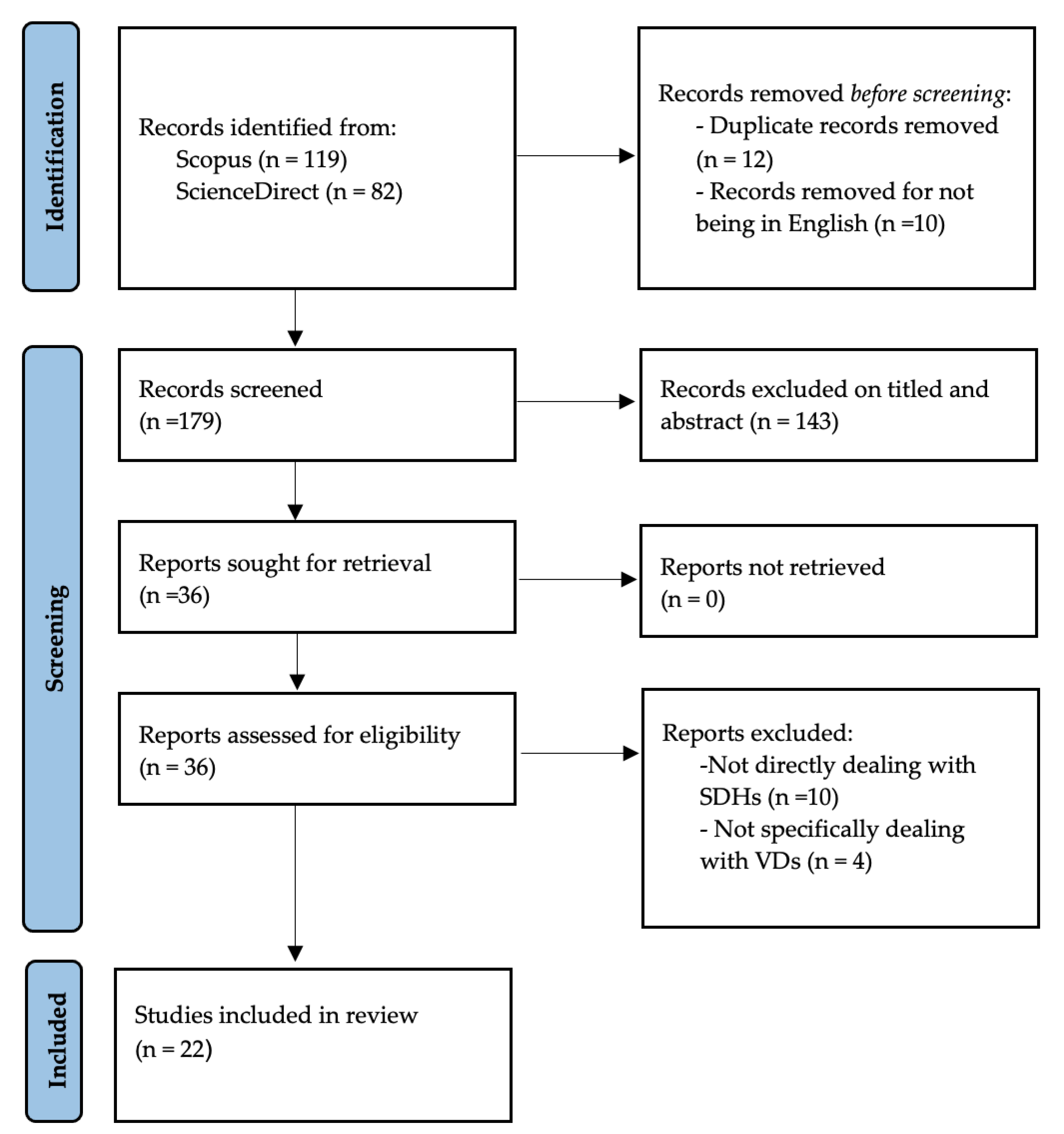
2.3. Study Selection
2.4. Data Extraction
3. Results
3.1. Selected Studies
3.2. Temporal Extension
3.3. Journal List
3.4. Articles and Types of Vascular Disease
3.5. General Characteristics of the Included Studies
3.6. Abdominal Arterial Aneurysm and Social Determinants of Health
3.6.1. Abdominal Arterial Aneurysm and Ethnicity
3.6.2. Abdominal Arterial Aneurysm and Gender
3.6.3. Abdominal Arterial Aneurysm and SES
3.7. Carotid Stenosis and the Social Determinants of Health
3.7.1. Carotid Stenosis and Ethnicity
3.7.2. Carotid Stenosis and SES
3.8. Peripheral Artery Disease and Social Determinants of Health
3.8.1. Peripheral Artery Disease and Ethnicity
3.8.2. Peripheral Artery Disease and SES
3.8.3. Peripheral Artery Disease and Gender
3.9. Chronic Venous Disease and the Social Determinants of Health
3.9.1. Chronic Venous Disease and SES
3.9.2. Chronic Venous Disease and Ethnicity
3.9.3. Chronic Venous Disease and Gender
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ballard, Jeffrey L., and John Bergan. 2000. Chronic Venous Insufficiency: Diagnosis and Treatment. Berlin/Heidelberg: Springer Science & Business Media. [Google Scholar]
- Barnes, Robert W. 1995. Vascular holism: The epidemiology of vascular disease. Annals of Vascular Surgery 9: 576–82. [Google Scholar] [CrossRef]
- Barshes, Neal, and Samantha Minc. 2021. Healthcare disparities in vascular surgery: A critical review. Journal of Vascular Surgery 74: 6S–14S. [Google Scholar] [CrossRef] [PubMed]
- Berkman, Lisa, Ichirō Kawachi, and Maria Glymour, eds. 2014. Social Epidemiology. New York: Oxford University Press. [Google Scholar]
- Blais, Claudia, Louis Rochette, Suzie Ouellet, and Thao Huynh. 2020. Complex Evolution of Epidemiology of Vascular Diseases, Including Increased Disease Burden: From 2000 to 2015. Canadian Journal of Cardiology 36: 740–46. [Google Scholar] [CrossRef]
- Brathwaite, Shayna, Lauren West-Livingston, D’Andre Williams, Channa Blakely, Jayne Rice, and Olamide Alabi. 2021. Moving forward: Recommendations to overcome existing structural racism. Journal of Vascular Surgery 74: 47S–55S. [Google Scholar] [CrossRef] [PubMed]
- Braveman, Paula. 2023. Social Determinants of Health and Health Disparities. New York: Oxford University Press. [Google Scholar]
- Brunner, Eric, Michael Shipley, David Blane, George Davey Smith, and Michael G. Marmot. 1999. When does cardiovascular risk start? Past and present socioeconomic circumstances and risk factors in adulthood. Journal of Epidemiology & Community Health 53: 757–64. [Google Scholar]
- Bulder, Ruth, Victoria Tedjawirja, Jaap Hamming, Mark Koelemay, Ron Balm, Jan Lindeman, and A Study Group Collaborators. 2022. Hypothesis of the High Mortality of Female Patients Following Elective Open Abdominal Aortic Aneurysm Repair. European Journal of Vascular and Endovascular Surgery 63: 773–74. [Google Scholar] [CrossRef] [PubMed]
- Camelo, Lidyane, Amanda Viana Machado, Dóra Chor, Rosane Harter Griep, José Geraldo Mill, Luisa Campos Caldeira Brant, and Sandhi Maria Barreto. 2022. Racial discrimination is associated with greater arterial stiffness and carotid intima-media thickness: The ELSA-Brasil study. Annals of Epidemiology 72: 40–47. [Google Scholar]
- Cardano, Mario, Giudo Giarelli, and Giovanna Vicarelli. 2020. Sociologia della Salute e della Medicina. Bologna: il Mulino, pp. 1–442. [Google Scholar]
- Cassel, John. 1976. The contribution of the Social environment to host resistance. American Journal of Epidemiology 104: 107–23. [Google Scholar] [CrossRef] [PubMed]
- Costa, Davide. 2023. Diversity and Health: Two Sides of the Same Coin. Italian Sociological Review 13: 69–90. [Google Scholar]
- Costa, Davide, Michele Andreucci, Nicola Ielapi, Giuseppe Filiberto, Serraino Pasquale, Mastroroberto Umberto, Marcello Bracale, and Raffaele Serra. 2023. Molecular Determinants of Chronic Venous Disease: A Comprehensive Review. International Journal of Molecular Sciences 24: 1928. [Google Scholar] [CrossRef]
- Costa, Davide, Nicola Ielapi, Francesco Caprino, Nicola Giannotta, Antonio Sisinni, Andrea Abramo, Lwanga Ssempijja, Michele Andreucci, Umberto Marcello Bracale, and Raffaele Serra. 2022. Social Aspects of Diabetic Foot: A Scoping Review. Social Sciences 11: 149. [Google Scholar]
- Criqui, Michael, H. Maritess, Jamosmos Arnost, Fronek Julie, O Denenberg, Robert D. Langer, John Bergan, and Beatrice A. Golomb. 2003. Chronic venous disease in an ethnically diverse population: The San Diego Population Study. American Journal of Epidemiology 158: 448–56. [Google Scholar] [CrossRef]
- Cross, Terry. 1989. Towards a Culturally Competent System of Care: A Monograph on Effective Services for Minority Children Who Are Severely Emotionally Disturbed. Washington, DC: ERIC—Education Resources Information Center. [Google Scholar]
- CSDH (Commision on Social Determinats of Health). 2008. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health—Final Report of the Commission on Social Determinants of Health. Genève: World Health Organization. Available online: https://www.who.int/publications/i/item/WHO-IER-CSDH-08.1 (accessed on 10 January 2023).
- Davies, Huw O. B., Matthew Popplewell, Gareth Bate, Lisa Kelly, Andreas Koutsoumpelis, and Andrew W. Bradbury. 2017. Impact of UK NICE Clinical Guidelines 168 and social deprivation on access to interventional treatment for symptomatic varicose vein and specialist referral for leg ulceration. Phlebology 32: 548–52. [Google Scholar] [CrossRef] [PubMed]
- Demsas, Falen, Malachi M. Joiner, Kate Telma, Alyssa M. Flores, Semhar Teklu, and Elsie Gyang Ross. 2022. Disparities in peripheral artery disease care: A review and call for action. Seminars in Vascular Surgery 35: 141–54. [Google Scholar] [CrossRef] [PubMed]
- Dewan, Pooja, Rasmus Rørth, Pardeep S. Jhund, Joao Pedro Ferreira, Faiez Zannad, Li Shen, Lars Køber, William T. Abraham, Akshay S. Desai, Kenneth Dickstein, and et al. 2019. Income Inequality and Outcomes in Heart Failure: A Global Between-Country Analysis. JACC Heart Failure 7: 336–46. [Google Scholar] [CrossRef]
- de Weerd, Marjolein, Jaboba Greving, Anne De Jong, Erik Buskens, and Michiel Bots. 2009. Prevalence of asymptomatic carotid artery stenosis according to age and sex: Systematic review and metaregression analysis. Stroke 40: 1105–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, C. J., F. G. R. Fowkes, C. V. Ruckley, and A. J. Lee. 1999. Prevalence of varicose veins and chronic venous insufficiency in men and women in the general population: Edinburgh Vein Study. Journal of Epidemiology and Community Health 53: 149–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Federman, D. G., J. T. Trent, C. W. Froelich, J. Demirovic, and R. S. Kirsner. 1998. Epidemiology of peripheral vascular disease: A predictor of systemic vascular disease. Ostomy Wound Manage 44: 58–62. [Google Scholar]
- Freund, Peter. 1990. The expressive body: A common ground for the sociology of emotions and health and illness. Sociology of Health & Illness 12: 452–77. [Google Scholar]
- Haider, Adil, David Efron, Elliott Haut, Stephen DiRusso, Thomas Sullivan, and Edward Cornwell III. 2007. Black children experience worse clinical and functional outcomes after traumatic brain injury: An analysis of the National Pediatric Trauma Registry. Journal of Trauma and Acute Care Surgery 62: 1259–63. [Google Scholar] [CrossRef]
- Hsu, Harold, Lu Tony, Hansraj Natasha, Russeau Andrew, Kougias Panagiotis, and Barshes Neal R. 2022. Gender, racial and ethnic disparities in index hospitalization operations for symptomatic carotid stenosis in Texas hospitals. Annals of Vascular Surgery 80: 152–57. [Google Scholar] [CrossRef]
- Jacomelli, Jo, Lisa Summers, Anne Stevenson, Timothy Lees, and Jonathan Earnshaw. 2017. Editor’s Choice—Inequalities in Abdominal Aortic Aneurysm Screening in England: Effects of Social Deprivation and Ethnicity. European Journal of Vascular and Endovascular Surgery: The Official Journal of the European Society for Vascular Surgery 53: 837–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, Saemi, Youngki Kim, Dongmug Kang, Se Yeong, Kim Inah, Kim Eun, and Mi Kim. 2020. Distribution of working position among workers with varicose veins based on the National Health Insurance and National Employment Insurance data. Annals of Occupational and Environmental Medicine 32: e21. [Google Scholar] [CrossRef] [PubMed]
- Kim, Sooyeon, Anna Pendleton, and Katharine McGinigle. 2022. Women’s vascular health: Peripheral artery disease in female patients. Seminars in Vascular Surgery 35: 155–61. [Google Scholar] [CrossRef]
- Krieger, Nancy. 2001. Theories for social epidemiology in the 21st century: An ecosocial perspective. International Journal of Epidemiology 30: 668–77. [Google Scholar] [CrossRef] [PubMed]
- Kunst, Anton, and Jonathan Mackenbach. 2000. Measuring Socioeconomic Inequalities in Health. Copenhagen: WHO Regional Office Europe. [Google Scholar]
- Levine, Sol. 1987. The changing terrains in medical sociology: Emergent concern with quality of life. Journal of Health and Social Behavior 28: 1–6. [Google Scholar] [CrossRef] [PubMed]
- Li, Shimena R., Katherine M. Reitz, Jason Kennedy, Lucine Gabriel, Amanda R. Phillips, Paula K. Shireman, Mohammad H. Eslami, and Edith Tzeng. 2022. Epidemiology of age-, sex-, and race-specific hospitalizations for abdominal aortic aneurysms highlights gaps in current screening recommendations. Journal of Vascular Surgery 76: 1216–26. [Google Scholar] [PubMed]
- Link, Bruce George, and Jo Phelan. 1995. Social conditions as fundamental causes of disease. Journal of Health and Social Behavior, 80–94. [Google Scholar] [CrossRef] [Green Version]
- Mackenbach, Johan. 2012. The persistence of health inequalities in modern welfare states: The explanation of a paradox. Social Science & Medicine 75: 761–69. [Google Scholar]
- Marcaccio, Cristina, and Marc Schermerhorn. 2021. Epidemiology of abdominal aortic aneurysms. Seminars in Vascular Surgery 34: 29–37. [Google Scholar] [CrossRef] [PubMed]
- Marmot, Michael. 2014. Review of Social Determinants and the Health Divide in the WHO European Region. Copenhagen: World Health Organization. Regional Office for Europe. [Google Scholar]
- Marmot, Michael. 2015. The health gap: The challenge of an unequal world. The Lancet 386: 2442–44. [Google Scholar] [CrossRef]
- Moreira, Carla. 2021. Developing cultural competency and maximizing its effect in vascular surgery. Journal of Vascular Surgery 74: 76S–85S. [Google Scholar] [CrossRef] [PubMed]
- Morin, Edgar. 2007. Restricted Complexity, General Complexity. Science and Us: Philosophy and Complexity. Singapore: World Scientific, pp. 1–25. [Google Scholar]
- Morrissey, Nicholas J., Jeannine Giacovelli, Natalia Egorova, Annetine Gelijns, Alan Moskowitz, James McKinsey, Kenneth Craig Kent, and Giampaolo Greco. 2007. Disparities in the treatment and outcomes of vascular disease in Hispanic patients. Journal of Vascular Surgery 46: 971–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, Alan. 2002. Unequal treatment: Confronting racial and ethnic disparities in health care. Journal of the National Medical Association 94: 666. [Google Scholar] [PubMed]
- Ohrlander, Tomasa Merlo Juanb, Henrik Ohlsson, Björna Sonesson, and Stefan Acosta. 2012. Socioeconomic position, comorbidity, and mortality in aortic aneurysms: A 13-year prospective cohort study. Annals of Vascular Surgery 26: 312–21. [Google Scholar] [CrossRef] [PubMed]
- Osborne, Nicholas H., Amit K. Mathur, Gilbert R. Upchurch, and Justin B. Dimick. 2010. Understanding the racial disparity in the receipt of endovascular abdominal aortic aneurysm repair. Archives of Urgery 145: 1105–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osborne, Nicholas H., Gilbert R. Upchurch, Amit K. Mathur, and Justin B. Dimick. 2009. Explaining racial disparities in mortality after abdominal aortic aneurysm repair. Journal of Vascular Surgery 50: 709–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ottersen, Ole Petter, Jashodhara Dasgupta, Chantal Blouin, Paulo Buss, Virasakdi Chongsuvivatwong, Julio Frenk, Sakiko Fukuda-Parr, Bience P. Gawanas, Rita Giacaman, John Gyapong, and et al. 2014. The political origins of health inequity: Prospects for change. The Lancet 383: 630–67. [Google Scholar] [CrossRef]
- Page, Matthew J., Joanne E. McKenzie, Patrick M. Bossuyt, Isabelle Boutron, Tammy C. Hoffmann, Cynthia D. Mulrow, Larissa Shamseer, Jennifer M. Tetzlaff, Elie A. Akl, Sue E. Brennan, and et al. 2021. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 372: n71. [Google Scholar] [CrossRef]
- Paudel, Sudarshan, Anwar Zaitoun, Saif Al-Najafi, Thaer Musa, R. N. Dawn Light, Rajendra H. Mehta, and Howard S. Rosman. 2017. The association of gender with quality of health in peripheral arterial disease following peripheral vascular intervention. Vascular Disease Management 14: E218–E224. [Google Scholar]
- Qaja, Erion, Prasanna Tadi, and Theetha Pramod Kariyanna. 2022. Carotid Artery Stenosis. In StatPearls [Internet]. Treasure Island: StatPearls Publishing. [Google Scholar]
- Ramkumar, Niveditta, Bjoern Suckow, Shipra Arya, Art Sedrakyan, Todd Mackenzie, Philip Goodney, and Jeremiah Brown. 2020. Association of Sex with Repair Type and Long-Term Mortality in Adults with Abdominal Aortic Aneurysm. JAMA Network Open 3: e1921240. [Google Scholar] [CrossRef] [Green Version]
- Raphael, Dennis. 2006. Social determinants of health: Present status, unanswered questions, and future directions. International Journal of Health Services 36: 651–77. [Google Scholar] [CrossRef]
- Samson, David, and Karen Schoelles. 2012. Medical tests guidance (2) developing the topic and structuring systematic reviews of med-512 ical tests: Utility of PICOTS, analytic frameworks, decision trees, and other frameworks. Journal of General Internal Medcine 27: 11–19. [Google Scholar] [CrossRef] [Green Version]
- Sandiford, Peter, Damien Mosquera, and Dale Bramley. 2012. Ethnic inequalities in incidence, survival and mortality from abdominal aortic aneurysm in New Zealand. Journal of Epidemiol Community Health 66: 12. [Google Scholar] [CrossRef]
- Schul, Marlin W., Ted King, and Lowell Kabnick. 2014. Inequalities of health insurance guidelines for the treatment of symptomatic varicose veins. Phlebology 29: 236–46. [Google Scholar] [CrossRef]
- Serra, Raffaele, Raffaele Grande, Lucia Butrico, Franceso Fugetto, and Stefano de Franciscis. 2016. Epidemiology, diagnosis and treatment of chronic venous disease: A systematic review. Chirurgia 29: 34–45. [Google Scholar]
- Siegrist, Johannes. 1996. Adverse health effects of high-effort/low-reward conditions. Journal of Occupational Health Psychology 1: 27. [Google Scholar] [CrossRef] [PubMed]
- Solar, Orielle, and Alec Irwin. 2010. A conceptual Framework for Action on the Social Determinants of Health. Geneva: WHO Document Production Services. [Google Scholar]
- Tüchsen, Finn, Neal Krause, Hermann Burr, and Tage Kristensen. 2000. Standing at work and varicose veins. Scandinavian Journal of Work, Environment & Health 26: 414–20. [Google Scholar]
- Wilkinson, Richard, and Kate Pickett. 2006. Income inequality and population health: A review and explanation of the evidence. Social Science & Medicine 62: 1768–84. [Google Scholar]
- Wright, A. P., D. C. Berridge, and D. J. A. Scott. 2006. Return to work following varicose vein surgery: Influence of type of operation, employment and social status. European Journal of Vascular and Endovascular Surgery: The Official Journal of the European Society for Vascular Surgery 31: 553–57. [Google Scholar] [CrossRef] [Green Version]
- Ziaja, Damian, Mariola Sznapka, Joanna Grzela, Jacek Kostecki, Grzegorz Biolik, Krzysztof Pawlicki, Krzysztof Ziaja, Jerzy Chudek, Marek Maruszynski, Aleksander Molski, and et al. 2015. Regional variations of symptoms of the chronic venous disease among primary health care patients in Poland. Acta Angiologica 21: 31–39. [Google Scholar] [CrossRef] [Green Version]
- Zommorodi, Sayid, Karin Leander, Joy Roy, Johnny Steuer, and Rebecka Hultgren. 2018. Understanding abdominal aortic aneurysm epidemiology: Socioeconomic position affects outcome. Journal Epidemiol Community Health 72: 904–10. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Keywords | Scopus | ScienceDirect |
|---|---|---|
| Chronic venous disease * AND inequality * OR inequity * OR social differences * | 37 | 29 |
| Peripheral * AND inequality * OR inequity * OR social differences * | 5 | 33 |
| Carotid stenosis *AND inequality * OR inequity * OR social differences * | 7 | 9 |
| Aortic aneurysm * AND inequality * OR inequity * OR social differences * | 70 | 11 |
| Parameter | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Source | Studies that studied the concept of SDHs in specific VDs (AAA, PAD, CVD.CS). | Studies that did not focus on SDHs in VDs focused on biological aspects as SDHs. |
| Intervention | Analysis of the SDHs factors affecting VDs. Analysis of the material contribution that SDHs has to VDs (AAA, CS, CVD, PAD). | Only if there are generic descriptions in terms of both VDs, without a specific analysis of each of them, and in terms of SDHs detected. Only if there are generic descriptions in terms of VDs, without a specific analysis of each of them, and in terms of SDHs |
| Comparator | Not applicable | Not applicable |
| Outcomes | To reduce the negative impact of the mismanagement of SDHs with VDs. | Interventions, approaches or tools not focused on SDHs in VDs |
| Timeframe | Unrestricted (final extraction: July 2022) | Unrestricted (final extraction: July 2022) |
| Study Type | Research and review articles published in peer-reviewed journals | Brief reports, draft, letter to editors, communications, supplements, book or book chapters, meeting abstracts, editorials, theses or dissertations, unavailable complete papers, reviews that did not meet the criteria of a systematic review |
| Language | English | Not in English |
| Type of Vascular Disease | |||||
|---|---|---|---|---|---|
| PAD | CVD | AAA | CS | AAA, PAD, and CS | |
| Number of articles | 3 | 8 | 8 | 2 | 1 |
| Authors | Publication Year | Country | Study Design | Main Results | SDH Studied | VD Studied |
|---|---|---|---|---|---|---|
| Evans et al. | 1999 | United Kingdom | Cross selectional survey | No evidence of bias in the study was found to account for this sex difference. Changes in lifestyle or other factors might contribute to an alteration in the epidemiology of CVD. | Gender | CVD |
| Tuchsen et al. | 2000 | Denmark | Prospective Cohort Study | For men working mostly in a standing position, the risk ratio for varicose veins was compared with that for all other men. Thus, working in a standing position was associated with subsequent hospitalization due to varicose veins for both men and women. | SES Gender | CVD |
| Criqui et al. | 2003 | United States | Cross selectional study | The authors found that women with different ethnicities had more superficial functional disease, whereas men had more deep functional disease. Nonetheless, discordance within the leg for visible functional and clinical disease was not uncommon. | Ethnicity Gender | CVD |
| Wright et al. | 2006 | United Kingdom | Retrospective cohort study | Employed patients and those involved in intensive manual labor were less likely to return to work early. There was no effect of gender or the incidence of complications. | SES Gender | CVD |
| Osborne et al. | 2009 | United States | Longitudinal study | Black patients had much higher risk-adjusted mortality after aneurysm repair than nonblack patients. Mortality rates were higher in hospitals treating a higher proportion of black patients. Adjusting for these differences in hospital quality, this disparity was no longer significant. | Ethnicity SES | AAA |
| Osborne et al. | 2010 | United States | Retrospective cross-sectional study | The relationship between race and type of AAA repair, controlling for differences in patient factors, and adjusting for the hospitals where patients received care. | Ethnicity SES | AAA |
| Ohrlander et al. | 2012 | Sweden | Prospective Cohort Study | Inferior socioeconomic position was associated with increased 3-year all-cause mortality in 60 to 79-year-old men with AAA. | Gender SES | AAA |
| Sandiford, et al. | 2012 | New Zealand | Retrospective cross-sectional study | Mahori had higher mortality rates, lower survival. Maori women, but not men, were found to have a significantly higher standardized incidence rate. Thus, ethnic variation in incidence, mortality, and cumulative relative survival of AAA resembled ethnic inequalities in other health outcomes. | Ethnicity Gender | AAA |
| Schul et al. | 2014 | United States | Review | Patients and physicians are increasingly ill-served by, and frustrated with, the clear lack of consistency in the medical policy criteria being created by US insurance carriers in covering the treatment of patients with symptomatic varicose veins. | SES | CVD |
| Ziaja et al. | 2015 | Poland | Multi-centre epidemiological study | There is a significant territorial diversity in Poland in the frequency of reported symptoms and of the conservative therapy of CVD. | SES | CVD |
| Davies et al. | 2017 | United Kingdom | Retrospective cohort study | There is an improvement in access to treatment, and referral may have disproportionately favored the more socio-economic privileged. Professional and public education is required to ensure that the beneficial impacts of recommendations are maximized and that those with the greatest health needs have equal access to evidence-based management of their CVD. | SES | CVD |
| Jacomelli et al. | 2017 | United Kingdom | Longitudinal study | Social deprivation affects the uptake of AAA screening in 65 -year-old men. Local factors are the most important determinants of uptake, so solutions to improve uptake must be designed at the local, not national level. | Ethnicity Gender | AAA |
| Sudarshan et al. | 2017 | United Stated | Prospective Cohort Study | The study complements the prior vascular literature and adds to our understanding of the impact of gender on health status in PAD. The gender-related impact on health status is more pronounced in the milder form of disease. | Gender | PAD |
| Zommorodi et al. | 2018 | Sweden | Retrospective cross-sectional study | Individuals with low SES were found to have an augmented risk of presenting and, in addition, to fare worse after repair. Consequently, it should be regarded as a relevant risk factor that should be included in considerations for improved care flow of patients with AAA. | SES | AAA |
| Jung et al. | 2020 | Korea | Retrospective cross-sectional study | This study was performed to determine the characteristics of CVD with different working posture among Korean workers. It is expected to be the basis of further studies on occupational musculoskeletal diseases. | SES | CVD |
| Ramkumar et al. | 2020 | United states | Retrospective cohort study | In this study, women were more likely than men to undergo open surgical repair. After EVR repair, women were more likely to die than men, although no sex-based difference in mortality was found after open surgical repair. The differential treatment benefit of EVR repair in women is concerning given the shift toward an EVR-first approach to AAA repair. | Gender | AAA |
| Brathwaite et al. | 2021 | United States | Review | The prevalence of PAD in Black Americans is significantly greater than that reported for White Americans. Black patients experienced major lower extremity amputation at two to four times the rate of white patients with PAD, with significant variation found among the various regions in the United States regarding the intensity of vascular care provided to vulnerable populations with PAD before major amputations. | Ethnicity | PAD |
| Barshes et al. | 2021 | United States | Review | Racial and ethnic disparities in AAA and CS have existed for decades. New approaches are needed to address these disparities. | SES Ethnicity Gender | AAA PAD CS |
| Li et al. | 2022 | United States | Retrospective cohort study | The contemporary incidence and risk of AAA hospitalization in the United States varied significantly by age, sex, and race. Female sex as well as racial minority groups were associated with substantial decreases, while older age and white race conferred significant increases in the incidence and adjusted odds of AAA hospitalization. | Gender Ethnicity | AAA |
| Hsu et al. | 2022 | United States | Retrospective cross-sectional study | Blacks and Browns presented worse profiles of subclinical vascular markers compared to Whites, and those exposed to racial discrimination seemed to have an additional vascular risk. | Ethnicity | CS |
| Demsas et al. | 2022 | United States | Review | The authors reviewed studies to provide a comprehensive analysis of the current impact of disparities on the treatment and management of PAD and offer action items that require strategic partnership with primary care providers, researchers, patients, and their communities. | Ethnicity Gender SES | PAD |
| Camelo et al. | 2022 | Brasil | Longitudinal study | Gender, race, and ethnicity appear to correlate with rates of carotid intervention at index hospitalization despite thorough risk adjustment for clinical, social, and demographic factors. | Ethnicity Gender | CS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, D.; Ielapi, N.; Bevacqua, E.; Ciranni, S.; Cristodoro, L.; Torcia, G.; Serra, R. Social Determinants of Health and Vascular Diseases: A Systematic Review and Call for Action. Soc. Sci. 2023, 12, 214. https://doi.org/10.3390/socsci12040214
Costa D, Ielapi N, Bevacqua E, Ciranni S, Cristodoro L, Torcia G, Serra R. Social Determinants of Health and Vascular Diseases: A Systematic Review and Call for Action. Social Sciences. 2023; 12(4):214. https://doi.org/10.3390/socsci12040214
Chicago/Turabian StyleCosta, Davide, Nicola Ielapi, Egidio Bevacqua, Salvatore Ciranni, Lucia Cristodoro, Giuseppina Torcia, and Raffaele Serra. 2023. "Social Determinants of Health and Vascular Diseases: A Systematic Review and Call for Action" Social Sciences 12, no. 4: 214. https://doi.org/10.3390/socsci12040214