Abstract
(1) Background: “To change the world, we must first change the way the babies are being born”, said Michel Odent, the famous French obstetrician and pioneer of the “natural birth” movement. This quotable phrase has been widespread in activism campaigns, and it refers to a project for social change that goes beyond birth. Conceiving childbirth in the broader social context, it is not surprising that this emblematic quote inspires emancipatory struggles around birth. This paper results from a study of childbirth activism in different European contexts, where the author explores the emergence and modes of action of social movements advocating for the humanization of childbirth and women’s rights in pregnancy and childbirth. (2) Methods: Starting from the analysis of the main characteristics of childbirth activism, in this paper the author briefly analyzes the cases of organizations from Portugal, Spain and the Netherlands, as well as a campaign promoted by the European Network of Childbirth Associations (ENCA). The author mobilizes empirical data resulting from a triangulation approach, essentially based on documentary analysis, complemented by conversations and participant observation in different settings. (3) Results: Preliminary results show how childbirth activism is contributing to the construction of alternative conceptions of birth, challenging established paradigms. (4) Conclusion: In its differences and similarities, childbirth activism assumes distinct features, but it also has the ability to adapt and promote changes, depending on the specificities of the contexts where it operates.
1. Introduction
Pregnancy and childbirth are major events for women, surrounded by many cultural understandings, rituals and practices (Iravani et al. 2015). In this sense, it is important to explore what narratives societies are building around such significant processes.
As a biographical episode, childbirth is a life-changing experience, full of vital and sometimes spiritual significance (Fedele 2015). As a social and collective phenomenon, childbirth may be conceived, in the context of medicalization of society, as a medical procedure involving a wide range of knowledge, practices and attitudes.
Nonetheless, for a long time, reproductive processes and experiences of mothering were broadly absent from the focus of social sciences. Even second-wave feminism, in its determination in distinguishing public and private spheres, has opposed women’s emancipation to reproductive labor, contributing to hiding the latter from the sociological gaze (Oakley 2016). It is through the intersection of feminist theories with the critiques of medicalization that, from the late 1970s, childbirth and maternity care started garnering more attention, even if they remain on the periphery of mainstream concerns of social sciences (McCourt and Dykes 2010; Oakley 2016; Santos and Neves 2021).
One of the topics approached by social studies on childbirth is related to paradigms of childbirth in contemporary societies. The use of terms such as “natural”, “normal” or “medicalized” birth is deeply influenced by Davis-Floyd’s definition of the three paradigms of childbirth: the technocratic, humanistic and holistic models (Davis-Floyd 2001). The concept of medicalization refers to the influence of medicine in many aspects of social life (Conrad 2007), and actually, in most European countries, pregnancy and childbirth are life events where risk management and technocratic practices of care are dominant (Pintassilgo and Carvalho 2017).
Additionally, research on maternity care has focused traditionally on the identification of risk factors and the reduction in adverse outcomes, with less attention given to the factors contributing to women’s and babies’ well-being and the wholeness of the birth experience (Todres et al. 2009; Smith 2014).
The transition to motherhood is a multidimensional phenomenon which can benefit from a transdisciplinary approach as it is able to integrate dimensions from medical, social, psychological, political and cultural perspectives. Currently, as an alternative to dominant conceptions, new perspectives are gaining relevance in public narratives on childbirth, promoting a more holistic definition and pushing practices of perinatal care towards a growing focus on women’s subjectivities and choices (the woman-centered perspective). Although in contexts such as the UK, US and Canada, these perspectives are not exactly new and have long been popularized in other European countries, particularly in Southern Europe, they are still in the initial stages (White and Schouten 2014; Fedele 2015).
In this sense, the critiques of medicalization have been a confluent territory for activists and academics. According to Oakley (2016), political activism reframed issues as “matters of concern”, and in this process, sociological research has been useful, providing “academic support” to women’s complaints.
Childbirth Activism: An Overview
Collective action is an established feature of any society and poses a challenge to inequality, exclusion and the oppression of people (Millward and Takhar 2019). A range of theories, from different areas of social and political sciences, have been developed over time to understand the rise of social movements and their achievements. Recent debates within new social movement theory tend to look at social movements from a cultural position, with claims more related to lifestyle rather than those that are structurally rooted. For Scott (1990, apud Millward and Takhar 2019), unlike classical mass movements, new social movements tend to be linked to a single broad theme or interest rather than the traditional focus on the working classes. As such, it is said that new social movements are not conceived to develop notions of total politics but to seek changes by lobbying specific social spheres.
Childbirth activism can be understood within the scope of new social movements. Even so, when Michel Odent states “to change the world, we must first change the way the babies are being born”,1 what is actually being assumed is that childbirth is a starting point for a broader social change. And it is not unintended that his quote became so emblematic of childbirth activism around the world.
But what do we actually know about childbirth activism? And what do childbirth organizations in Western countries do? Although it is an overlooked topic within mainstream studies on social movements and collective action, according to Akrich et al. (2014, pp. 1–2), a review of the existing literature on childbirth movements in Europe “reveals a degree of similarity in their causes which cluster around four key goals: (1) problematising medical/technical intervention in birth; (2) promoting ‘natural’/’normal’ or ‘mother friendly’ birth; (3) demanding birth practices and settings that are attentive to and respectful of the desires of birthing women and their families and (4) championing women’s right to make informed choices about type and place of birth”.
Besides a critical positioning towards mainstream medical practices of birth, efforts to promote ‘natural’/’normal’ birth and a focus on women’s choices and rights, what seems to be distinctive of childbirth activism is its evidence-based orientation. Akrich et al. (2014) highlight that, despite the pluralism of the movement and the diversity of the organizations’ trajectories, childbirth activism is, in its pivotal focus, committed to evidential work and a recognition of the power of knowledge. Organizations usually collect, produce, mobilize and share different forms of knowledge, from evidence derived from women’s voices and based on their own experiences of birth to scientific evidence resulting from medical expertise and healthcare authorities.
Moreover, work on evidence plays an important role in increasing the real possibilities to produce changes in various settings. On the one hand, it contributes to the legitimization of the movement, facilitating negotiations with health institutions and policy makers. On the other, through the dissemination of knowledge and evidence-based recommendations, childbirth activism allows women and families to be informed and aware about rights and healthcare procedures, empowering them in their relationship with healthcare providers.
2. Materials and Methods
This paper draws on sociological research on childbirth activism in different European contexts, where the author explores the emergence and the modes of action of social movements advocating for the humanization of childbirth and women’s rights in pregnancy and birth. The work focuses on the cases of organizations from Portugal, Spain and the Netherlands, as well as on a campaign promoted by the European Network of Childbirth Associations (ENCA). The data mobilized in the analysis result from documentary research in official sources of the organizations (websites, leaflets, etc.), complemented by informal conversations with representatives of the organizations and participant observation at meetings. The contact and communication with the Portuguese organization (APDMGP) have been more constant, given the author’s participation in the Portuguese activist movement since 2016. It was in the quality of birth rights advocacy that the author became acquainted with ENCA and its member organizations. Participant observation and direct conversations with representatives of Spanish and Dutch organizations (Birth is Ours and ENCA Nederland) took place in May 2019, during the annual ENCA meeting in Zagreb, Croatia. Following a data triangulation approach (Denzin 1978), both the contact with members of the organizations and the participant observation served as means for accessing, deepening or confirming the collected information about the history, characteristics and modes of action of each organization under analysis.
3. Results and Discussion
3.1. Childbirth Organizations from Spain, Portugal and The Netherlands
Spain and Portugal are two southern European countries that have improved perinatal health indicators in the last decades (Euro-Peristat Project 2013, 2018; WHO 2014; Wang et al. 2014). As in many other Western countries, maternal and perinatal health paradigms have been focusing on preventing maternal and perinatal severe morbidity and mortality as the ultimate purpose. In this context, risk management has become a central issue in pregnancy and birth assistance, being associated with increased obstetric surveillance and intervention (Conrad 2007; Pintassilgo and Carvalho 2017).
Still, the case of Spain is more heterogeneous, as it constitutes regions with autonomy to define their healthcare systems, resulting in a greater diversity in terms of perinatal assistance in the country.
The Spanish organization under study is El Parto es Nuestro (Birth is Ours), founded in 2003. It is a non-profit and non-professional association, essentially composed of mothers and families and pursuing improvement in the assistance conditions for mothers and children during pregnancy, birth and postpartum.
Concerning agendas, in Spain, especially in recent years, there have been some intersections between childbirth activism and women’s rights movements, as the conceptualization of obstetric violence as violence against women shows. El Parto es Nuestro is also represented in Latin America, through a group in Ecuador and another in Argentina, and it has, under the Spanish organization, other concerns related to sexual and reproductive health and rights in its field of action, such as abortion rights.
In addition to the reporting of obstetric mistreatment and the disseminating of recommendations from international authorities for the promotion of good practices in obstetric care, the most striking feature of this organization concerns the horizontality and decentralization of its functioning. El Parto es Nuestro practices a peer-to-peer transmission, promoting many local groups of sharing and support throughout the national territory on a regular basis.
Like Spain, Portugal presents high rates of medical intervention in childbirth, reflected in trends such as the strong presence of doctors during birth, the increase in instrumental deliveries or the growth of caesarean rates, particularly in private hospitals (Pintassilgo and Carvalho 2017). Moreover, medical interventions that are recommended against in the scientific literature, such as episiotomy, are common in Portuguese maternity health services, sometimes without the informed consent or even against the explicit will of parturients.2
The Portuguese Association for Women’s Rights in Pregnancy and Childbirth3 (APDMGP) is a non-profit organization, founded in 2014 with the aim of promoting human rights in pregnancy and birth. The functioning of the APDGMP is especially based on direct contact with and support for women and families, providing emotional and judicial support, producing and sharing tools and resources on the website and organizing antenatal discussion groups. The APDMGP also develops collaborative work with public institutions such as governmental entities working on health and gender equality areas and political parties, as well as with other civil society organizations, particularly women’s organizations and health professionals’ associations. Despite its recent inception, the Portuguese childbirth movement has already managed to put women’s rights in childbirth on the political and public agenda and has contributed, through advocacy, to important legislative advances in this area. Given the broad spectrum of its mission and setting, it seems reasonable to say that this Portuguese activist organization stands somewhere in between a human rights organization and an association of healthcare services users/consumers.
Compared to the previous countries discussed, the Netherlands represents a very different reality in terms of maternity care assistance. Its model reflects lower levels of institutionalization and medicalization of childbirth and the predominance of what is called the midwifery care model. In 2020, 15% of the births in the country were homebirths and 12% occurred in small maternity units. The C-section rate was 17% and the episiotomy rate was 16% (Perined 2021).
Just as the model of birth is different from other countries, the ways of activism in the country are quite singular too. Founded in 2006, ENCA Nederland is a platform organization composed of many member organizations. This platform supports birth activism, focusing on the perinatal education of women/couples and promoting knowledge and health literacy. It also seeks to gather and disseminate evidence and recommendations from international health authorities.
ENCA Nederland flags the midwifery care model as a distinctive feature of the country, considering it a trait to be preserved, acknowledged and reinforced. Member organizations of this platform are distinctive and closely related to private services and professional associations acting in the perinatal field, such as associations of yoga professionals, antenatal educators, midwives’ organizations and doulas associations. Thus, professional dynamics in the birth scenario are also an important issue to this activist organization.
ENCA Nederland directly addresses women and families on the one hand through the provision of ante- and postnatal services, and health professional groups on the other by promoting synergy between different providers, such as perinatal educators, midwives, doctors and doulas, and by advocating for better guarantees for them.
3.2. International Network and Campaigns
3.2.1. The European Network of Childbirth Associations
The European Network of Childbirth Associations (ENCA) was launched in 1993 in Frankfurt (Germany) and is a network of organizations campaigning for improvements in perinatal care for mothers and babies. Depending on the organizations, the members joining ENCA are user activists, mothers, health providers or childbirth educators who recognize the need to develop strategies to improve conditions and rights in pregnancy, birth and postpartum throughout Europe.
ENCA is oriented by principles, supported by its member organizations: (1) empowerment of women; (2) family-oriented birth; (3) breastfeeding; (4) midwife care model.
This international network is currently spread over 19 European countries. National representatives meet regularly and develop joint actions and campaigns, such as the campaign for the dissemination of the World Health Organization’s recommendations on perinatal care and for the sharing of good practices based on scientific evidence. Each organization is responsible for disseminating the information and the results of these actions to the public, civil society and decision-makers in its own country.
3.2.2. International Week for Respecting Childbirth
The International Week for Respecting Childbirth (IWRC) is an international campaign, focusing on a specific topic related to the promotion of gentle birth. The IWRC was launched for the first time in 2004 by the French Alliance for Respected Childbirth4 (AFAR), a French non-profit society. Since 2011, the coordination of this campaign has been handed over to the European Network of Childbirth Associations (ENCA).
The IWRC takes place every year during the month of May. Depending on the theme, objectives and ideas for action are proposed and debated during the ENCA annual meeting. Individuals or groups may then work out the particular steps, taking advantage of the material that has been collectively prepared and made available on the website: posters, folders, leaflets, etc. Depending on the national contexts and resources, many events can be organized at a smaller or larger scale, such as exhibitions, meetings and conferences.
For the analysis of the birth narratives and conceptions, the IWRC campaign reflects demands that are consensually chosen each year by childbirth organizations from different countries. Through each slogan, we can perceive what issues have been prioritized over the years as transversal needs to many European countries and not strictly related to national contingencies.
From 2012 to 2024, these were the slogans of the IWRC Campaign:
- The Economics of Birth (2012);
- Do not disturb! Birth in Progress (2013);
- Birth is Empowering! (2014);
- Continuous love and support for me and my baby! (2015);
- My decision, my body, my baby! (2016);
- 40 weeks? Birth has a right time, not a scheduled time (2017);
- Less Interference, More Care (2018);
- The power for birth is IN you (2019);
- My decision must be respected (2020);
- Respect for the needs of mother and her baby in any situation (2021);
- Better birth for a better future (2022);
- Supporting Birth = Supporting Families (2023);
- Hard Data, Mother’s Choice, Flexible Care (2024).
In contrast with dominant approaches to childbirth in mainstream health institutions, which activism depicts as disrespectful and non-evidence-based care, the core of the IWRC demands over the 13 years under ENCA’s hosting could be encapsulated as (1) care (support), (2) respect for physiology (less routine intervention) and (3) rights in childbirth (women’s decision/agency) (3). The following images, relating to three specific years of the campaign, are examples of this.
In 2015, beside the statement of birth as a public health issue, the IWRC campaign advocated for continuous support for women during childbirth (Figure 1). Continuous support in labor is defined as continuing support to women provided by one provider, from at least early labor through until at least the birth. This definition includes emotional support (continuous presence, reassurance and praise), information about the progress of labor, advice on techniques for pain relief, techniques to improve comfort, etc. Authors have highlighted that, historically, women have generally been supported by other women during labor. This has changed throughout the twentieth century, as the institutionalization of birth has led to big changes in birth care. Currently, in hospitals worldwide, the workload and institutional protocols make one-to-one intra-partum care difficult, and continuous support during labor has often become the exception rather than the norm (Bergström 2011; Hodnett et al. 2013; Bohren et al. 2017).
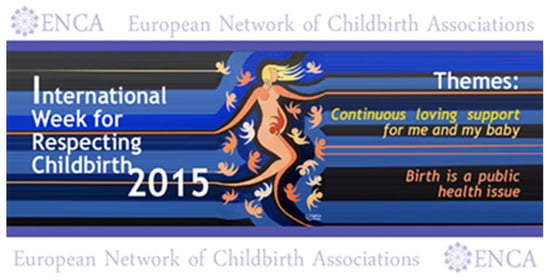
Figure 1.
IWRC campaign banner in 2015.
Thus, continuous support during labor and childbirth has become a banner of birth activism, as scientific evidence demonstrates its benefits for women and babies, making clear the weaknesses of the dominant health care models in our society. Support in labor may reduce anxiety and stress, which has a negative effect on the childbirth experience and on the course of labor (Bergström 2011). Other reported benefits include positive feelings about the childbirth experience; increased spontaneous vaginal birth; shorter duration of labor; decreased caesarean birth, instrumental vaginal birth and use of any analgesia and low five-minute Apgar score (Bohren et al. 2017). In this sense, as in the 2015 IWRC campaign, childbirth organizations are committed to disseminating scientific evidence reiterating that all women should have support throughout labor and birth, in order to improve maternity care assistance, women’s satisfaction about birth experiences and health outcomes.
In 2017, the IWRC was dedicated to the theme of less interference in childbirth, pointing out a generalized practice of abusive labor inductions and obstetric interventions in general (Figure 2). As in other years, the focus was on a fundamental issue to the conceptualization of childbirth: time. Childbirth activists believe that respecting the natural process of giving birth also means honoring the time it takes, as they trust that nature knows best.

Figure 2.
IWRC campaign banner in 2017.
This view opposes the institutionalized and medicalized model of childbirth, dominant in many European countries, where clinical environments commonly based on notions of risk and pathology prevail, and the control of time has a preponderant role, with the consequence of high rates of obstetric intervention.
The European Perinatal Health Report (Euro-Peristat Project 2018)—an international survey that gathers epidemiological evidence on birth on a comparative basis—shows that countries such as Portugal and Spain are among those with the highest rates of induction of labor, among other interventions. In this way, opposition to interference with time in birth has become very common in the activism rhetoric and critical thinking, raising suspicions about the negative effects of the prevalence of the technocratic model in childbirth care (McCourt and Dykes 2010). In an evident manner, the tendency for time control in pregnancy and birth shows up in phenomena such as the standardization of pregnancy duration around 40 weeks, as well as in a higher frequency of births on certain weekdays (Pintassilgo and Carvalho 2017). However, other perspectives which have an impact on childbirth activism go further in the discussion, considering the potential lasting consequences of the excess of interventionism for mothers’ and infants’ lives and the impact for the next generations (Odent 2015).
The campaign of 2020 was enlightening about the central characteristics and ways of action of childbirth activism organizations (Figure 3). The theme of the IWRC 2020 was chosen in 2019, during the annual meeting of ENCA, before the COVID-19 pandemic had started and far from foreseeing all the constraints that maternal healthcare systems would face worldwide.
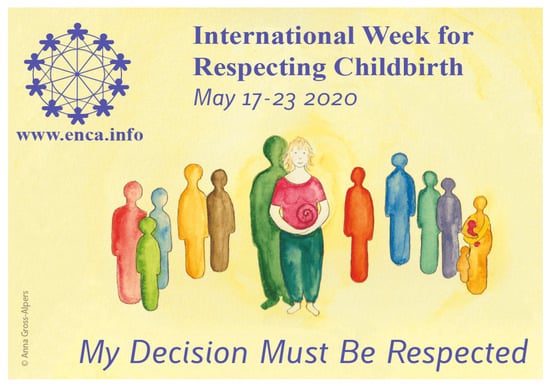
Figure 3.
IWRC campaign banner in 2020.
Under the motto “My decision must be respected”, the IWRC campaign endeavored to point out women’s rights in pregnancy and birth and to disseminate recommendations from international authorities in terms of respectful and woman-centered care. On the ENCA website, some images were released, accompanied by quotes from The United Nation Office of the High Commissioner for Human Rights (UN Human Rights), showing facts and recommendations regarding women’s rights in childbirth (Figure 4).
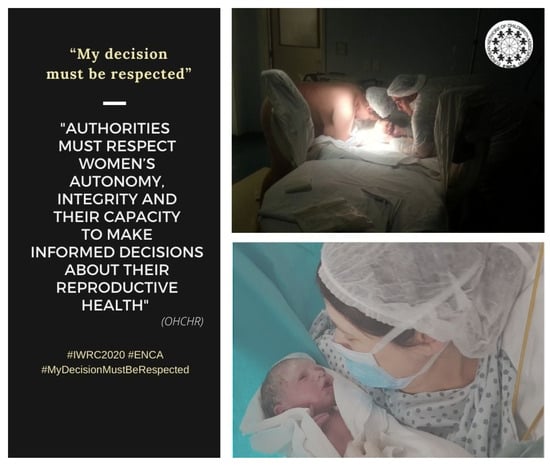
Figure 4.
Images of the 2020 IWRC campaign.
However, the COVID-19 pandemic showed the extent to which the achievements of childbirth rights over the years can be easily overridden, despite the tenacity of activists’ demands for the reinstatement of women’s rights in obstetric care services.
In many European countries, childbirth organizations reacted to the COVID-19 pandemic in the maternity care system by seeking to disseminate international guidelines and mobilizing evidence-based arguments, often contradicting the measures adopted by national authorities and health institutions. Under the guise of preventive measures, health institutions invested in already existing practices that tend to objectify women and to limit their agency in childbirth, considering personal rights as revocable in the face of a major threat to human life and to society (Neves and Barata 2023; Barata et al. 2020).
When ENCA chose the theme of IWRC 2020, nobody knew the world would be facing a pandemic with such a huge impact on childbirth assistance worldwide. Nonetheless, in face of this dismissal of respect for women’s decisions resulting from COVID-19 containment measures, this campaign took on particular significance.
4. Conclusions
New childbirth cultures have emerged in European societies, by the hands of new social actors, professional groups and civil society movements. The latter, mobilizing the voices of women, families and healthcare providers, provide dialogue with instances of political power and decision makers, seeking to inform new policies and promote changes in mainstream birth assistance.
In its diversity, and in general terms, birth activism seems to be a reaction to the following: (1) a paradigm that conceives and therefore manages childbirth as a highly medicalized and institutionalized phenomenon; (2) the disrespect of human rights and women’s loss of autonomy and agency in the birthing process and (3) the normalization of disrespectful care practices and interventions, alien to women’s choices or scientific evidence, in mainstream maternity care services.
Through the mobilization of specific examples of national organizations and international campaigns, this paper sheds light on the role of social movements in the construction of alternative birth narratives in contemporary societies. Looking at the similarities between cases, as well as their specificities, it has highlighted the ways these movements tend to contradict medicalized and technocratic models of childbirth, focusing on understanding childbirth as a personal and highly significant experience. Furthermore, evidential work is a transversal characteristic, allied to the dissemination of knowledge and the search for increasing health literacy and women’s satisfaction with childbirth experiences.
Nonetheless, differences between the contexts under analysis (namely in terms of the mainstream birth care provided) produce some diversity and nuances in the goals and the capacity for intervention within birth activism in Europe.
First, childbirth movements in Europe have different dimensions and origins. Some were founded by women and their families in a logic of users’ rights or peer-to-peer support, while some draw on professional confederations, and others derive from the congregation of multiple perinatal sectors, without excluding the private sector and business, as in the Dutch case. As a result, discourses and revindications may be more or less politicized, namely in terms of proposing—or not—social and political changes that go beyond the birth setting.
Childbirth activists also differ with respect to their ability and interest in establishing intersections and sharing agendas with other social movements, for instance, with feminist and women’s organizations. Still, in terms of institutional relations, and due not only to internal variances but also to differences in the political contexts in which these organizations operate, there is a differential capacity to advise decision makers and to influence new health and family policies.
In short, and as a final remark, through their activities, childbirth organizations produce knowledge, establish new fields of action and create new discourses and conceptualizations. The combination of evidence-based activism and the capacity to reframe issues related to childbirth goes beyond mere opposition to medicalization (Akrich et al. 2014), which deserves, from researchers and academics, a closer look and more systematic attention.
Funding
This work was supported by the Fundação para a Ciência e a Tecnologia (FCT) through the funding of the R&D Unit UIDB/03126/2020 and SFRH/BPD/94537/2013.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and according to the Code of Conduct of Ethics of Iscte—Instituto Universitário de Lisboa, 2016, in the general framework of the mission and duties of the Ethics Committee of Iscte (Order No. 7095/2011; Diário da República, 2.ª série—N.º 90—10 June 2011).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
This work was based on data available on websites and other public documents produced and disseminated by the forementioned organizations. No personal information is mentioned, nor are any subjects identified in this study.
Conflicts of Interest
The author declares no conflict of interest.
Notes
| 1 | Although this quotation is attributed to Michel Odent on various occasions, encapsulating the idea that the author develops in several works and lectures, it is difficult to define its exact origin. In an interview published in 2023, Michel Odent mentioned he had written this phrase “a long time ago”, “perhaps in 1976”, without specifying its origin (Ramos 2023, p. 31). |
| 2 | In 2015, this fact motivated an urgent recommendation from the Committee for the Elimination of Discrimination against Women (CEDAW) to the Portuguese government: https://plataformamulheres.org.pt/site/wp-content/ficheiros/2015/11/RecomendacoesCEDAW-PT-TraducaoPpDM30Nov2015.pdf (accessed on 14 July 2024). |
| 3 | Associação Portuguesa pelos Direitos da Mulher na Gravidez e Parto. |
| 4 | Alliance Française pour l’Accouchement Respecté. |
References
- Akrich, Madeleine, Máire Leane, Celia Roberts, and João Arriscado Nunes. 2014. Practising childbirth activism: A politics of evidence. BioSocieties 9: 129–52. [Google Scholar] [CrossRef]
- Barata, Catarina, Dulce Morgado Neves, and Mário Santos. 2020. COVID-19 Containment Measures, Perinatal Experiences, and the Fight for Childbirth Rights in Portugal. Medical Anthropology Quarterly—Blog on COVID-19 Responses. Hoboken: Willey. [Google Scholar]
- Bergström, Malin. 2011. Continuous support in labour has beneficial effects for mother and baby. BMJ Evidence-Based Medicine 16: 182–83. [Google Scholar] [CrossRef] [PubMed]
- Bohren, Meghan A., Gustav Justus Hofmeyr, Carol Sakala, Rieko K. Fukuzawa, and Anna Cuthbert. 2017. Continuous support for women during childbirth. Cochrane Database Systematic Review 7: CD003766. [Google Scholar] [CrossRef] [PubMed]
- Conrad, Peter. 2007. The Medicalization of Society: On the Transformation of Human Conditions into Treatable Disorders. Baltimore: Johns Hopkins University Press. [Google Scholar]
- Davis-Floyd, Robbie. 2001. The technocratic, humanistic, and holistic paradigms of childbirth. International Journal of Gynaecology and Obstetrics 75: S5–S23. [Google Scholar] [CrossRef] [PubMed]
- Denzin, Norman. 1978. The Research Act: A Theoretical Introduction to Sociological Methods. New York: Mc Graw-Hill. [Google Scholar]
- Euro-Peristat Project. 2013. European Perinatal Health Report. Health and Care of Pregnant Women and Babies in Europe in 2010. Paris: INSERM. [Google Scholar]
- Euro-Peristat Project. 2018. European Perinatal Health Report. Core Indicators of the Health and Care of Pregnant Women and Babies in Europe in 2015. Paris: INSERM. [Google Scholar]
- Fedele, Anna. 2015. Spiritual Mothering. In Portugal: Some Initial Reflections from an Anthropological Perspective. ISSRC Working Paper. Lausane: UNIL. [Google Scholar]
- Hodnett, Edward, Shawn Gates, Carol Sakala, and Gustav Justus Hofmeyr. 2013. Continuous support for women during childbirth. Cochrane Database of Systematic Reviews 7: CD003766. [Google Scholar] [PubMed]
- Iravani, Mina, Elahe Zarean, Mohsen Janghorbani, and Masod Bahrami. 2015. Women’s needs and expectations during normal labor and delivery. International Journal of Health Promotion and Education 4: 31–37. [Google Scholar]
- McCourt, Christine, and Fiona Dykes. 2010. From Tradition to Modernity: Time and Childbirth in Historical Perspective. In Childbirth, Midwifery and Concepts of Time. Edited by Christine McCourt. New York: Berghahn Books. [Google Scholar]
- Millward, Peter, and Shaminder Takhar. 2019. Social Movements, Collective Action and Activism. Socioilogy 53: 1–12. [Google Scholar] [CrossRef]
- Neves, Dulce Morgado, and Catarina Barata. 2023. Direitos, resistências e mudanças nos cuidados perinatais durante a pandemia por COVID-19 em Portugal: O papel e a ação da Associação Portuguesa pelos Direitos da Mulher na Gravidez e Parto. Miscellanea 19: 48–53. [Google Scholar]
- Oakley, Ann. 2016. The sociology of childbirth: An autobiographical journey through four decades of research. Sociology of Health & Illness 38: 689–705. [Google Scholar]
- Odent, Michel. 2015. Do We Need Midwives? London: Pinter & Martin. [Google Scholar]
- Perined. 2021. Perinatale zorg in Nederland anno 2020—Duiding door landelijke perinatale audit en registratie. Utrecht: Perined. [Google Scholar]
- Pintassilgo, Sónia, and Helena Carvalho. 2017. Trends and consequences of the technocratic paradigm of childbirth in Portugal: A population-based analysis of birth conditions and social characteristics of parents. Sexual and Reproductive Healthcare 13: 58–67. [Google Scholar] [CrossRef] [PubMed]
- Ramos, Leiva. 2023. Michel Odent—‘Esquecemos completamente quais são as necessidades básicas da mulher em trabalho de parto’. Miscellanea 19: 25–31. [Google Scholar]
- Santos, Mário J. D. S., and Dulce Morgado Neves. 2021. A Manifest against the Homogenisation of Childbirth Experiences: Preserving Subjectiveness in a Large Dataset of the «Babies Born Better» Survey. Social Sciences 10: 388. [Google Scholar] [CrossRef]
- Smith, Valerie. 2014. Salutogenically focused outcomes in systematic reviews of intrapartum interventions: A systematic review of systematic reviews. Midwifery 30: 151–56. [Google Scholar] [CrossRef] [PubMed]
- Todres, Les, Kathleen T. Galvin, and Immy Holloway. 2009. The humanization of healthcare: A value framework for qualitative research. International Journal of Qualitative Studies on Health and Well-Being 4: 68–77. [Google Scholar] [CrossRef]
- Wang, Haidong, Chelsea A. Liddell, Matthew M. Coates, Meghan D. Mooney, Carly E. Levitz, Austin E. Schumacher, Henry Apfel, Marissa Iannarone, Bryan Phillips, Katherine T. Lofgren, and et al. 2014. Global, regional, and national levels of neonatal, infant, and under-5 mortality during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 384: 957–79. [Google Scholar] [CrossRef] [PubMed]
- White, Joanna, and Maria Johanna Schouten, eds. 2014. Normal Birth: Experiences from Portugal and Beyond. Braga: CICS. Lisbon: CRIA. [Google Scholar]
- World Health Organization (WHO). 2014. The Prevention and Elimination of Disrespect and Abuse during Facility-Based Childbirth: WHO Statement. Geneva: WHO. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).