1. Introduction
Immigrant women are subject to high levels of stress due to economic, social, adaptation, and discrimination difficulties; their health and mood are characterized by suffering, limited social relations, low socioeconomic status, lack of family support, lack of community integration, abuse by their employers, and difficulties in accessing housing and justice and health institutions in the host countries (
Collazos Sánchez et al. 2014). They frequently have a greater responsibility to look after their families and may complete long hours of work, have greater difficulties related to social integration, and have difficulties with social integration. They may face discrimination, experience difficulties with economic integration, and deal with the stresses of migration and resettlement.
Ruzzante et al. (
2009), in research carried out in Spain, compared the levels of daily stress and depression in groups of immigrant and non-immigrant women and observed a higher prevalence in immigrant women;
Davison et al. (
2019) observed the highest prevalence of depression in immigrant women in Canada and
Olukotun et al. (
2019) and
Santillanes-Allende (
2017) in the United States for groups of African migrant women and Mexican migrant women.
Studies conducted in Spain between 1982 and 2012 have shown mental health problems, specifically those related to anxiety and depression problems, among the immigrant population to a greater extent than among the non-immigrant population, relating to a very high incidence of stress in the case of immigrants (
Campbell et al. 2015). We must bear in mind that this type of vulnerable population is poorly represented in research addressing technology, mobile communication, and health (
García and Alda 2005).
Text message therapy has been applied to a variety of pathologies, such as depression, anxiety, stress, addiction, etc. (
Aguilera 2015;
Aguilera et al. 2015;
Campbell et al. 2015;
Hall et al. 2015;
Kong et al. 2014;
Proudfoot et al. 2013;
Stevens et al. 2019). In general, text messages contribute to the effectiveness of face-to-face therapy, improve attention, and allow users to be advised more intensely and frequently by avoiding face-to-face consultations with a therapist. However, these studies did not differentiate therapies by degree of depression, the specific text messages used for men and women, or for highly vulnerable people, such as immigrant women.
Aguilera et al. (
2017) highlighted the need to investigate the impact of text message therapies on vulnerable social groups, such as immigrant women.
This article is part of the research area on therapies using mobile communication systems among vulnerable women’s groups in Spain. We applied psychosocial therapies with text messages to immigrant women in an intervention group and compared the results to the control group. This study was published in
García et al. (
2019), where we demonstrated the effectiveness of text message therapy when combined with face-to-face therapy sessions. In this article, we analyze the effectiveness of text message therapies among immigrant women according to their degree of depression at the beginning of the study. We followed the methodology for the design of a quasi-experimental investigation (
Handley et al. 2018). We proceeded to measure the mood and symptoms of depression at the beginning and end of the message delivery period and identified significant changes in the effectiveness of text message therapy in the four subgroups classified according to their depressive intensity.
2. Method
Each participating immigrant woman was a resident in the urban area of the city of Santiago de Compostela in Galicia, Spain, and all of them had a personal mobile phone and sufficient knowledge to communicate orally and with messages written in Spanish, Galician, or Portuguese.
We requested the collaboration of the social services offices of the regional and local government to identify cases of immigrant women with social exclusion problems. We were able to identify 46 women who had requested help or social support and proceeded to contact all of them personally. There was no intermediation or contact from the social services offices.
We interviewed all women face to face by establishing a telephone contact and making an appointment in an accessible place for them. In the interview, we explained to each one personally what we wanted to do. Only in one case there was rejection. All participants (n = 45) gave us their informed consent by signing a specific document.
We made a psychological and social diagnosis of each woman through the information collected with questions about concerns, health, eating habits, sleep, moods, medical treatments, social and family relationships, professional activities, economics, and physical activity. In general, the interview took place for about 30 min in each case. We also had access to psychosocial information from official records. All this previous identification and diagnosis work took us 2 months.
In the personal interviews, we conducted an evaluation of each participant’s mood and possible depression. In this way, the group was reduced to 44 cases, since in one case, we were able to verify that the personal health status measured with (Personal Health Questionnaire) PHQ−9 was optimal and could be ruled out.
We combined face-to-face and remote psychosocial therapy with text messages to the personal mobile phone and timely telephone calls. The therapeutic attention period with the messages was 26 days. We had telephone contact with each woman at the beginning of the investigation, after 15 days, and at the end. In general terms, phone calls were about 5 min per call, and we made 3 calls to each woman.
All the women participants knew that they were totally free to answer our messages if they wanted to, but that we would not answer them directly.
We informed all of them that we would give them advice to improve their physical, mental, and social health, and we told them that the reception and response of the messages were totally free for them. The expenses of the answers were paid to them at the end of the study according to the price of SMS in Spain. In 36 cases out of 44, they decided to donate the message response costs to the project in order to contribute to its continuity.
The SMS sending system allowed us to ensure that all women received messages without having an Internet connection. Among the women, phones with prepaid cards predominated and there were difficulties in connecting to the Internet permanently (n = 34).
Each woman received 4 text messages daily on her personal mobile phone, at 9:00 a.m., 1:00 p.m., 5:00 p.m. and 9:00 p.m. We used the remote system for sending and receiving messages used in previous research (
García et al. 2017) called HealthySMS, which was developed by the University of California at Berkeley.
It was necessary to write the specific content of the messages according to the general psychosocial characteristics of the participating women. These messages were grouped in message banks focused on (a) strengthening of positive thinking, (b) capacity for reflection, (c) improvement of health, (d) promotion of physical activity, (e) capacity for planning and organization of tasks, and (f) improvement of social relations.
The messages were brief and direct of the following type: “Have you identified any negative thoughts today? You must set it aside and think positively”; “Plan a pleasant activity with a person with whom you feel comfortable”; “Think and identify positive people who make you feel good”; “Organize your schedules always reserving a leisure time for you”; “What are you going to do this week to take care of your health?”.
All women received 104 text messages in total. In general, we formulated specific questions, advice, and guidance on daily habits, in order to change negative behaviors for positive and healthy ones.
In order to prevent possible aggressive episodes of self-harm or tendencies towards suicide, we use a keyword identification system in the answers. Fortunately, there were no incidents, so it was not necessary to alert the urgent care services.
3. Measures
In order to obtain a statistical indicator that allowed us to compare changes and evolution in mood and depressive symptoms, we decided to use the personal health questionnaire validated by
Kroenke et al. (
2001) and called PHQ–9, which allows us to identify cases of mild depression with scores of less than 5 units, cases of moderate depression with scores between 5 and 15 units, and cases of severe depression with scores greater than 15 units.
Secondly, we decided to use the final questionnaire that measures the degree of satisfaction with text messages (FQTM), which is an instrument validated by
Aguilera et al. (
2017). With this FQTM questionnaire, we asked the women participants at the end of the therapy about the positive and negative aspects identified in the messages, about their effectiveness, about their opinion about the number of messages received, about the changes experienced in their daily lives, and about their interest in continuing to receive messages. We also used it as an indicator of the number of messages answered and the personal adherence to the medications prescribed by the doctor.
We used a paired sample t-test and a Wilcoxon signed rank test as a nonparametric test to compare the average range of the two related samples.
4. Participants
The set of case studies consisted of immigrant women, with an average of 9.9 years of residence in Galicia, Spain, who were applicants for public assistance in the social services offices of the local public administration (100%), had an average age of 39.8 years (SD = 10.71, range = 19–65), and had 2.1 children (SD = 1.32, range: 0–6). They were a heterogeneous social group, with cases of prostitution (
n = 2) and gender violence (36.4%,
n = 16). The participants were from 12 different nationalities, especially from Latin America—Dominican Republic, Brazil, Colombia, and Venezuela—and to a lesser extent from Portugal, Italy, Romania, Hungary, Russia, and Morocco. We identified cases with mental problems (27.3%,
n = 12). These women resided mostly in urban environments (56.8%,
n = 25). A basic level of education predominated, with 56.8% (
n = 25) at the primary level, 27.3% (
n = 12) at the secondary level, and 6.8% (
n = 3) had university/higher education. Only 9.1% (
n = 4) had no studies. The cohort included divorced or separated women (45.4%,
n = 20), 31.8% (
n = 14) single women, and 31.8% (
n = 14) married women (see
Table 1).
Almost all the women (84.1%, n = 37) were engaged in low-skilled, informal, and legally unlawful activities, mainly in elderly or disabled care services, cleaning services, hospitality services, or retail trade. They were women without a legal residence permit in Spain, who had serious problems accessing legal jobs and obtaining the legal equivalence of educational degrees obtained in their countries. There were cases that had difficulty bringing their children to Spain from their countries of origin (n = 4), and some women were recognized by the Spanish authorities as political exiles (n = 3). Notably, almost all of the women had social relationship problems and suffered community isolation outside of their family circle (81.8%, n = 36).
On the other hand, we must emphasize that in general, the participating women showed a high adherence to the medication recommended by their doctors. We were able to verify a high prevalence regarding the number of women taking medications in the last month: 82.9% (n = 34) compared to the total number of women who responded (n = 41); 17.1% (n = 7) did not take the medication and 6.8% did not respond (n = 3 of n = 44). Regarding the observation of the frequency of taking medications following the instructions of their doctors, we observed that this was very high since 85.3% of all women answered that they always took their medications. However, when asked how many times they forgot to take the medication, 61.8% said never, 14.7% once, and 23.5% twice or more.
Regarding ethical considerations, the entire procedure was approved by the biology and research protection committees with human subjects of the University of California-Berkeley and the University of Santiago de Compostela.
5. Results
The participation was very high. To a greater or lesser extent, all women (n = 44) answered several messages or adequately answered personal phone calls; in only 4 cases, they only answered phone calls (9.1%), and in the remaining 40 cases they responded with messages and also answered phone calls (81.8%). Each participating woman answered an average of 26.4 messages (SD = 32.64, range = 1–197, IQR was 30 (34-4)). We next asked those who never answered the messages (n = 4). These participants noted that they had not answered the messages due to feelings of insecurity, because they did not know what to say, because they found themselves with a very high workload, because they were taking care of their families, or because they doubted when they could recover the cost of the responses that we had previously agreed to pay them. We also detected 14 cases (35.0%) that said they did not answer everything they would have liked for having an insufficient balance on the prepaid cards of their mobile phones and the exhaustion of available credit for several days.
Regarding the evaluation of experience with therapy, we must bear in mind that most of the women commented that the text messages made them feel more secure and identified with the local community in their environment; women who said they agreed were 65.9% of all participants (
n = 29). Furthermore, 86.3% (
n = 38) of the women stated that they agreed that the messages had helped them improve their mood and 86.6% commented that they would like to continue receiving more messages (
n = 39) with a frequency and intensity of 4 or more daily messages (84.1%,
n = 37). As we can see in
Table 2, the general evaluation of the therapy received through text messages was very positive. However, we also verified that immigrant women need specific therapies to boost and improve their social relationships outside the family environment; 34.1% (
n = 15) responded that message therapy had not been useful in this regard.
The response rate to the messages received was 25.4% (SD = 31.4%, with a range of 1.0%–189.4%). It was interesting to note that 36 women (81.2%, n = 44) claimed to keep the texts received to re-read them in the future and have them as references for needing new emotional support or advice.
The observation of the correlation between age and the number of messages answered was negative; we found that older women responded fewer times (r = −0.38), which may be related to less training than young women for the use of writing functions on the mobile phone.
Moreover, the final questionnaire to evaluate the experience they had with text messages (FQTM) highlights the fact that all women responded positively (100%,
n = 44). We directly asked all the participating women to note if the messages had helped them in any way, what they liked best about the therapy received, and how they believed that we could improve this therapy to improve the health of other women with similar problems. The responses received were grouped on a scale of increasingly general concepts based on the open coding method of grounded theory (
Chamaz 2006). By applying this method, we developed an inductive classification process that allowed us to associate and synthesize all the response messages into four main thematic categories: (a) thinking, with comments on how their mood had improved, how the therapy made them feel more safe or relaxed, and how it increased their concentration or reflection; (b) organization, with reference to planning and forecasting daily life, changing habits and attitudes, increased motivation, or achieving small goals by themselves; (c) monitoring, with reference to feeling supported, accompanied, and advised, including improvement in familial and social relationships; and (d) healthy habits, including improving their diet, overcoming depression, reducing anxiety, remembering to take medication, exercising, or taking better care of themselves.
The answers regarding what they would improve and what they least liked, underline that in five cases, some of the messages were considered repetitive (11.4%, n = 44), in three cases, they responded that it was necessary to have more time to think and to be able to respond (6.8%, n = 44), in two cases, they stated that they preferred more personal therapy and less in one group (4.5%, n = 44), in two cases, they responded that they would like to receive more face-to-face care (4.5%, n = 44) and one woman said that she would have liked to receive more tips and reminders of healthy habits to change your bad diet. Finally, we must value the fact that in no case were there any mentions of having had problems regarding the daily hours of reception or the content of the messages.
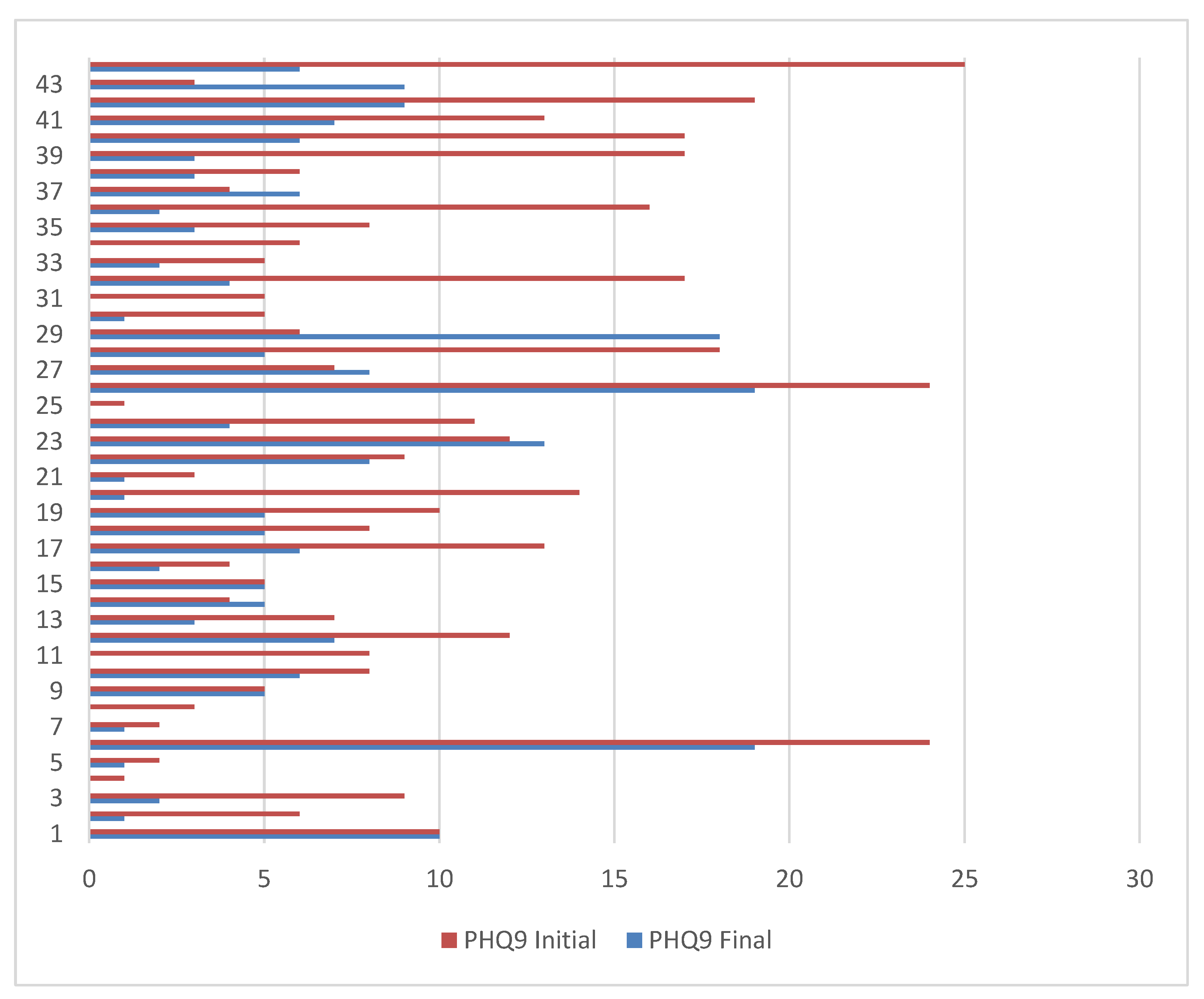
At the end of the therapy period, we gave the PHQ–9 questionnaire to all women again, which made it possible to compare their results with the initial ones. Note that for the group of all women participants (
n = 44), the evolution was positive—the results went from the initial score of 9.4 (SD = 6.4, range 1–25) to 5.0 at the end of the message therapy period (SD = 4.8), with a significant difference in the paired sample
t-test: t (44) = 2.01;
p = 7.80. In 39 of the cases (88.6%), the PHQ–9 decreased and in five cases (11.4%), it increased (see
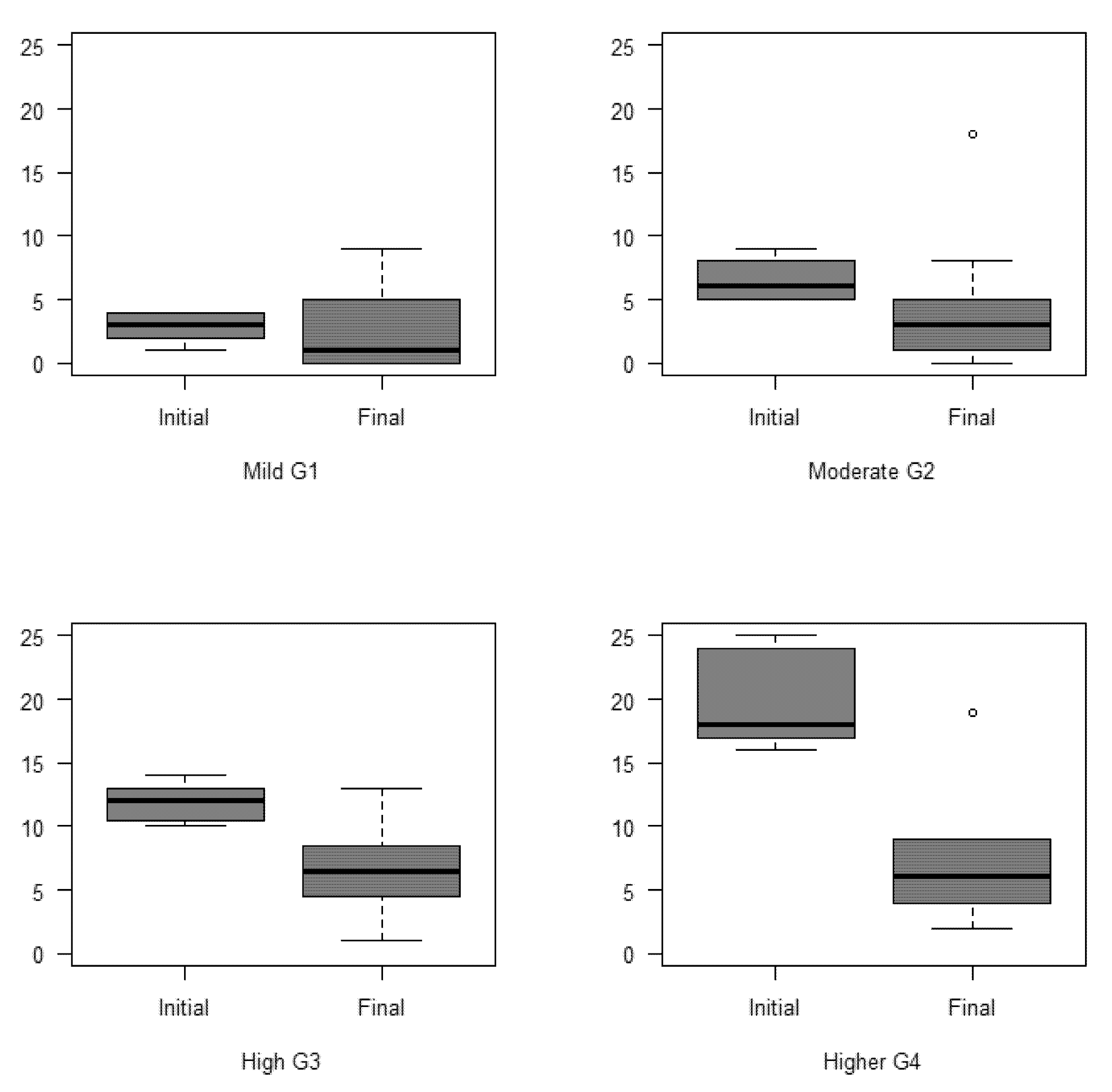
Figure 1). Secondly, we distinguished between four groups with different degrees of depression: Mild G1 (PHQ−9 < 5,
n = 10); Moderate G2 (PHQ−9 ≥ 5 and <10,
n = 17); Moderate High G3 (PHQ−9 ≥ 10 and < 15,
n = 8); Higher G4 (PHQ−9 ≥ 15,
n = 9), and in all of them, the final results after therapy show an improvement in the personal health of women (
Figure 2); however, the differences between the initial and final PHQ−9 are significant in all groups except in the G1 of Mild Depression, according to the paired simple
t test and the Wilcoxon test (
Table 3).
The Wilcoxon signed ranges test is a non-parametric test to compare the average range of two related samples and to determine if there are differences between them. We have used it as an alternative to the Student’s t test when the normality of these samples cannot be assumed.
In order to apply the paired simple t test, the data must be normal in each group which we wanted to contrast—for example, if in G1 we observe normality of initial PHQ−9 and final PHQ−9. If there was normality, we applied the paired simple t test, but the non-parametric alternative test we applied was the Wilcoxon test.
We applied the normality tests and we obtained the following results
Table 4):
6. Discussion
We agree with
Agyapong et al. (
2016,
2017) that text message therapy allows geographical and social gaps to be overcome by providing psychological treatment to patients residing in rural or socially vulnerable spaces, as well as in the possibilities these therapies offer for implementation in mental health programs.
The research that we carried out in Spain shows the viability and effectiveness of therapies using text messages for groups of immigrant women who use social services and have depression problems. We agree with
Aguilera et al. (
2017) in the need to investigate the impact of text message therapies on vulnerable social groups of different categories (sex, age, culture, educational level, etc.).
Text message therapy to personal mobile phones is effective with immigrant women who demand social assistance from the public administration. The differences between the initial and final PHQ−9 are significant in all groups except in the group of mild depression; the symptoms of depression and women’s mood improved significantly with text message psychotherapy when the initial depression was medium or high grade.
Therefore, we interpret that the effectiveness of text messages is greater in women with significant moods and depression—that is, those that significantly affect relationships with other people, eating habits, sleep quality, physical activity, cognitive thinking, and personal health. We have verified that immigrant women suffer from social isolation and that personal attention with text messages to their mobile phones is very well accepted. However, we still need to know if the messages on the mobile phone contribute to reducing the taking of antidepressant and anxiolytic medications, which should be treated in a new investigation.
The system of management and programmed delivery of text messages that we have designed can become a tool for psychotherapeutic intervention to treat groups of vulnerable people who remain outside the public health and social integration programs. We can think of isolated rural populations, people at risk of social exclusion due to poverty, drug addiction, homelessness, ethnic minorities, etc., who do not access social or health services or require daily psychotherapeutic attention.
We did not detect problems with the reception of SMS on women’s phones. The SMS does not depend on the Internet connection and has no cost to the receiver. However, the problems arose with the SMS responses because, not being free, women showed reluctance in the fear of depleting the balance of their prepaid phone cards. Their economic vulnerability forces immigrant women to depend on free Wi-Fi connections in order to access the Internet, which limits the frequency and time schedule for sending messages from the remote system.
We wrote text messages with advice, guidance, and key questions to motivate reflection based on personal data obtained from face-to-face interviews with each of the women. It was possible to group and link recipients and messages by the degree of depression and mood of the recipient, in order to guide positive changes in the behavior of the recipients.
In our quasi-experimental study, we obtained positive results, but the group of participating women was not homogeneous in terms of age, country of origin, education, or marital status.
We must continue with new research to design specialized text message banks according to cultural, social, economic, and demographic diversity. It is necessary to extend the periods of reception of messages to more than 26 days and to evaluate changes and evolution of moods and the symptoms of depression, as well as introducing combinations with face-to-face group therapies in a timely manner and telephone attention. We did not include a control group and did not find significant statistical correlations between the effectiveness of the therapy with text messages and social variables, such as marital status, urban-rural origin, nationality, etc. The small sample size of the study participants did not allow for this comparison.
7. Conclusions
Psychosocial therapy with text messages to personal mobile phones combined with telephone attention is effective; it allows the counselling, monitoring, and guiding of positive behaviors in situations of depressive mood. Initial face-to-face contact with the therapist is necessary to assess the physical, mental, and social health status of the people undergoing intervention. With this, it is possible to identify the negative psychosocial behaviors in the recipients and define and write specific message banks with content-oriented to change towards positive behaviors.
Automatic message delivery systems allow the therapist to schedule specific days, hours, and periods of time to send messages to each individual case or in groups; the system allows the monitoring of the changes experienced in the recipient from the reading and observation of the response messages and allows the design of specific surveys and questions on psychotherapeutic issues such as medication adherence or the evaluation of moods or symptoms of anxiety or depression.
This type of therapy allows vulnerable social groups, such as immigrant women, to receive specialized care without having to physically move to receive face-to-face therapies. It is, therefore, flexible and economical and allows personalized attention. We are not aware of official public health or social services programs in Spain or internationally that offer this type of text message therapy to vulnerable women. We believe that such therapies using mobile phones are applicable in both urban and rural settings and that social work and health service professionals could use this type of therapy.







{kind=link}
{kind=link}