
Emergence of Besnoitia besnoiti in Belgium



Abstract
1. Introduction
2. Results
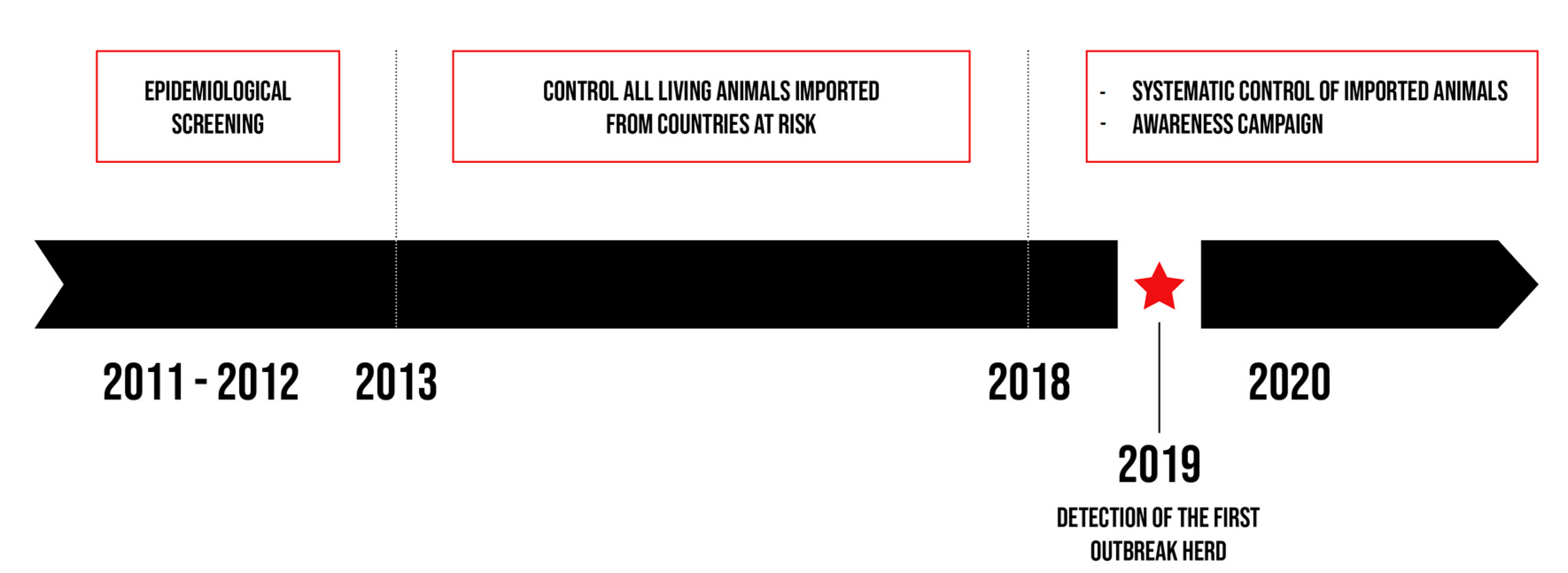
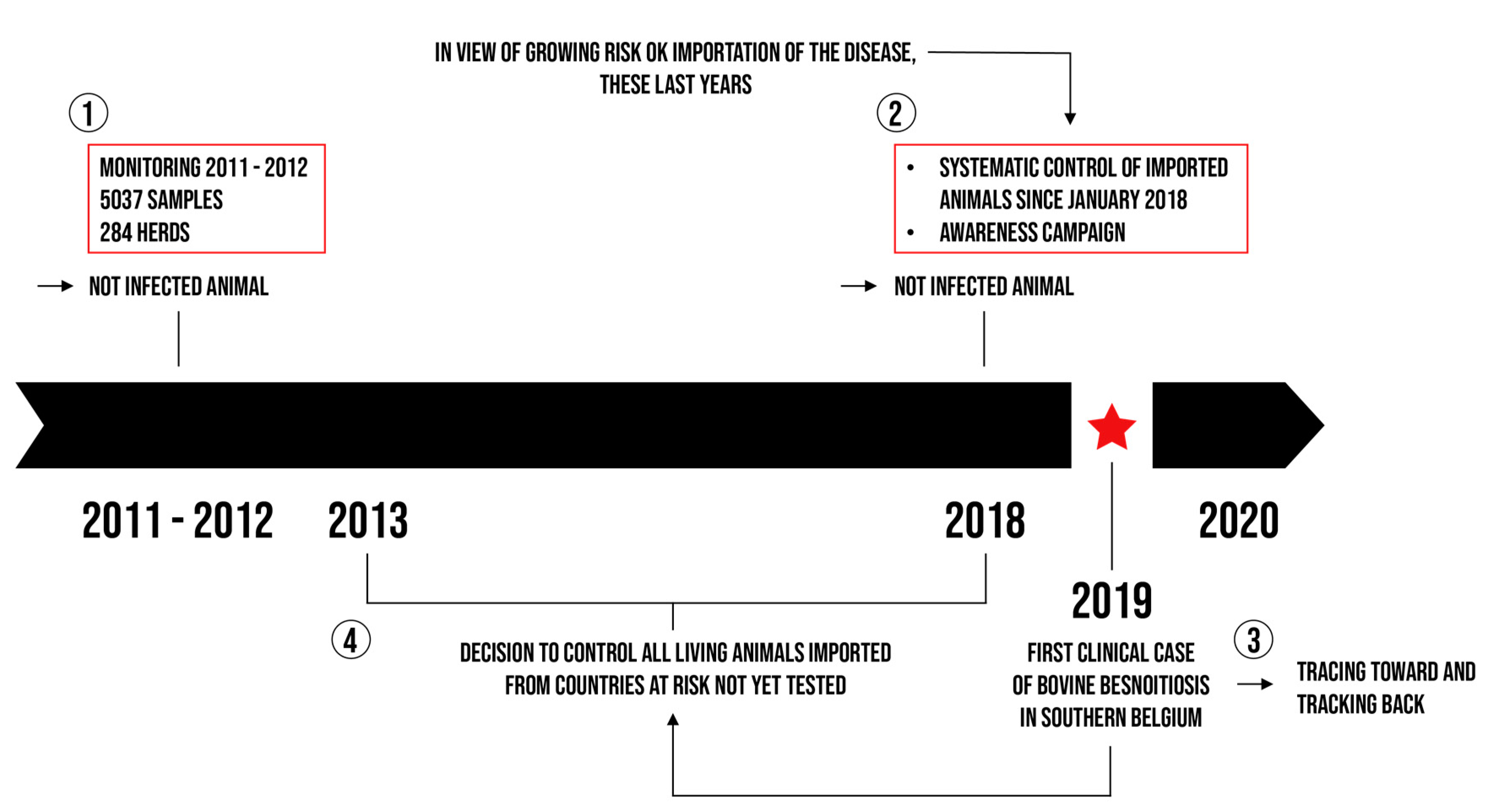
2.1. Active Surveillance
2.1.1. Epidemiological Screening
2.1.2. Serological Testing of Imported Live Cattle
2.1.3. Control of All Live Animals Imported from Countries at Risk
2.2. Awareness Campaign and Passive Surveillance
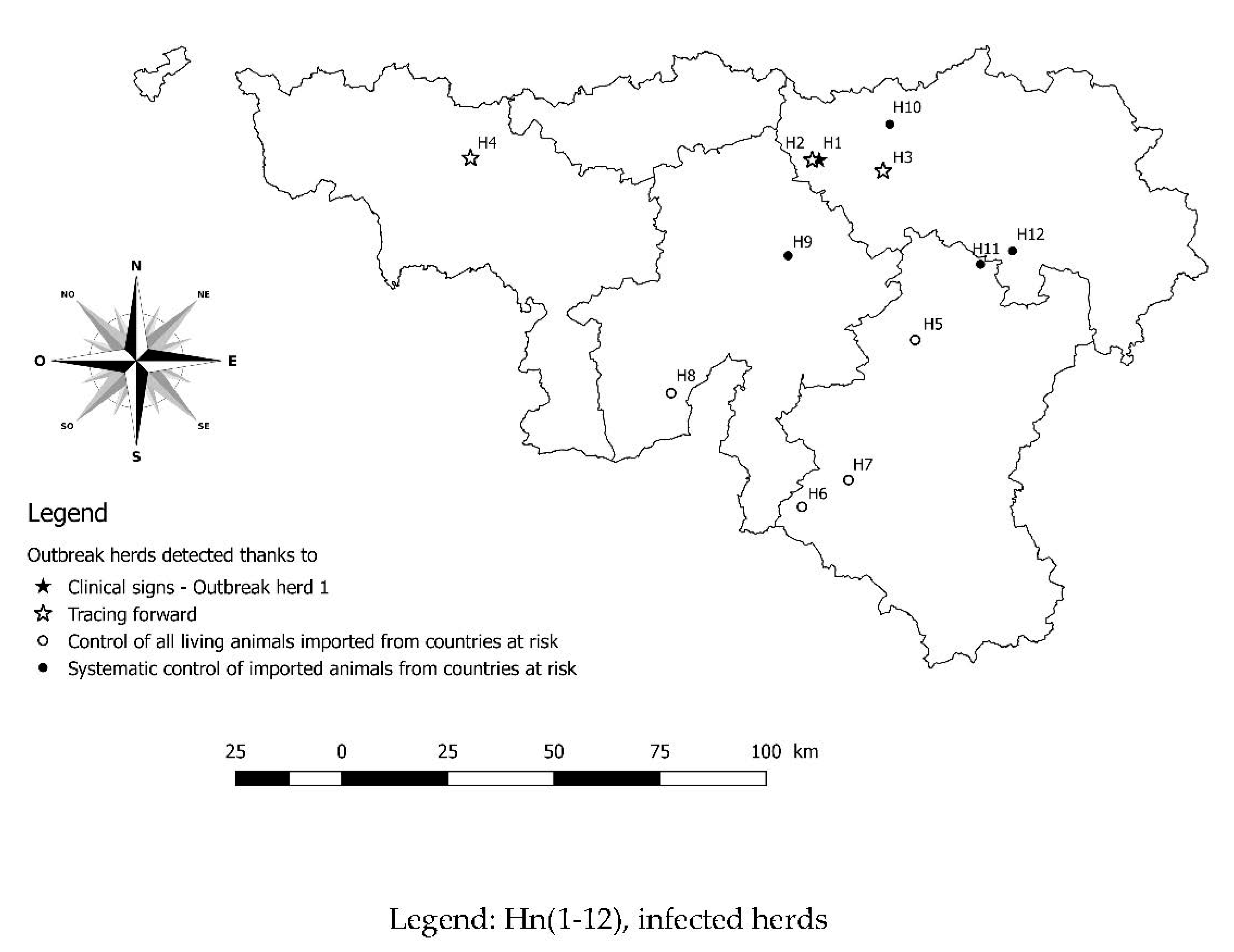
2.3. Tracing Back
2.4. Tracing Forward
3. Discussion
4. Materials and Methods
4.1. Study Area
4.2. Sampling
4.2.1. Epidemiological Screening
4.2.2. Serological Testing at Importation
4.2.3. Control of All Live Animals Imported from Countries at Risk
4.2.4. Awareness Campaign towards the Breeding Sector
4.3. Epidemiological Inquiry
4.4. Clinical Presentation
4.5. Serological Examination
Serological Screening
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ellis, J.T.; Holmdahl, O.J.; Ryce, C.; Njenga, J.M.; Harper, P.A.; Morrison, D.A. Molecular phylogeny of Besnoitia and the genetic relationships among Besnoitia of cattle, wildebeest and goats. Protist 2000, 151, 329–336. [Google Scholar] [CrossRef][Green Version]
- Dubey, J.P.; Sreekumar, C.; Donovan, T.; Rozmanec, M.; Rosenthal, B.M.; Vianna, M.C.; Belden, J.S. Redescription of Besnoitia bennetti (Protozoa: Apicomplexa) from the donkey (Equus asinus). Int. J. Parasitol. 2005, 35, 659–672. [Google Scholar] [CrossRef]
- Cortes, H.; Leitao, A.; Gottstein, B.; Hemphill, A. A review on bovine besnoitiosis: A disease with economic impact in herd health management, caused by Besnoitia besnoiti (Franco and Borges, 1916). Parasitology 2014, 141, 1406–1417. [Google Scholar] [CrossRef] [PubMed]
- Alzieu, J.P.; Cortes, H.; Gottstein, B.; Jacquiet, P.; Dorchies, P.; Schelcher, F.; L’hostis, M. La besnoitiose bovine: Actualités épidémiologiques et diagnostiques. Bull. G.T.V.—Hors Série Parasitol. Bov. Nouv. Approche 2007, 40, 41–49. [Google Scholar]
- Lienard, E.; Salem, A.; Grisez, C.; Prevot, F.; Bergeaud, J.P.; Franc, M.; Gottstein, B.; Alzieu, J.P.; Lagalisse, Y.; Jacquiet, P. A longitudinal study of Besnoitia besnoiti infections and seasonal abundance of Stomoxys calcitrans in a dairy cattle farm of southwest France. Vet. Parasitol. 2011, 177, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Lienard, E.; Salem, A.; Jacquiet, P.; Grisez, C.; Prevot, F.; Blanchard, B.; .Bouhsira, E.; Franc, M. Development of a protocol testing the ability of Stomoxys calcitrans (Linnaeus, 1758) (Diptera: Muscidae) to transmit Besnoitia besnoiti (Henry, 1913) (Apicomplexa: Sarcocystidae). Parasitol. Res. 2013, 112, 479–486. [Google Scholar] [CrossRef][Green Version]
- Cortes, H.; Leitao, A.; Vidal, R.; Vila-Vicosa, M.J.; Ferreira, M.L.; Caeiro, V.; Hjerpe, C.A. Besnoitiosis in bulls in Portugal. Vet. Rec. 2005, 157, 262–264. [Google Scholar] [CrossRef]
- Juste, R.A.; Cuervo, L.A.; Marco, J.C.; Oregui, L.M. La besnoitiosis bovina: ¿ desconocida en España? Med. Vet. 1990, 7, 613–618. [Google Scholar]
- Pols, J.W. Studies on bovine besnoitiosis with special reference to the aetiology. Onderstepoort J. Vet. Res. 1960, 28, 265–356. [Google Scholar]
- Efsa. Bovine Besnoitiosis: An emerging disease in Europe. Efsa J. 2010, 8, 1499. [Google Scholar]
- Jacquiet, P.; Lienard, E.; Franc, M. Bovine besnoitiosis: Epidemiological and clinical aspects. Vet. Parasitol. 2010, 174, 30–36. [Google Scholar] [CrossRef]
- Alvarez-Garcia, G.; Frey, C.F.; Mora, L.M.; Schares, G. A century of bovine besnoitiosis: An unknown disease re-emerging in Europe. Trends Parasitol. 2013, 29, 407–415. [Google Scholar] [CrossRef]
- Mehlhorn, H.; Klimpel, S.; Schein, E.; Heydorn, A.O.; Al-Quraishy, S.; Selmair, J. Another African disease in Central Europa: Besnoitiosis of cattle. I. Light and electron microscopical study. Parasitol. Res. 2009, 104, 861–868. [Google Scholar] [CrossRef]
- Mutinelli, F.; Schiavon, E.; Ceglie, L.; Fasolato, M.; Natale, A.; Rampin, F.; Carminato, A. Bovine besnoitiosis in imported cattle in Italy. Vet. Parasitol. 2011, 178, 198. [Google Scholar] [CrossRef]
- Lesser, M.; Braun, U.; Deplazes, P.; Gottstein, B.; Hilbe, M.; Basso, W. First cases of besnoitiosis in cattle in Switzerland. Schweiz. Arch. Tierheilkd. 2012, 154, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Hornok, S.; Fedak, A.; Baska, F.; Hofmann-Lehmann, R.; Basso, W. Bovine besnoitiosis emerging in Central-Eastern Europe, Hungary. Parasit Vectors 2014, 7, 20. [Google Scholar] [CrossRef][Green Version]
- Vanhoudt, A.; Pardon, B.; De Schutter, P.; Bosseler, L.; Sarre, C.; Vercruysse, J.; Deprez, P. First confirmed case of bovine besnoitiosis in an imported bull in Belgium. Vlaams Diergeneeskd. Tijdschr. 2015, 84, 205–211. [Google Scholar] [CrossRef]
- Gentile, A.; Militerno, G.; Schares, G.; Nanni, A.; Testoni, S.; Bassi, P.; Gollnick, N.S. Evidence for bovine besnoitiosis being endemic in Italy--first in vitro isolation of Besnoitia besnoiti from cattle born in Italy. Vet. Parasitol. 2012, 184, 108–115. [Google Scholar] [CrossRef]
- Renault, V.; Damiaans, B.; Sarrazin, S.; Humblet, M.F.; Dewulf, J.; Saegerman, C. Biosecurity practices in Belgian cattle farming: Level of implementation, constraints and weaknesses. Transbound. Emerg. Dis. 2018, 65, 1246–1261. [Google Scholar] [CrossRef] [PubMed]
- Bigalke, R.D. New concepts on the epidemiological features of bovine besnoitiosis as determined by laboratory and field investigations. Onderstepoort J. Vet. Res. 1968, 35, 3–137. [Google Scholar]
- Alzieu, J.-P.; Lienard, E.; Franc, M. New data on kinetics of infection by Besnoitiosis in cattle herds from endemic and non-endemic french areas. In Proceedings of the European Buiatrics Forum, Marseille, France, 16–18 November 2011. [Google Scholar]
- Gazzonis, A.L.; Alvarez Garcia, G.; Maggioni, A.; Zanzani, S.A.; Olivieri, E.; Compiani, R.; Sironi, G.; Ortega-Mora, L.M.; Manfredi, M.T. Serological dynamics and risk factors of Besnoitia besnoiti infection in breeding bulls from an endemically infected purebred beef herd. Parasitol. Res. 2017, 116, 1383–1393. [Google Scholar] [CrossRef]
- Nieto-Rodriguez, J.M.; Calero-Bernal, R.; Alvarez-Garcia, G.; Gutierrez-Exposito, D.; Redondo-Garcia, E.; Fernandez-Garcia, J.L.; Martinez-Estellez, M.A. Characterization of an outbreak of emerging bovine besnoitiosis in southwestern Spain. Parasitol. Res. 2016, 115, 2887–2892. [Google Scholar] [CrossRef]
- Fernandez-Garcia, A.; Alvarez-Garcia, G.; Risco-Castillo, V.; Aguado-Martinez, A.; Marcen, J.M.; Rojo-Montejo, S.; Castillo, J.A.; Ortega-Mora, L.M. Development and use of an indirect ELISA in an outbreak of bovine besnoitiosis in Spain. Vet. Rec. 2010, 166, 818–822. [Google Scholar] [CrossRef]
- Baldacchino, F.; Gardes, L.; De Stordeur, E.; Jay-Robert, P.; Garros, C. Blood-feeding patterns of horse flies in the French Pyrenees. Vet. Parasitol. 2014, 199, 283–288. [Google Scholar] [CrossRef]
- Gollnick, N.S.; Scharr, J.C.; Schares, G.; Langenmayer, M.C. Natural Besnoitia besnoiti infections in cattle: Chronology of disease progression. BMC Vet. Res. 2015, 11, 35. [Google Scholar] [CrossRef]
- Gutierrez-Exposito, D.; Arnal, M.C.; Martinez-Duran, D.; Regidor-Cerrillo, J.; Revilla, M.; de Luco, L.F.; Jimenez-Melendez, A.; Calero-Bernal, R.; Habela, M.A.; Garcia-Bocanegra, I.; et al. The role of wild ruminants as reservoirs of Besnoitia besnoiti infection in cattle. Vet. Parasitol. 2016, 223, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Saegerman, C.; Bertagnoli, S.; Meyer, G.; Ganiere, J.P.; Caufour, P.; De Clercq, K.; Jacquiet, P.; Fournie, G.; Hautefeuille, C.; Etore, F.; et al. Risk of introduction of lumpy skin disease in France by the import of vectors in animal trucks. PLoS ONE 2018, 13, e0198506. [Google Scholar] [CrossRef]
- Anonymous. Arrêté Royal Relatif à la Lutte Contre la Rhinotrachéite Infectieuse Bovine. Retrieved from JUSTEL—Législation Consolidée. Available online: http://www.ejustice.just.fgov.be/eli/arrete/2016/11/25/2016024273/justel (accessed on 1 November 2021).
- Cortes, H.; Nunes, S.; Reis, Y.; Staubli, D.; Vidal, R.; Sager, H.; Gottstein, B. Immunodiagnosis of Besnoitia besnoiti infection by ELISA and Western blot. Vet. Parasitol. 2006, 141, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Lunar, P.; Ortega-Mora, L.M.; Schares, G.; Gollnick, N.S.; Jacquiet, P.; Grisez, C.; Prevot, F.; Frey, C.F.; Gottstein, B.; Alvarez-Garcia, G. An inter-laboratory comparative study of serological tools employed in the diagnosis of Besnoitia besnoiti infection in bovines. Transbound. Emerg. Dis. 2013, 60, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Millan, J.; Sobrino, R.; Rodriguez, A.; Oleaga, A.; Gortazar, C.; Schares, G. Large-scale serosurvey of Besnoitia besnoiti in free-living carnivores in Spain. Vet. Parasitol. 2012, 190, 241–245. [Google Scholar] [CrossRef]
- Schares, G.; Basso, W.; Majzoub, M.; Rostaher, A.; Scharr, J.C.; Langenmayer, M.C.; Selmair, J.; Dubey, J.P.; Cortes, H.C.; Conraths, F.J.; et al. Comparative evaluation of immunofluorescent antibody and new immunoblot tests for the specific detection of antibodies against Besnoitia besnoiti tachyzoites and bradyzoites in bovine sera. Vet. Parasitol. 2010, 171, 32–40. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Nb of Herds Importing Cattle from Areas at Risk | Nb of Imported Cattle Tested with B. besnoiti Ab ELISA | Nb of Bovines with Non-Negative B. besnoiti Ab ELISA (Confirmed by WB) | Nb of Herds with Non-Negative B. besnoiti Ab ELISA (Confirmed by WB) |
|---|---|---|---|---|
| 2018 | 206 | 1816 | 0 (0) | 0 (0) |
| 2019 | 221 | 1868 | 0 (0) | 0 (0) |
| 2020 | 236 | 2441 | 6 (1) | 2 (1) |
| 2021 | 159 | 1497 | 6 (4) | 4 (3) |
| Total | 822 | 7622 | 12 (5) | 6 (4) |
| Year | Nb of Herds Importing Cattle from Areas at Risk | Nb of Imported Cattle Tested with B. besnoiti Ab ELISA | Nb of Bovines with Non-Negative B. besnoiti Ab ELISA (Confirmed by WB) | Nb of Herds with Non-Negative B. besnoiti Ab ELISA (Confirmed by WB) |
|---|---|---|---|---|
| 2019 | 130 | 676 | 1 (1) | 1 (1) |
| 2020 | 546 | 2785 | 7 (5) | 5 (3) |
| 2021 | 67 | 162 | 0 | 0 |
| Total | 743 | 3623 | 8 (6) | 6 (4) |
| Age Category | Nb Tested | Nb Seropositive ELISA (Confirmed by WB) | % Positive in B. besnoiti Ab ELISA | % Positive in WB * |
|---|---|---|---|---|
| 6–12 months | 35 | 2 (2) | 5.7 | 5.7 |
| 1–2 years | 14 | 0 (0) | 0 | 0 |
| 2–4 years | 18 | 7 (4) | 38.9 | 22.2 |
| 4–6 years | 7 | 3 (0) | 42.9 | 0 |
| 6–8 years | 12 | 3 (2) | 25 | 16.7 |
| >8 years | 11 | 4 (2) | 36.4 | 18.2 |
| Total | 97 | 19 (10) | 19.6 | 10.3 |
| Infected Herd | Tracing Back |
|---|---|
| H1 | Import of animals coming from three different herds of two departments: Aveyron, Cantal |
| H2 | Grazing contact with pasture from H1 |
| H3 | Purchase of animals from H1 |
| H4 | Purchase of an animal from H2 |
| H5 | Import of animals coming from one herd of one department: Arriège |
| H6 | Import of animals coming from one herd of one department: Hautes-Pyrénées |
| H7 | Import of animals coming from one herd of one department: Gironde |
| H8 | Import of animals coming from one herd of one department: Doubs |
| H9 | Import of animals coming from one herd of one department: Allier |
| H10 | Import of animals coming from two herds of two departments: Hautes-Pyrénées, Lot-et-Garonne |
| H11 | Import of animals coming from one herd of one department: Haute-Vienne |
| H12 | Import of animals coming from one herd of one department: Arriège |
| Age Category | Nb Tested | Nb Seropositive B. besnoiti Ab ELISA (WB) | % Positive in B. besnoiti Ab ELISA | % Positive in WB |
|---|---|---|---|---|
| 6–12 months | 5 | 0 (0) | 0 | 0 |
| 1–2 years | 7 | 0 (0) | 0 | 0 |
| 2–4 years | 29 | 2 (2) | 6.9 | 6.9 |
| 4–6 years | 11 | 0 (0) | 0 | 0 |
| 6–8 years | 2 | 0 (0) | 0 | 0 |
| >8 years | 1 | 0 (0) | 0 | 0 |
| Total | 55 | 2 (2) | 3.6 | 3.6 |
| Herd Size | Number of Cattle to Sample |
|---|---|
| >260 | 20 |
| 80–260 | 19 |
| 40–79 | 18 |
| 20–39 | 16 |
| 16–19 | 13 |
| 14–15 | 12 |
| 13 | 11 |
| 12 | 10 |
| 10–11 | 9 |
| 1–9 | All animals |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delooz, L.; Evrard, J.; Mpouam, S.E.; Saegerman, C. Emergence of Besnoitia besnoiti in Belgium. Pathogens 2021, 10, 1529. https://doi.org/10.3390/pathogens10121529
Delooz L, Evrard J, Mpouam SE, Saegerman C. Emergence of Besnoitia besnoiti in Belgium. Pathogens. 2021; 10(12):1529. https://doi.org/10.3390/pathogens10121529
Chicago/Turabian StyleDelooz, Laurent, Julien Evrard, Serge Eugene Mpouam, and Claude Saegerman. 2021. "Emergence of Besnoitia besnoiti in Belgium" Pathogens 10, no. 12: 1529. https://doi.org/10.3390/pathogens10121529
APA StyleDelooz, L., Evrard, J., Mpouam, S. E., & Saegerman, C. (2021). Emergence of Besnoitia besnoiti in Belgium. Pathogens, 10(12), 1529. https://doi.org/10.3390/pathogens10121529