1. Introduction
According to the World Malaria Report 2020, India contributed to the largest reductions in malaria cases in South East (SE) Asia from ~20 million cases in 2000 to ~5.6 million in 2019. However, it still accounted for 86% of all malaria deaths of the SE Asia region [
1].
India is aiming for malaria elimination by 2030, and a National Strategic Plan (NSP) has been taken up accordingly. According to the National Strategic Plan (NSP 2017-22), districts of India have been stratified into four distinct categories in terms of transmission intensity, which is measured by the annual parasite incidence (API). Category III Districts, the high transmission areas with API > 2, are in an intensified control stage and need concerted efforts to bring down the disease burden [
2]. Many of the districts of NE states in India, such as Tripura, Meghalaya, and Mizoram, are in Category III. A few pockets inside such districts could be regarded as extreme areas, having disproportionately high API values (>10), with hilly forested tribal dominated regions largely contributing to malaria. Mass screening is considered as one of the strategies by the National Vector Borne Disease Control Program (NVBDCP) surveillance to reduce the vast transmission reservoir. Accordingly, several cross-sectional mass surveys were conducted in malaria-endemic regions of NE India in the last two years. The hilly, forested, and tribal-dominated areas of NE India continue to be malaria-infested and are prone to outbreaks. Tripura is one such state where a major outbreak occurred in 2014, affecting >50,000 people and causing ~70 deaths, most of whom were children [
3] and again one in 2018. Several endemic villages of Tripura were selected by national and state malaria programs for the cross-sectional surveys during 2019–2020. This year (2021), several such surveys were planned; these included one in the dry post-winter season, February to March 2021.
Studies have shown that in the dry season, when the clinical incidence of malaria is generally low, malaria cases are found with low parasitemia and are asymptomatic. As clinical malaria is seasonal and mainly in the rainy season, subclinical
P. falciparum infections persist throughout the dry season, playing the role of the reservoir infections for the transmission season, which would be several months later [
4,
5,
6].
Host survival during the dry months is considered essential to resume
P. falciparum transmission in the subsequent rainy season. The parasite has been thought to have evolved strategies for preventing potentially fatal host pathology. It ensures persistence during periods when there are few or no mosquito vectors [
7]. In Sudan, it has been demonstrated that low-density asymptomatic infections perpetuate transmission over the dry season [
4].
Additionally, parasite reservoirs are thought to be associated with low-density asymptomatic infections. There is a clear evolutionary advantage to the parasite for sustaining it, since asymptomatic individuals do not seek treatment and represent a parasite reservoir from which malaria vectors can become infected [
8,
9]. In some studies, these reservoirs of asymptomatic cases, as found by the maps of PCR-detected
P. vivax infections by households, are fewer and more tightly clustered during the dry season, while they expand during the wet season with the expansion of the breeding ground [
10]. Another study found clusters of
P. vivax infections in the dry season, where only one symptomatic case of malaria was found by Rapid Diagnostic Test (RDT), indicating that the observed clusters are almost exclusively composed of asymptomatic carriers. It was also shown that groups of homesteads consisting of asymptomatic carriers could act as stable clusters for several years. These asymptomatic, potentially long-term infections might be sufficient for sustaining malaria transmission and therefore can be targeted for malaria control and elimination [
11]. Hence, finding the asymptomatic, submicroscopic cases in the dry season can be potential targets for cutting the transmission chain. A study in Bangladesh showed that malaria prevalence in the winter survey (dry season) was not significantly lower than that in the summer survey where both
P. falciparum and
P. vivax were found, and most cases were asymptomatic [
12].
With this background, this study was planned to assess the burden of malaria infections and whether asymptomatic and submicroscopic malaria cases are present in dry post-winter months in malaria-endemic pockets of Dhalai district in Tripura. Dhansinghpara and Bidyapara villages, under the Gurudhanpara sub-center (SC), were amongst the highly malaria-endemic pockets in Dhalai and chosen by the National and State Malaria Programs for mass survey in February 2021–March 2021. The detection method used in the survey was RDT. Considering that RDT might miss asymptomatic submicroscopic cases, mostly with low parasitemia, this study was planned to use more sensitive nested PCR. A subset of samples was also screened by microscopy.
3. Discussion
The present study found a staggeringly large number of malaria cases and a high proportion of
P. vivax along with
P. vivax and
P. falciparum mixed cases among them. These were not detected by RDT during the mass surveillance from febrile and afebrile people in dry winter and spring months in two malaria-endemic villages of Dhalai District. While many cases are reported yearly in the study area, cases are very high during monsoon and post-monsoon times. A few cases are found in routine active and passive surveillance from January to March. Analysis of data of Ambassa PHC under which the study villages fall shows 2–5% of yearly cases in January to March, as evident from the data of 2018–2021 (
Supplementary Table S1a). Yearly case data for 2019 and 2020 include mass surveillance data from the program conducted in monsoon and post-monsoon seasons. Similar analysis of yearly and monthly malaria case data for the study villages Bidyapara and Dhansinghpara showed 5–10% of annual cases during January to March (
Supplementary Table S1b). Very few (six) malaria cases were reported during February and March 2021 from these two villages, even when the malaria program undertook mass screening using RDT. Ambassa PHC cases, as reported by the program, also showed a similar ratio of cases during January–March.
In contrast, this study showed a considerable number of cases with a very high prevalence of ~48%, especially of P. vivax and mixed infections during this dry period, which totally remains undetected by routine active and passive surveillance and even by mass surveillance if only RDT is used. There are even cases beyond microscopic detection. While these submicroscopic cases are most likely low-density ones (<50 parasites/µL), and the majority of the cases detected by microscopy were found to have <100 parasites/µL, there were a few microscopically detected cases with a higher density, such as 600–720 parasites/µL, yet they were undetected by RDT for both parasite species. In the case of P. falciparum, these cases might have HRP II/III gene deletion, which is worthy of future exploration. In the case of P. vivax, this might indicate a lower sensitivity of RDT kits in field samples of this area, which again needs to be investigated in future. Furthermore, while the majority of these cases were asymptomatic, some of them were symptomatic as well, which were submicroscopic.
Interestingly, most
P. vivax and mixed infections found in this study were asymptomatic in all the age groups, i.e., in below 15 years and more than 15 years groups. While there was no significant association of the symptomatic infections with the age group, the proportion was higher in the <5 age group (
Table 2)
Unusually high P. vivax cases were detected from a subset of the samples analyzed for malaria. Although the sample size was not very big, we covered a considerable portion of the population (we covered 373 people by RDT, which is >55% of the population of 679 of these two villages who were considered for mass survey) in the survey in an unbiased manner. The survey was attempted to include all the people who were available and willing to give blood, irrespective of their febrile status.
This study thus warrants the use of molecular techniques in the mass survey for detecting parasite positives, especially P. vivax, and the importance of screening in the dry season, which can assist in determining the course for control and elimination of malaria. Previously, a study conducted during winter in Tripura after the epidemic had shown a high prevalence of low-density asymptomatic cases (unpublished data).
Although the infectivity of the asymptomatic and submicroscopic cases was not tested in this study, several reports [
8,
9,
10] have shown the infectivity of asymptomatic low-density infection of both the parasite species. Especially the study in Thailand, which showed the presence of a low-density infectious reservoir of
P. vivax as clusters, raises the possibility of these infections serving as the infectious reservoir. More direct proof of transmission in cold, dry months comes from our finding on the presence of parasites in
A. minimus in January. Although traditionally it has been thought that temperatures below 18 °C would not be conducive to parasite development in the vectors, recent studies are challenging this notion. Waite et al. (2019) [
13] showed the feasibility of schizogony, though a prolonged one up to 16 °C. As their research involves laboratory-adapted mosquito and parasite strains, they have stressed the need for a more detailed assessment of other parasite strains and species of malaria parasites from the field and exploring studies with local mosquito–parasite pairings. These studies would be worthwhile to assess the extent of malaria transmission in low temperatures. There have been reports of mosquitoes having transmission in an amicable environment like indoor or other places, which would not be that cold in the cold months. It is very much possible that the vectors find local microenvironments where the temperature is not low in the cold months, and thus, they sustain the infection in the dry cold seasons.
There have been reports of some mass surveillance studies from other parts of India. One study [
14] in Chennai (Tamil Nadu), Nadiad (Gujarat), and Rourkela (Odisha), during 2012–2015, where the study period included dry winter and post-winter seasons as well, showed asymptomatic infections ranging from 21% in Gujarat and 64% in Rourkela to 71% in Chennai, and different proportions of parasite species found in different study sites among asymptomatic, submicroscopic carriers, and age groups but very few mixed infections. A survey conducted in Chhattisgarh in 2016 during the low transmission season detected ~35% submicroscopic and ~77% afebrile malaria cases. The sensitivities of RDT, microscopy, and PCR were 53.3, 47.5, and 87.4%, respectively, showing that a significant number of infections can be missed during routine testing by RDT and microscopy [
15]. Another study in Balaghat, Madhya Pradesh, showed the relevance of afebrile parasitemia due to both
P. falciparum and
P. vivax [
16]. A survey in June 2012 from Purulia district of West Bengal on asymptomatic and submicroscopic infections detected only ~1% submicroscopic infections in 963 participants while detecting five infections of
P. falciparum and none of
P. vivax, which were not seen by RDT [
17]. A cross-sectional survey conducted during May–June 2017 in the Kandhamal district of Odisha reported [
18] that of ~30% randomly selected samples analyzed using real-time PCR, the following species-specific prevalence by qPCR among asymptomatic positive cases was found: 57%
P. falciparum, 29%
P. vivax, and 14%
P. falciparum +
P. vivax.
However, there have been few such studies in NE India, which has multiple malaria-endemic pockets. A previous study in 2014 in dry winter months (January–February) in the Missamari area of Assam, situated in northeast India, found no positive cases by RDT, microscopy, or PCR [
19]. Although a similar PCR method was used in that study, it may be mentioned that dry blood spots were used in that study while whole blood was used in this study.
This study found a considerably higher positivity rate in RDT negative samples than all other studies reported in India. Among them, the proportion of P. vivax and mixed infections was also much higher, and that too in the dry post-winter month, which is not typical malaria season.
The NE states were shown to be co-endemic for
P. falciparum and
P. vivax species. High proportions of
P. vivax cases (60–80%) were seen in Arunachal Pradesh and Nagaland in the north with the alpine environment, 42–67% in Manipur, whereas in Assam, they varied from 23 to 31% with a subtropical and tropical climate. On the other hand, Tripura, with a warm and humid tropical climate and large stretches of tropical evergreen, semi-evergreen and moist deciduous forest and Meghalaya and Mizoram, had the lowest proportion of
P. vivax cases [
20].
In Tripura,
P. falciparum has been consistently the dominating species as per the clinical cases reported by the national malaria program [
21]. Traditionally,
P. vivax malaria cases have been reported as very low by NVBDCP for the whole of Tripura, where the results are primarily RDT-based and only to some extent on microscopic examination while being performed exclusively on the symptomatic febrile cases. The same can be seen from the data from 2008 to 2019 (
Supplementary Table S2), where less than 10% of the total malaria cases (ranging from 3.1 to 9.5%) of
P. vivax were detected. However, for the first time, this study reports the presence of a substantial asymptomatic and submicroscopic burden of
P. vivax infections singly or mixed with
P. falciparum in NE India. This study shows the importance of conducting similar cross-sectional surveillance studies using molecular methods in other areas of NE India to determine the real burden of
P. falciparum and
P. vivax cases.
Once regarded as a relatively benign disease,
P. vivax malaria is now acknowledged as a significant public health concern leading to life-threatening complications, miscarriage, chronic infection, and increased mortality. A growing list of evidence challenges the previously-existing notion of
P. vivax being benign [
22,
23,
24]. Additionally,
P. vivax poses specific difficulties to elimination, mainly due to its ability to relapse weeks to months after the initial infection. It is responsible for a significant burden of malaria worldwide, accounting for half of all the cases in Asia and Latin America [
25]. According to the 2019 World Malaria Report, of the total global
P. vivax burden, 53% is in the WHO South-East Asia Region, and India alone accounts for 47% of this burden [
26].
P. vivax is known to cause lower parasite densities than
P. falciparum. In many cases beyond the limit of RDT detection or even microscopic detection leading to high rates of false-negative
P. vivax symptomatic cases [
27,
28]. In Columbia, ~56% of the asymptomatic
P. vivax carriers were infective to
A. albimanus mosquitoes [
29]. Another study involving asymptomatic volunteers from Thailand using
P. vivax and
A. dirus mosquitoes showed 13% samples were infective [
8]. In both these studies, low-density asymptomatic
P. vivax was infective, thus establishing their role in the transmission.
There is a possibility that some of the
P. vivax cases detected in this study are relapse cases, as the transmission may not be high during this period, which is evident from the
Anopheles density found in the entomological surveillance. This can be indicative of the absence or incomplete treatment of primaquine. As all the
P. vivax infections, symptomatic or asymptomatic if left untreated, go undetected in routine surveillance programs where RDT/microscopy is used, it is quite probable that a large proportion of
P. vivax remains as hypnozoites in the liver, which can later relapse. These hypnozoites can become spontaneously activated and induce asymptomatic periodical infection or clinical episodes [
30]. It has been shown that dormant
P. vivax hypnozoites can activate at variable periodicity depending on geographical region [
31], which means that untreated sub-microscopic infections can continue to relapse in the future. In addition, these parasites can cause multiple clinical attacks over the months (up to approximately two years) following a single infectious bite by the
Anopheles vector species. This can potentially carry on the transmission with each relapse.
Hence, the determination of accurate
P. vivax burden, including the low-density asymptomatic burden, is important from the malaria control and elimination point of view in the known
P. falciparum endemic areas as well. However, most research and published literature on malaria still focuses on
P. falciparum and much less on
P. vivax [
22]. So far, the data on the
P. vivax sub-microscopic burden is limited in India, with almost no available data from NE India.
P. falciparum malaria has receded in many regions in Asia and South America. In contrast,
P. vivax malaria has remained a harder challenge as it responds much more slowly to the established control methods that have driven
P. falciparum to near elimination in those areas [
32]. In India, a similar trend can be found upon analysis of the incidence of
P. falciparum and
P. vivax for the past few years (
Supplementary Figure S1). It shows that although the overall malaria clinical burden has been dropping over the last decade, it is mainly the burden of
P. falciparum that is decreasing while
P. vivax is not. This can very well be the situation of states like Tripura. This might be attributed to the non-detection of low to moderate density
P. vivax malaria in traditionally known
P. falciparum areas and incomplete treatment of
P. vivax cases, leading to relapses and a considerable burden of low-density asymptomatic infections.
Malaria elimination efforts are being ramped up in India and worldwide to eliminate the disease by 2030. From this perspective, the findings of this study are significant, which showed a very high hidden burden of
P. vivax and mixed cases, most of which are sub-microscopic and asymptomatic in
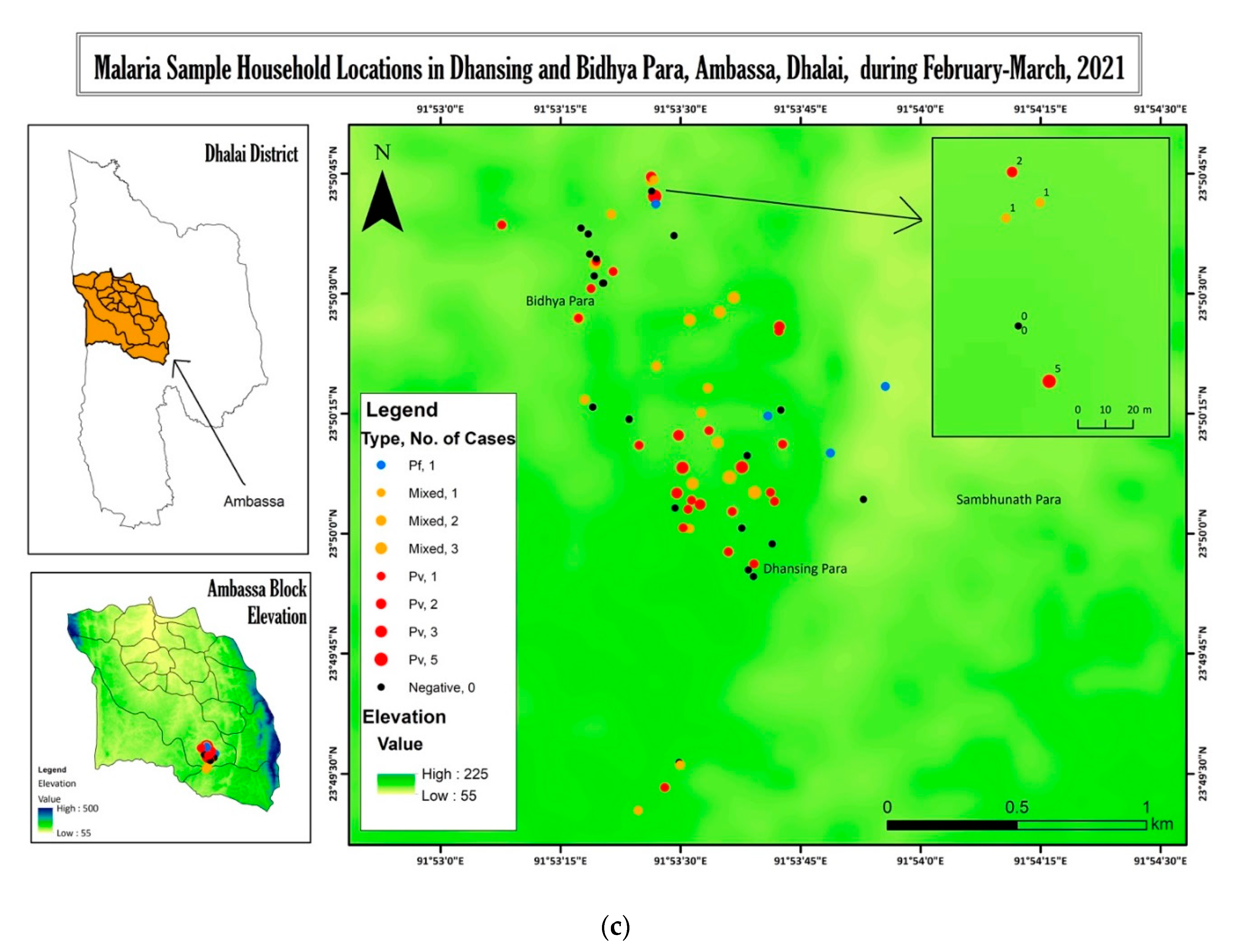
P. falciparum predominant area. This study also suggests that sensitive diagnostic methods like PCR, other than microscopy, may be used for mass surveillance, especially in the dry post-winter season, to unearth the reservoir of infection. Ecological maps (
Figure 2) show that the cases are in the vicinity of the forested regions and Jhum cultivation lands, and there are several households with 2–5 cases. Some of these households are located in proximity to each other. As the maps are constructed from the satellite images of 2019, and the shifting cultivation, open forest, and dense forest areas are interchanged among themselves, we have not associated the proximity of cases to any particular forest type. Still, it can be seen that they are in close vicinity to the forest land. It would be worth finding out whether there are clusters and targeting them with intervention [
33] and treatment aimed at malaria control and elimination. These reservoirs can fuel transmission in the subsequent months. It is all the more relevant for these areas as most of the people in the study area are Jhum cultivators. Jhum cultivation has been shown as a risk factor for malaria in adjacent Bangladesh [
34] and Tripura as well [
35]. Jhum cultivation involves shifting cultivation in the deep forested areas, which involves the temporary stay of the cultivators or their majority of time being spent in the forests from April onwards, reducing their availability to health workers. Therefore, screening for the reservoir in pre-Jhum months (February to mid-April) and treating the positive cases with antimalarial drugs may help reduce transmission.
4. Methodology
4.1. Study Site and Population
Tripura is one of the smallest states among the eight states of northeast India that shares 84% of its total border with Bangladesh. Dhalai is the largest district of the state, situated approximately between longitude 91° 51.608″ E and latitude 23° 55.501″ N with a population of 378,000 according to 2011–2018 census data. Dhansinghpara and Bidyapara villages are located at 23°49′55″ N latitude, and 91°53′33″ E longitude, respectively, and about 155 m above mean sea level (MSL) and about 12 km south of the town of Ambassa, which is the district headquarters. About 40% of the area is under forest cover, while 45% is under scrubland. Agriculture land use covers about 0.13%, while about 6% of the site is under shifting cultivation.
4.2. Community Mass Survey
A door-to-door and health camp-based mass survey was carried out in Gurudhan subcenter under the Ambassa Primary Health Centre (PHC) in Dhalai District, from the third week of February 2021 to the first week of April 2021, by state health workers and volunteers. As these two villages are high endemic villages in the area (
Supplementary Table S1), these two villages were chosen to study malaria burden, symptomatic and asymptomatic cases, and plasmodium species distribution in dry winter months.
Health camp-based mass surveys are those where health camps are organized by the health department in the village premises, and villagers are informed beforehand to come and get tested, irrespective of fever status. Regarding the choice of household or individuals, the aim of the survey, as decided by Health Department and Malaria Program was to cover as many villagers as possible, if not all. Thus, whoever was available for testing and willing to get tested was tested and treated.
The total population in the two villages was 1009, namely 626 in Dhansingh and 383 in Bidyapara. Anyone available during the survey time and willing to give blood, irrespective of the presence of symptoms, was recruited for taking blood. There were some villagers who were not present in the village for a more extended period, either for a job or study or other reasons. They were not considered for the mass survey. Total such temporary absentees were 330: 203 in Dhansinghpara and 127 in Bidyapara. Hence, a total of 679 people was considered for the mass survey. During our survey in this period, among the available people, a total of 104 refused, namely 71 in Dhansinghpara and 33 in Bidyapara. Thus, 373 people (~55% of the considered population) could be covered, and blood was taken from them to test RDT. The rest of the people who live in the villages but were not found during the survey as they had gone out to the forest for Jhum cultivation or some other work were termed as unavailable. This year, due to elections in this area and other unrest, evening time visits were not possible, which are usually undertaken while conducting a mass survey to reach people who are unavailable during the daytime. However, as it could not be done this year, there was a high number of unavailable people. Questions on age, relations to HH head, fever history, travel history, forest exposure history, symptoms, and vector control measures were asked during the mass survey. In the case of febrile patients, detailed questionnaires were filled up.
4.3. Blood Sample Collection
Finger-prick blood samples were collected from individuals irrespective of the febrile status. Finger-prick blood samples were used for microscopic slide preparation and collected in small tubes with EDTA powder for molecular technique. Written informed consent from the participant or the guardians in case of minors was obtained. Blood spots were also taken on filter paper, air-dried, and stored at 4 °C for future molecular analysis.
All the 373 samples collected were tested by RDT by the Malaria Program. Blood slides and blood spots on filter papers were taken, and also whole blood was taken from the same finger prick in a tube containing EDTA, wherever available. For only 150 samples could whole blood be collected in the tubes. From the others, finger-prick blood could not be collected in tubes, as sufficient blood was not there. Therefore, in this study, we conducted PCR on these 150 whole blood samples collected in the tubes, not on the dried blood spots.
4.4. Rapid Diagnostic Test (RDT)
An RDT was performed only on febrile cases (people complaining of fever in the last seven days). Blood samples were collected to detect the presence of P. falciparum and P. vivax parasites using an RDT Malarigen kit (Aspen Laboratories) supplied by NVBDCP, India, according to the manufacturer’s protocol.
4.5. Blood Slide Examination (BSE)
Both thick and thin blood smears were examined. Thick smears were hemolyzed, and thin smears were fixed with methanol and stained with 10% Giemsa stain. Stained blood smears were examined under 100X oil immersion using a Zeiss microscope by three experienced technicians to confirm the presence of the
Plasmodium parasite [
36].
4.6. Parasite DNA Extraction
Parasite DNA was extracted from the blood samples that were collected in 0.5 mL microcentrifuge tubes containing EDTA. Briefly, 200 µL 1× phosphate-buffered saline (PBS) was added to the tube, followed by a short spin. DNA extraction was carried out using QIAamp DNA blood mini kit as per the manufacturer’s protocol (Qiagen, CA, USA). Then, DNA was eluted in 50 µL elution buffer and extracted DNA was stored at −20 °C for further molecular analysis.
4.7. Plasmodium Species Detection by Nested PCR (nPCR)
Species-specific nested PCR was performed to confirm the presence of
Plasmodium species targeting the 18S rRNA as described by Siwal et al. (2018) [
37]. For each sample, nest-1 PCR was carried out in a final volume of 20 µL reaction containing 1× Promega master mix, 0.25 µM primer, 2 mM MgCl
2, and 5 µL of DNA template. Nest-2 PCR was carried out in a final volume of 10 µL reaction containing 1× Promega master mix, 0.5 µM primer, 2 mM MgCl
2, and 2.8 µL of nest-1 PCR product as template. Laboratory adapted Dd2 and 3D7
Plasmodium falciparum, and previously confirmed positive
P. vivax DNA samples were included as positive controls for every set of PCR. Nuclease free water and DNA of healthy individuals were also included as negative controls for the PCR assays. The amplified products were then visualized in 2% agarose gel stained with 0.5 µg/mL ethidium bromide under BioRad XR UV transilluminator.
4.8. Light Trap Collections
Host seeking adult female mosquitoes were collected using the CDC miniature light trap fitted in human dwellings of Dhansinghpara and Bidyapara villages. Light traps were fitted in the verandah, an outdoor porch with a roof outside the house. Collections were made monthly using five light traps in each village with two index houses fixed per month and three randomly rotated. Based on the baseline data, collections were made from two fixed houses every month and a few randomly selected houses, often those households which reported malaria cases. Traps were usually placed adjacent to the bed.
4.9. Mosquito Identification
Anopheles mosquitoes collected in the field were brought to the laboratory and identified morphologically using the keys of Nagpal and Sharma 1991 [
38]. Morphologically identified specimens belonging to the Dirus and Minimus complexes were confirmed to species level by molecular methods using DNA extracted from leg or abdomen of the mosquito through allele-specific polymerase chain reaction (ASPCR) assays [
39,
40,
41].
4.10. Plasmodium Species Detection by Nested Quantitative PCR (nqPCR)
The very sensitive nested real-time PCR method targeting the
Plasmodium cytochrome
b gene as described by Canier et al. (2013) in
Plasmodium blood stages was performed to detect
Plasmodium species with some modifications [
42] in the known primary vectors of the area, i.e.,
Anopheles minimus and
Anopheles baimaii [
4,
38]. For parasite sporozoite screening in mosquitoes, we used DNA extracted from the head and thorax dissected from a single
Anopheles specimen for each reaction. As we obtained little DNA from the head and thorax part of a single mosquito, we used the more sensitive technique of detection by nested quantitative PCR (nqPCR) for cytochrome b gene, which has more copy numbers, and this method is more sensitive in detecting a low amount. For all the real-time assays, in a 10 µL reaction volume, Promega 2× SYBR green master mix was used with carboxy-X-rhodamine (CXR) passive dye where 2.5 µL DNA was used as a template, and for every sample, the reaction was carried out in duplicate.
4.11. Meteorological Data Collection
The study used rainfall data from National Aeronautics and Space Administration’s (NASA) GPM (Global Precipitation Measurement) project from January to March 2021. The dataset used is the Integrated Multi-Satellite Retrievals for GPM (IMERG) Late Daily 10 × 10 km Level-3 Integrated Multi-Satellite Retrievals for GPM Daily Late Run (GPM 3IMERGDL) of GPM Level 3, derived from the dataset of the half-hourly 3IMERGHL. The result is an accelerated late estimate of the accumulated daily precipitation. The temperature and relative humidity data were taken from NASA’s MERRA-2 (Modern-Era Retrospective analysis for Research and Applications) model. The used products are the daily maximum (T2MMAX), minimum (T2MMIN), average temperature (T2MMEAN), and relative humidity on a spatial resolution of 50 km × 62.5 km. The datasets were downloaded in NetCDF formats, which were further extracted using software codes.
4.12. Preparation of Ecological Maps
Land use land cover mapping was prepared using orthorectified Indian Remote Sensing satellite data, Cartosat-1 (2.5 m) and LISS-IV (5.8 m), employing on-screen visual interpretation techniques in the GIS (Geographical Information System) platform. Major land use and land cover categories and subcategories were delineated and updated using the latest data (2019) on the spatial layer initially prepared under NRSC/ISRO (National Remote Sensing Centre/Indian Space Research Organization).
Space-based Information Support for Decentralized Planning at the Panchayat level was used. The mapping was done at 1:10,000 scale. Field verifications were made by the project team to check the accuracy of the interpreted data. Geolocations of P. vivax positive households were collected during the survey and plotted on the map for analyses of the proximity of the households to the Jhum fields/plantations/open forests/deep forests/croplands.
4.13. Statistical Analysis
IBM SPSS 20 and Epi InfoTM version 7, CDC (Atlanta, GA, USA) were used for statistical analysis.
4.14. Malaria Case Records
Malaria yearly cases, API, and cases from January to March for Bidyapara and Dhansingh villages were compiled from the reports and registers of health workers and volunteers, which include routine active/passive surveillance and mass surveillance data. Data on annual malaria cases were taken from the reports of the Malaria Program, which include routine active/passive surveillance and mass surveillance data.


 ,
, 






{kind=link}
{kind=link}
{kind=link}