
Evaluation of Gene Polymorphism and Gingival Crevicular Fluid Levels of Matrix Metalloproteinase-3 in a Group of Turkish Periodontitis Patients

 , ,
, , 
Abstract
:1. Introduction
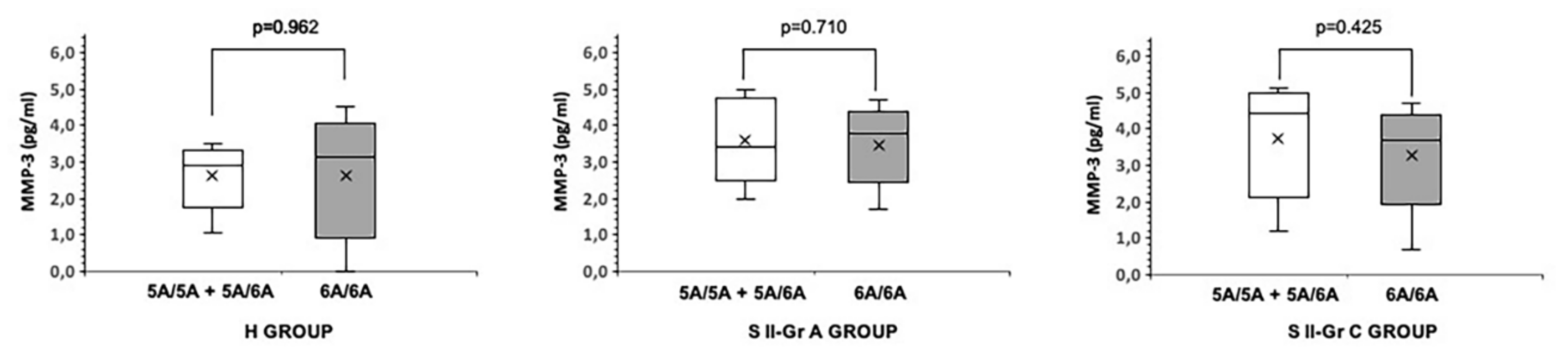
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Population and Clinical Assessment
4.2. Genetic Analysis
4.3. Gingival Crevicular Fluid Collection
4.4. ELISA Analysis
4.5. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef]
- Finoti, L.S.; Nepomuceno, R.; Pigossi, S.C.; Corbi, S.C.; Secolin, R.; Scarel-Caminaga, R.M. Association between interleukin-8 levels and chronic periodontal disease: A PRISMA-compliant systematic review and meta-analysis. Medicine 2017, 96, e6932. [Google Scholar] [CrossRef]
- Yucel-Lindberg, T.; Båge, T. Inflammatory mediators in the pathogenesis of periodontitis. Expert Rev. Mol. Med. 2013, 5, 15. [Google Scholar] [CrossRef] [Green Version]
- Almehmadi, A.H.; Alghamdi, F. Biomarkers of alveolar bone resorption in gingival crevicular fluid: A systematic review. Arch. Oral Biol. 2018, 93, 12–21. [Google Scholar] [CrossRef]
- Kinane, D.F. Regulators of tissue destruction and homeostasis as diagnostic aids in periodontology. Periodontology 2000, 24, 215–225. [Google Scholar] [CrossRef]
- Hart, T.C. Genetic considerations of risk in human periodontal disease. Curr. Opin. Periodontol. 1994, 3–11. [Google Scholar]
- Franco, C.; Patricia, H.R.; Timo, S.; Claudia, B.; Marcela, H. Matrix Metalloproteinases as Regulators of Periodontal Inflammation. Int. J. Mol. Sci. 2017, 18, 440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Checchi, V.; Maravic, T.; Bellini, P.; Generali, L.; Consolo, U.; Breschi, L.; Mazzoni, A. The Role of Matrix Metalloproteinases in Periodontal Disease. Int. J. Environ. Res. Public Health 2020, 17, 4923. [Google Scholar] [CrossRef] [PubMed]
- Astolfi, C.M.; Shinohara, A.L.; da Silva, R.A.; Santos, M.C.; Line, S.R.; de Souza, A.P. Genetic polymorphisms in the MMP-1 and MMP-3 gene may contribute to chronic periodontitis in a Brazilian population. J. Clin. Periodontol. 2006, 33, 699–703. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Tjäderhane, L.; Konttinen, Y.T.; Lauhio, A.; Salo, T.; Lee, H.M.; Golub, L.M.; Brown, D.L.; Mäntylä, P. Matrix metalloproteinases: Contribution to pathogenesis, diagnosis and treatment of periodontal inflammation. Ann. Med. 2006, 38, 306–321. [Google Scholar] [CrossRef] [PubMed]
- Kiili, M.; Cox, S.W.; Chen, H.Y.; Wahlgren, J.; Maisi, P.; Eley, B.M.; Salo, T.; Sorsa, T. Collagenase-2 (MMP-8) and collagenase-3 (MMP-13) in adult periodontitis: Molecular forms and levels in gingival crevicular fluid and immunolocalisation in gingival tissue. J. Clin. Periodontol. 2002, 29, 224–232. [Google Scholar] [CrossRef]
- Cao, Z.; Li, C.; Jin, L.; Corbet, E.F. Association of matrix metalloproteinase-1 promoter polymorphism with generalized aggressive periodontitis in a Chinese population. J. Periodontal. Res. 2005, 40, 427–431. [Google Scholar] [CrossRef]
- Cao, Z.; Li, C.; Zhu, G. MMP-1 promoter gene polymorphism and susceptibility to chronic periodontitis in a Chinese population. Tissue Antigens. 2006, 68, 38–43. [Google Scholar] [CrossRef]
- Da Silva, M.K.; de Carvalho, A.C.G.; Alves, E.H.P.; da Silva, F.R.P.; Pessoa, L.D.S.; Vasconcelos, D.F.P. Genetic Factors and the Risk of Periodontitis Development: Findings from a Systematic Review Composed of 13 Studies of Meta-Analysis with 71,531 Participants. Int. J. Dent. 2017, 2017, 1914073. [Google Scholar] [CrossRef]
- Weng, H.; Yan, Y.; Jin, Y.H.; Meng, X.Y.; Mo, Y.Y.; Zeng, X.T. Matrix metalloproteinase gene polymorphisms and periodontitis susceptibility: A meta-analysis involving 6162 individuals. Sci. Rep. 2016, 6, 24812. [Google Scholar] [CrossRef] [Green Version]
- Ding, C.; Chen, X.; Zhang, P.T.; Huang, J.P.; Xu, Y.; Chen, N.; Zhong, L.J. Matrix Metalloproteinase-3 -1171 5A/6A Polymorphism (rs35068180) is Associated with Risk of Periodontitis. Sci. Rep. 2015, 5, 11667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilmaz, M.; Kasnak, G.; Polat, N.G.; Topcuoglu, N.E.; Kulekci, G.; Firatli, E. Pathogen profile and MMP-3 levels in areas with varied attachment loss in generalized aggressive and chronic periodontitis. Cent. Eur. J. Immunol. 2019, 44, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.E.; Golub, L.M. Modulation of matrix metalloproteinase activities in periodontitis as a treatment strategy. Periodontology 2000, 24, 226–238. [Google Scholar] [CrossRef]
- Ogata, Y.; Enghild, J.J.; Nagase, H. Matrix metalloproteinase 3 (stromelysin) activates the precursor for the human matrix metalloproteinase 9. J. Biol. Chem. 1992, 267, 3581–3584. [Google Scholar] [CrossRef]
- Kornman, K.S.; Crane, A.; Wang, H.Y.; di Giovine, F.S.; Newman, M.G.; Pirk, F.W.; Wilson, T.G., Jr.; Higginbottom, F.L.; Duff, G.W. The interleukin-1 genotype as a severity factor in adult periodontal disease. J. Clin. Periodontol. 1997, 24, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Xiao, L.; Hu, J. Matrix metalloproteinase-1 promoter -1607 1G/2G polymorphism and chronic periodontitis susceptibility: A meta-analysis and systematic review. J. Clin. Periodontol. 2013, 40, 1095–1103. [Google Scholar] [CrossRef]
- Ding, C.; Ji, X.; Chen, X.; Xu, Y.; Zhong, L. TNF-α gene promoter polymorphisms contribute to periodontitis susceptibility: Evidence from 46 studies. J. Clin. Periodontol. 2014, 41, 748–759. [Google Scholar] [CrossRef]
- Albuquerque, C.M.; Cortinhas, A.J.; Morinha, F.J.; Leitão, J.C.; Viegas, C.A.; Bastos, E.M. Association of the IL-10 polymorphisms and periodontitis: A meta-analysis. Mol. Biol. Rep. 2012, 39, 9319–9329. [Google Scholar] [CrossRef]
- Letra, A.; Silva, R.M.; Rylands, R.J.; Silveira, E.M.; de Souza, A.P.; Wendell, S.K.; Garlet, G.P.; Vieira, A.R. MMP3 and TIMP1 variants contribute to chronic periodontitis and may be implicated in disease progression. J. Clin. Periodontol. 2012, 39, 707–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loo, W.T.; Wang, M.; Jin, L.J.; Cheung, M.N.; Li, G.R. Association of matrix metalloproteinase (MMP-1, MMP-3 and MMP-9) and cyclooxygenase-2 gene polymorphisms and their proteins with chronic periodontitis. Arch. Oral Biol. 2011, 56, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Yue, Y.; Tian, Y.; Li, J.L.; Wang, M.; Liang, H.; Liao, P.; Loo, W.T.; Cheung, M.N.; Chow, L.W. Association of matrix metalloproteinase (MMP)-1, 3, 9, interleukin (IL)-2, 8 and cyclooxygenase (COX)-2 gene polymorphisms with chronic periodontitis in a Chinese population. Cytokine 2012, 60, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Itagaki, M.; Kubota, T.; Tai, H.; Shimada, Y.; Morozumi, T.; Yamazaki, K. Matrix metalloproteinase-1 and -3 gene promoter polymorphisms in Japanese patients with periodontitis. J. Clin. Periodontol. 2004, 31, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Majumder, P.; Ghosh, S.; Dey, S.K. Matrix metalloproteinase gene polymorphisms in chronic periodontitis: A case-control study in the Indian population. J. Genet. 2019, 98, 32. [Google Scholar] [CrossRef] [PubMed]
- Ustun, K.; Alptekin, N.O.; Hakki, S.S.; Hakki, E.E. Investigation of matrix metalloproteinase-1 -1607 1G/2G polymorphism in a Turkish population with periodontitis. J. Clin. Periodontol. 2008, 35, 1013–1019. [Google Scholar] [CrossRef]
- Pirhan, D.; Atilla, G.; Emingil, G.; Sorsa, T.; Tervahartiala, T.; Berdeli, A. Effect of MMP-1 promoter polymorphisms on GCF MMP-1 levels and outcome of periodontal therapy in patients with severe chronic periodontitis. J. Clin. Periodontol. 2008, 35, 862–870. [Google Scholar] [CrossRef]
- Gürkan, A.; Emingil, G.; Saygan, B.H.; Atilla, G.; Cinarcik, S.; Köse, T.; Berdeli, A. Matrix metalloproteinase-2, -9, and -12 gene polymorphisms in generalized aggressive periodontitis. J. Periodontol. 2007, 78, 2338–2347. [Google Scholar] [CrossRef]
- Emingil, G.; Han, B.; Gürkan, A.; Berdeli, A.; Tervahartiala, T.; Salo, T.; Pussinen, P.J.; Köse, T.; Atilla, G.; Sorsa, T. Matrix metalloproteinase (MMP)-8 and tissue inhibitor of MMP-1 (TIMP-1) gene polymorphisms in generalized aggressive periodontitis: Gingival crevicular fluid MMP-8 and TIMP-1 levels and outcome of periodontal therapy. J. Periodontol. 2014, 85, 1070–1080. [Google Scholar] [CrossRef]
- Keles, G.C.; Gunes, S.; Sumer, A.P.; Sumer, M.; Kara, N.; Bagci, H.; Koprulu, H. Association of matrix metalloproteinase-9 promoter gene polymorphism with chronic periodontitis. J. Periodontol. 2006, 77, 1510–1514. [Google Scholar] [CrossRef]
- Laine, M.L.; Crielaard, W.; Loos, B.G. Genetic susceptibility to periodontitis. Periodontology 2000 2012, 58, 37–68. [Google Scholar] [CrossRef]
- Huynh-Ba, G.; Lang, N.P.; Tonetti, M.S.; Salvi, G.E. The association of the composite IL-1 genotype with periodontitis progression and/or treatment outcomes: A systematic review. J. Clin. Periodontol. 2007, 34, 305–317. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J. Disease progression: Identification of high-risk groups and individuals for periodontitis. J. Clin. Periodontol. 2005, 32, 196–209. [Google Scholar] [CrossRef]
- Lambert, E.; Dassé, E.; Haye, B.; Petitfrère, E. TIMPs as multifacial proteins. Crit. Rev. Oncol. Hematol. 2004, 49, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Bchir, S.; Ben Nasr, H.; Garrouch, A.; Ben Anes, A.; Abbassi, A.; Tabka, Z.; Chahed, K. MMP-3 (-1171 5A/6A; Lys45Glu) variants affect serum levels of matrix metalloproteinase (MMP)-3 and correlate with severity of COPD: A study of MMP-3, MMP-7 and MMP-12 in a Tunisian population. J. Gene Med. 2018, 20, 2999. [Google Scholar] [CrossRef]
- Toyman, U.; Tüter, G.; Kurtiş, B.; Kıvrak, E.; Bozkurt, Ş.; Yücel, A.A.; Serdar, M. Evaluation of gingival crevicular fluid levels of tissue plasminogen activator, plasminogen activator inhibitor 2, matrix metalloproteinase-3 and interleukin 1-β in patients with different periodontal diseases. J. Periodontal. Res. 2015, 50, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, P.F.; Huang, H.; McAninley, S.; Alfant, B.; Harrison, P.; Aukhil, I.; Walker, C.; Shaddox, L.M. Periodontal treatment reduces matrix metalloproteinase levels in localized aggressive periodontitis. J Periodontol. 2013, 84, 1801–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tüter, G.; Kurtiş, B.; Serdar, M.; Yücel, A.; Ayhan, E.; Karaduman, B.; Ozcan, G. Effects of phase I periodontal treatment on gingival crevicular fluid levels of matrix metalloproteinase-3 and tissue inhibitor of metalloproteinase-1. J. Clin. Periodontol. 2005, 32, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Windsor, L.J. Porphyromonas gingivalis affects host collagen degradation by affecting expression, activation, and inhibition of matrix metalloproteinases. J. Periodontal. Res. 2006, 41, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Domeij, H.; Yucel-Lindberg, T.; Modéer, T. Cell interactions between human gingival fibroblasts and monocytes stimulate the production of matrix metalloproteinase-1 in gingival fibroblasts. J. Periodontal. Res. 2006, 41, 108–117. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Sanz, M. Implementation of the new classification of periodontal diseases: Decision-making algorithms for clinical practice and education. J. Clin. Periodontol. 2019, 46, 398–405. [Google Scholar] [CrossRef]
- Mäntylä, P.; Stenman, M.; Kinane, D.F.; Tikanoja, S.; Luoto, H.; Salo, T.; Sorsa, T. Gingival crevicular fluid collagenase-2 (MMP-8) test stick for chair-side monitoring of periodontitis. J. Periodontal. Res. 2003, 38, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S162–S170. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Groups | p Value | ||||||
|---|---|---|---|---|---|---|---|
| H | S II-Gr A | S II-Gr C | H vs. S II-Gr A | H vs. S II-Gr C | S II-Gr A vs. S II-Gr C | ||
| Clinical Measures, Age, and Gender | Age (years) (Mean (Min–Max)) | 31.8 (28–35) | 33.7 (29–37) | 30.7 (26–34) | p = 0.598 | p = 0.768 | p = 0.632 |
| Gender (Female % (n)) | 48.6% (35) | 48.5% (33) | 46.8% (30) | p = 0.788 | p = 0.539 | p = 0.572 | |
| PPD (mm) | 2.6 ± 1.16 | 4.14 ± 1.02 | 4.78 ± 1.29 | p < 0.01 | p < 0.01 | p = 0.198 | |
| CAL (mm) | 2.81 ± 0.85 | 4.78 ± 1.84 | 4.87 ± 1.71 | p < 0.01 | p < 0.01 | p = 0.136 | |
| PI | 0.48 ± 0.60 | 2.67 ± 0.39 | 1.46 ± 0.44 | p < 0.01 | p < 0.01 | p = 0.029 | |
| GI | 0.44 ± 0.52 | 2.24 ± 0.19 | 2.19 ± 0.18 | p < 0.01 | p < 0.01 | p = 0.374 | |
| Rate % (n) | |||||||
|---|---|---|---|---|---|---|---|
| H | S II-Gr A | S II-Gr C | H vs. S II-Gr A | H vs. S II-Gr C | S II-Gr A vs. S II-Gr C | ||
| MMP-3 Genotype (rs35068180) | 5A/5A | 1.38% (1) | 1.47% (1) | 3.12% (2) | 0.973 | 0.054 | 0.063 |
| 5A/6A | 26.38% (19) | 26.47% (18) | 34.37% (22) | ||||
| 6A/6A | 72.22% (52) | 72.05% (49) | 62.50% (40) | ||||
| Allele Frequency | 5A | 14.58% (21) | 14.70% (20) | 19.40% (26) | 0.918 | 0.084 | 0.098 |
| 6A | 85.41% (123) | 85.29% (116) | 80.59% (108) | ||||
| Carriage Rate | 5A+ | 27.77% (20) | 27.94% (19) | 37.50% (24) | 0.946 | 0.052 | 0.053 |
| 5A− | 72.22% (52) | 72.05% (49) | 62.50% (40) | ||||
| Stage II Grade A | Stage II Grade C | |||||||
|---|---|---|---|---|---|---|---|---|
| Age | Gender | Allele Carriage (5A/5A and 5A/6A) | Age | Gender | Allele Carriage (5A/5A and 5A/6A) | |||
| <30 Years | >30 Years | <30 Years | >30 Years | |||||
| OR | 2.39 | 5.58 | 8.80 | 1.32 | 4.40 | 8.55 | 9.46 | 0.38 |
| 95% CI | 0.13–42.30 | 0.31–98.76 | 0.49–155.77 | 0.07–23.36 | 0.24–77.87 | 0.48–151.32 | 0.53–167.43 | 0.02–6.72 |
| p Value | 0.142 | 0.460 | 0.838 | 0.741 | 0.689 | 0.128 | 0.758 | 0.550 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasnak, G.; Yılmaz, M.; Ünsal, R.B.K.; Polat, N.G.; Fıratlı, E. Evaluation of Gene Polymorphism and Gingival Crevicular Fluid Levels of Matrix Metalloproteinase-3 in a Group of Turkish Periodontitis Patients. Pathogens 2021, 10, 1260. https://doi.org/10.3390/pathogens10101260
Kasnak G, Yılmaz M, Ünsal RBK, Polat NG, Fıratlı E. Evaluation of Gene Polymorphism and Gingival Crevicular Fluid Levels of Matrix Metalloproteinase-3 in a Group of Turkish Periodontitis Patients. Pathogens. 2021; 10(10):1260. https://doi.org/10.3390/pathogens10101260
Chicago/Turabian StyleKasnak, Gökhan, Mustafa Yılmaz, Revan Birke Koca Ünsal, Nuray Gürel Polat, and Erhan Fıratlı. 2021. "Evaluation of Gene Polymorphism and Gingival Crevicular Fluid Levels of Matrix Metalloproteinase-3 in a Group of Turkish Periodontitis Patients" Pathogens 10, no. 10: 1260. https://doi.org/10.3390/pathogens10101260
APA StyleKasnak, G., Yılmaz, M., Ünsal, R. B. K., Polat, N. G., & Fıratlı, E. (2021). Evaluation of Gene Polymorphism and Gingival Crevicular Fluid Levels of Matrix Metalloproteinase-3 in a Group of Turkish Periodontitis Patients. Pathogens, 10(10), 1260. https://doi.org/10.3390/pathogens10101260